
Women’s Narratives about COVID-19, Preventive Practices and Sources of Information in Northwestern Tanzania



{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
Study Design and Methods
3. Results
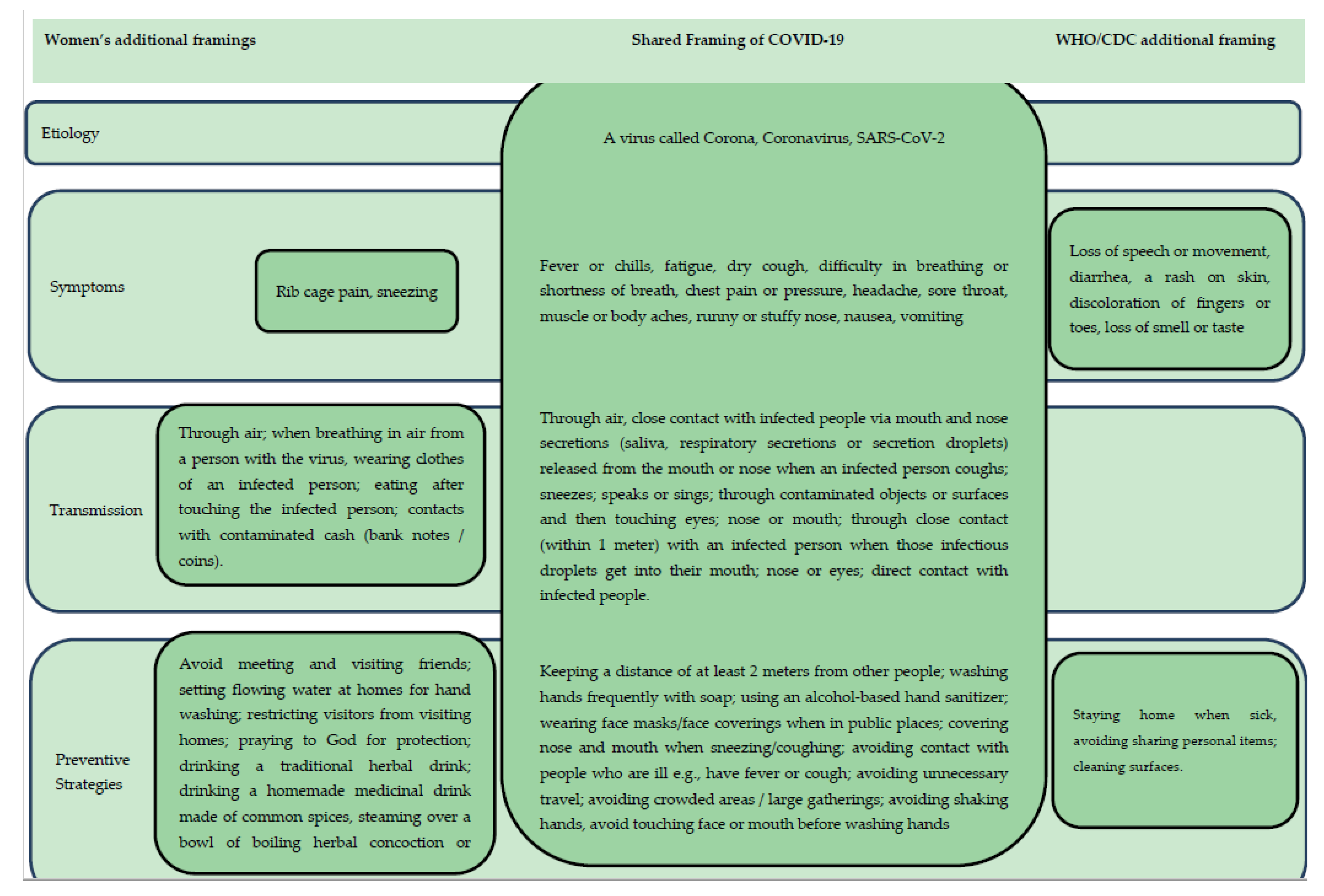
3.1. Women’s Understanding of COVID-19
3.1.1. COVID-19 as a Deadly Disease
“This disease kills fast and quickly, it can kill a large number of people within a short period of time, it makes one not breath as normal and it affects the lungs and by affecting the lungs it causes death easily.” (1DI-16)
“As I understand, this coronavirus disease is very dangerous. It is a deadly disease.” (1DI-01)
“Corona is a bad disease that kills for a short period of time. It can kill many people in a short period of time.” (IDI-17)
“From what I understand, this corona virus disease is a disease just like any other. We got the feeling that it was new because we had never seen it or heard of it but then after staying with it for several months, we have just started considering it as any other disease. Therefore, we have to protect ourselves like we do with other diseases.” (IDI-03)
3.1.2. Perceived Etiology of COVID-19
Participants appeared to have a clear concept of the etiology of COVID-19, understanding that the disease is infectious, caused by a virus called corona. As one woman put it, “Coronavirus disease is a disease caused by a virus known as COVID-19.” (IDI-16)
3.1.3. Perceived Symptoms of COVID-19
“The symptoms of corona virus disease include severe headache, having high fever, sore throat, difficult breathing, and one may fail to breath and sometimes vomits a lot. I think those are the main signs […] including body weakness.” (ID-I1)
“The symptoms of this coronavirus disease are coughing, high fever, sore throat, rib cage pain, chest pain and severe headache.” (IDI-10)
“We were told that the symptoms of the disease include rib cage pain, severe headache, sneezing, and others.” (IDI-06)
“When corona was announced, there was a time when I felt sick. I had high fever, flu, and I felt very cold. I think you know it is the seasonal period when people get sick often. So, I thought to myself may be this is corona because the flu got really serious, so I took malaria and flu medicine and I later felt fine. You just find yourself worried and taking other precautions, as for me, I decided to stay indoors and even used the traditional medicines and remedies for my own sake. The sickness lasted for a week and I was back to being normal.” (IDI-16)
3.1.4. Perceived Transmission Routes of COVID-19
“Corona is a disease that is transmitted through the respiratory system. When someone sneezes without wearing barakoa (face mask/face covering) or blocking the propelled droplets with a hand, when the watery substances reach another person, it is one of the sources through which one could be infected with coronavirus.” (1DI-01)
“Coronavirus disease spreads through the nose and mouth when a person splits watery substance. […] When the infected person sneezes and he is near you, the watery substances coming from their mouth or nose if it gets to you, it’s likely for you to be affected by the disease.” (IDI-16)
“If you touch a person with corona you get the disease […] another way is if you eat after touching the infected person you can easily get the disease. And also, if you wear clothes of the infected person you can also get the disease, and the final one is through money exchange like changes from the shop, public transports and others, if the money has been touched with an infected person and you also touch it, you can easily get corona, I think those are the ways of being infected with coronavirus.” (IDI-04)
“We were told that one might get the disease by holding each other’s hands, hugging each other, touching eyes, nose or mouth.” (IDI-06)
“Someone can also get the disease if they touch a person with the disease without any protection. You might touch her/him and get in contact with those viruses.” (IDI-15)
“They taught us that one can even get it (COVID-19) through air. When you stay close to someone with the corona virus disease, they spread it to you through air [...] that’s what I was taught.” (IDI-12)
“Corona virus disease is the disease that spreads through air [...] if someone breathes in air from a person with the coronavirus disease [...] that’s how you can get the disease.” (IDI-10)
“First of all, I know that this is a disease that spreads through air and other things like those. That’s how I understand. I don’t know about other things. I know it spreads through air and sitting or staying close to someone else.” (IDI-09)
“It’s a dangerous disease that is transmitted through air or watery substance like saliva.” (IDI-7)
“What I know about corona is that schools and even some businesses were closed because of it, this was because the disease spreads through air.” (IDI-16)
3.2. Preventive Practices against COVID-19
3.2.1. Preventive Practices Based on WHO/CDC or Biomedical Frame
“What I actually did was avoiding large gatherings. When I went out, I made sure I have my barakoa on. I also stopped going to the bar or meeting up with friends.” (IDI-16)
“Was by washing hands more often, using sanitizers when am back home or even going out even in public transportation I really had to wear barakoa but also in places which are very crowded.” (IDI-17)
“I prepared a bucket full of water and a liquid hand washing soap. So, whenever I received a visitor or when my children came from school, they had to wash their hands first before coming in.” (IDI-09)
“You know I even stopped entertaining visitors at home, we were told not to invite people at our homes, you can invite a person but you don’t know if they have corona or not.” (IDI-13)
“Whenever my kids wanted to go to church it was a must they go with their masks on. We placed a cane full of water and soap so that the children would wash their hands whenever they came back from anywhere. So, we protected ourselves in that design.” (IDI-15)
3.2.2. Preventive Practices Based on the Traditional Medicine Frame
“I have steamed myself a lot, my kids as well have done that, […] what I know about the steaming process is that you really sweat. The ingredients that I used were eucalyptus, guava leaves and other herbs, we boiled them, then steamed ourselves while covering with a sheet that doesn’t allow air to penetrate, we all did this, even my husband, after the whole process we felt okay, you feel like you’re no longer tired.” (IDI-#02)
“We decided to steam ourselves because we heard people saying that the disease has no cure so we should take all the necessary precautions and even steam ourselves.” (IDI-#02)
3.2.3. Preventive Practices Based on Religious Frame
“I also prayed to God that this disease should end. I just prayed to God for protection.” (IDI-08)
“We prayed and reminded God to protect Tanzania from the coronavirus disease and he listened. The situation is as you can see right now. We don’t wear barakoa like before. We only wash our hands with flowing water, in the past we stopped gathering but now we can attend our gatherings as usual.” (IDI-01)
3.3. Sources of Information about COVID-19
“The first time I heard of it was on radio and TV. They said there was an outbreak of a dangerous disease called corona. They announced that we had to be very careful.” (IDI-06)
“I got information about the disease from the radio […] I heard from the Television that there is a disease called corona which started in China, but later spread to other countries then reached Kenya and finally in Tanzania. I got news about the disease before it even reached in our country through the Media.” (IDI-16)
“I got more information from the Television but also radios and phone. I got information from the social media like Facebook and WhatsApp.” (IDI-10)
“I really like watching You Tube videos, I first saw news about the disease from there, they said it killed many people in China, so from there I started making follow ups on what was going on until it reached Tanzania. What I can say is YouTube was my source of information, or generally the internet gave me information.” (IDI-04)
“I got news through the radio and also in church, but for church they really emphasized about it, they made us become really aware of the disease existence […] so that made us realize that the disease is serious. Although they talked about it in the TV, we came to take it serious when we heard from the church.” (IDI-07)
“I also got the information from the religious sources. They announced this (about COVID-19) for us in mosques.” (IDI-05)
“I heard from the television but also the church really talked about it, and it’s when I realized that this was serious.” (IDI-17)
“From the beginning I got information from people around me, my neighbors, workmates and business partners, in our daily conversations we would talk about the increase of patients confirmed having COVID-19 by the government and so on.” (IDI-16)
“I got the information from people who were going around announcing about the disease and teaching us how to protect ourselves.” (IDI-12)
“I heard about the disease through community sensitization which was done by the government through the local government and other government officials who were selected to provide us information on coronavirus. They gave us education on precaution to be taken like washing of hands, using of masks and others.” (IDI-11)
“We were also informed in the small supportive groups we attend. We formed these groups to support one another (financially) but we had to close them to avoid gatherings.” (IDI-06)
“I liked listening to news which I heard from the government through our local leaders, or the media, they gave us trusted news on the spread of the disease and the precautions to be taken. I really didn’t believe much on the news from the social media because people gave rumors that brought fear to us, so I had to avoid such news.” (IDI-11)
“I trusted what was broadcasted in the radio, and you know when you listen to people, they would give you false information, but the media gives you trusted news/information.” (IDI-04)
“I got information from the media like the television and radios […]. I couldn’t consider information I heard from other sources like people. I only trusted the media.” (IDI-17)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Munster, V.J.; Koopmans, M.; Van Doremalen, N.; Van Riel, D.; De Wit, E. A novel coronavirus emerging in China—Key questions for impact assessment. N. Engl. J. Med. 2020, 382, 692–694. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19); WHO: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 7 May 2021).
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Zar, H.J.; Dawa, J.; Fischer, G.B.; Castro-Rodriguez, J.A. Challenges of COVID-19 in children in low- and middle-income countries. Paediatr. Respir. Rev. 2020, 35, 70–74. [Google Scholar] [CrossRef]
- Gupta, M.; Wahl, B.; Adhikari, B.; Bar-Zeev, N.; Bhandari, S.; Coria, A.; Erchick, D.J.; Gupta, N.; Hariyani, S.; Kagucia, E.W.; et al. The need for COVID-19 research in low- and middle-income countries. Glob. Health Res. Policy 2020, 5, 1–4. [Google Scholar] [CrossRef]
- Tarimo, C.S.; Wu, J. The first confirmed case of COVID-19 in Tanzania: Recommendations based on lesson learned from China. Trop. Med. Health 2020, 48, 1–3. [Google Scholar] [CrossRef] [PubMed]
- MoHCDEC Tanzania. Government Measures to Curb the Spread of Coronavirus in Tanzania. Available online: https://www.moh.go.tz/en/covid-19-info (accessed on 19 March 2021).
- Goffman, E. Frame Analysis: An Essay on the Organization of Experience; Northwestern University Press: Boston, MA, USA, 1974. [Google Scholar]
- Entman, R.M. Framing: Toward clarification of a fractured paradigm. J. Commun. 1993, 43, 51–58. [Google Scholar] [CrossRef]
- Mshana, G.; Mchome, Z.; Aloyce, D.; Peter, E.; Kapiga, S.; Stöckl, H. Contested or complementary healing paradigms? Women’s narratives of COVID-19 remedies in Mwanza, Tanzania. J. Ethnobiol. Ethnomed. 2021, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mchome, Z.; Mshana, G.; Aloyce, D.; Peter, E.; Malibwa, D.; Dwarumpudi, A.; Kapiga, S.; Stöckl, H. “Don’t you think it is violence forcing me to have sex while not happy?” Women’s conceptualization of enjoyable sex and sexual intimate partner violence in Mwanza, Tanzania. Int. J. Environ. Res. Public Health 2020, 17, 7937. [Google Scholar] [CrossRef]
- Kapiga, S.; Harvey, S.; Mshana, G.; Hansen, C.H.; Mtolela, G.J.; Madaha, F.; Hashim, R.; Kapinga, I.; Mosha, N.; Abramsky, T.; et al. A social empowerment intervention to prevent intimate partner violence against women in a microfinance scheme in Tanzania: Findings from the MAISHA cluster randomised controlled trial. Lancet Glob. Health 2019, 7, e1423–e1434. [Google Scholar] [CrossRef] [Green Version]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Kebede, Y.; Yitayih, Y.; Birhanu, Z.; Mekonen, S.; Ambelu, A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma University Medical Center visitors, Southwest Ethiopia. PLoS ONE 2020, 15, e0233744. [Google Scholar] [CrossRef] [PubMed]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Lau, L.L.; Hung, N.; Go, D.J.; Ferma, J.; Choi, M.; Dodd, W.; Wei, X. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: A cross-sectional study. J. Glob. Health 2020, 10. [Google Scholar] [CrossRef]
- Azlan, A.A.; Hamzah, M.R.; Sern, T.J.; Ayub, S.H.; Mohamad, E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS ONE 2020, 15, e0233668. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Jimenez, J.L.; Prather, K.A.; Tufekci, Z.; Fisman, D.; Schooley, R. Ten scientific reasons in support of airborne transmission of SARS-CoV-2. Lancet 2021, 397, 1603–1605. [Google Scholar] [CrossRef]
- Downs, J.A.; Fuunay, L.D.; Fuunay, M.; Mbago, M.; Mwakisole, A.; Peck, R.N.; Downs, D.J. ‘The body we leave behind’: A qualitative study of obstacles and opportunities for increasing uptake of male circumcision among Tanzanian Christians: Table 1. BMJ Open 2013, 3, e002802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, M.E. Risks of self-medication practices. Curr. Drug Saf. 2010, 5, 315–323. [Google Scholar] [CrossRef]
- World Health Organization. Q&A: Influenza and COVID-19—Similarities and Differences. Available online: https://www.who.int/westernpacific/news/q-a-detail/q-a-similarities-and-differences-covid-19-and-influenza (accessed on 20 March 2021).
- US Centers for Disease Control and Prevention. Similarities and Differences between Flu and COVID-19. Available online: https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm (accessed on 20 March 2021).
- Ano, G.G.; Vasconcelles, E.B. Religious coping and psychological adjustment to stress: A meta-analysis. J. Clin. Psychol. 2005, 61, 461–480. [Google Scholar] [CrossRef] [PubMed]
- Baer, H.A. Medical pluralism. In The International Encyclopedia of Anthropology; Wiley: Hoboken, NJ, USA, 2018; pp. 1–3. [Google Scholar]
- Muela, S.H.; Ribera, J.M.; Tanner, M. Fake malaria and hidden parasites—The ambiguity of malaria. Anthr. Med. 1998, 5, 43–61. [Google Scholar] [CrossRef]
- Brewster, C.T.; Choong, J.; Thomas, C.; Wilson, D.; Moiemen, N. Steam inhalation and paediatric burns during the COVID-19 pandemic. Lancet 2020, 395, 1690. [Google Scholar] [CrossRef]
- Burnard, P. The telephone interview as a data collection method. Nurse Educ. Today 1994, 14, 67–72. [Google Scholar] [CrossRef]
- Fontana, A.; Frey, J.H. The interview: From neutral stance to political involvement. In The SAGE Handbook of Qualitative Research; Lincoln, Y.S., Denzin, N.K., Eds.; Sage Publishing: Thousand Oaks, CA, USA, 2005; pp. 695–727. [Google Scholar]
- Opdenakker, R. Advantages and disadvantages of four interview techniques in qualitative research. Forum Qual. Sozialforsch. 2006, 7. [Google Scholar] [CrossRef]
- Sturges, J.E.; Hanrahan, K.J. Comparing telephone and face-to-face qualitative interviewing: A research note. Qual. Res. 2004, 4, 107–118. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mchome, Z.; Mshana, G.; Peter, E.; Aloyce, D.; Kapiga, S.; Stöckl, H. Women’s Narratives about COVID-19, Preventive Practices and Sources of Information in Northwestern Tanzania. Int. J. Environ. Res. Public Health 2021, 18, 5261. https://doi.org/10.3390/ijerph18105261
Mchome Z, Mshana G, Peter E, Aloyce D, Kapiga S, Stöckl H. Women’s Narratives about COVID-19, Preventive Practices and Sources of Information in Northwestern Tanzania. International Journal of Environmental Research and Public Health. 2021; 18(10):5261. https://doi.org/10.3390/ijerph18105261
Chicago/Turabian StyleMchome, Zaina, Gerry Mshana, Esther Peter, Diana Aloyce, Saidi Kapiga, and Heidi Stöckl. 2021. "Women’s Narratives about COVID-19, Preventive Practices and Sources of Information in Northwestern Tanzania" International Journal of Environmental Research and Public Health 18, no. 10: 5261. https://doi.org/10.3390/ijerph18105261