
EASIX, Modified EASIX and Simplified EASIX as an Early Predictor for Intensive Care Unit Admission and Mortality in Severe COVID-19 Patients


Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bermejo-Martin, J.F.; Almansa, R.; Torres, A.; Gonzalez-Rivera, M.; Kelvin, D.J. COVID-19 as a Cardiovascular Disease: The Potential Role of Chronic Endothelial Dysfunction. Cardiovasc. Res. 2020, 116, E132–E133. Available online: https://pubmed.ncbi.nlm.nih.gov/32420587/ (accessed on 18 January 2020). [CrossRef]
- Yazan Abou-Ismail, M.; Diamond, A.; Kapoor, S.; Arafah, Y.; Nayak, L. The Hypercoagulable State in COVID-19: Incidence, Pathophysiology, and Management. Thromb. Res. 2020, 194, 101–115. [Google Scholar] [CrossRef]
- Liang, W.H.; Guan, W.J.; Li, C.C.; Li, Y.M.; Liang, H.R.; Zhao, Y.; Liu, X.Q.; Sang, L.; Chen, R.C.; Tang, C.L.; et al. Clinical Characteristics and Outcomes of Hospitalised Patients with COVID-19 Treated in Hubei (Epicentre) and Outside Hubei (non-epicentre): A Nationwide Analysis of China. Eur. Respir. J. 2020, 55, 6. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7144336/ (accessed on 7 February 2020). [CrossRef] [Green Version]
- Feng, X.; Li, P.; Ma, L.; Liang, H.; Lei, J.; Li, W.; Wang, K.; Song, Y.; Li, S.; Yang, W.; et al. Clinical Characteristics and Short-Term Outcomes of Severe Patients with COVID-19 in Wuhan, China. Front. Med. 2020, 7, 491. [Google Scholar] [CrossRef]
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Li, Y.; Ashcroft, T.; Chung, A.; Dighero, I.; Dozier, M.; Horne, M.; McSwiggan, E.; Shamsuddin, A.; Nair, H. Risk factors for poor outcomes in hospitalised COVID-19 patients: A systematic review and meta-analysis. J. Glob. Health 2021, 11, 10001. [Google Scholar] [CrossRef]
- Alqahtani, J.S.; Oyelade, T.; Aldhahir, A.M.; Alghamdi, S.M.; Almehmadi, M.; Alqahtani, A.S.; Quaderi, S.; Mandal, S.; Hurst, J.R. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: A rapid systematic review and meta-analysis. PLoS ONE 2020, 15, e0233147. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. Available online: https://pubmed.ncbi.nlm.nih.gov/31986264/ (accessed on 17 January 2022). [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. Available online: https://pubmed.ncbi.nlm.nih.gov/32171076/ (accessed on 17 January 2022). [CrossRef]
- Kompaniyets, L.; Pennington, A.F.; Goodman, A.B.; Rosenblum, H.G.; Belay, B.; Ko, J.Y.; Chevinsky, J.R.; Schieber, L.Z.; Summers, A.D.; Lavery, A.M.; et al. Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized with COVID-19, March 2020–March 2021. Prev. Chronic Dis. 2021, 18, E66. [Google Scholar] [CrossRef]
- Rorat, M.; Zińczuk, A.; Szymański, W.; Simon, K.; Guziński, M. Usefulness of a portable chest radiograph in the initial diagnosis of coronavirus disease 2019. Pol. Arch. Int. Med. 2020, 130, 906–909. Available online: https://pubmed.ncbi.nlm.nih.gov/32666780/ (accessed on 7 February 2022).
- Rorat, M.; Jurek, T.; Simon, K.; Guzinski, M. Value of quantitative analysis in lung computed tomography in patients severely ill with COVID-19. PLoS ONE 2021, 16, e0251946. Available online: https://pubmed.ncbi.nlm.nih.gov/34015025/ (accessed on 7 February 2022). [CrossRef]
- Salvatore, C.; Roberta, F.; Angela, D.L.; Cesare, P.; Alfredo, C.; Giuliano, G.; Giulio, L.; Giuliana, G.; Maria, R.G.; Paola, B.M.; et al. Clinical and laboratory data, radiological structured report findings and quantitative evaluation of lung involvement on baseline chest CT in COVID-19 patients to predict prognosis. Radiol. Med. 2021, 126, 29–39. Available online: https://pubmed.ncbi.nlm.nih.gov/33047295/ (accessed on 7 February 2022). [CrossRef]
- Iba, T.; Connors, J.M.; Levy, J.H. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm. Res. 2020, 69, 1181–1189. [Google Scholar] [CrossRef]
- Kalicińska, E.; Szymczak, D.; Zińczuk, A.; Adamik, B.; Smiechowicz, J.; Skalec, T.; Nowicka-Suszko, D.; Biernat, M.; Bogucka-Fedorczuk, A.; Rybka, J.; et al. Immunosuppression as a hallmark of critical covid-19: Prospective study. Cells 2021, 10, 1293. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Levy, J.H.; Iba, T.; Olson, L.B.; Corey, K.M.; Ghadimi, K.; Connors, J.M. COVID-19: Thrombosis, thromboinflammation, and anticoagulation considerations. Int. J. Lab. Hematol. 2021, 43, 29–35. [Google Scholar] [CrossRef]
- Ghahramani, S.; Tabrizi, R.; Lankarani, K.B.; Kashani, S.M.A.; Rezaei, S.; Zeidi, N.; Akbari, M.; Heydari, S.T.; Akbari, H.; Nowrouzi-Sohrabi, P.; et al. Laboratory features of severe vs. non-severe COVID-19 patients in Asian populations: A systematic review and meta-analysis. Eur. J. Med. Res. 2020, 25, 30. [Google Scholar] [CrossRef]
- Garcia PD, W.; Fumeaux, T.; Guerci, P.; Heuberger, D.M.; Montomoli, J.; Roche-Campo, F.; Wong, J. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort. EClin. Med. 2020, 25, 100449. [Google Scholar]
- Smadja, D.M.; Guerin, C.L.; Chocron, R.; Yatim, N.; Boussier, J.; Gendron, N.; Khider, L.; Hadjadj, J.; Goudot, G.; Debuc, B.; et al. Angiopoietin-2 as a marker of endothelial activation is a good predictor factor for intensive care unit admission of COVID-19 patients. Angiogenesis 2020, 23, 611–620. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7262337/ (accessed on 18 January 2022). [CrossRef] [Green Version]
- Gavriilaki, E.; Anyfanti, P.; Gavriilaki, M.; Lazaridis, A.; Douma, S.; Gkaliagkousi, E. Endothelial Dysfunction in COVID-19: Lessons Learned from Coronaviruses. Curr. Hypertens. Rep. 2020, 22, 63. Available online: https://pubmed.ncbi.nlm.nih.gov/32852642/ (accessed on 18 January 2022). [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Luft, T.; Benner, A.; Terzer, T.; Jodele, S.; Dandoy, C.E.; Storb, R.; Kordelas, L.; Beelen, D.; Gooley, T.; Sandmaier, B.M.; et al. EASIX and mortality after allogeneic stem cell transplantation. Bone Marrow Transpl. 2020, 55, 553–561. Available online: https://pubmed.ncbi.nlm.nih.gov/31558788/ (accessed on 17 January 2022). [CrossRef]
- Luft, T.; Benner, A.; Jodele, S.; Dandoy, C.E.; Storb, R.; Gooley, T.; Sandmaier, B.M.; Becker, N.; Radujkovic, A.; Dreger, P.; et al. EASIX in patients with acute graft-versus-host disease: A retrospective cohort analysis. Lancet Haematol 2017, 4, e414–e423. Available online: https://pubmed-1ncbi-1nlm-1nih-1gov-1yxc2mlpl150f.han.bg.umed.wroc.pl/28733186/ (accessed on 17 January 2022). [CrossRef]
- Luft, T.; Wendtner, C.M.; Kosely, F.; Radujkovic, A.; Benner, A.; Korell, F.; Kihm, L.; Bauer, M.F.; Dreger, P.; Merle, U. EASIX for Prediction of Outcome in Hospitalized SARS-CoV-2 Infected Patients. Front. Immunol. 2021, 12, 2425. [Google Scholar] [CrossRef]
- Kalicińska, E.; Biernat, M.; Rybka, J.; Zińczuk, A.; Janocha-Litwin, J.; Rosiek-Biegus, M.; Morawska, M.; Waszczuk-Gajda, A.; Drozd-Sokołowska, J.; Szukalski, Ł.; et al. Endothelial Activation and Stress Index (EASIX) as an Early Predictor for Mortality and Overall Survival in Hematological and Non-Hematological Patients with COVID-19: Multicenter Cohort Study. J. Clin. Med. 2021, 10, 4373. [Google Scholar] [CrossRef]
- Pérez-García, F.; Bailén, R.; Torres-Macho, J.; Fernández-Rodríguez, A.; Jiménez-Sousa, M.Á.; Jiménez, E.; Pérez-Butragueño, M.; Cuadros-González, J.; Cadiñanos, J.; García-García, I.; et al. Age-Adjusted Endothelial Activation and Stress Index for Coronavirus Disease 2019 at Admission Is a Reliable Predictor for 28-Day Mortality in Hospitalized Patients with Coronavirus Disease 2019. Front. Med. 2021, 8, 1445. [Google Scholar] [CrossRef]
- WHO: Clinical management of COVID-19; Interim Guidance 27 May 2020, Geneva, World Health Organization. Technical Documents. Available online: https://apps.who.int/iris/handle/10665/332196 (accessed on 11 November 2021).
- Pennisi, M.; Sanchez-Escamilla, M.; Flynn, J.R.; Shouval, R.; Alarcon Tomas, A.; Silverberg, M.L.; Batlevi, C.; Brentjens, R.J.; Dahi, P.B.; Devlin, S.M.; et al. Modified EASIX predicts severe cytokine release syndrome and neurotoxicity after chimeric antigen receptor T cells. Blood Adv. 2021, 5, 3397–3406. Available online: https://pubmed.ncbi.nlm.nih.gov/34432870/ (accessed on 18 January 2022). [CrossRef]
- Greenbaum, U.; Strati, P.; Saliba, R.M.; Torres, J.; Rondon, G.; Nieto, Y.; Hosing, C.; Srour, S.A.; Westin, J.; Fayad, L.E.; et al. CRP and ferritin in addition to the EASIX score predict CAR-T-related toxicity. Blood Adv. 2021, 5, 2799–2806. Available online: https://pubmed.ncbi.nlm.nih.gov/34264268/ (accessed on 18 January 2022). [CrossRef]
- Zhang, Z.L.; Hou, Y.L.; Li, D.T.; Li, F.Z. Laboratory findings of COVID-19: A systematic review and meta-analysis. Scand. J. Clin. Lab. Investig. 2020, 80, 441–447. Available online: http://www.ncbi.nlm.nih.gov/pubmed/32449374 (accessed on 18 January 2022). [CrossRef]
- Verma, S.K.; Molitoris, B.A. Renal endothelial injury and microvascular dysfunction in acute kidney injury. Semin. Nephrol. 2015, 35, 96–107. Available online: https://pubmed.ncbi.nlm.nih.gov/25795503/ (accessed on 18 January 2022). [CrossRef] [Green Version]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The Vascular Endothelium and Human Diseases. Int. J. Biol. Sci. 2013, 9, 1057. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3831119/ (accessed on 18 January 2022). [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Outcome | ||||
|---|---|---|---|---|
| Variable | No. of Patients, n = 370 | Non-Survivors, n = 243 | Survivors, n = 127 | p-Value |
| Male | 242 (65.4%) | 155 (63.8%) | 87 (68.5%) | 0.365 |
| Age | 66.9 (12.9), 68 [60.8–74.3] | 69.7 (11.4), 70 [63–77] | 61.6 (14), 65 [52–70] | <0.001 |
| Death | 243 (65.7%) | |||
| Concomitant diseases | ||||
| Cardiovascular diseases | 251 (67.8%) | 176 (72.4%) | 75 (59.1%) | 0.009 |
| Hypertension | 231 (62.4%) | 161 (66.3%) | 70 (55.1%) | 0.036 |
| Atrial fibrillation | 47 (12.7%) | 38 (15.6%) | 9 (7.1%) | 0.019 |
| Ischemic heart disease | 86 (23.2%) | 70 (28.8%) | 16 (12.6%) | <0.001 |
| Pulmonary diseases | 38 (9.7%) | 26 (10.7%) | 10 (7.9%) | 0.384 |
| Asthma | 19 (5.1%) | 13 (5.3%) | 6 (4.7%) | 0.796 |
| COPD | 11 (3.0%) | 8 (3.3%) | 3 (2.4%) | 0.617 |
| Other | 8 (2.2%) | 7 (2.9%) | 1 (0.8%) | 0.189 |
| Diabetes | 134 (36.2%) | 97 (39.9%) | 37 (29.1%) | 0.103 |
| Malignant neoplasm | 57 (15.4%) | 44 (18.1%) | 13 (10.2%) | 0.046 |
| Chronic kidney disease | 33 (8.9%) | 30 (12.3%) | 3 (2.4%) | 0.001 |
| Obesity | 105 (28.4%) | 68 (28.0%) | 37 (29.1%) | 0.816 |
| SpO2 without oxygen supply | 83.4 (12.1), 86 [80–92] | 82.4 (13.6), 86.5 [78–92] | 85.4 (7.92), 86 [82–90] | 0.442 |
| Severity (according to WHO scale) | 0.171 | |||
| 1 | 5 (1.4%) | 3 (1.2%) | 2 (1.6%) | |
| 2 | 103 (27.8%) | 69 (28.4%) | 34 (26.8%) | |
| 3 | 222 (60.0%) | 136 (56.0%) | 86 (67.7%) | |
| 4 | 40 (10.8%) | 35 (14.4%) | 5 (3.9%) | |
| Duration of hospitalisation, days | 19.3 (15.2), 16 [10–24] | 16.1 (12.6), 14 [8–21] | 25.5 (17.7), 21 [13–31.8] | <0.001 |
| Duration of symptoms before hospital admission, days | 7.1 (4.4), 7 [4–9] | 6.7 (4.5), 6 [4–8] | 7.8 (4.1), 7 [5–10] | 0.026 |
| Deterioration, days (from disease onset) | 8.5 (5.8), 7 [5–10] | 8.4 (6.6), 7 [5–10] | 8.8 (4.2), 8 [6–11] | 0.564 |
| ICU admission | 216 (58.4%) | 182 (74.9%) | 34 (26.8%) | <0.001 |
| Non-rebreather mask 10–15 L/min | 352 (95.1%) | 229 (94.2%) | 123 (96.9%) | 0.268 |
| Non-rebreather mask 10–15 L/min duration, days | 2.6 (3.3), 2 [1–3] | 2.6 (3.6), 2 [1–3] | 2.6 (2.6), 2 [1–3] | 0.925 |
| HFNO | 253 (68.4%) | 147 (60.5%) | 106 (83.5%) | <0.001 |
| HFNO duration, days | 5.6 (5.0), 4 [2–8] | 3.6 (3.2), 2 [1–5] | 8.3 (5.8), 7 [4–11] | <0.001 |
| NIV | 69 (18.6%) | 60 (24.7%) | 9 (7.1%) | <0.001 |
| NIV duration, days | 4.9 (4.8), 3 [1–6.5] | 4.8 (4.9), 3 [1.3–6] | 5.1 (5.4), 3 [1–7] | 0.829 |
| IMV | 220 (59.5%) | 186 (76.5%) | 34 (26.8%) | <0.001 |
| IMV duration, days | 13.8 (12.9), 11 [6–17] | 12.3 (11.0), 10 [5.5–17] | 22.6 (19.3), 17 [11.3–26.3] | 0.001 |
| Lab test results | ||||
| CRP (>6 mg/L) | 140.30 (99.23), 123.40 [62–199.2] | 142.30 (100.60), 125.00 [63.59–198.30] | 136.40 (97.20), 117.6 [59.90–201.10] | 0.478 |
| Procalcitonin (>0.05 ng/mL) | 1.74 (4.57), 0.26 [0.1–0.86] | 2.12 (5.14), 0.35 [0.13–1.14] | 1.08 (3.31), 0.15 [0.08–0.39] | 0.110 |
| Ferritin (>274.66 ng/mL | 1846.93 (2210.77), 1527.24 [593.86–2325.59] | 1910.18 (2228.75), 1304.80 [632.49–2489.59] | 1763.91 (2212.21), 1138.11 [566.72–2308.85] | 0.699 |
| LDH (>220 U/L) | 575 (315), 530 [397–671] | 602 (368), 550 [388–734] | 524 (161), 504 [411–608] | 0.026 |
| White blood count (4–10 G/L) | 9.00 (9.51), 7.56 [5.46–10.49] | 9.47 (11.4), 7.99 [5.47–11.02] | 8.09 (3.83), 7.39 [5.43–9.77] | 0.180 |
| Neutrophils (1.8–7 G/L) | 7.10 (4.1), 6.3 [4.1–8.8] | 7.22 (4.29), 6.5 [4.1–9.5] | 6.75 (3.73), 6.00 [4.28–8.03] | 0.362 |
| Lymphocytes (1–4 G/L) | 1.00 (0.7), 0.8 [0.6–1.2] | 1.00 (0.8), 0.8 [0.6–1.2] | 0.90 (0.4), 0.8 [0.6–1.1] | 0.188 |
| Haemoglobin (13.5–18.0 g/dL) | 13.20 (2.21), 13.4 [12.1–14.7] | 12.90 (2.39), 13.1 [11.8–14.5] | 13.70 (1.71), 14.10 [12.7–14.9] | 0.860 |
| Thrombocytes (150–420 G/L) | 222 (106), 197 [152–265] | 216 (109), 192 [145–260] | 233 (99.9), 206 [167–277] | 0.130 |
| D-dimer (>500 ng/mL) | 4073.30 (10,041.6), 1409.5 [876.5–2676.75] | 5163.78 (12,060), 1797 [976–3327] | 2060.79 (3681.20), 1145.00 [728.00–2104.00] | 0.018 |
| INR (0.8–1.2) | 1.17 (0.37), 1.09 [1.02–1.19] | 1.20 (0.41), 1.11 [1.03–1.23] | 1.12 (0.29), 1.06 [1.00–1.14] | 0.073 |
| AST (>34 U/L) | 69.34 (57.95), 54.70 [39.00–80.23] | 71.07 (61.80), 53 [38.85–82.90] | 66.24 (50.73), 57.00 [39.30–73.00] | 0.479 |
| ALT (>55 U/L) | 52.83 (54.03), 39.35 [25.85–64.40] | 51.02 (60.1), 37 [22.85–63.45] | 56.27 (40.37), 42.80 [29.20–68.60] | 0.386 |
| Creatinine (>1.15 mg/dL) | 1.43 (1.57), 1.03 [0.81–1.44] | 1.58 (1.78), 1.13 [0.83–1.66] | 1.14 (1.03), 0.92 [0.78–1.11] | 0.016 |
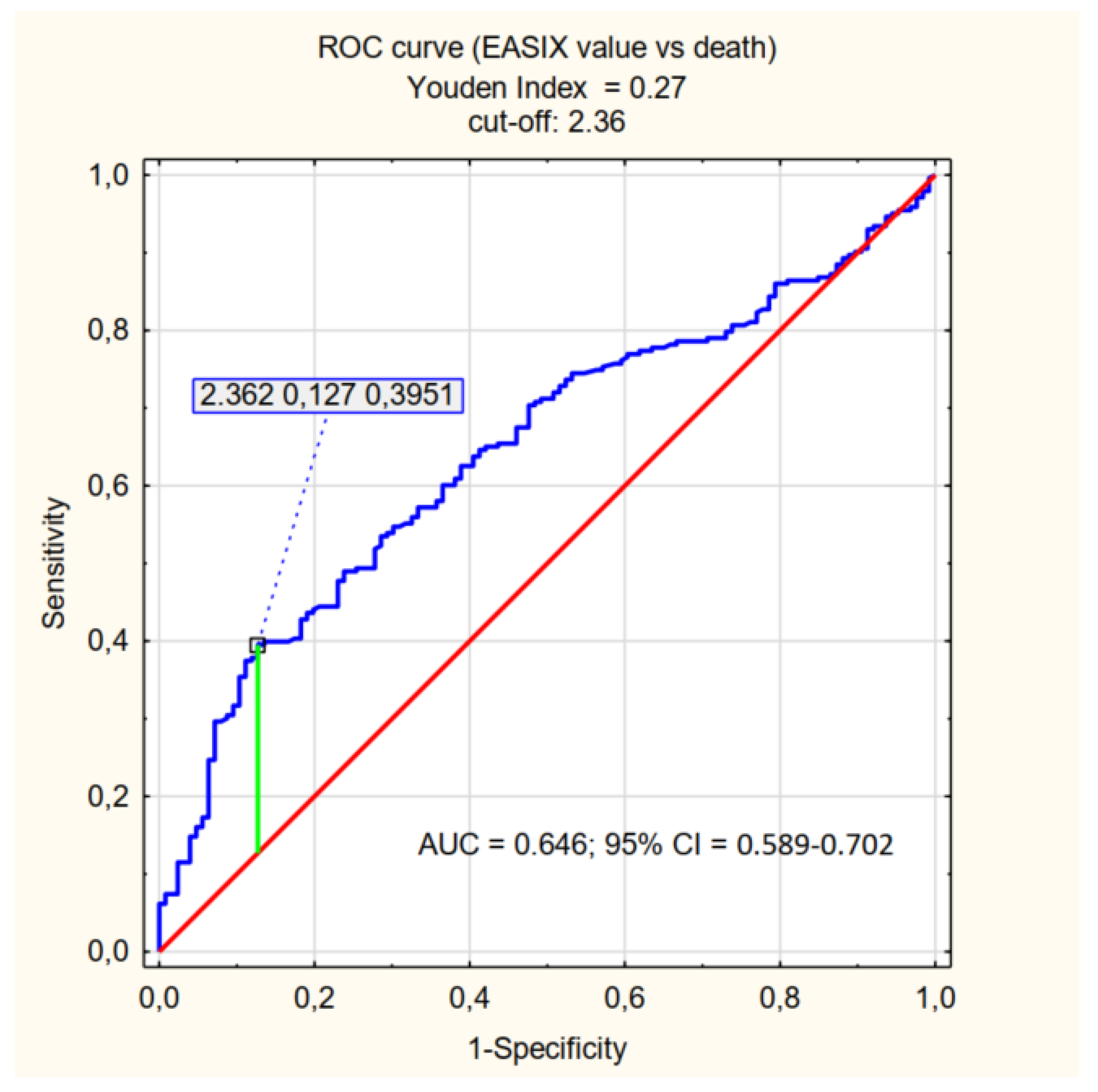
| EASIX | 5.39 (11.04), 2.73 [1.68–4.82] | 6.66 (13.29), 3.11 [1.89–5.87] | 2.94 (2.92), 2.05 [1.59–3.18] | <0.001 |
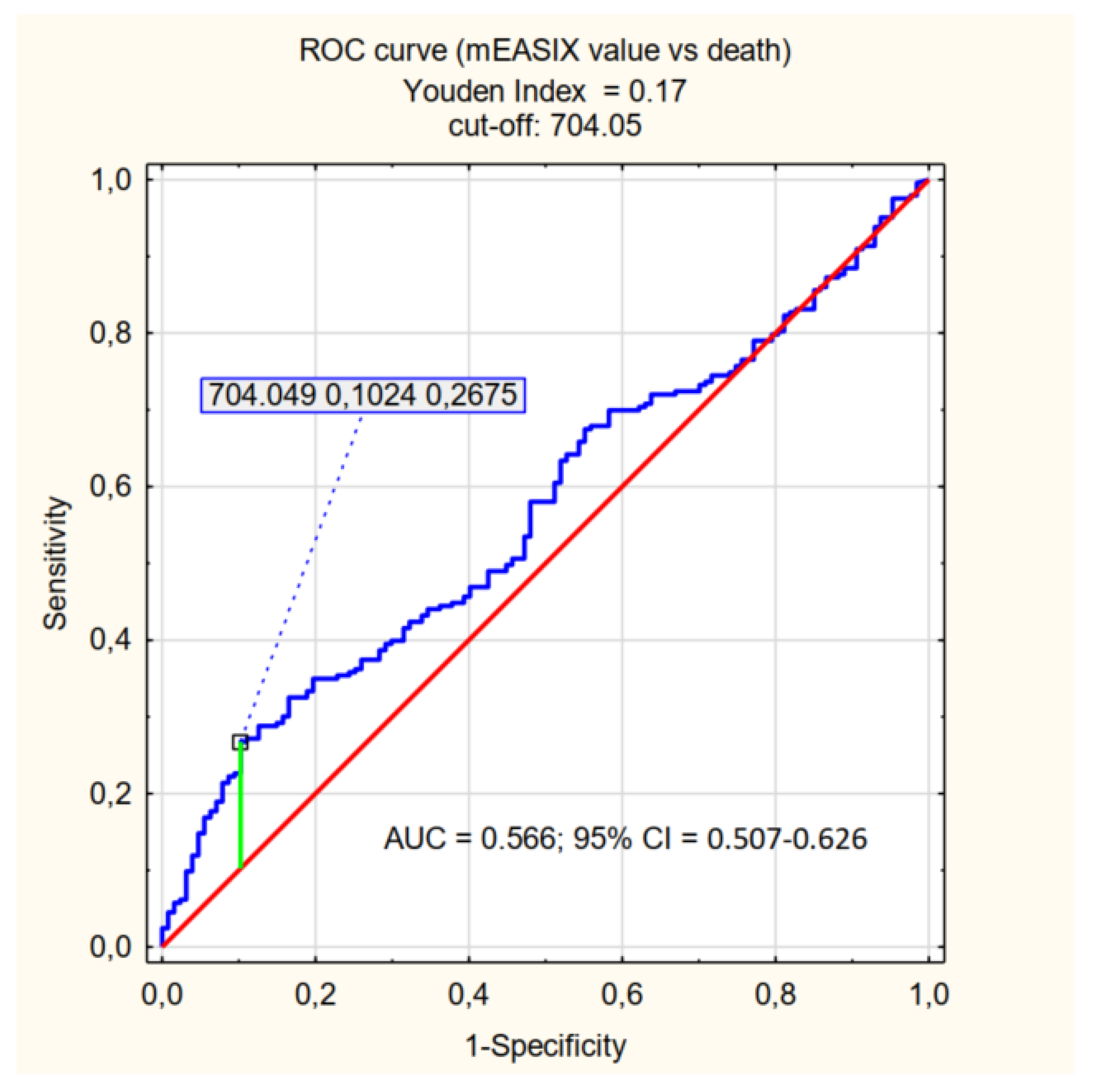
| mEASIX | 497.49 (783.11), 303.36 [130.07–598.69] | 571.22 (924.56), 315.37 [130.23–740.82] | 356.42 (358.55), 264.14 [125.57–468.00] | <0.001 |
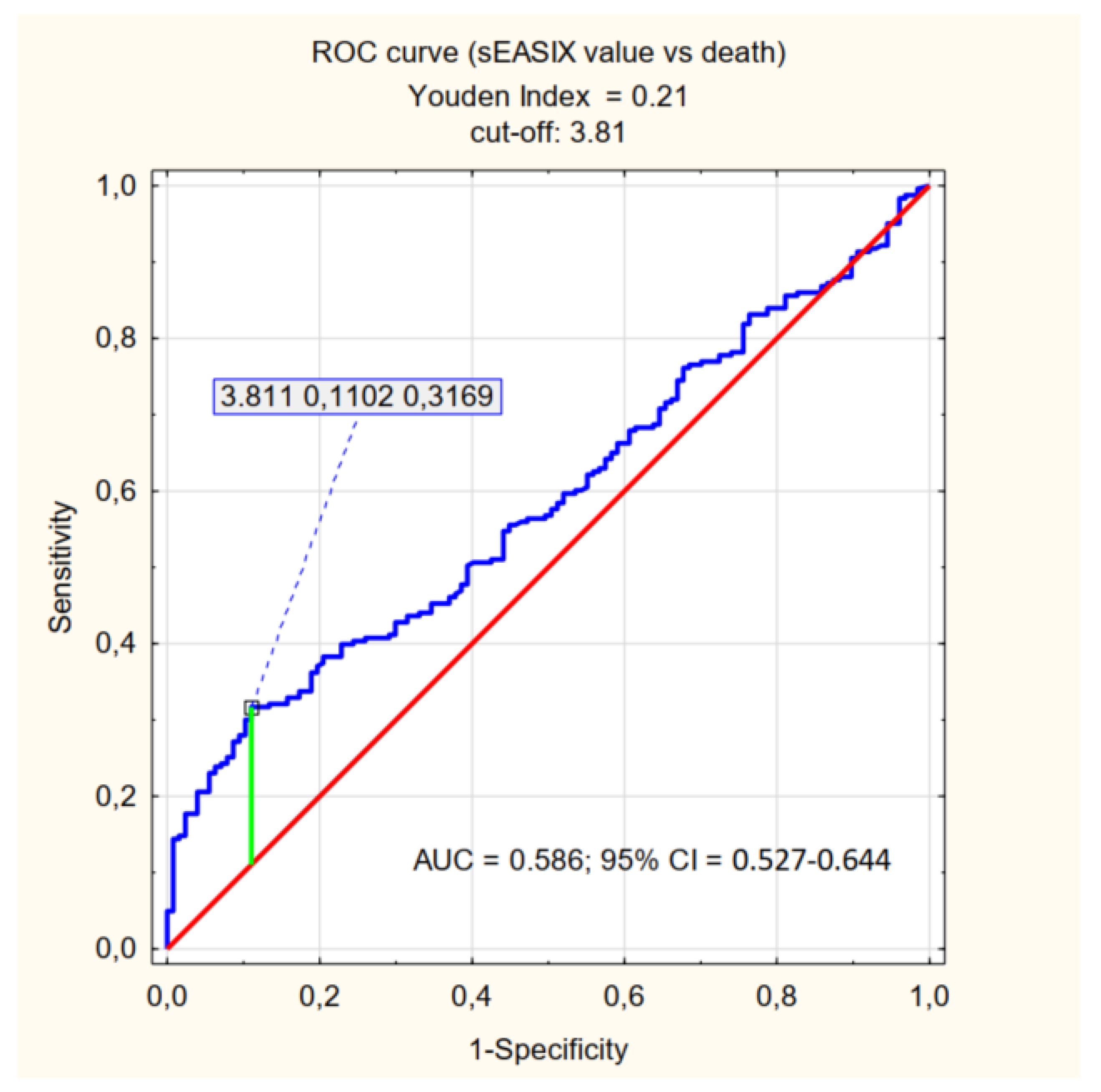
| sEASIX | 3.40 (4.76), 2.49 [1.81–3.79] | 3.86 (5.77), 2.60 [1.88–4.25] | 2.52 (1.18), 2.36 [1.74–3.23] | <0.001 |
| p-Value | Cut-Off | AUC | 95% CI | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|
| Variable | ||||||
| Age | <0.001 | ≥72 | 0.662 | 0.603–0.720 | 0.44 | 0.80 |
| Duration of symptoms before hospital admission, days | 0.026 | <7 | 0.581 | 0.520–0.642 | 0.72 | 0.40 |
| Lab test parameters | ||||||
| LDH | 0.026 | ≥656 | 0.540 | 0.482–0.599 | 0.34 | 0.86 |
| D-dimer | 0.018 | ≥1714 | 0.636 | 0.576–0.696 | 0.53 | 0.68 |
| Creatinine | 0.016 | ≥1.23 | 0.642 | 0.585–0.698 | 0.44 | 0.85 |
| AUC | 95% CI | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|---|
| High EASIX | 0.646 | 0.589–0.702 | 0.40 | 0.87 | 0.86 | 0.43 |
| High mEASIX | 0.566 | 0.507–0.626 | 0.27 | 0.90 | 0.83 | 0.38 |
| High sEASIX | 0.586 | 0.527–0.644 | 0.32 | 0.89 | 0.83 | 0.41 |
| EASIX | ||||||
|---|---|---|---|---|---|---|
| Effect of: | p | Cut-Off | AUC | 95% CI | Sensitivity | Specificity |
| HFNO | 0.622 | |||||
| NIV | 0.271 | |||||
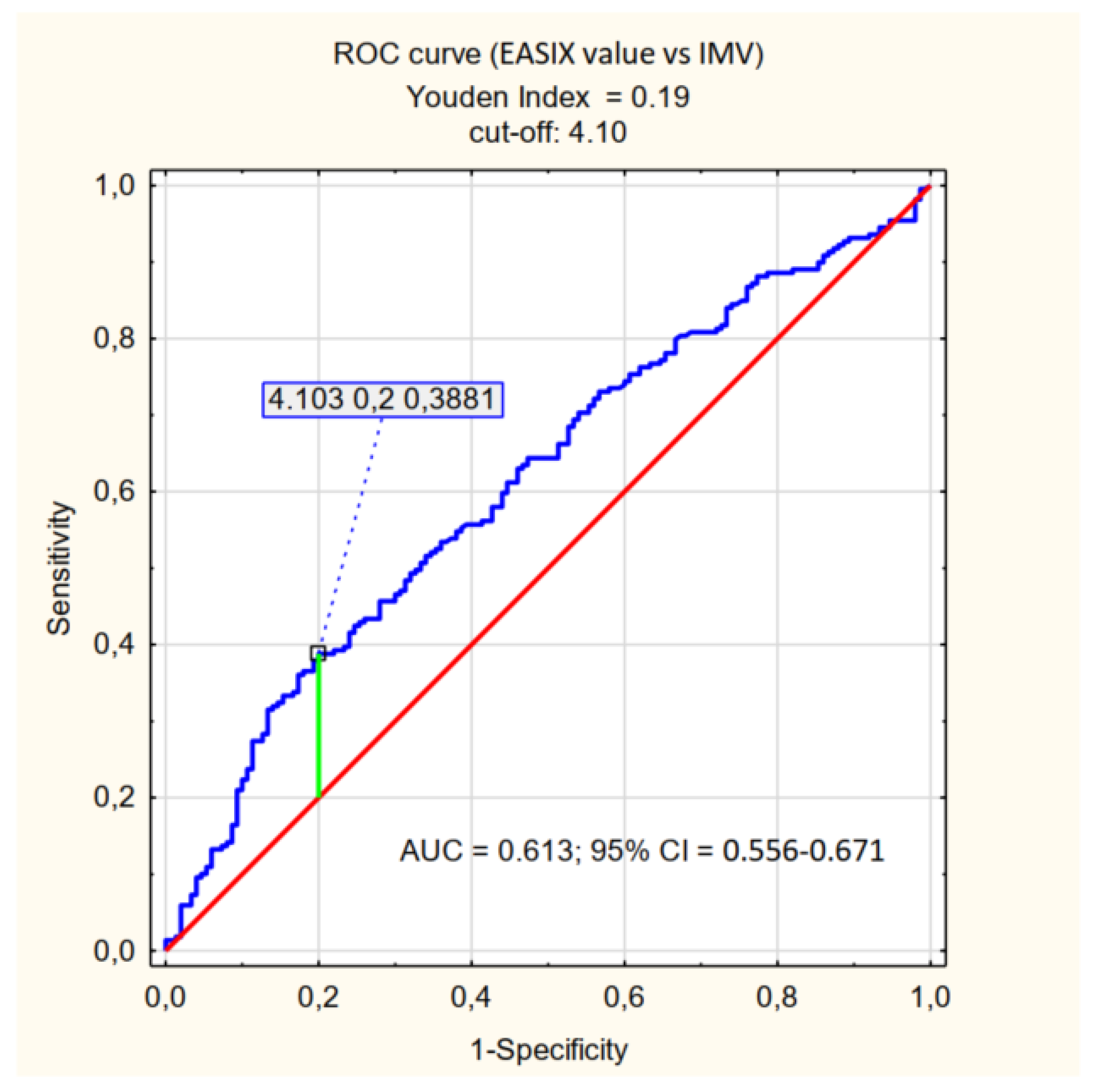
| IMV | <0.001 | 4.10 | 0.613 | 0.556–0.671 | 0.39 | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zińczuk, A.; Rorat, M.; Simon, K.; Jurek, T. EASIX, Modified EASIX and Simplified EASIX as an Early Predictor for Intensive Care Unit Admission and Mortality in Severe COVID-19 Patients. J. Pers. Med. 2022, 12, 1022. https://doi.org/10.3390/jpm12071022
Zińczuk A, Rorat M, Simon K, Jurek T. EASIX, Modified EASIX and Simplified EASIX as an Early Predictor for Intensive Care Unit Admission and Mortality in Severe COVID-19 Patients. Journal of Personalized Medicine. 2022; 12(7):1022. https://doi.org/10.3390/jpm12071022
Chicago/Turabian StyleZińczuk, Aleksander, Marta Rorat, Krzysztof Simon, and Tomasz Jurek. 2022. "EASIX, Modified EASIX and Simplified EASIX as an Early Predictor for Intensive Care Unit Admission and Mortality in Severe COVID-19 Patients" Journal of Personalized Medicine 12, no. 7: 1022. https://doi.org/10.3390/jpm12071022