
Predicting COVID-19 Infections in Eswatini Using the Maximum Likelihood Estimation Method


Abstract
:1. Introduction
2. Materials and Methods
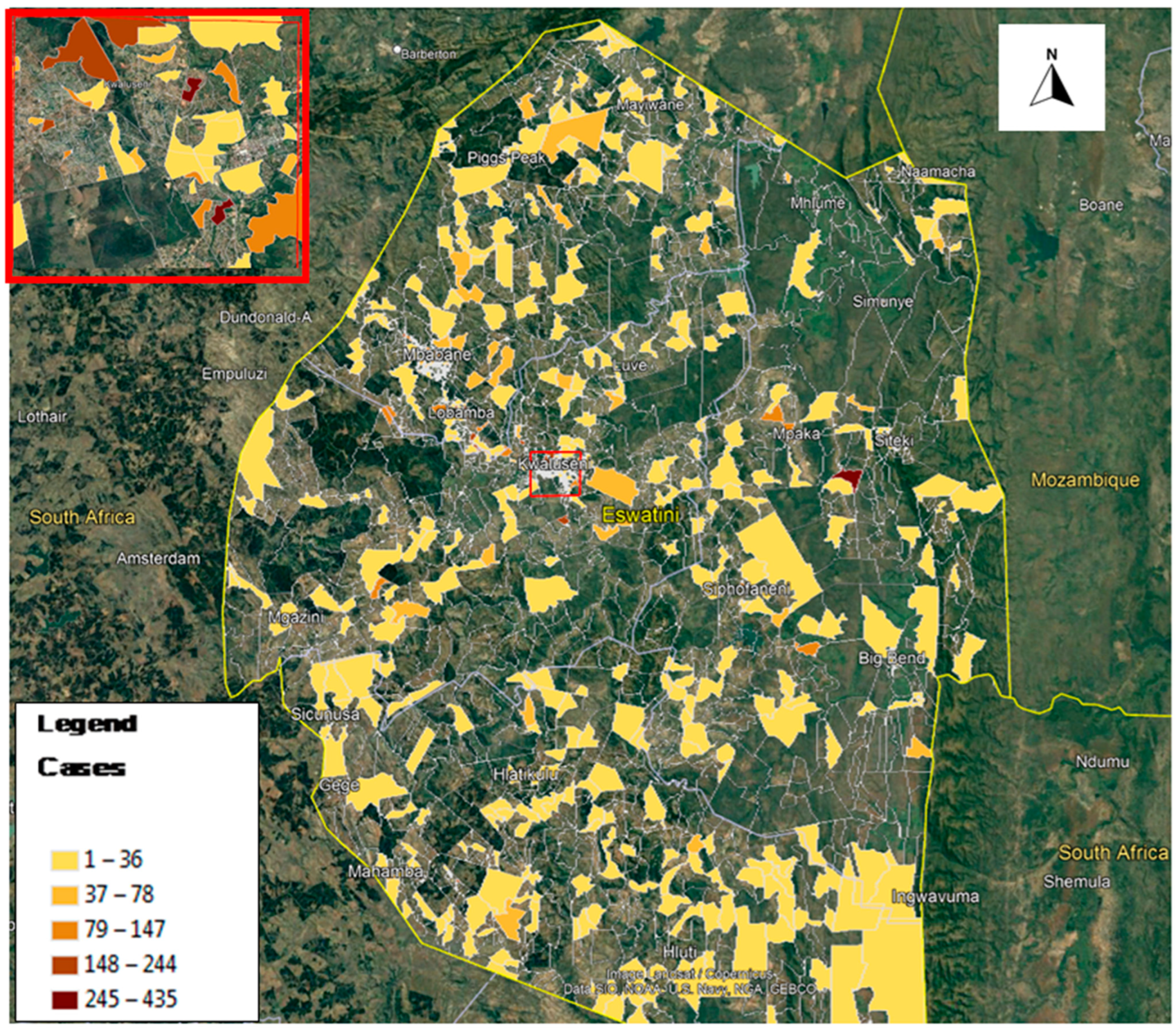
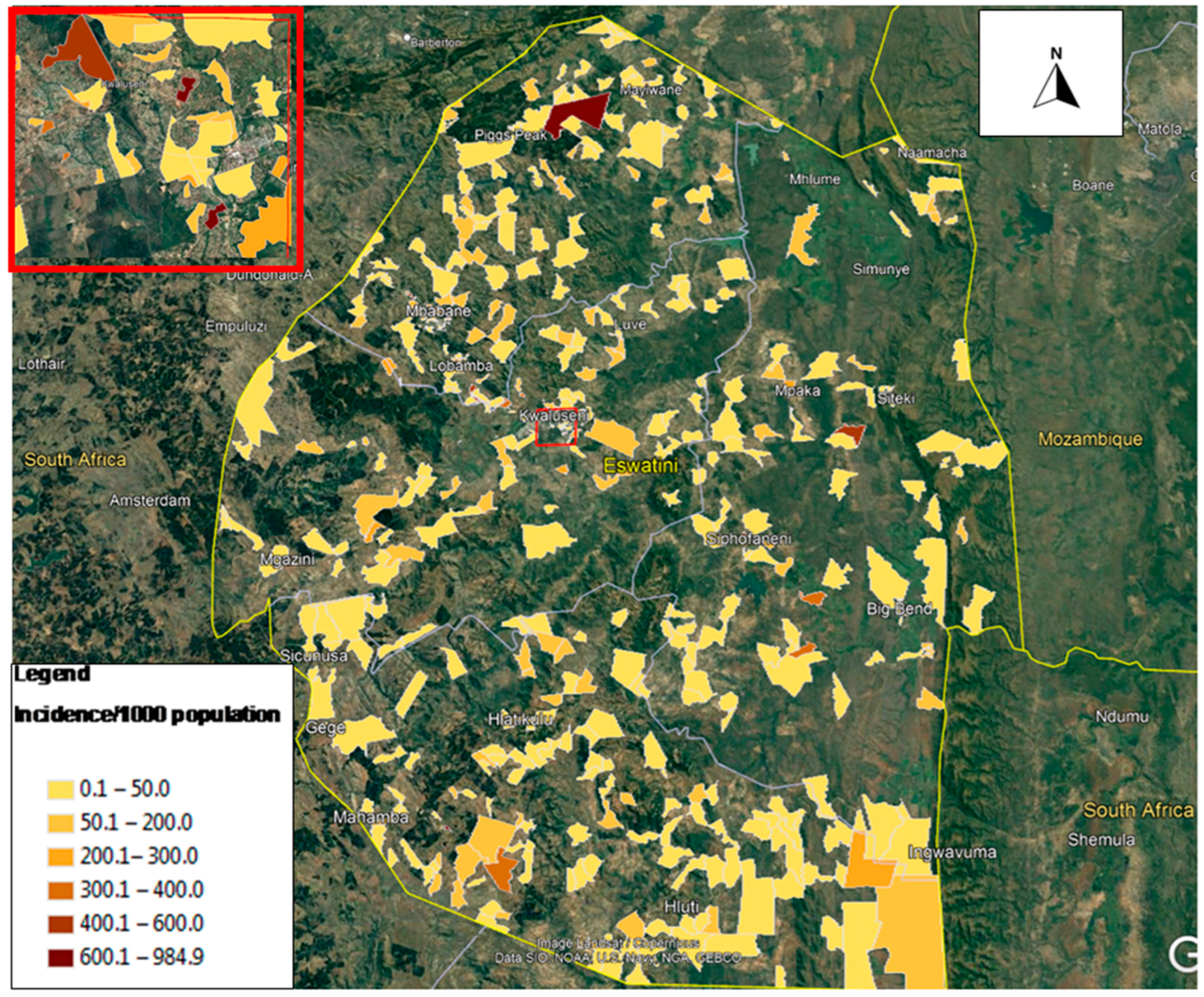
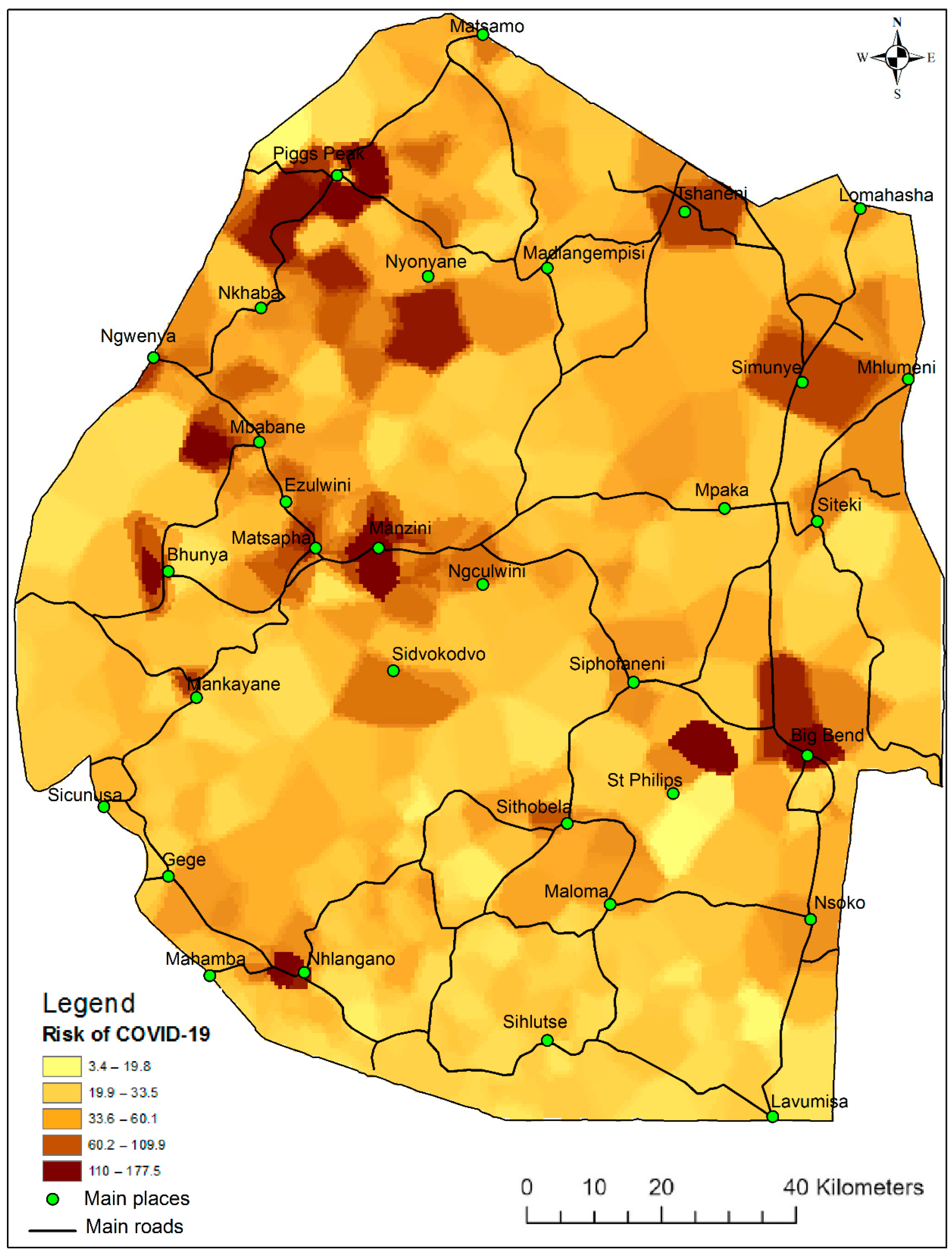
2.1. Study Area and Data Sources
2.2. Statistical Modeling
3. Results and Discussion
3.1. Generalized Poisson Regression Model
3.2. Age and COVID-19 Infections
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, X.; Yu, B. First two months of the 2019 Coronavirus Disease (COVID-19) epidemic in China: Real-time surveillance and evaluation with a second derivative model. Glob. Health Res. Policy 2020, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.C.; Cicinelli, M.V.; Gilbert, S.S.; Honavar, S.G.; Murthy, G.V.S. COVID-19 pandemic: Lessons learned and future directions. Indian J. Ophthalmol. 2020, 68, 703–710. [Google Scholar] [CrossRef]
- Chaudhry, R.; Dranitsaris, G.; Mubashir, T.; Bartoszko, J.; Riazi, S. A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes. EClinicalMedicine 2020, 25, 100464. [Google Scholar] [CrossRef] [PubMed]
- Qian, M.; Jiang, J. COVID-19 and social distancing. J. Public Health 2022, 30, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, D.; Biswasroy, P.; Kumar Naik, P.; Ghosh, G.; Rath, G. A Review of Current Interventions for COVID-19 Prevention. Arch. Med. Res. 2020, 51, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Hashim, M.J.; Alsuwaidi, A.R.; Khan, G. Population Risk Factors for COVID-19 Mortality in 93 Countries. J. Epidemiol. Glob. Health 2020, 10, 204–208. [Google Scholar] [CrossRef]
- Sorci, G.; Faivre, B.; Morand, S. Explaining among-country variation in COVID-19 case fatality rate. Sci. Rep. 2020, 10, 18909. [Google Scholar] [CrossRef]
- Demombynes, G. COVID-19 Age-Mortality Curves Are Flatter in Developing Countries; World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Peters, D.J. Community Susceptibility and Resiliency to COVID-19 Across the Rural-Urban Continuum in the United States. J. Rural Health 2020, 36, 446–456. [Google Scholar] [CrossRef]
- Pasquali, G.; Godfrey, S. Governance of Eswatini Apparel Regional Value Chains and the Implications of Covid-19. Eur. J. Dev. Res. 2022, 34, 473–502. [Google Scholar] [CrossRef]
- Nhapi, T.G.; Dhemba, J. The conundrum of old age and COVID-19 responses in Eswatini and Zimbabwe. Int. Soc. Work 2020, 63, 842–846. [Google Scholar] [CrossRef]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, e2146. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Koh, V.; Marimuthu, K.; Ng, O.T.; Young, B.; Vasoo, S.; Chan, M.; Lee, V.J.M.; De, P.P.; Barkham, T.; et al. Epidemiological and Clinical Predictors of COVID-19. Clin. Infect. Dis. 2020, 71, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; Chorath, K.; Rajasekaran, K.; Burmeister, F.; Ahmed, M.; Moreira, A. Demographic predictors of hospitalization and mortality in US children with COVID-19. Eur. J. Pediatr. 2021, 180, 1659–1663. [Google Scholar] [CrossRef]
- Dlamini, W.M.; Dlamini, S.N.; Mabaso, S.D.; Simelane, S.P. Spatial risk assessment of an emerging pandemic under data scarcity: A case of COVID-19 in Eswatini. Appl. Geogr. 2020, 125, 102358. [Google Scholar] [CrossRef] [PubMed]
- Consul, P.C.; Famoye, F. Generalized poisson regression model. Commun. Stat.-Theory Methods 1992, 21, 89–109. [Google Scholar] [CrossRef]
- COVID-19 Eswatini. Available online: http://datastudio.google.com/reporting/b847a713-0793-40ce-8196-e37d1cc9d720/page/2a0LB?feature=opengraph (accessed on 6 July 2022).
- Thompson, B. Stepwise Regression and Stepwise Discriminant Analysis Need Not Apply here: A Guidelines Editorial. Educ. Psychol. Meas. 1995, 55, 525–534. [Google Scholar] [CrossRef]
- Currie, I.; Korabinski, A. Some Comments on Bivariate Regression. J. R. Stat. Soc. Ser. Stat. 1984, 33, 283–293. [Google Scholar] [CrossRef]
- Gardner, W.; Mulvey, E.P.; Shaw, E.C. Regression analyses of counts and rates: Poisson, overdispersed Poisson, and negative binomial models. Psychol. Bull. 1995, 118, 392–404. [Google Scholar] [CrossRef]
- Greene, W.H. Accounting for Excess Zeros and Sample Selection in Poisson and Negative Binomial Regression Models; Social Science Research Network: Rochester, NY, USA, 1994. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Schober, P.; Vetter, T.R. Count Data in Medical Research: Poisson Regression and Negative Binomial Regression. Anesth. Analg. 2021, 132, 1378–1379. [Google Scholar] [CrossRef]
- Farshbafnadi, M.; Kamali Zonouzi, S.; Sabahi, M.; Dolatshahi, M.; Aarabi, M.H. Aging & COVID-19 susceptibility, disease severity, and clinical outcomes: The role of entangled risk factors. Exp. Gerontol. 2021, 154, 111507. [Google Scholar] [CrossRef]
- Leung, C. Risk factors for predicting mortality in elderly patients with COVID-19: A review of clinical data in China. Mech. Ageing Dev. 2020, 188, 111255. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Liu, Y.; Liu, Y.; Zhang, K.; Su, D.; Zhong, M.; Meng, X. Clinical characteristics and manifestations in older patients with COVID-19. BMC Geriatr. 2020, 20, 395. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Li, R.; Han, Y.; Zhang, R.; Li, J. COVID-19: Insight into the asymptomatic SARS-COV-2 infection and transmission. Int. J. Biol. Sci. 2020, 16, 2803–2811. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Rao, N.M.; Goenka, A.; Roderick, M.; Ramanan, A.V. Coronavirus Disease 2019 (COVID-19) in Children—What We Know So Far and What We Do Not. Indian Pediatr. 2020, 57, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Peng, J.; Xiong, Q.; Liu, Z.; Lin, H.; Tan, X.; Kang, M.; Yuan, R.; Zeng, L.; Zhou, P.; et al. Clinical, immunological and virological characterization of COVID-19 patients that test re-positive for SARS-CoV-2 by RT-PCR. eBioMedicine 2020, 59, 102960. [Google Scholar] [CrossRef]
- Pillay, J. COVID-19 Shows the Need to Make Church More Flexible. Transformation 2020, 37, 266–275. [Google Scholar] [CrossRef]
- Sigler, T.; Mahmuda, S.; Kimpton, A.; Loginova, J.; Wohland, P.; Charles-Edwards, E.; Corcoran, J. The socio-spatial determinants of COVID-19 diffusion: The impact of globalisation, settlement characteristics and population. Glob. Health 2021, 17, 56. [Google Scholar] [CrossRef]
- Liu, P.; McQuarrie, L.; Song, Y.; Colijn, C. Modelling the impact of household size distribution on the transmission dynamics of COVID-19. J. R. Soc. Interface 2021, 18, 20210036. [Google Scholar] [CrossRef]
- Hamidi, S.; Hamidi, I. Subway Ridership, Crowding, or Population Density: Determinants of COVID-19 Infection Rates in New York City. Am. J. Prev. Med. 2021, 60, 614–620. [Google Scholar] [CrossRef]
- Sugg, M.M.; Spaulding, T.J.; Lane, S.J.; Runkle, J.D.; Harden, S.R.; Hege, A.; Iyer, L.S. Mapping community-level determinants of COVID-19 transmission in nursing homes: A multi-scale approach. Sci. Total Environ. 2021, 752, 141946. [Google Scholar] [CrossRef]
- Gershengorn, H.B.; Patel, S.; Shukla, B.; Warde, P.R.; Bhatia, M.; Parekh, D.; Ferreira, T. Association of Race and Ethnicity with COVID-19 Test Positivity and Hospitalization Is Mediated by Socioeconomic Factors. Ann. Am. Thorac. Soc. 2021, 18, 1326–1334. [Google Scholar] [CrossRef] [PubMed]
- Bargain, O.; Aminjonov, U. Poverty and COVID-19 in Africa and Latin America. World Dev. 2021, 142, 105422. [Google Scholar] [CrossRef] [PubMed]
- Sehra, S.T.; George, M.; Wiebe, D.J.; Fundin, S.; Baker, J.F. Cell Phone Activity in Categories of Places and Associations With Growth in Cases of COVID-19 in the US. JAMA Intern. Med. 2020, 180, 1614–1620. [Google Scholar] [CrossRef]
- Shekhar, H.; Rautela, M.; Maqsood, M.; Paris, R.; Flores de León, R.M.; Romero-Aguirre, M.F.; Balinos, M.; Velázquez, M.E.; Amri, G.S.; Rahman, T.; et al. Are leading urban centers predisposed to global risks- An analysis of the global south from COVID-19 perspective. Habitat Int. 2022, 121, 102517. [Google Scholar] [CrossRef]
- Chung, S.-C.; Marlow, S.; Tobias, N.; Alogna, A.; Alogna, I.; You, S.-L.; Khunti, K.; McKee, M.; Michie, S.; Pillay, D. Lessons from countries implementing find, test, trace, isolation and support policies in the rapid response of the COVID-19 pandemic: A systematic review. BMJ Open 2021, 11, e047832. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | Variable | Variable Short Name | Format | Description |
|---|---|---|---|---|
| 1. | Cellphone usage | Cellphone | Floating point Values ranging from 0 to 1 | Proportion of cellphone users per EA |
| 2. | Church-distance | Church_dis | Floating point Distance (km) | Distance between EA and church |
| 3. | Elderly above 55 years | Elderly_55 | Floating point Values ranging from 0 to 100 | Percentage or number of people above 55 years of age per 1000 people in each EA |
| 4. | Household density | Hhld_dens | Floating point Number of buildings per unit area (km2) | Numerical quantities of the built up surface area in each EA |
| 5. | Household size | Hhld_size | Integer number Number of people per household | Number of persons living in a private dwelling unit |
| 6. | HIV Prevalence | HIV_prev | Floating point Values ranging from 0 to 100 | Percentage of people living with HIV in each EA |
| 7. | Internet connectivity | Internet | Floating point values ranging from 0 to 100 | Percentage of people connected to internet either via a computer or other devices |
| 8. | Poverty index | Po_index | Floating point Values ranging from 0 to 100 | Percentage of people living below USD 2 per day in each EA. |
| 9. | Building density | People_bld | Floating point Values ranging from 0 to 100 | Percentage of built up area in each EA |
| 10. | Youth proportion | Youth_prop | Floating point Values ranging from 0 to 100 | Percentage or rate of people below 35 years per 1000 people of age in each EA. |
| 11. | Shopping distance | Shop_dist | Floating point Distance (km) | Distance between EA and shopping area |
| 12. | Supermarket distance | Supmkt_dis | Floating point Distance (km) | Distance between EA and supermarket |
| 13. | Temperature | Temp | Floating point Degrees celcius | Hot/cold |
| 14. | Traffic mean | Traff_mean | Floating point Number of vehicles moving through an area per day per unit area (km2) | Numerical quantities of average traffic moving through each EA approximated as a surface area of that EA |
| 15. | Population density | Pop_dens | Floating point Number of people/per unit area (km2) | Numerical quantities of the populated surface area in each EA. |
| 16. | Total population | Integer number Number of people | Number of people in the entire country obtained by summing up the number of people recorded in each EA |
| Individual | IRR | Std Err. | z | P > z | 95% CI | |
|---|---|---|---|---|---|---|
| cellphone | 3.336945 | 2.693032 | 1.49 | 0.135 | 0.6861192 | 16.229 |
| church_dis | 0.991159 | 0.016569 | −0.53 | 0.595 | 0.9592107 | 1.0242 |
| elderly_55 | 0.984678 | 0.0025786 | −5.9 | 0.000 * | 0.979637 | 0.9897 |
| hhld_dens | 1.000045 | 0.0001841 | 0.25 | 0.806 | 0.9996845 | 1.0004 |
| hhld_size | 0.9565653 | 0.0408021 | −1.04 | 0.298 | 0.8798463 | 1.04 |
| hiv_prev | 0.3712601 | 0.3929613 | −0.94 | 0.349 | 0.046636 | 2.9555 |
| internet | 0.936553 | 0.4262686 | −0.14 | 0.885 | 0.3838055 | 2.2854 |
| p0_index | 1.00156 | 0.0044225 | 0.35 | 0.724 | 0.99293 | 1.0103 |
| people_bld | 0.9836968 | 0.0358074 | −0.45 | 0.652 | 0.9159606 | 1.0564 |
| pop_dens | 1.000002 | 0.0000865 | 0.03 | 0.977 | 0.999833 | 1.0002 |
| youth_prop | 0.0816543 | 0.0646422 | −3.16 | 0.002 * | 0.0173029 | 0.3853 |
| shop_dist | 0.9976175 | 0.0178658 | −0.13 | 0.894 | 0.9632086 | 1.0333 |
| supmkt_dis | 1.002583 | 0.0159068 | 0.16 | 0.871 | 0.9718864 | 1.0343 |
| temp | 0.9545037 | 0.0276899 | −1.61 | 0.108 | 0.9017466 | 1.0103 |
| traff_mean | 0.9999643 | 0.0000665 | −0.54 | 0.591 | 0.9998339 | 1.0001 |
| Mean Age by Symptoms | ||||
|---|---|---|---|---|
| Symptoms | Mean | SD | N | % N |
| No symptoms | 33.4 | 13.75 | 5566 | 42.86 |
| Mild | 34.8 | 11.23 | 4681 | 36.05 |
| Moderate to severe | 48.0 | 16.97 | 177 | 1.36 |
| Severe | 29.0 | 12.35 | 88 | 0.68 |
| Recovered | 36.0 | 10.78 | 1236 | 9.52 |
| Deceased | 58.0 | 1.41 | 177 | 1.36 |
| Unknown | 36.2 | 9.39 | 1060 | 8.16 |
| Total | 34.9 | 12.47 | 12,986 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dlamini, S.N.; Dlamini, W.M.; Fall, I.S. Predicting COVID-19 Infections in Eswatini Using the Maximum Likelihood Estimation Method. Int. J. Environ. Res. Public Health 2022, 19, 9171. https://doi.org/10.3390/ijerph19159171
Dlamini SN, Dlamini WM, Fall IS. Predicting COVID-19 Infections in Eswatini Using the Maximum Likelihood Estimation Method. International Journal of Environmental Research and Public Health. 2022; 19(15):9171. https://doi.org/10.3390/ijerph19159171
Chicago/Turabian StyleDlamini, Sabelo Nick, Wisdom Mdumiseni Dlamini, and Ibrahima Socé Fall. 2022. "Predicting COVID-19 Infections in Eswatini Using the Maximum Likelihood Estimation Method" International Journal of Environmental Research and Public Health 19, no. 15: 9171. https://doi.org/10.3390/ijerph19159171