
Associations between the Severity of the Post-Acute COVID-19 Syndrome and Echocardiographic Abnormalities in Previously Healthy Outpatients Following Infection with SARS-CoV-2

 ,
,  , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 31 January 2021).
- del Rio, C.; Collins, L.F.; Malani, P. Long-term health consequences of COVID-19. JAMA 2020, 324, 1723. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute Covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- Gandhi, R.T.; Lynch, J.B.; del Rio, C. Mild or moderate Covid-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- de Graaf, M.A.; Antoni, M.L.; ter Kuile, M.M.; Arbous, M.S.; Duinisveld, A.J.F.; Feltkamp, M.C.W.; Groeneveld, G.H.; Hinnen, S.C.H.; Janssen, V.R.; Lijfering, W.M.; et al. Short-term outpatient follow-up of COVID-19 patients: A multidisciplinary approach. EClinicalMedicine 2021, 32, 100731. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F. Gemelli against COVID-19 post-acute care study group persistent symptoms in patients after acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- ESC. ESC Guidance for the Diagnosis and Management of CV Disease During the COVID-19 Pandemic. Available online: https://www.escardio.org/Education/COVID-19-and-Cardiology/ESC-COVID-19-Guidance (accessed on 30 January 2021).
- Klok, F.A.; Boon, G.J.A.M.; Barco, S.; Endres, M.; Geelhoed, J.J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The post-COVID-19 functional status (PCFS) scale: A tool to measure functional status over time after COVID-19. Eur. Respir. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Machado, F.V.C.; Meys, R.; Delbressine, J.M.; Vaes, A.W.; Goërtz, Y.M.J.; van Herck, M.; Houben-Wilke, S.; Boon, G.J.A.M.; Barco, S.; Burtin, C.; et al. Construct validity of the post-COVID-19 functional status scale in adult subjects with COVID-19. Health Qual. Life Outcomes 2021, 19, 40. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B.K.; et al. The role of chest imaging in patient management during the COVID-19 pandemic: A multinational consensus statement from the fleischner society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [Green Version]
- EuroQol. EQ-5D User Guides—EQ-5D. Available online: www.euroqol.org (accessed on 10 January 2021).
- Algahtani, F.D.; Hassan, S.-U.-N.; Alsaif, B.; Zrieq, R. Assessment of the quality of life during COVID-19 pandemic: A cross-sectional survey from the Kingdom of Saudi Arabia. Int. J. Environ. Res. Public. Health 2021, 18, 847. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American society of echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European society of cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.C.; Marino, P.N.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2009, 22, 107–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry task force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Baycan, O.F.; Barman, H.A.; Atici, A.; Tatlisu, A.; Bolen, F.; Ergen, P.; Icten, S.; Gungor, B.; Caliskan, M. Evaluation of biventricular function in patients with COVID-19 using speckle tracking echocardiography. Int. J. Cardiovasc. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Croft, L.B.; Krishnamoorthy, P.; Ro, R.; Anastasius, M.; Zhao, W.; Buckley, S.; Goldman, M.; Argulian, E.; Sharma, S.K.; Kini, A.; et al. Abnormal left ventricular global longitudinal strain by speckle tracking echocardiography in COVID-19 patients. Future Cardiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Argulian, E.; Sud, K.; Vogel, B.; Bohra, C.; Garg, V.P.; Talebi, S.; Lerakis, S.; Narula, J. Right ventricular dilation in hospitalized patients with COVID-19 infection. JACC Cardiovasc. Imaging 2020, 13, 2459–2461. [Google Scholar] [CrossRef] [PubMed]
- Gemelli Against COVID-19 Post-Acute Care Study Group. Post-COVID-19 global health strategies: The need for an interdisciplinary approach. Aging Clin. Exp. Res. 2020, 32, 1613–1620. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of cardiac manifestations in COVID-19: A systematic echocardiographic study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.; Prokup, J.A.; Butson, K.; Jordan, K. Acute effusive pericarditis: A late complication of COVID-19. Cureus 2020, 12, e9074. [Google Scholar] [CrossRef]
- Singh, S.; Jain, A.; Chaudhari, P.; Malik, F.A.; Desai, V.; Abu Hassan, F.; Shah, V.; Patel, V.; Desai, R. Pericardial complications in patients with COVID-19: A systematic review of published cases. Circulation 2020, 142, A16344. [Google Scholar] [CrossRef]
- SeyedAhmad, S.; Maryam, G.; Mehrnaz, A.G.; Fereshteh, G. Constrictive pericarditis associated with coronavirus disease 2019 (COVID-19): A case report. Infect. Disord. Drug Targets 1969, 20, 1–3. [Google Scholar]
- Tenforde, M.W. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network—United States, March–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69. [Google Scholar] [CrossRef] [PubMed]
- Simonelli, C.; Paneroni, M.; Fokom, A.G.; Saleri, M.; Speltoni, I.; Favero, I.; Garofali, F.; Scalvini, S.; Vitacca, M. How the COVID-19 infection tsunami revolutionized the work of respiratory physiotherapists: An experience from Northern Italy. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, M.; Garofano, M.; Palumbo, R.; Di Pietro, P.; Izzo, C.; Damato, A.; Venturini, E.; Iesu, S.; Virtuoso, N.; Strianese, A.; et al. Exercise training and cardiac rehabilitation in COVID-19 patients with cardiovascular complications: State of art. Life 2021, 11, 259. [Google Scholar] [CrossRef] [PubMed]
- Tozato, C.; Ferreira, B.F.C.; Dalavina, J.P.; Molinari, C.V.; dos Alves, V.L.S. Cardiopulmonary rehabilitation in post-COVID-19 patients: Case series. Rev. Bras. Ter. Intensiva 2021, 33, 167–171. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics of Patients | Without Significant Cardiac Abnormalities 112 (74.66%) | With Cardiac Abnormalities 38 (25.33%) | p | |
|---|---|---|---|---|
| Age (years) | 39.52 (31–46.75) | 48.86 (46.75–53.25) | <0.001 a | |
| Gender | male 63 | 48 | 15 | 0.715 b |
| female 87 | 64 | 23 | ||
| BMI kg/m2 | 26.63 (23.53–29.41) | 30.48 (28.34–32.77) | <0.001 a | |
| Severity form: | mild | 110 | 1 | <0.001 c |
| moderate | 2 | 37 | ||
| O2 saturation during COVID-19% | 97.55 (97–99) | 94.73 (94–96) | <0.001 a | |
| TCT assessed injury (%) | 0 (0–0) | 30.5 (30–35) | <0.001 a | |
| Initial CRP (mg/dL) | 22.1 (18.54–29) | 36.58 (31–41.75) | <0.001 a | |
| Heart rate (b/min) | 73 (70–80) | 75 (75–80) | 0.126 a | |
| No. of persisting symptoms | 2.59 (2–3) | 4.47 (3–6) | <0.001 a | |
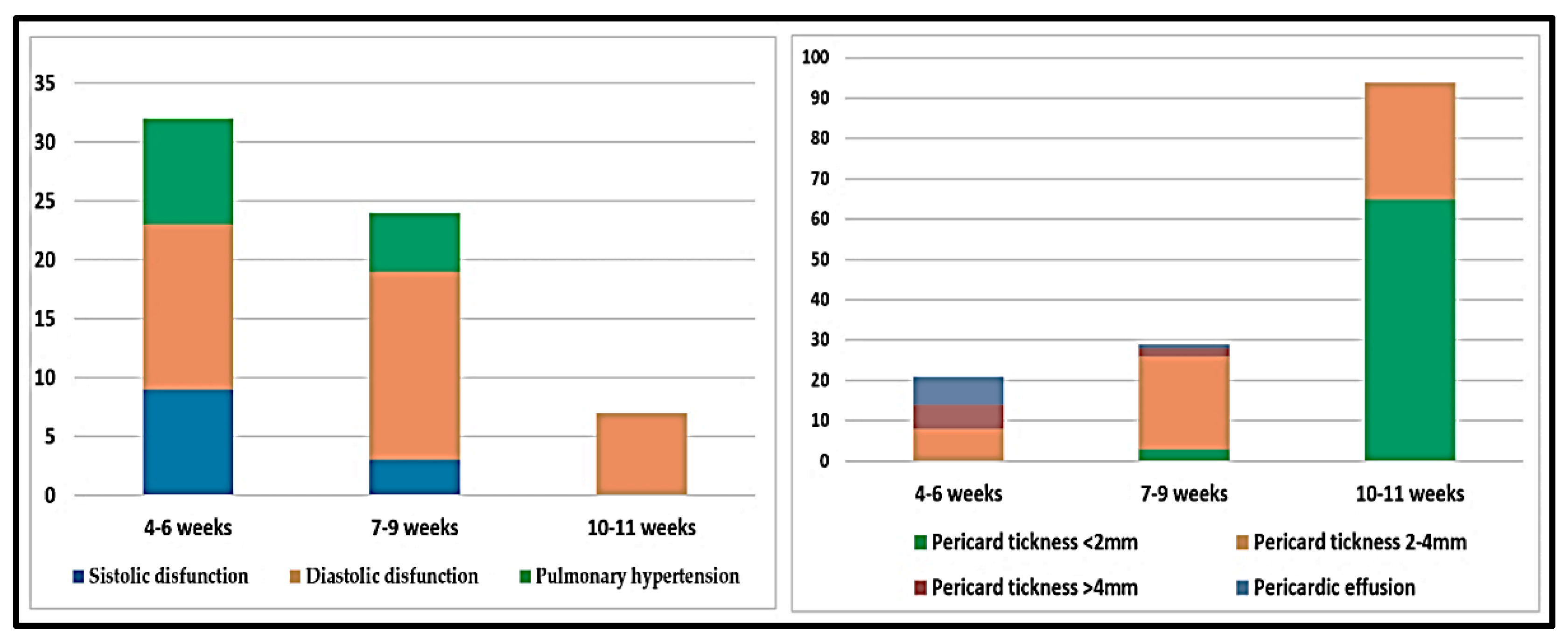
| Weeks since COVID-19 | 10.08 (10–11) | 7.44 (5.75–9) | <0.001 a | |
| PCFS score | 1 (1–1) | 2 (2–3) | <0.001 a | |
| Quality of life—VAS score | 76.28 (70–82) | 62 (55–69) | <0.001 a | |
| Echocardiographic parameters | ||||
| Pericardial abnormalities | ||||
| Thickness | 1.5 (1.42–2.3) | 3.57 (2–5.1) | <0.001 a | |
| Exudate | - | 8 | 0.004 c | |
| LVMI | 86.84 (75.53–96.2) | 105 (97.27–114.73) | <0.001 a | |
| LAVI | 17.42 (13.45–20.16) | 30.19 (27.91–34.56) | <0.001 a | |
| E/A | 1.15 (0.96–1.33) | 1.19 (0.75–1.32) | 0.216 a | |
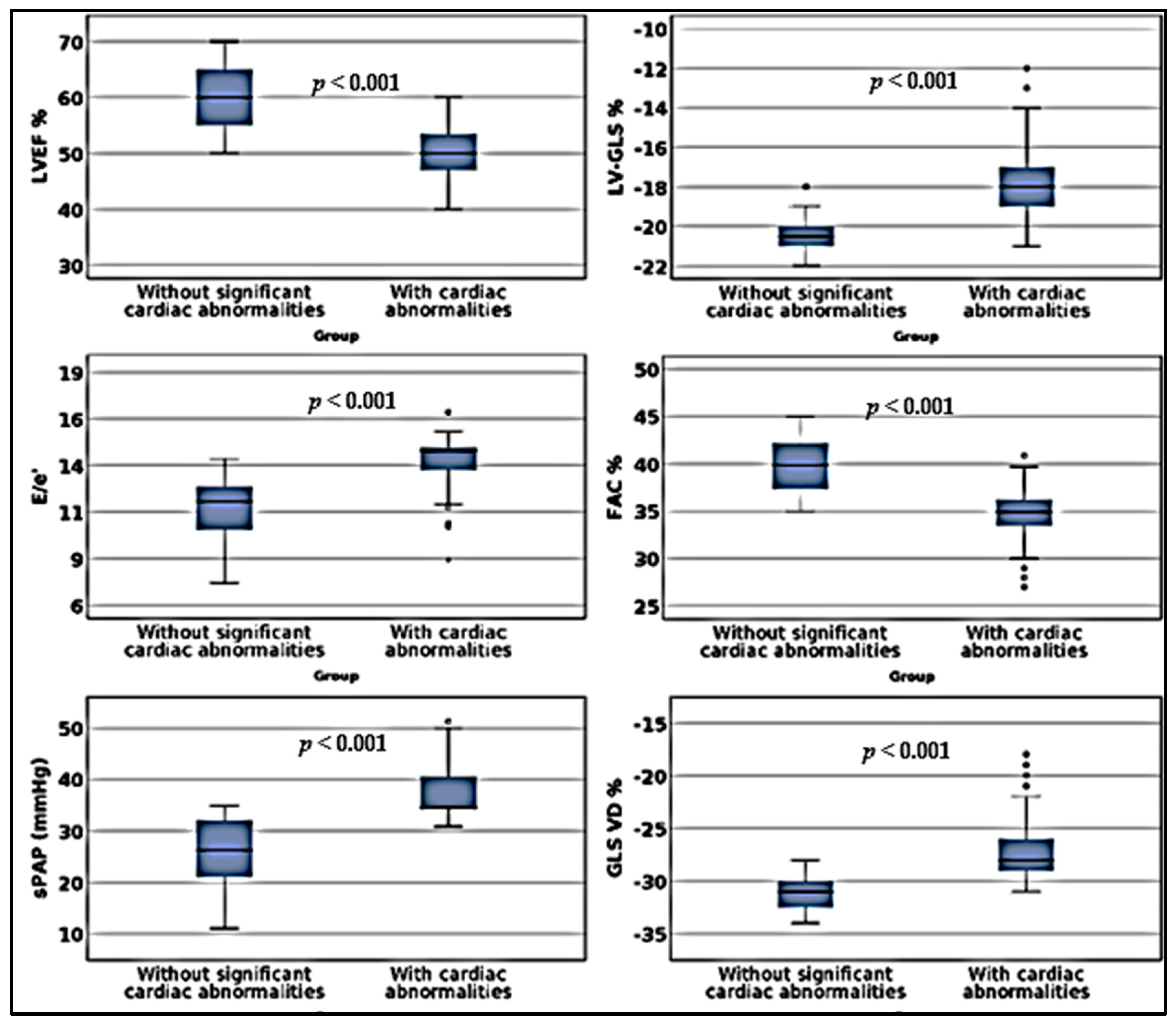
| E/e′ | 11.15 (10–12.36) | 13.63 (13.21–14.49) | <0.001 a | |
| TRV | 2.26 (2–2.6) | 2.84 (2.7–2.98) | <0.001 a | |
| sPAP | 26.11 (21–32) | 37.5 (34.16–40.64) | <0.001 a | |
| TAPSE | 23.35 (21.25–25) | 18.34 (15.75–20) | <0.001 a | |
| FAC | 39.68 (37.34–42.21) | 34.38 (33.17–36.23) | <0.001 a | |
| RV-GLS | −30.9 (−32.75–−30) | −17.741 (−19–−17) | <0.001 a | |
| MAPSE | 16.23 (15–18) | 12.33 (8.75–15.62) | <0.001 a | |
| LVEF | 60 (55–65) | 50.48 (47–53.62) | <0.001 a | |
| LV-GLS | −20.43 (−21–−20) | −26.55 (−29–−25.75) | <0.001 a | |
| Analyzed Parameters | No. of Remaining Symptoms | Quality of Life | ||||
|---|---|---|---|---|---|---|
| r | 95%CI | p | r | 95%CI | p | |
| Initial TCT injury | 0.664 | 0.548; 0.751 | <0.001 | −0.670 | −0.751; −0.567 | <0.001 |
| Initial CRP | 0.709 | 0.609; 0.788 | <0.001 | −0.761 | −0.832; −0.667 | <0.001 |
| PCFS score | 0.775 | 0.701; 0.837 | <0.001 | −0.758 | −0.817; −0.681 | <0.001 |
| Weeks since COVID-19 | −0.856 | −0.898; −0.796 | <0.001 | 0.847 | 0.783; 0.896 | <0.001 |
| LVEF | −0.553 | −0.671; −0.433 | <0.001 | 0.687 | 0.587; 0.77 | <0.001 |
| LV-GLS | 0.606 | 0.49; 0.707 | <0.001 | −0.687 | −0.77; −0.592 | <0.001 |
| MAPSE | −0.433 | −0.574; −0.285 | <0.001 | 0.537 | 0.407; 0.654 | <0.001 |
| FAC | −0.78 | −0.838; −0.707 | <0.001 | 0.831 | 0.758; 0.883 | <0.001 |
| RV-GLS | 0.816 | 0.53; 0.865 | <0.001 | −0.895 | −0.931; −0.844 | <0.001 |
| TAPSE | −0.671 | −0.775; −0.554 | <0.001 | 0.725 | 0.626; 0.805 | <0.001 |
| sPAPs | 0.791 | 0.726; −0.837 | <0.001 | −0.843 | −0.885; −0.777 | <0.001 |
| E/e′ | 0.470 | 0.326; 0.587 | <0.001 | −0.562 | −0.668; −0.420 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tudoran, C.; Tudoran, M.; Pop, G.N.; Giurgi-Oncu, C.; Cut, T.G.; Lazureanu, V.E.; Oancea, C.; Parv, F.; Ciocarlie, T.; Bende, F. Associations between the Severity of the Post-Acute COVID-19 Syndrome and Echocardiographic Abnormalities in Previously Healthy Outpatients Following Infection with SARS-CoV-2. Biology 2021, 10, 469. https://doi.org/10.3390/biology10060469
Tudoran C, Tudoran M, Pop GN, Giurgi-Oncu C, Cut TG, Lazureanu VE, Oancea C, Parv F, Ciocarlie T, Bende F. Associations between the Severity of the Post-Acute COVID-19 Syndrome and Echocardiographic Abnormalities in Previously Healthy Outpatients Following Infection with SARS-CoV-2. Biology. 2021; 10(6):469. https://doi.org/10.3390/biology10060469
Chicago/Turabian StyleTudoran, Cristina, Mariana Tudoran, Gheorghe Nicusor Pop, Catalina Giurgi-Oncu, Talida Georgiana Cut, Voichita Elena Lazureanu, Cristian Oancea, Florina Parv, Tudor Ciocarlie, and Felix Bende. 2021. "Associations between the Severity of the Post-Acute COVID-19 Syndrome and Echocardiographic Abnormalities in Previously Healthy Outpatients Following Infection with SARS-CoV-2" Biology 10, no. 6: 469. https://doi.org/10.3390/biology10060469