
Novel Ratio Soluble Fms-like Tyrosine Kinase-1/Angiotensin-II (sFlt-1/ANG-II) in Pregnant Women Is Associated with Critical Illness in COVID-19

 ,
,  ,
,  ,
,  ,
,  , ,
, ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Plasma Measurements of ACE-2, ANG-II, and sFlt-1
2.4. Outcome
2.5. Statistical Analysis
3. Results
3.1. Description of the Cohort and Characteristics of the Study Population
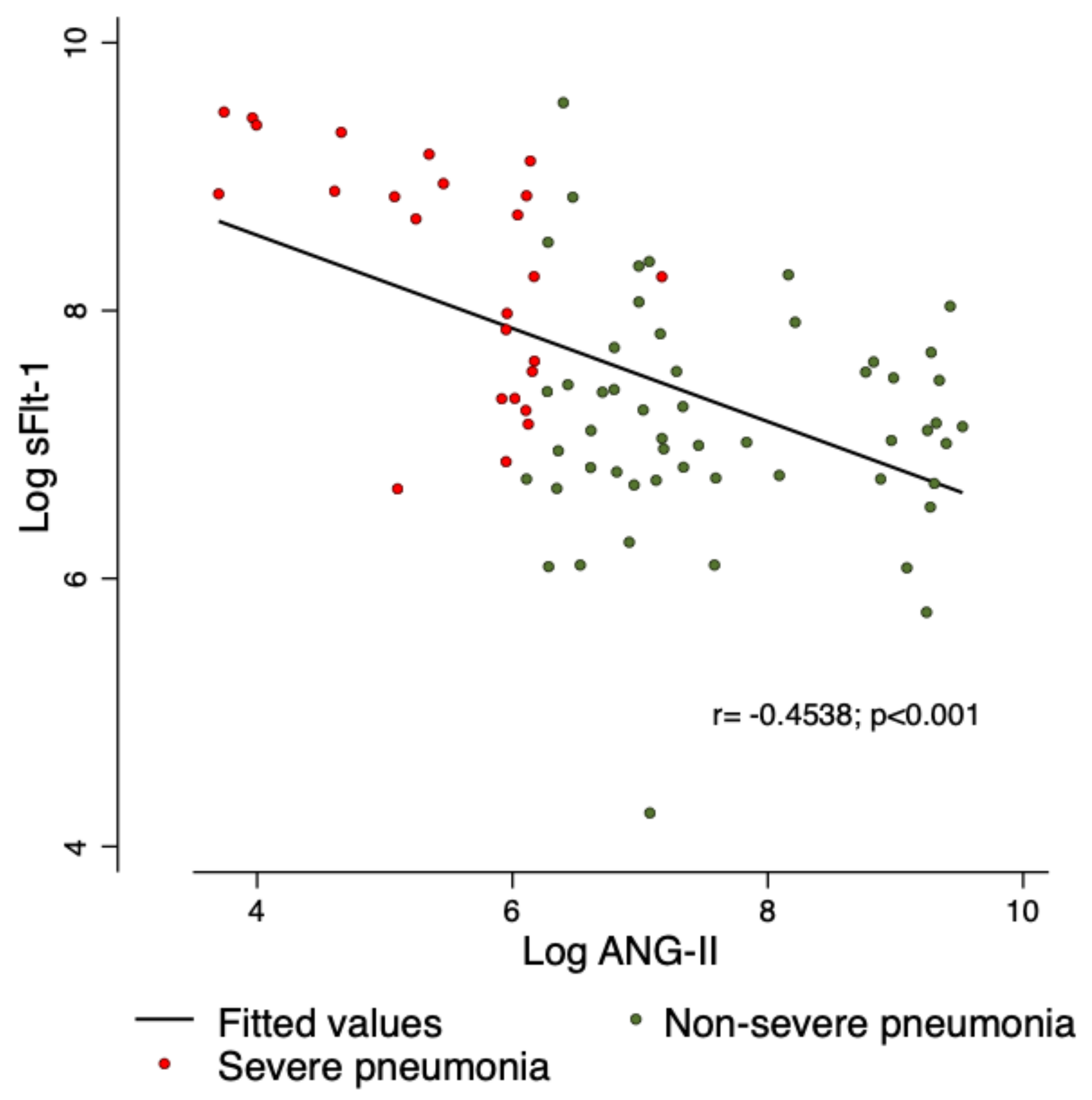
3.2. Correlation between sFlt-1 and ANG-II
3.3. Association with the Primary and Secondary Outcomes
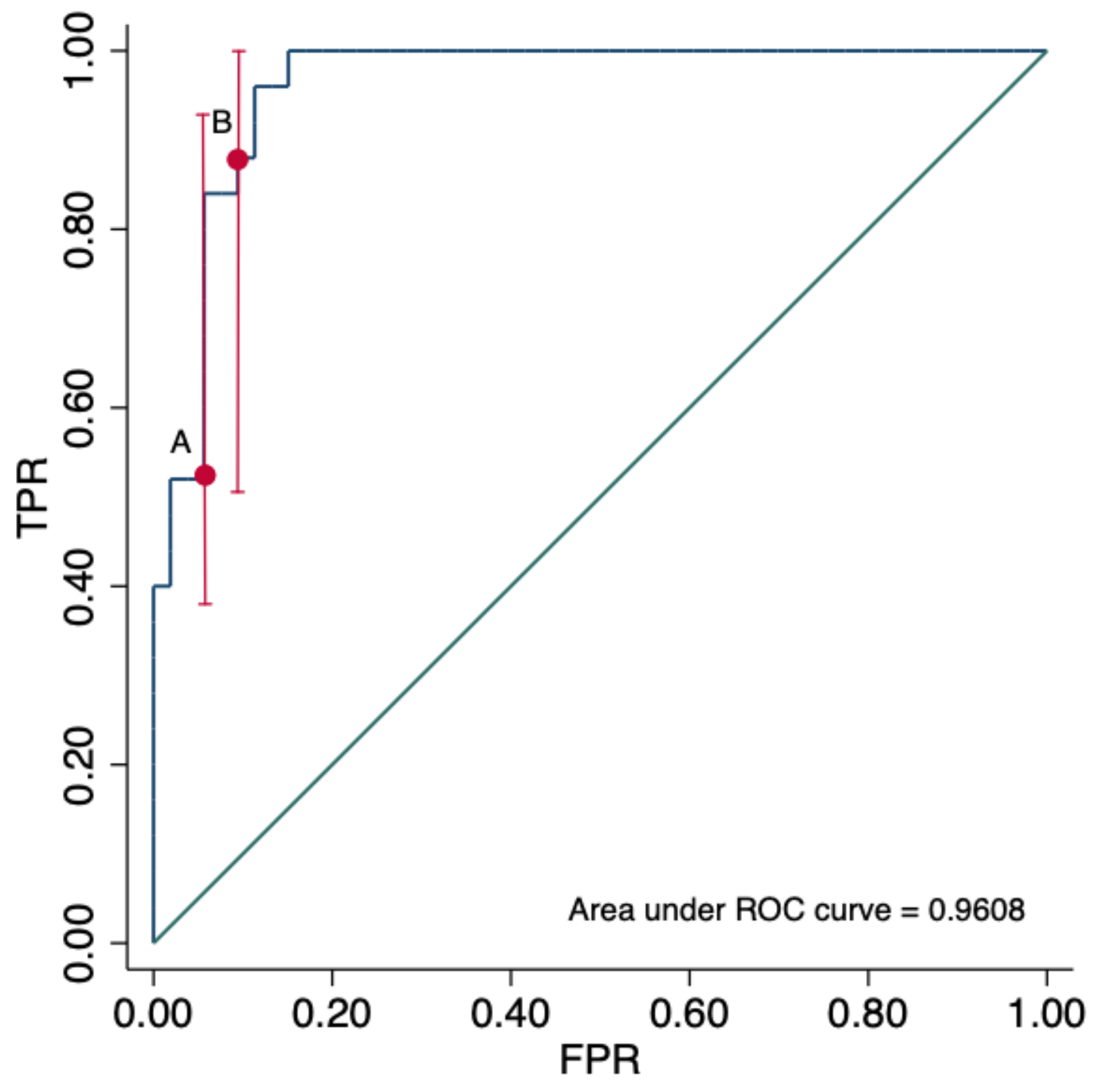
3.4. sFlt-1/ANG-II Ratio for the Prediction of Adverse Outcomes in COVID-19
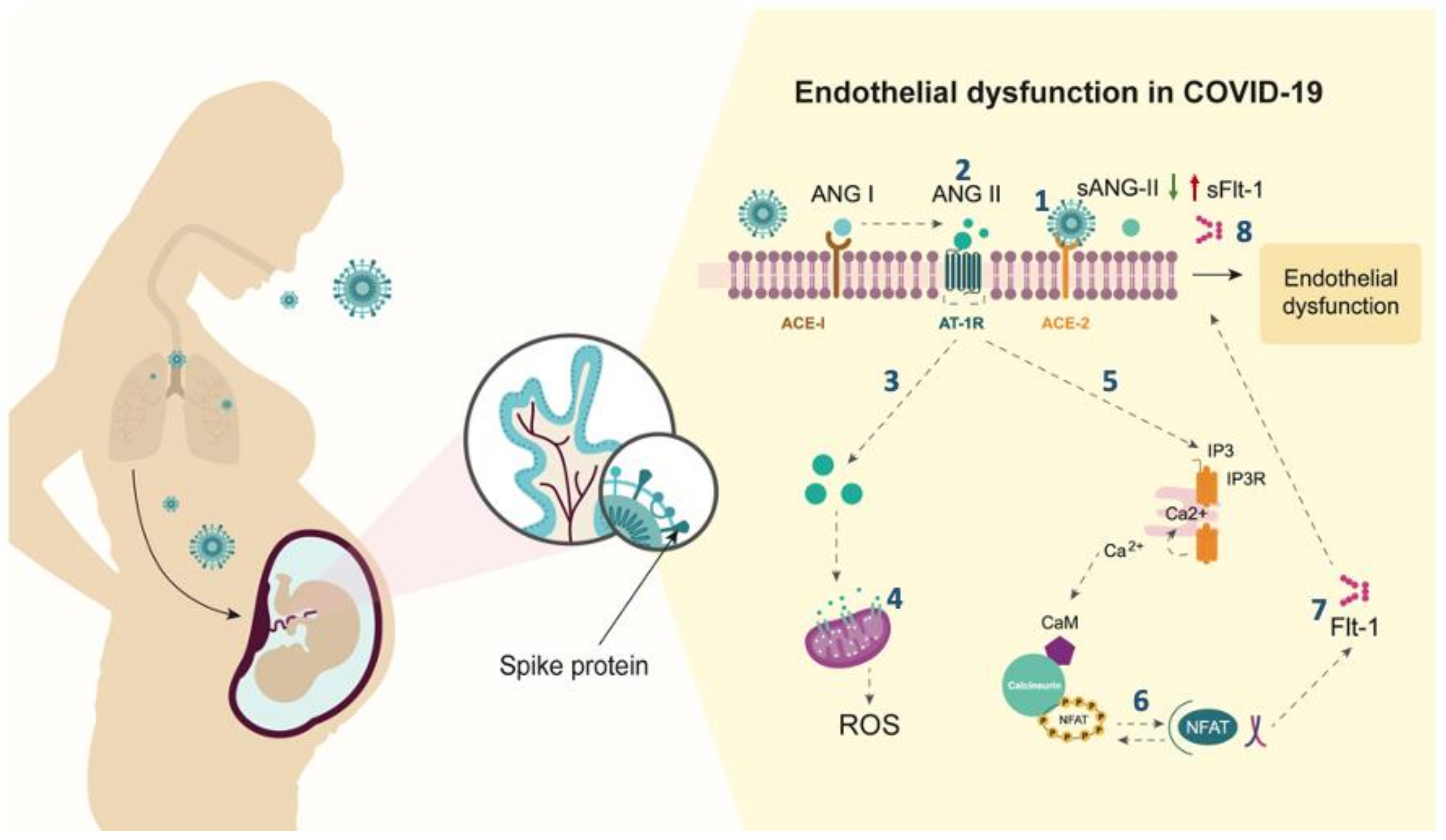
3.5. Hypothetical Molecular Mechanisms Contributing to the Pathogenesis of Severe COVID-19 in Pregnant Women
4. Discussion
4.1. Main Findings
4.2. Comparison with Existing Literature
4.3. Strengths and Limitations
4.4. Clinical Interpretation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martinez-Portilla, R.J.; Sotiriadis, A.; Chatzakis, C.; Torres-Torres, J.; Espino, Y.S.S.; Sandoval-Mandujano, K.; Castro-Bernabe, D.A.; Medina-Jimenez, V.; Monarrez-Martin, J.C.; Figueras, F.; et al. Pregnant women with SARS-CoV-2 infection are at higher risk of death and pneumonia: Propensity score matched analysis of a nationwide prospective cohort (COV19Mx). Ultrasound Obstet. Gynecol. 2021, 57, 224–231. [Google Scholar] [CrossRef]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F., 3rd; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status-United States, 22 January–3 October 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, R.A.S.; Sampaio, W.O.; Alzamora, A.C.; Motta-Santos, D.; Alenina, N.; Bader, M.; Campagnole-Santos, M.J. The ACE2/Angiotensin-(1-7)/MAS Axis of the Renin-Angiotensin System: Focus on Angiotensin-(1-7). Physiol. Rev. 2018, 98, 505–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luther, J.M.; Gainer, J.V.; Murphey, L.J.; Yu, C.; Vaughan, D.E.; Morrow, J.D.; Brown, N.J. Angiotensin II induces interleukin-6 in humans through a mineralocorticoid receptor-dependent mechanism. Hypertension 2006, 48, 1050–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sargiacomo, C.; Sotgia, F.; Lisanti, M.P. COVID-19 and chronological aging: Senolytics and other anti-aging drugs for the treatment or prevention of corona virus infection? Aging 2020, 12, 6511–6517. [Google Scholar] [CrossRef]
- Pringle, K.G.; Tadros, M.A.; Callister, R.J.; Lumbers, E.R. The expression and localization of the human placental prorenin/renin-angiotensin system throughout pregnancy: Roles in trophoblast invasion and angiogenesis? Placenta 2011, 32, 956–962. [Google Scholar] [CrossRef]
- Irani, R.A.; Xia, Y. The functional role of the renin-angiotensin system in pregnancy and preeclampsia. Placenta 2008, 29, 763–771. [Google Scholar] [CrossRef] [Green Version]
- Pavličev, M.; Wagner, G.P.; Chavan, A.R.; Owens, K.; Maziarz, J.; Dunn-Fletcher, C.; Kallapur, S.G.; Muglia, L.; Jones, H. Single-cell transcriptomics of the human placenta: Inferring the cell communication network of the maternal-fetal interface. Genome Res. 2017, 27, 349–361. [Google Scholar] [CrossRef]
- Powe, C.E.; Levine, R.J.; Karumanchi, S.A. Preeclampsia, a disease of the maternal endothelium: The role of antiangiogenic factors and implications for later cardiovascular disease. Circulation 2011, 123, 2856–2869. [Google Scholar] [CrossRef]
- AlGhatrif, M.; Cingolani, O.; Lakatta, E.G. The Dilemma of Coronavirus Disease 2019, Aging, and Cardiovascular Disease: Insights From Cardiovascular Aging Science. JAMA Cardiol. 2020, 5, 747–748. [Google Scholar] [CrossRef] [Green Version]
- Ni, W.; Yang, X.; Yang, D.; Bao, J.; Li, R.; Xiao, Y.; Hou, C.; Wang, H.; Liu, J.; Yang, D.; et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit. Care 2020, 24, 422. [Google Scholar] [CrossRef]
- Sacks, D.; Baxter, B.; Campbell, B.C.V.; Carpenter, J.S.; Cognard, C.; Dippel, D.; Eesa, M.; Fischer, U.; Hausegger, K.; Hirsch, J.A.; et al. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int. J. Stroke 2018, 13, 612–632. [Google Scholar] [CrossRef] [Green Version]
- Campbell, N.; LaMarca, B.; Cunningham, M.W., Jr. The Role of Agonistic Autoantibodies to the Angiotensin II Type 1 Receptor (AT1-AA) in Pathophysiology of Preeclampsia. Curr. Pharm. Biotechnol. 2018, 19, 781–785. [Google Scholar] [CrossRef]
- Murphy, S.R.; Cockrell, K. Regulation of soluble fms-like tyrosine kinase-1 production in response to placental ischemia/hypoxia: Role of angiotensin II. Physiol. Rep. 2015, 3, e12310. [Google Scholar] [CrossRef] [PubMed]
- Flores-Pliego, A.; Miranda, J.; Vega-Torreblanca, S.; Valdespino-Vázquez, Y.; Helguera-Repetto, C.; Espejel-Nuñez, A.; Borboa-Olivares, H.; Espino, Y.S.S.; Mateu-Rogell, P.; León-Juárez, M.; et al. Molecular Insights into the Thrombotic and Microvascular Injury in Placental Endothelium of Women with Mild or Severe COVID-19. Cells 2021, 10, 364. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet. Gynecol. 2020, 135, e237–e260. [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Yang, H.; Kapur, A.; Melamed, N.; Dao, B.; Divakar, H.; McIntyre, H.D.; Kihara, A.B.; Ayres-de-Campos, D.; Ferrazzi, E.M.; et al. Global interim guidance on coronavirus disease 2019 (COVID-19) during pregnancy and puerperium from FIGO and allied partners: Information for healthcare professionals. Int. J. Gynaecol. Obstet. 2020, 149, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Yang, J.; Mei, J.; Jin, Y.; Lu, Y. Head-to-head comparison of qSOFA and SIRS criteria in predicting the mortality of infected patients in the emergency department: A meta-analysis. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 56. [Google Scholar] [CrossRef] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, L.; Zhang, D.; Xu, J.; Dai, H.; Tang, N.; Su, X.; Cao, B. SARS-CoV-2 and viral sepsis: Observations and hypotheses. Lancet 2020, 395, 1517–1520. [Google Scholar] [CrossRef]
- Cunningham, M.W., Jr.; Castillo, J.; Ibrahim, T.; Cornelius, D.C.; Campbell, N.; Amaral, L.; Vaka, V.R.; Usry, N.; Williams, J.M.; LaMarca, B. AT1-AA (Angiotensin II Type 1 Receptor Agonistic Autoantibody) Blockade Prevents Preeclamptic Symptoms in Placental Ischemic Rats. Hypertension 2018, 71, 886–893. [Google Scholar] [CrossRef]
- Xia, Y.; Ramin, S.M.; Kellems, R.E. Potential roles of angiotensin receptor-activating autoantibody in the pathophysiology of preeclampsia. Hypertension 2007, 50, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Li, X.C.; Zhou, X.; Zhuo, J.L. Evidence for a Physiological Mitochondrial Angiotensin II System in the Kidney Proximal Tubules: Novel Roles of Mitochondrial Ang II/AT(1a)/O(2)(-) and Ang II/AT(2)/NO Signaling. Hypertension 2020, 76, 121–132. [Google Scholar] [CrossRef]
- Kawai, T.; Forrester, S.J.; O’Brien, S.; Baggett, A.; Rizzo, V.; Eguchi, S. AT1 receptor signaling pathways in the cardiovascular system. Pharmacol. Res. 2017, 125, 4–13. [Google Scholar] [CrossRef]
- Giardini, V.; Carrer, A.; Casati, M.; Contro, E.; Vergani, P.; Gambacorti-Passerini, C. Increased sFLT-1/PlGF ratio in COVID-19: A novel link to angiotensin II-mediated endothelial dysfunction. Am. J. Hematol. 2020, 95, e188–e191. [Google Scholar] [CrossRef]
- Negro, A.; Fama, A.; Penna, D.; Belloni, L.; Zerbini, A.; Giuri, P.G. SFLT-1 levels in COVID-19 patients: Association with outcome and thrombosis. Am. J. Hematol. 2021, 96, e41–e43. [Google Scholar] [CrossRef] [PubMed]
- Eleuteri, D.; Montini, L.; Cutuli, S.L.; Rossi, C.; Alcaro, F.; Antonelli, M. Renin-angiotensin system dysregulation in critically ill patients with acute respiratory distress syndrome due to COVID-19: A preliminary report. Crit. Care 2021, 25, 91. [Google Scholar] [CrossRef]
- Orfanos, S.E.; Armaganidis, A.; Glynos, C.; Psevdi, E.; Kaltsas, P.; Sarafidou, P.; Catravas, J.D.; Dafni, U.G.; Langleben, D.; Roussos, C. Pulmonary capillary endothelium-bound angiotensin-converting enzyme activity in acute lung injury. Circulation 2000, 102, 2011–2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurol-Urganci, I.; Jardine, J.E.; Carroll, F.; Draycott, T.; Dunn, G.; Fremeaux, A.; Harris, T.; Hawdon, J.; Morris, E.; Muller, P.; et al. Maternal and perinatal outcomes of pregnant women with SARS-CoV-2 infection at the time of birth in England: National cohort study. Am. J. Obstet. Gynecol. 2021, 2021. [Google Scholar] [CrossRef]
- Mendoza, M.; Garcia-Ruiz, I.; Maiz, N.; Rodo, C.; Garcia-Manau, P.; Serrano, B.; Lopez-Martinez, R.M.; Balcells, J.; Fernandez-Hidalgo, N.; Carreras, E.; et al. Pre-eclampsia-like syndrome induced by severe COVID-19: A prospective observational study. BJOG Int. J. Obstetr. Gynaecol. 2020, 127, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Papageorghiou, A.T.; Deruelle, P.; Gunier, R.B.; Rauch, S.; García-May, P.K.; Mhatre, M.; Usman, M.A.; Abd-Elsalam, S.; Etuk, S.; Simmons, L.E.; et al. Preeclampsia and COVID-19: Results from the INTERCOVID prospective longitudinal study. Am. J. Obstet. Gynecol. 2021, 225, 289.e1–289.e17. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Non-Severe COVID-19 n = 55 | Severe COVID-19 n = 25 | p-Value |
|---|---|---|---|
| Maternal age (years) | 29.05 (24.94–33.5) | 30.56 (28.40–33.73 | 0.185 |
| Gestational age at diagnosis (weeks) | 33.4 (28.0–38.1) | 32.0 (27.2–36.1) | 0.557 |
| pBMI (kg/m2) | 29.72 (25.0–33.8) | 28.2 (23.4–33.5) | 0.739 |
| MAP (mmHg) | 87.7 (82.7–95.0) | 86.0 (80.0–89.7) | 0.301 |
| Smoking | 1 (1.82%) | 0 | 0.497 |
| Chronic hypertension | 3 (5.45%) | 1 (4.00%) | 0.782 |
| Pre-gestational diabetes | 3 (5.45%) | 0 | 0.234 |
| Asthma | 1 (1.82%) | 0 | 0.497 |
| Chronic renal disease | 4 (7.27%) | 1 (4.00%) | 0.575 |
| SpO2% | 94.5 (92.5–96.0) | 92.5 (78–97.5) | 0.713 |
| Preeclampsia (clinical diagnosis) | 11 (20.75%) | 5 (20.0%) | 0.939 |
| True preeclampsia (Suspected preeclampsia + anormal sFlt-1/PlGF ratio) | 6 (10.9%) | 2 (8.0%) | 0.118 |
| Threatened preterm labor | 2 (3.77%) | 1 (4.00%) | 0.961 |
| Fetal growth restriction | 4 (7.55%) | 5 (20.0%) | 0.108 |
| Stillbirth | 0 | 1 (4.00%) | 0.143 |
| Pneumonia | 0 | 25 (100%) | <0.0001 |
| ICU admission | 0 | 11 (44.0%) | <0.0001 |
| Intubation | 0 | 7 (31.82%) | <0.0001 |
| Viral sepsis | 0 | 3 (12.0%) | 0.009 |
| Multiple organ dysfunction | 0 | 3 (12.0%) | 0.009 |
| Maternal death | 0 | 2 (8.00%) | 0.034 |
| Characteristic | Non-Severe COVID-19 n = 55 | Severe COVID-19 n = 25 | p-Value |
|---|---|---|---|
| Leukocytes (×10/L) | 8.15 (7.2–10.1) | 8.5 (7.1–13.5) | 0.339 |
| Neutrophils (×10/L) | 6.40 (5.30–7.60) | 7.1 (5.6–12.6) | 0.093 |
| Lymphocytes (×10/L) | 1.30 (1.0–1.5) | 1.0 (0.6–1.4) | 0.071 |
| Hemoglobin (g/dL) | 12.4 (11.3–13.9) | 11.9 (11–12.7) | 0.086 |
| Hematocrit % | 37.6 (34.0–41.6) | 35.7 (32.6–38.7) | 0.245 |
| Platelets (×103/L) | 212 (184–270) | 227 (170–271) | 0.975 |
| Glucose (mg/dL) | 78.0 (73–85) | 84 (72–120) | 0.260 |
| Creatinine (mg/dL) | 0.55 (0.49–0.64) | 0.54 (0.46–0.67) | 0.624 |
| Uric acid (mg/dL) | 4.4 (3.8–5.8) | 3.9 (3.4–5.0) | 0.285 |
| AST (U/L) | 20.5 (17–28) | 26 (21–36) | 0.042 |
| ALT (U/L) | 17.5 (12–25) | 23 (17–40) | 0.082 |
| LDH (U/L) | 173 (146–212) | 197 (152–295) | 0.112 |
| Direct bilirubin (mg/dL) | 0.10 (0.06–0.14) | 0.19 (0.07–0.42) | 0.029 |
| Indirect bilirubin(mg/dL) | 0.32 (0.25–0.43) | 0.34 (0.28–0.48) | 0.464 |
| Triglycerides (mg/dL) | 263 (203–313) | 265 (210–312) | 0.885 |
| Total cholesterol (mg/dL) | 197 (172–235) | 154 (118–217) | 0.017 |
| D-dimer (ng/mL) | 1549 (1242–2981) | 1438 (1248–2511) | 0.302 |
| Fibrinogen (mg/dL) | 526 (481–591) | 570 (428–611) | 0.521 |
| PTT (seconds) | 26.2 (24.8–29.2) | 26.9 (24.8–28.9) | 0.949 |
| PT (seconds) | 10.8 (10.55–11.4) | 10.3 (9.9–11) | 0.398 |
| C-RP (mg/L) | 21.1 (6.45–81.7) | 61.15 (16.5–188) | 0.014 |
| Procalcitonin (ng/mL) | 0.05 (0.03–0.13) | 0.2 (0.07–0.53) | 0.0006 |
| PlGF (pg/mL) | 150.1 (56–215.6) | 114.3 (32.29–212.3) | 0.186 |
| sFlt-1 (pg/mL) | 1424 (1054–2099) | 6119 (2099–7900) | 0.0001 |
| ACE-2 (pg/mL) | 8754 (6040–27480) | 7904 (5928–14216) | 0.324 |
| ANG-II (pg/mL) | 1479 (915.3–7873) | 404.3 (180.8–471) | 0.0001 |
| sFlt1/PlGF ratio | 11.21 (5.43–26.38) | 53.72 (31.87–126.12) | 0.0001 |
| sFlt-1/ANG-II ratio | 0.92 (0.25–2.03) | 14.27 (4.47–42.46) | 0.0001 |
| Biochemical Marker | OR | 95% CI | p-Value |
|---|---|---|---|
| AST (U/L) | 1.00 | 0.99–1.00 | 0.636 |
| Direct bilirubin (mg/dL) | 15.69 | 0.81–303.44 | 0.069 |
| Total cholesterol (mg/dL) | 0.99 | 0.98–1.00 | 0.064 |
| C-RP (mg/L) | 1.01 | 1.00–1.02 | 0.025 |
| Procalcitonin (ng/mL) | 1.12 | 0.67–1.88 | 0.651 |
| sFlt1 (pg/mL) | 1.01 | 1.00–1.01 | <0.0001 |
| ANG-II (pg/mL) | 0.99 | 0.98–0.99 | 0.001 |
| sFlt1/PlGF | 1.02 | 1.00–1.03 | 0.002 |
| sFlt-1/ANG-II | 1.31 | 1.09–1.56 | 0.003 |
| Outcome | Se (95% CI) | Sp 95% CI | Positive LR 95% CI | Negative LR (95% CI) |
|---|---|---|---|---|
| Severe pneumonia | 0.96 (0.88–1.0) | 0.886 (0.80–0.972) | 8.48 (3.97–18) | 0.045 (0.01–0.31) |
| ICU admission | 1.0 (1.0–1.0) | 0.716 (0.443–0.789) | 3.52 (2.26–4.95) | 0.01 (0.01–0.88) |
| Intubation | 1.0 (1.0–1.0) | 0.705 (0.567–0.784) | 3.4 (1.93–4.20) | 0.01 (0.01–1.54) |
| Viral sepsis | 1.0 (1.0–1.0) | 0.64 (0.531–0.748) | 2.77 (1.50–3.89) | 0.01 (0.01–2.63) |
| Maternal death | 1.0 (1.0–1.0) | 0.631 (0.523–0.74) | 2.71 (1.26–4.04) | 0.01 (0.01–3.34) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espino-y-Sosa, S.; Martinez-Portilla, R.J.; Torres-Torres, J.; Solis-Paredes, J.M.; Estrada-Gutierrez, G.; Hernandez-Pacheco, J.A.; Espejel-Nuñez, A.; Mateu-Rogell, P.; Juarez-Reyes, A.; Lopez-Ceh, F.E.; et al. Novel Ratio Soluble Fms-like Tyrosine Kinase-1/Angiotensin-II (sFlt-1/ANG-II) in Pregnant Women Is Associated with Critical Illness in COVID-19. Viruses 2021, 13, 1906. https://doi.org/10.3390/v13101906
Espino-y-Sosa S, Martinez-Portilla RJ, Torres-Torres J, Solis-Paredes JM, Estrada-Gutierrez G, Hernandez-Pacheco JA, Espejel-Nuñez A, Mateu-Rogell P, Juarez-Reyes A, Lopez-Ceh FE, et al. Novel Ratio Soluble Fms-like Tyrosine Kinase-1/Angiotensin-II (sFlt-1/ANG-II) in Pregnant Women Is Associated with Critical Illness in COVID-19. Viruses. 2021; 13(10):1906. https://doi.org/10.3390/v13101906
Chicago/Turabian StyleEspino-y-Sosa, Salvador, Raigam Jafet Martinez-Portilla, Johnatan Torres-Torres, Juan Mario Solis-Paredes, Guadalupe Estrada-Gutierrez, Jose Antonio Hernandez-Pacheco, Aurora Espejel-Nuñez, Paloma Mateu-Rogell, Angeles Juarez-Reyes, Francisco Eduardo Lopez-Ceh, and et al. 2021. "Novel Ratio Soluble Fms-like Tyrosine Kinase-1/Angiotensin-II (sFlt-1/ANG-II) in Pregnant Women Is Associated with Critical Illness in COVID-19" Viruses 13, no. 10: 1906. https://doi.org/10.3390/v13101906