
Developing the First Telenursing Service for COVID-19 Patients: The Experience of South Korea


Abstract
:1. Introduction
- To investigate the process of establishing the non-contact nursing counseling service;
- To review the contents of the educational materials and nursing service needed to establish the non-contact nursing counseling service;
- To analyze which factors associated with patients’ satisfaction with the non-contact nursing counseling service based on the discharge record sheets patients submitted at their discharge from the CTC.
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Non-Contact Nursing Counseling Service and Protocol
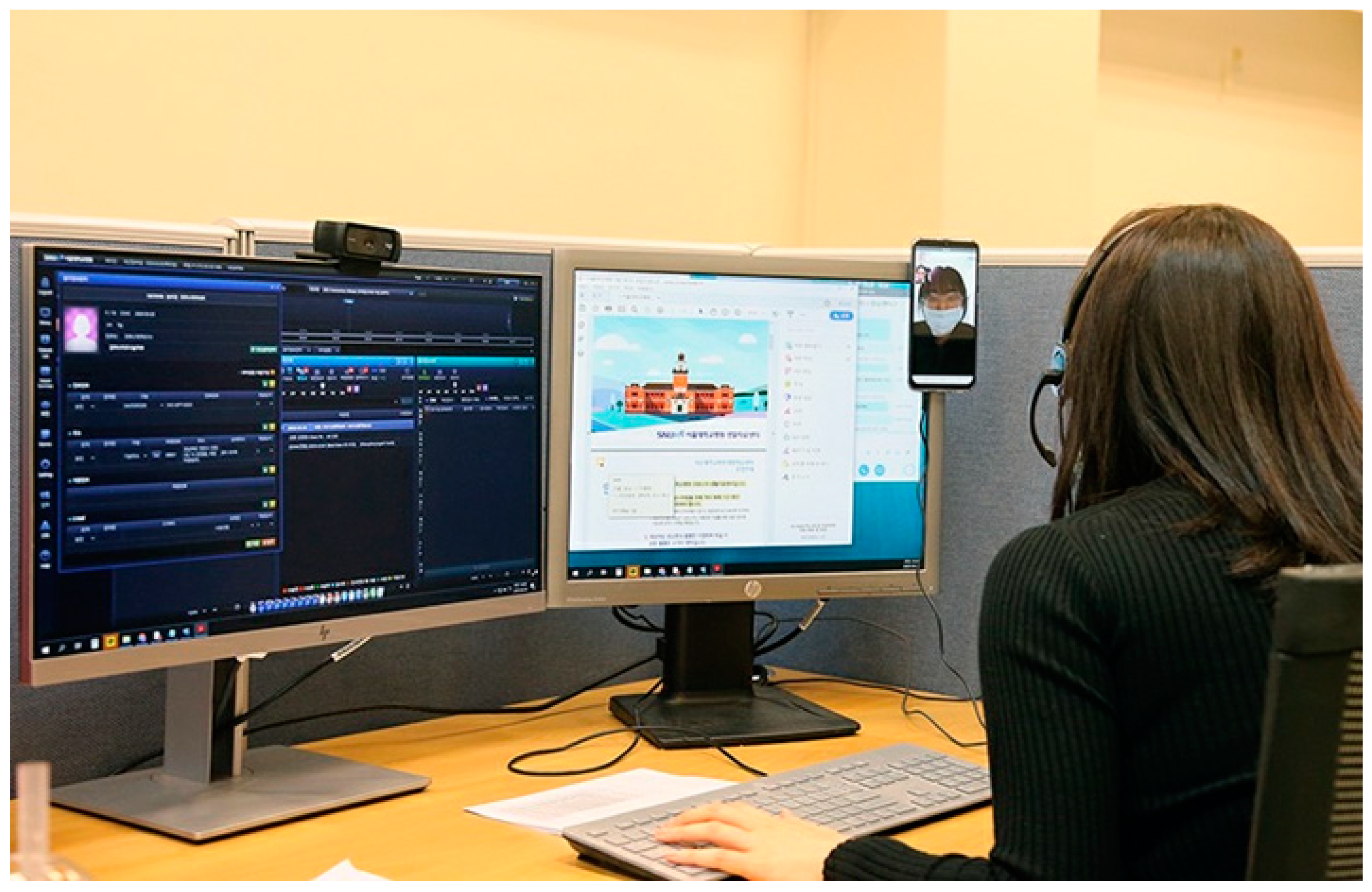
2.3.1. Non-Contact Nursing Counseling Service
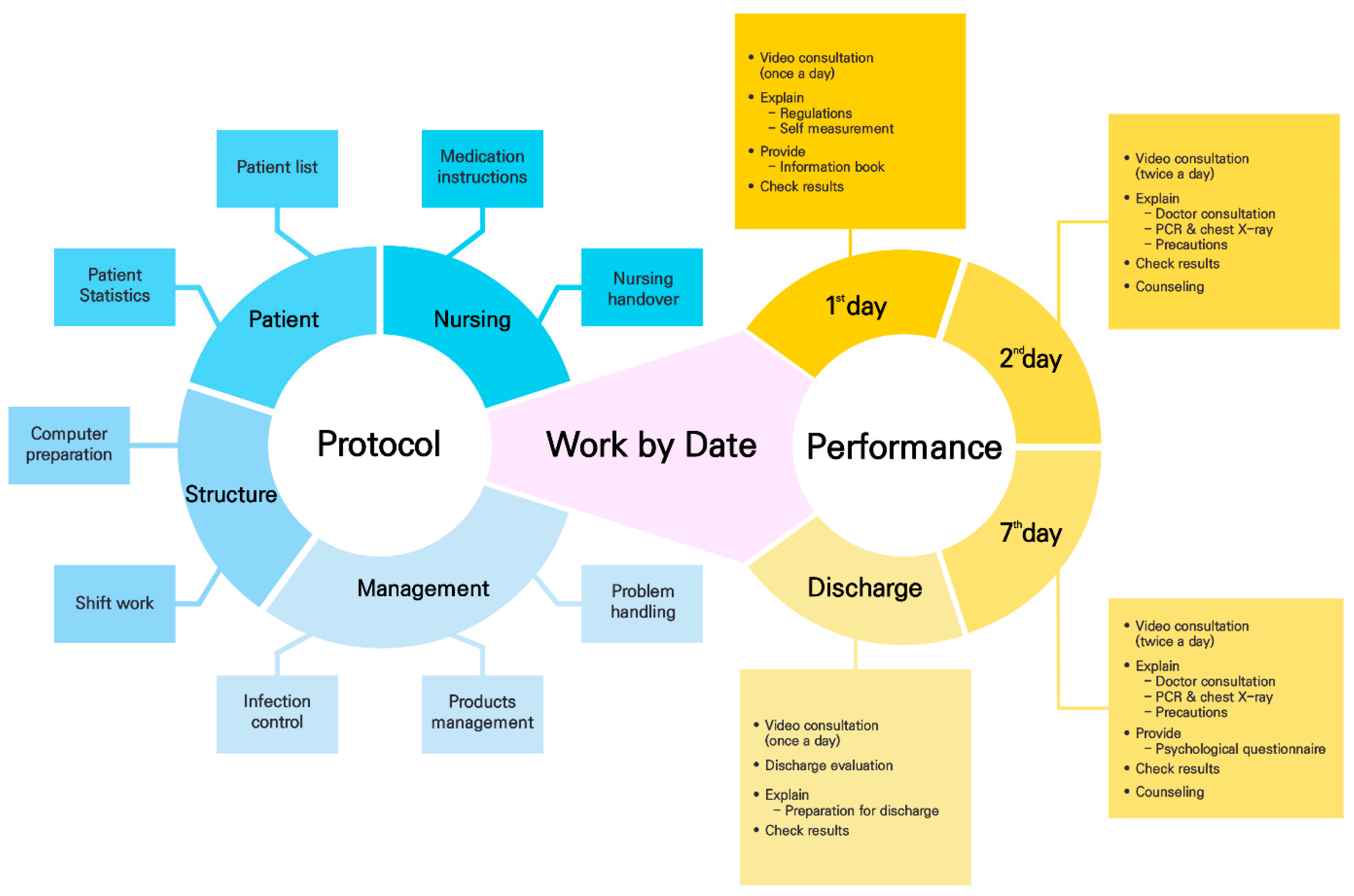
2.3.2. Non-Contact Nursing Counseling Service Protocol
- Day 1: The nurse in charge provided the video consultation (i.e., the initial evaluation) to the allocated patients to explain the living regulations and method of self-measurement; sent the video explaining the vital signs’ self-measurement method; checked the results on the basic admission information sheet, and provided information about the next day’s test.
- Day 2: A video consultation (i.e., the interim evaluation) was performed twice a day, and the information about the non-contact doctor’s counseling service and tests for individual patients was provided. In addition, counseling was performed regarding infection control, living in the CTC, and utilizing the facility.
- Day 7: In addition to the work performed on Day 2, information about a psychological test was provided.
- Discharge Day: A video consultation (i.e., the discharge evaluation) was performed, which offered details and guidance on preparing to leave the CTC.
2.4. Study Tools
2.5. Data Collection
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Establishing the Non-Contact Nursing Counseling Service System
3.2. Formats for Individual Departments and Educational Materials for the Non-Contact Nursing Counseling Service
3.3. Satisfaction and Convenience with Non-Contact Nursing Counseling Service
3.4. Patient Characteristics
3.5. Factors Associated with the Satisfaction and Convenience Level of Overall CTC Life
3.6. Stepwise Regression for the Satisfaction and Convenience Level of Overall CTC Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Welfare, Coronavirus Disease-19, Republic of Korea. Available online: http://ncov.mohw.go.kr/en/tcmBoardView.do?brdId=12&brdGubun=125&dataGubun=&ncvContSeq=4457&contSeq=4457&board_id=&gubun= (accessed on 22 December 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare, Coronavirus Disease-19, Republic of Korea. Available online: http://ncov.mohw.go.kr/en/tcmBoardView.do?brdId=12&brdGubun=125&dataGubun=&ncvContSeq=1279&contSeq=1279&board_id=&gubun= (accessed on 22 December 2020).
- Kim, J. Nurses’ experience of Middle East Respiratory Syndrome patients care. J. Korea Acad. Ind. Coop. Soc. 2017, 18, 185–196. [Google Scholar] [CrossRef]
- Im, S.B.; Baumann, S.L.; Ahn, M.N.; Kim, H.O.; Youn, B.H.; Park, M.K.; Lee, O.J. The experience of Korean nurses during the Middle East Respiratory Syndrome outbreak. Nurs. Sci. Q. 2018, 31, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.E.; Lee, E.S. A study on knowledge, attitude, infection management intention & educational needs of new respiratory infectious disease among nurses who unexperienced NRID (SARS & MERS). J. Korea Acad. Ind. Coop. Soc. 2019, 20, 721–731. [Google Scholar] [CrossRef]
- Kang, H.S.; Son, Y.D.; Chae, S.M.; Corte, C. Working experiences of nurses during the Middle East Respiratory Syndrome outbreak. Int. J. Nurs. Pract. 2018, 24, e12664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza-Junior, V.D.; Mendes, I.A.C.; Mazzo, A.; Godoy, S. Application of telenursing in nursing practice: An integrative literature review. Appl. Nurs. Res. 2016, 29, 254–260. [Google Scholar] [CrossRef]
- Jong, Y.K.; Kwan, I.L. Advantages and necessities of telehealth care service. Korean J. Med. 2020, 95, 217–227. [Google Scholar] [CrossRef]
- Kang, E.; Lee, S.Y.; Jung, H.; Kim, M.S.; Cho, B.; Kim, Y.S. Operating protocols of a community treatment center for isolation of patients with Coronavirus Disease, South Korea. J. Emerg. Infect. Dis. 2020, 26, 2329–2337. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. Available online: http://bokjiro.go.kr/nwel/welfareinfo/livwelnews/news/retireveIssueDetail.do?dataSid=6693695 (accessed on 17 November 2020).
- St George, I.; Cullen, M.; Gardiner, L.; Karabatsos, G. Universal telenursing triage in Australia and New Zealand—A new primary health service. Aust. Fam. Physician 2008, 37, 476–479. [Google Scholar] [PubMed]
- Rodríguez-Gázquez Mde, L.; Arredondo-Holguín, E.; Herrera-Cortés, R. Effectiveness of an educational program in nursing in the self-care of patients with heart failure: Randomized controlled trial. Rev. Lat. Am. Enferm. 2012, 20, 296–306. [Google Scholar] [CrossRef] [Green Version]
- Battaglia, C.; Benson, S.L.; Cook, P.F.; Prochazka, A. Building a tobacco cessation telehealth care management program for veterans with Posttraumatic Stress Disorder. J. Am. Psychiatr. Nurses Assoc. 2013, 19, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Vergara, J.; Parish, A.; Smallheer, B. Telehealth: Opportunities in geriatric patient care during COVID-19. Geriatr. Nurs. 2020, 41, 657–658. [Google Scholar] [CrossRef] [PubMed]
- Fisk, M.; Livingstone, A.; Pit, S.W. Telehealth in the context of COVID-19: Changing perspectives in Australia, the United Kingdom, and the United States. J. Med. Internet Res. 2020, 22, e19264. [Google Scholar] [CrossRef] [PubMed]
- Imlach, F.; McKinlay, E.; Middleton, L.; Kennedy, J.; Pledger, M.; Russell, L.; Churchward, M.; Cumming, J.; McBride-Henry, K. Telehealth consultations in general practice during a pandemic lockdown: Survey and interviews on patient experiences and preferences. BMC Fam. Pract. 2020, 21, 269. [Google Scholar] [CrossRef]
- Oh, E.G. Perspectives on nursing profession for a post-COVID-19 new normal. Korean J. Adult Nurs. 2020, 32, 221–222. [Google Scholar] [CrossRef]
- Schlachta-Fairchild, L.; Varghese, S.B.; Deickman, A.; Castelli, D. Telehealth and telenursing are live: APN policy and practice implications. J. Nurse Pract. 2010, 6, 98–106. [Google Scholar] [CrossRef]
- Taylor, J.; Coates, E.; Brewster, L.; Mountain, G.; Wessels, B.; Hawley, M.S. Examining the use of telehealth in community nursing: Identifying the factors affecting frontline staff acceptance and telehealth adoption. J. Adv. Nurs. 2015, 71, 326–337. [Google Scholar] [CrossRef] [Green Version]
- Martich, D. Telehealth Nursing: Tools and Strategies for Optimal Patient Care; Springer Publishing Company: New York, NY, USA, 2017; pp. 11–13. [Google Scholar]
- American Academy of Ambulatory Care Nursing. Scope and Standards of Practice for Professional Telehealth Nursing, 6th ed.; Anthony J. Jannetti, Inc.: Pitman, NJ, USA, 2018. [Google Scholar]
- American Nurses Association. Core Principles for Telehealth Nursing; American Nurses: Washington, DC, USA, 1999. [Google Scholar]
- Cho, M.S.; Lee, H.Y. Construction of telemedicine service model in home healthcare. Korean Public Health Res. 2017, 43, 81–101. [Google Scholar]
- Peine, A.; Paffenholz, P.; Martin, L.; Dohmen, S.; Marx, G.; Loosen, S.H. Telemedicine in Germany during the COVID-19 pandemic: Multi-professional national survey. J. Med. Internet Res. 2020, 22, e19745. [Google Scholar] [CrossRef]
- Montemurro, N. Will COVID-19 change neurosurgical clinical practice? Br. J. Neurosurg. 2020, 1, 1–2. [Google Scholar] [CrossRef]
- Montemurro, N. Intracranial hemorrhage and COVID-19, but please do not forget “old diseases” and elective surgery. Brain Behav. Immun. 2021, 92, 207–208. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.; Paprottka, F.; Escudero, R.; Casabona, G.; Montes, J.; Fakin, R.; Moke, L.; Stasch, T.; Richter, D.; Benito-Ruiz, J. Elective, non-urgent procedures and aesthetic surgery in the wake of SARS-COVID-19: Clinical management. Aesthet. Plast. Surg. 2020, 44, 1014–1042. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Question No. | Contents |
|---|---|
| Q 9 | Overall, how did you feel about the Community Treatment Center’s quarantine life? When you think that “you were very satisfied” with 5 points and “you are completely not satisfied” with 1 point, please indicate how satisfied you are. |
| Q 10 | Overall, were you comfortable and was it convenient living in isolation at the Community Treatment Center? When you think “it was very convenient” with 5 points and “completely uncomfortable” with 1 point, please indicate the degree of convenience you felt. |
| Q 19 | What did you think of the overall video consultation system? When you think that ‘you were very satisfied’ with 5 points and “you are completely not satisfied” with 1 point, please indicate how satisfied you are. |
| Q 20 | Was the overall video consultation system convenient? When you think “it was very convenient” with 5 points and 1 point for “completely uncomfortable”, please respond to the level of convenience you felt. |
| Q 21 | How did you feel about the self-monitoring service of vital signs (blood pressure, body temperature, etc.)? When you think that “you were very satisfied” with 5 points and “you are completely not satisfied” with 1 point, please indicate how satisfied you are. |
| Q 22 | Was the self-vital-sign monitoring service convenient? When you think that 5 points for very convenient cases and 1 point for completely uncomfortable cases, please respond to the level of convenience you felt. |
| Q 23 | What did you think of the video guide on how to measure vital signs at the time of admission? If you are very satisfied with 5 points and when you are not satisfied with 1 point, please answer the level of satisfaction you are satisfied with. |
| Q 24 | Was the video guide on how to measure vital signs convenient? When you think “very convenient” with 5 points and 1 point for completely uncomfortable cases, please respond to the level of convenience you felt. |
| Q 25 | How did you feel about the quality of the non-contact medical service via the video consultations you received? If you think that you are very satisfied with 5 points and when you are not satisfied with 1 point, please answer the level of satisfaction you are satisfied with. |
| Characteristic | Early Stage | Middle Stage | Final Stage |
|---|---|---|---|
| Method | Record by hand | Electronic documentation | Application |
| Transmission | Send questionnaire URL | Automatically send URL | Push alarm |
| Record | Check results, Input, and sign | Check results and sign | Check results and sign |
| Service Characteristic | Categories | Mean ± SD 1 |
|---|---|---|
| Overall quarantine life in SNUH community treatment center | Satisfaction (Q9) | 4.45 ± 0.65 |
| Convenience (Q10) | 4.54 ± 0.74 | |
| Video consultation system | Satisfaction (Q19) | 4.65 ± 0.59 |
| Convenience (Q20) | 4.62 ± 0.62 | |
| Self-measured vital signs monitoring | Satisfaction (Q21) | 4.52 ± 0.66 |
| Convenience (Q22) | 4.51 ± 0.68 | |
| Vital signs measurement video guide | Satisfaction (Q23) | 4.71 ± 0.64 |
| Convenience (Q24) | 4.72 ± 0.64 | |
| Video consultation quality (Q25) | 4.62 ± 0.67 |
| Characteristic | Categories | n (%) |
|---|---|---|
| Sex | Male | 54 (47.8) |
| Female | 59 (52.2) | |
| Age(years) (Mean ± SD) | 30.4 ± 12.9 | |
| Fever | At admission | 1 (0.9) |
| ≤3 days | 4 (3.5) | |
| ≤2 weeks | 15 (13.3) | |
| Never | 98 (86.7) | |
| Symptoms at admission | Cough | 31 (27.4) |
| Sputum | 25 (22.1) | |
| Rhinorrhea | 18 (15.9) | |
| Chest discomfort | 8 (7.1) | |
| Sore throat | 7 (6.2) | |
| Dyspnea | 5 (4.4) | |
| Underlying disease | Hypertension | 4 (3.5) |
| Diabetes | 1 (0.9) | |
| Asthma | 1 (0.9) | |
| Chronic bronchitis | 1 (0.9) | |
| None | 106 (93.8) |
| Q9 | Q10 | Q19 | Q20 | Q21 | Q22 | Q23 | Q24 | Q25 | |
|---|---|---|---|---|---|---|---|---|---|
| Q9 | 1 | 0.590 ** | 0.526 ** | 0.496 ** | 0.406 ** | 0.407 ** | 0.209 | 0.265 * | 0.360 ** |
| Q10 | 0.590 ** | 1 | 0.502 ** | 0.479 ** | 0.416 ** | 0.418 ** | 0.208 | 0.255 * | 0.267 * |
| Q19 | 0.526 ** | 0.502 ** | 1 | 0.882 ** | 0.667 ** | 0.669 ** | 0.389 ** | 0.444 ** | 0.709 ** |
| Q20 | 0.496 ** | 0.479 ** | 0.882 ** | 1 | 0.671 ** | 0.671 ** | 0.311 ** | 0.402 ** | 0.683 ** |
| Q21 | 0.406 ** | 0.416 ** | 0.667 ** | 0.671 ** | 1 | 0.885 ** | 0.364 ** | 0.383 ** | 0.726 ** |
| Q22 | 0.407 ** | 0.418 ** | 0.669 ** | 0.671 ** | 0.885 ** | 1 | 0.342 ** | 0.361 ** | 0.820 ** |
| Q23 | 0.209 | 0.208 | 0.389 ** | 0.311 ** | 0.364 ** | 0.342 ** | 1 | 0.947 ** | 0.359 ** |
| Q24 | 0.265 * | 0.255 * | 0.444 ** | 0.402 ** | 0.383 ** | 0.361 ** | 0.947 ** | 1 | 0.409 ** |
| Q25 | 0.360 ** | 0.267 * | 0.709 ** | 0.683 ** | 0.726 ** | 0.820 ** | 0.359 ** | 0.409 ** | 1 |
| B | SE | β | t | p | |
|---|---|---|---|---|---|
| Constant | 1.738 | 0.540 | 3.217 | 0.002 | |
| Q19 | 0.583 | 0.115 | 0.526 | 5.057 | 0.000 |
| R2 = 0.276; Adj R2 = 0.265; F = 25.574 (p = 0.000). | |||||
| B | SE 1 | β | t | p | |
|---|---|---|---|---|---|
| Constant | 1.612 | 0.621 | 2.594 | 0.012 | |
| Q19 | 0.629 | 0.132 | 0.502 | 4.746 | 0.000 |
| R2 = 0.252; Adj R2 = 0.240; F = 22.521 (p = 0.000). | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, H.; Lee, K.; Jung, E.; Lee, H. Developing the First Telenursing Service for COVID-19 Patients: The Experience of South Korea. Int. J. Environ. Res. Public Health 2021, 18, 6885. https://doi.org/10.3390/ijerph18136885
Heo H, Lee K, Jung E, Lee H. Developing the First Telenursing Service for COVID-19 Patients: The Experience of South Korea. International Journal of Environmental Research and Public Health. 2021; 18(13):6885. https://doi.org/10.3390/ijerph18136885
Chicago/Turabian StyleHeo, Hyunsook, Kyungyi Lee, Eunhee Jung, and Hyangyuol Lee. 2021. "Developing the First Telenursing Service for COVID-19 Patients: The Experience of South Korea" International Journal of Environmental Research and Public Health 18, no. 13: 6885. https://doi.org/10.3390/ijerph18136885