
Post-Vaccination SARS-CoV-2 Infections among Health Workers at the University Hospital of Verona, Italy: A Retrospective Cohort Survey

 , ,
, ,  , ,
, , 
 ,
,
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design, Setting, and Population
2.2. Vaccine Administration
2.3. SARS-CoV-2 Health Surveillance
2.4. Symptom Definition and Data Collection of Clinical Infection
2.5. Pre-Existing Medical Conditions
2.6. Outcomes and Endpoints
2.7. Statistical Analysis
3. Results
Sensitivity Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gruppo Italiano per la Medicina Basata sulle Evidenze (GIMBE). Available online: https://coronavirus.gimbe.org/ (accessed on 19 December 2021).
- World Health Organization (WHO). Available online: https://covid19.who.int/ (accessed on 19 December 2021).
- EPICENTRO. Available online: https://www.epicentro.iss.it/corona/www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sovirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_15-dicembre-2021.pdf (accessed on 19 December 2021).
- Istituto Superiore di Sanità (ISS). Available online: https://covid19.infn.it/iss/ (accessed on 19 December 2021).
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Presidenza del Consiglio dei Ministri. Available online: https://www.governo.it/it/cscovid19/report-vaccini/ (accessed on 19 December 2021).
- Russo, A.G.; Tunesi, S.; Consolazio, D.; Decarli, A.; Bergamaschi, W. Evaluation of the anti-COVID-19 vaccination campaign in the Metropolitan Area of Milan (Lombardy Region, Northern Italy). Valutazione della campagna vaccinale anti-COVID-19 nella ATS di Milano. Epidemiol. Prev. 2021, 45, 6. [Google Scholar] [CrossRef]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef]
- Calzetta, L.; Ritondo, B.L.; Coppola, A.; Matera, M.G.; Di Daniele, N.; Rogliani, P. Factors Influencing the Efficacy of COVID-19 Vaccines: A Quantitative Synthesis of Phase III Trials. Vaccines 2021, 9, 341. [Google Scholar] [CrossRef] [PubMed]
- Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M.; Butler, J.C. SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA Netw. Open. 2021, 4, e2035057. [Google Scholar] [CrossRef]
- Huff, H.V.; Singh, A. Asymptomatic Transmission During the Coronavirus Disease 2019 Pandemic and Implications for Public Health Strategies. Clin. Infect Dis. 2020, 71, 2752–2756. [Google Scholar] [CrossRef]
- Harder, T.; Koch, J.; Vygen-Bonnet, S.; Külper-Schiek, W.; Pilic, A.; Reda, S.; Scholz, S.; Wichmann, O. Efficacy and effectiveness of COVID-19 vaccines against SARS-CoV-2 infection: Interim results of a living systematic review, 1 January to 14 May 2021. Eurosurveillance 2021, 26, 2100563. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Rahman, M.M.; Miah, M.; Begum, M.N.; Sarmin, M.; Mahfuz, M.; Hossain, M.E.; Rahman, M.Z.; Chisti, M.J.; Ahmed, T. COVID-19 reinfections among naturally infected and vaccinated individuals. Sci. Rep. 2022, 12, 1438. [Google Scholar] [CrossRef]
- Malhotra, S.; Mani, K.; Lodha, R.; Bakhshi, S.; Mathur, V.P.; Gupta, P.; Kedia, S.; Sankar, J.; Kumar, P.; Kumar, A. SARS-CoV-2 Reinfection Rate and Estimated Effectiveness of the Inactivated Whole Virion Vaccine BBV152 Against Reinfection Among Health Care Workers in New Delhi, India. JAMA Netw Open. 2022, 5, e2142210. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Acuti Martellucci, C.; Soldato, G.; Carota, R.; Fazii, P.; Caponetti, A.; Manzoli, L. Rate of reinfections after SARS-CoV-2 primary infection in the population of an Italian province: A cohort study. J. Public Health 2021, 8, fdab346. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, A.M.; Spicer, K.B.; Thoroughman, D.; Glick, C.; Winter, K. Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination—Kentucky, May–June 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol Infect. 2022, 28, P202–P221. [Google Scholar] [CrossRef] [PubMed]
- Shastri, J.; Parikh, S.; Aggarwal, V.; Agrawal, S.; Chatterjee, N.; Shah, R.; Devi, P.; Mehta, P.; Pandey, R. Severe SARS-CoV-2 Breakthrough Reinfection with Delta Variant After Recovery from Breakthrough Infection by Alpha Variant in a Fully Vaccinated Health Worker. Front Med. 2021, 20, 737007. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.who.int/publications/m/item/enhancing-readiness-for-omicron-(b.1.1.529)-technical-brief-and-priority-actions-for-member-states (accessed on 1 February 2022).
- Khandia, R.; Singhal, S.; Alqahtani, T.; Kamal, M.A.; El-Shall, N.A.; Nainu, F.; Desingu, P.A.; Dhama, K. Emergence of SARS-CoV-2 Omicron (B.1.1.529) variant, salient features, high global health concerns and strategies to counter it amid ongoing COVID-19 pandemic. Environ. Res. 2022, 27, 112816. [Google Scholar] [CrossRef] [PubMed]
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Angel, Y.; Spitzer, A.; Henig, O.; Saiag, E.; Sprecher, E.; Padova, H.; Ben-Ami, R. Association Between Vaccination with BNT162b2 and Incidence of Symptomatic and Asymptomatic SARS-CoV-2 Infections Among Health Care Workers. JAMA J. Am. Med. Assoc. 2021, 325, 2457. [Google Scholar] [CrossRef] [PubMed]
- Bennson, S.; Oster, Y.; Cohen, M.J.; Nir-Paz, R. BNT162b2 mRNA COVID-19 Vaccine Effectiveness among Health Care Workers. N. Engl. J. Med. 2021, 384, 1775–1777. [Google Scholar] [CrossRef] [PubMed]
- Sansone, E.; Sala, E.; Tiraboschi, M.; Albini, E.; Lombardo, M.; Indelicato, A.; Rosati, C.; Boniotti, M.B.; Castelli, F.; De Palma, G. Effectiveness of BNT162b2 vaccine against SARS-CoV-2 among healthcare workers. Med. Lav. 2021, 112, 250–255. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Alishaq, M.; Nafady-Hego, H.; Jeremijenko, A.; Al Ajmi, J.A.; Elgendy, M.; Vinoy, S.; Fareh, S.B.; Plaatjies, J.V.; Nooh, M.; Alanzi, N.; et al. Risk factors for breakthrough SARS-CoV-2 infection in vaccinated healthcare workers. PLoS ONE 2021, 16, e0258820. [Google Scholar] [CrossRef]
- Chodick, G.; Tene, L.; Patalon, T.; Gazit, S.; Ben Tov, A.; Cohen, D.; Muhsen, K. Assessment of Effectiveness of 1 Dose of BNT162b2 Vaccine for SARS-CoV-2 Infection 13 to 24 Days After Immunization. JAMA Netw. Open 2021, 4, e2115985. [Google Scholar] [CrossRef] [PubMed]
- Scobie, H.M.; Johnson, A.G.; Suthar, A.B.; Severson, R.; Alden, N.B.; Balter, S.; Bertolino, D.; Blythe, D.; Brady, S.; Cadwell, B.; et al. Monitoring Incidence of COVID-19 Cases, Hospitalizations, and Deaths, by Vaccination Status—13 U.S. Jurisdictions, April 4–July 17, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Porru, S.; Carta, A.; Monaco, M.G.L.; Verlato, G.; Battaggia, A.; Parpaiola, M.; Lo Cascio, G.; Pegoraro, M.; Militello, V.; Moretti, F.; et al. Health Surveillance and Response to SARS-CoV-2 Mass Testing in Health Workers of a Large Italian Hospital in Verona, Veneto. Int. J. Environ. Res. Public Health 2020, 17, 5104. [Google Scholar] [CrossRef] [PubMed]
- Porru, S.; Monaco, M.G.L.; Carta, A.; Spiteri, G.; Parpaiola, M.; Battaggia, A.; Galligioni, G.; Ferrazzi, B.; Cascio, G.L.; Gibellini, D.; et al. SARS-CoV-2 Infection in Health Workers: Analysis from Verona SIEROEPID Study during the Pre-Vaccination Era. Int. J. Environ. Res. Public Health 2021, 18, 6446. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Available online: https://www.ema.europa.eu/en/documents/product-information/comirnaty-epar-product-information_en.pdf (accessed on 7 November 2021).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/vaccines/covid-19/index.html. (accessed on 7 September 2021).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html (accessed on 7 September 2021).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/media/releases/2021/p0607-mrna-reduce-risks.html (accessed on 7 September 2021).
- Istituto Superiore di Sanità. Interim Guidance on Measures for the Prevention and Control of SARS-CoV-2 Infections in Terms of Variants and Vaccination against COVID-19; Version of 13 March 2021; Rapporto ISS COVID-19 n. 4/2021 ; ISS Infection Prevention and Control Working Group: Rome, Italy, 2021; 14p. (In Italian) [Google Scholar]
- Filia, A.; Urdiales, A.M.; Rota, M.C. Guide to Contact tracing for COVID-19; Version of June 25, 2020; Rapporto ISS COVID-19, n. 53/2020; Istituto Superiore di Sanità: Rome, Italy, 2020. [Google Scholar]
- Società Italiana di Cure Palliative. MINISTERO DELLA SALUTE CIRCOLARE N. 18584 DEL 29 MAG 2020 RICERCA E GESTIONE DEI CONTATTI DI CASI COVID-19). Available online: https://www.sicp.it/normative/2020/06/ministero-della-salute-circolare-n-18584-del-29-mag-2020/ (accessed on 10 January 2022).
- Gazzetta Ufficiale. President of Italian Republic. Legislative Decree no. 44/2021 1st April 2021. Available online: https://www.gazzettaufficiale.it/eli/id/2021/04/01/21G00056/sg. (accessed on 31 January 2022).
- Gazzetta Ufficiale. President of Italian Republic. Legislative Decree no.122/2021 10th September 2021. Available online: https://www.gazzettaufficiale.it/eli/id/2021/09/10/21G00134/sg. (accessed on 31 January 2022).
- Gazzetta Ufficiale. President of Italian Republic. Legislative Decree no. 1/2022 7th January 2022. Available online: https://www.gazzettaufficiale.it/eli/id/2022/01/07/22G00002/sg. (accessed on 31 January 2022).
- Gazit, S.; Mizrahi, B.; Kalkstein, N.; Neuberger, A.; Peretz, A.; Mizrahi-Reuveni, M.; Ben-Tov, A.; Patalon, T. BNT162b2 mRNA Vaccine Effectiveness Given Confirmed Exposure: Analysis of Household Members of COVID-19 Patients. Clin. Infect Dis. 2021, ciab973. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, T.; Spencer, E.A.; Brassey, J.; Onakpoya, I.J.; Rosca, E.C.; Plüddemann, A.; Evans, D.H.; Conly, J.M.; Heneghan, C.J. Transmission of Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) from pre and asymptomatic infected individuals: A systematic review. Clinical Microbiol Infect. 2021, 28, P178–P189. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. The Proportion of SARS-CoV-2 Infections That Are Asymptomatic : A Systematic Review. Ann. Intern. Med. 2021, 174, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Gribben, C.; Bishop, J.; Hanlon, P.; Caldwell, D.; Wood, R.; Reid, M.; McMenamin, J.; Goldberg, D.; Stockton, D.; et al. Effect of Vaccination on Transmission of SARS-CoV-2. N. Engl. J. Med. 2021, 385, 1718–1720. [Google Scholar] [CrossRef]
- Harris, R.; Hall, J.; Zaidi, A.; Andrews, N.J.; Dunbar, J.K.; Dabrera, G. Impact of vaccination on household transmission of SARS-CoV-2 in England. N. Engl. J. Med. 2021, 385, 759–760. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. SIREN Study Group. COVID-19 vaccine coverage in healthcare workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Fabiani, M.; Ramigni, M.; Gobbetto, V.; Mateo-Urdiales, A.; Pezzotti, P.; Piovesan, C. Effectiveness of the Comirnaty (BNT162b2, BioNTech/Pfizer) vaccine in preventing SARS-CoV-2 infection among healthcare workers, Treviso province, Veneto region, Italy, 27 December 2020 to 24 March 2021. Eurosurveillance 2021, 26, 2100420. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Group A | Group B | Group C | Total | p-Value | |
|---|---|---|---|---|---|
| All | 1718 | 434 | 7659 | 9811 | |
| Sex | 0.294 | ||||
| Male | 513 (17.1) | 120 (4.0) | 2364 (78.9) | 2997 (100.0) | |
| Female | 1205 (17.7) | 314 (4.6) | 5295 (77.7) | 6814 (100.0) | |
| Age (median, p25–p75) | 31, 26–46 | 33.5, 26–51 | 37, 28–52 | <0.001 | |
| Job task | <0.001 | ||||
| Administrative | 184 (22.2) | 32 (3.9) | 612 (73.9) | 828 (100.0) | |
| Physician | 461 (16.9) | 84 (3.1) | 2182 (80.0) | 2727 (100.0) | |
| Nurse | 368 (14.9) | 115 (4.7) | 1980 (80.4) | 2463 (100.0) | |
| Other health professionals | 705 (18.6) | 203 (5.4) | 2885 (76.1) | 3793 (100.0) |
| Positive (n = 177) | Negative (n = 9634) | p-Value | |
|---|---|---|---|
| Sex | 0.139 | ||
| Men | 45 (25.4) | 2952 (30.6) | |
| Women | 132 (74.6) | 6682 (69.4) | |
| Age (median, p25–p75) | 47, 35–55 | 35, 27–51 | <0.001 |
| Job task | <0.001 | ||
| Administrative | 12 (6.8) | 816 (8.5) | |
| Physician | 36 (20.3) | 2691 (27.9) | |
| Nurse | 70 (39.5) | 2393 (24.8) | |
| Other health professional | 59 (33.3) | 3734 (38.8) | |
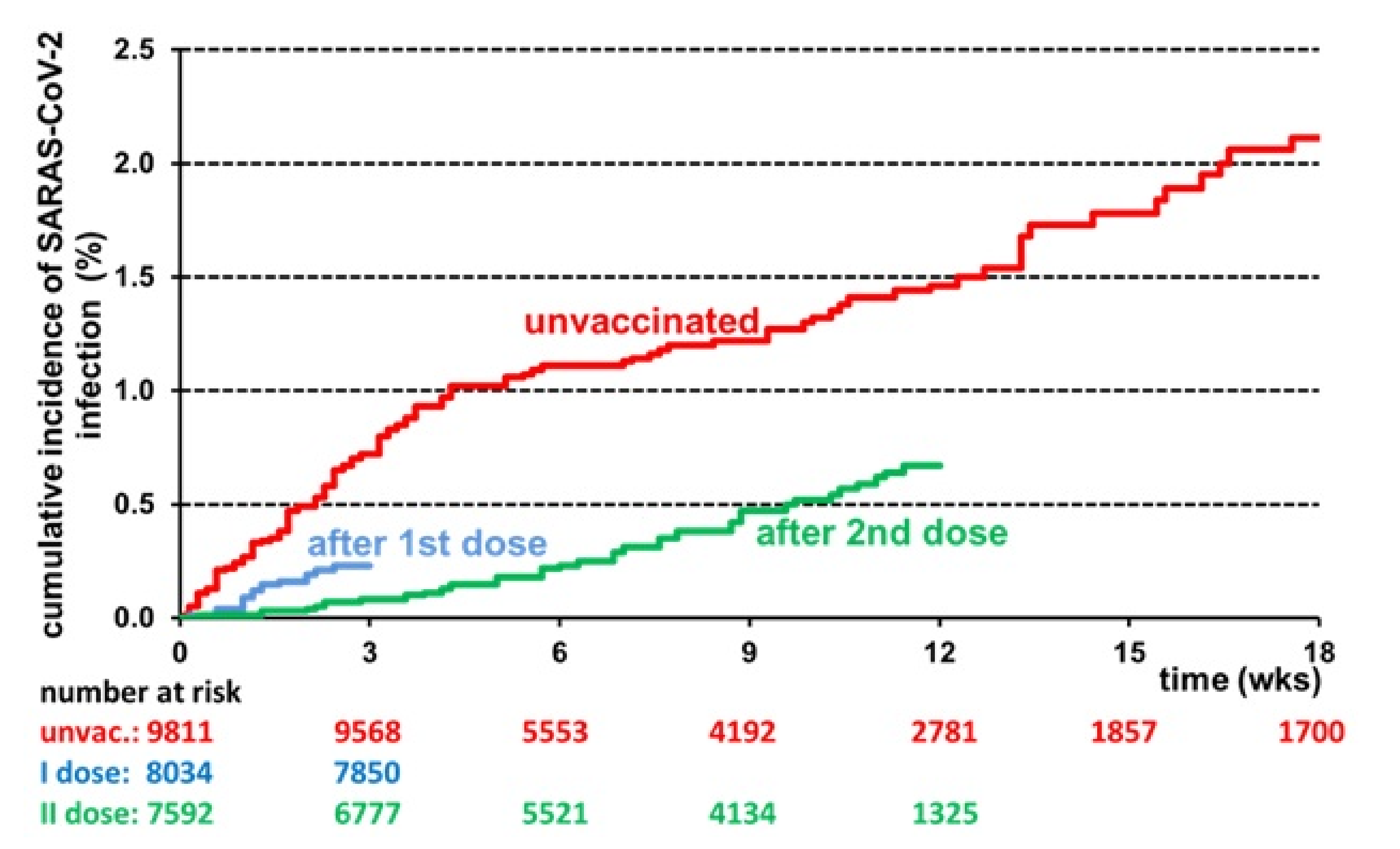
| Vaccination | <0.001 | ||
| None | 77 (43.5) | 1641 (17.0) | |
| 1st dose | 45 (25.4) | 389 (4.0) | |
| 2nd dose | 55 (31.1) | 7604 (78.9) |
| Group A (n = 114) | Group B (n = 17) | Group C (n = 34) | p Value | |
|---|---|---|---|---|
| Infection setting | 0.064 | |||
| Work | 60 (53) | 7 (41) | 9 (26) | |
| Family | 24 (21) | 3 (18) | 9 (26) | |
| Unknown | 30 (26) | 7 (41) | 16 (47) | |
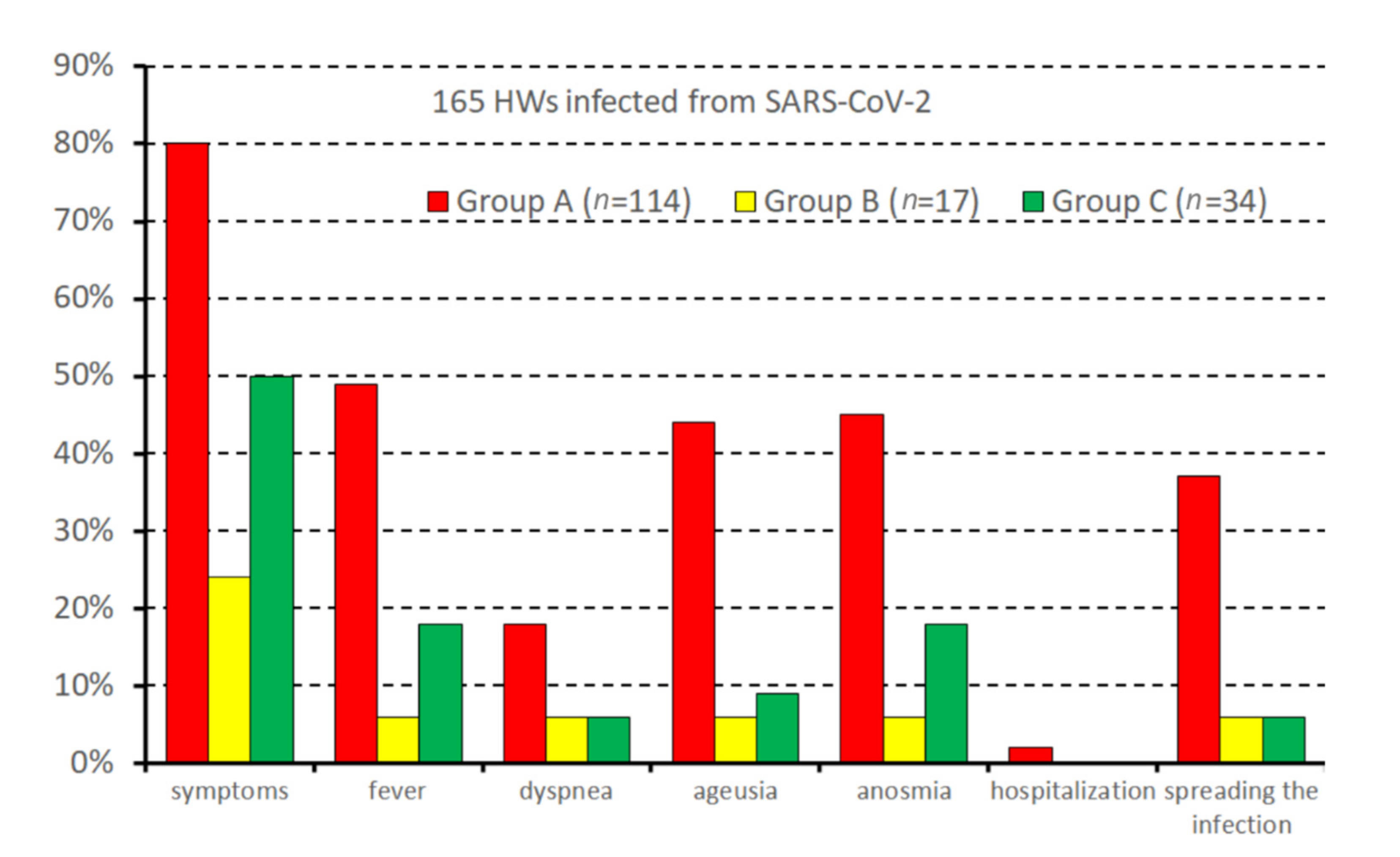
| Infection spreading | 42 (37) | 1 (6) | 2 (6) | <0.001 |
| COVID-19 | ||||
| Symptoms | 91 (80) | 4 (24) | 17 (50) | <0.001 |
| Fever | 56 (49) | 1 (6) | 6 (18) | <0.001 |
| Dyspnoea | 21 (18) | 1 (6) | 2 (6) | 0.126 |
| Ageusia | 50 (44) | 1 (6) | 3 (9) | <0.001 |
| Anosmia | 51 (45) | 1 (6) | 6 (18) | <0.001 |
| Hospitalization | 2 (2) | 0 | 0 | 1.000 |
| Hazard Ratio (95% CI) | p Value | |
|---|---|---|
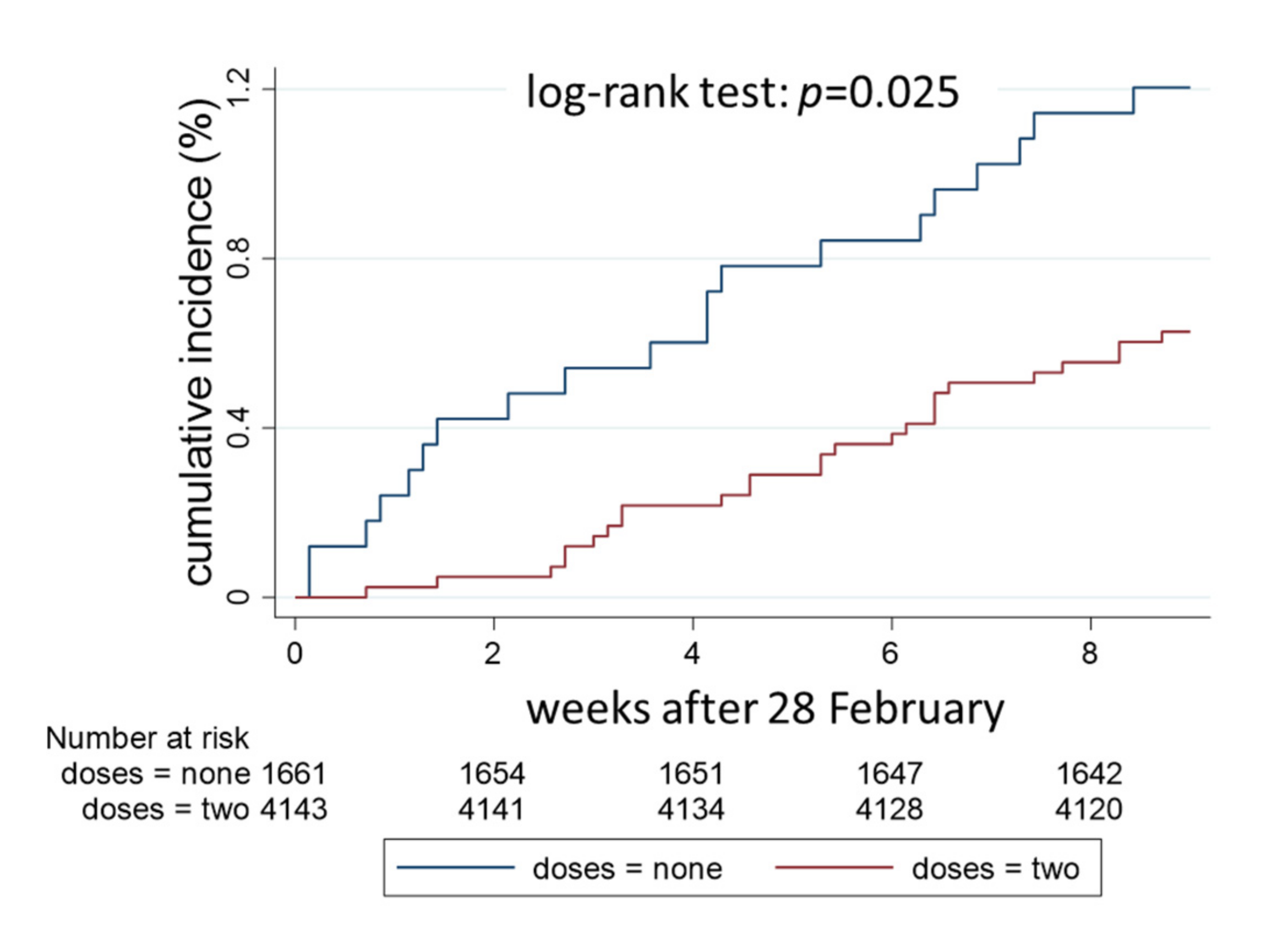
| Fully vaccinated vs. unvaccinated | 0.37 (0.20–0.69) | 0.002 |
| Gender (women vs. men) | 0.87 (0.46–1.67) | 0.682 |
| Age (per 10-year increase) | 1.61 (1.27–2.04) | <0.001 |
| Job task | ||
| Administrative | 1 (reference) | |
| Physician | 1.62 (0.43–6.11) | 0.474 |
| Nurse | 2.13 (0.60–7.65) | 0.245 |
| Other health professional | 2.46 (0.71–8.51) | 0.154 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porru, S.; Spiteri, G.; Monaco, M.G.L.; Valotti, A.; Carta, A.; Lotti, V.; Diani, E.; Lippi, G.; Gibellini, D.; Verlato, G. Post-Vaccination SARS-CoV-2 Infections among Health Workers at the University Hospital of Verona, Italy: A Retrospective Cohort Survey. Vaccines 2022, 10, 272. https://doi.org/10.3390/vaccines10020272
Porru S, Spiteri G, Monaco MGL, Valotti A, Carta A, Lotti V, Diani E, Lippi G, Gibellini D, Verlato G. Post-Vaccination SARS-CoV-2 Infections among Health Workers at the University Hospital of Verona, Italy: A Retrospective Cohort Survey. Vaccines. 2022; 10(2):272. https://doi.org/10.3390/vaccines10020272
Chicago/Turabian StylePorru, Stefano, Gianluca Spiteri, Maria Grazia Lourdes Monaco, Alessandro Valotti, Angela Carta, Virginia Lotti, Erica Diani, Giuseppe Lippi, Davide Gibellini, and Giuseppe Verlato. 2022. "Post-Vaccination SARS-CoV-2 Infections among Health Workers at the University Hospital of Verona, Italy: A Retrospective Cohort Survey" Vaccines 10, no. 2: 272. https://doi.org/10.3390/vaccines10020272