1. Introduction
To construct a large-scale comprehensive view of biological systems, several smaller models may need to be integrated. However, this can be difficult to accomplish, as models can exhibit significant inner variation due to the different expertise of modelers or perspectives of model.
Infectious disease modeling is an expansive field with a long history, encompassing a range of methods and assumptions that are not necessarily comparable or even designed for the same purpose. During the ongoing COVID-19 pandemic, the scientific community consider computer modeling as a possible solving factor given the enormous uncertainty about the evolution of the pandemic. In this context, epidemiological models can be critical planning tools for policymakers, clinicians, and public health practitioners [
1]. Currently, COVID-19 modeling studies follow one of two general approaches: forecasting models and mechanistic models. However, these well-constructed statistical frameworks have several limits. These can be used for short-term forecasts through machine learning or regression to crunch past epidemiological data or data from different locations to make projections for the future [
2].
Traditionally, the study of infectious disease systems was based on two main theories: infectious disease causation theory and infectious disease transmission theory.
The infectious disease causation theory incudes series of theories progressively refined, one after another as new knowledge, to explain the causes of infectious diseases and considers the infectious disease as systems [
3]. The current and modern infectious disease causation theory considers infectious disease systems organized into hierarchical multilevel and multiscale complex systems, with levels ranging from cellular to macroecosystem one. The infectious disease transmission mechanism theory, instead, is based on the idea that infectious disease dynamics consist of transmission as main dynamic process at each hierarchical level (cell, tissue, host, etc.). Specific transmission models can be developed to study an infectious disease system at a particular level of organization. The standard approach to developing such models is to classify the reference population (may be population of cells at cell level or a population of hosts for the host level, and so on) into compartments within unit exanimated (cells, hosts, etc.). The knowledge about transmission mechanisms allows to develop quantitative models of infectious disease dynamics [
4,
5].
However, an infectious disease system is also result of the interaction of three subsystems (host, pathogen, and environment) organized into hierarchical multilevel and multiscale complex systems, with levels ranging from the cellular level to the macro-ecosystem level. The subsystems are decomposed into levels and then into scales. Therefore, to describe the phenomenon of infectious disease both in time and in space, it needs to define a model, where infectious disease systems are identified as multilevel and multiscale systems [
5,
6].
Recent advances in systems biology spawned the view of human disease as a manifestation of genetic and environmental perturbations to the human interactome, a key postulate being that similar perturbation patterns lead to similar disease phenotypes [
7]. However, infectious diseases are extremely complex, as the dynamics of infection into the host could be influenced by the pathogen and the host response could induce adaptation events into the pathogen [
8,
9].
Computational modeling can contribute to a deeper understanding of relevant chemical and biological phenomena based on their underlying mechanisms, applying network-based model of viral–host interaction [
10,
11,
12]. Simulations of models can help investigating a complete biological process instead of considering smaller segments or aspects, detailing a segment of a process. Moreover, data-driven inferences could suggest or even address future experiments, predicting with high statistical significance the behavior of system under given conditions and identifying unknown causal relationships from observational time series data [
13].
Disease maps are an emerging concept, bridging bioinformatics, molecular biology, and clinical research, with the potential to link the domains of biomedical knowledge and data, providing an intermediate step between a conceptual and an executable model [
14,
15]. Such representation is an important tool to capture not only biochemical interactions, but also physiological mechanisms, describing the complexity of disease.
Previously, we carried out a scoping review of the literature based on conceptual domains to understand the molecular pathophysiology linking SARS-CoV-2 infection to its clinical manifestations (Montaldo and colleagues).
Thus, the further aim of our research group was to use the results of this scoping review along with other data from literature to design a multilevel and multiscale model framework for COVID-19. For this aim, at first a conceptual framework was built based on current literature evidence following these steps: to identify the molecular pathophysiology related to the clinical manifestations and course of COVID-19; to collect the mechanistic knowledge scattered across the scientific literature and bioinformatic databases; to integrate it using a logical/conceptual model systems biology. In the future, we will expect to assess the model in decision support.
In summary, here we describe the process and the methodology followed to build the modular design and conceptual framework of disease model for COVID-19.
2. Materials and Methods
The model building process began from building a domain-based literature review regarding a multi omics approach to COVID-19 (Montaldo and colleagues: Multiomics approach to COVID-19: a domain-based literature review). The results of this review allowed to define and validate a conceptual framework for COVID-19, representing these results on a multilevel and multiscale model.
The same interdisciplinary working groups that carried out the scoping review were involved for this purpose.
2.1. Step-by-Step Workflow for a Conceptual Framework of Disease Model
The conceptual framework for disease model of COVID-19 was designed investigating mainly interacting subsystems of host and pathogen. Such framework must be based on standard evidence derived from literature, appropriately identified and reviewed by domain-expert group. We carried out also a short literature review concerning methods, principles, and referral concept on infectious diseases modeling.
This methodological review, which we will call “short review”, is distinct from COVID-19 domain-based scoping review. The results of the short review are extensively reported in
Supplement text.
To define the framework of this COVID-19 model, we followed the steps described below.
2.1.1. Step 1: Multiomics Approach and Domains Identification Literature-Based
A conceptual model of a disease must contain disease-related signaling and metabolic and gene regulatory processes, with evidence of their relationships to pathophysiological causes and outcomes.
Therefore, it is necessary to develop and exploit protocols for high-quality representation of multilevel and multiscale information, including subcellular, cellular, tissue, organ, and organism levels.
Such amount of literature information must be reviewed and sorted by domain-expert group.
For this purpose, we assumed as conceptual reference the same studies, which were used to identify the conceptual domains on which our previous scoping review was based:
- -
Gordon and colleagues [
16], which highlights interactions between SARS-CoV-2 proteins and human proteins involved in several complexes and biological processes, and multiple innate immune pathways involvement.
- -
Ostaszewski and colleagues [
17,
18]. The COVID-19 Disease Map is an open-access collection of curated computational diagrams and models of molecular mechanisms implicated in the disease.
Moreover, we consider the domain-based scoping review results, as reported in separated paper (Montaldo and colleagues). This scoping review is based on four conceptual domains (virus characterization, host signature, pathways and phenotypes) addressed within a disease network model. The results can be summarized as follows:
- -
the interactome method (as conceptually defined by Gordon and colleagues) is helpful to study the biology of the viral–host interactions and the biochemical pathways involved;
- -
the disease progression is mediated by commonly dysregulated pathways of innate immune responses, such as complement activation, inflammatory responses, neutrophil activation and degranulation, platelet degranulation, and dysregulation of blood coagulation and metabolism.
Table 1 reports the scoping review results detailed, aggregated in domains, and divided in subdomains.
Such results were especially useful in evaluating host response and identifying clinical COVID-19 phenotypes and could contribute to elaborate omics-based disease maps.
2.1.2. Step 2: Defining Criteria and Framework for the COVID-19 Disease Model
To define criteria useful to building a logical model disease framework, we considered the following studies, which were more extensively reported in
Supplement text:
Wong and colleagues (2020) [
19]. A multiscale tissue simulator developed by an international and multi-disciplinary coalition, which could be used to investigate mechanisms of intracellular viral replication, infection of epithelial cells, host immune response, and tissue damage. It is a prototype of multiscale model of SARS-CoV-2 dynamics in lung tissue iteratively refined. To build the simulator, a modular design was used: an overall tissue-scale model integrates an array of targeted submodels that simulate critical processes (e.g., receptor binding and trafficking and virus replication). Each submodel is clearly specified to enable interoperability and to allow subteams to simultaneously develop and test the model components in parallel.
Perfetto and colleagues (2020) [
20]. A dataset of physical molecular interactions, manually extracted by IMEx Consortium curators from 86 publications, focused on proteins from SARS-CoV-2, SARS-CoV and other members of the Coronaviridae family, currently comprises over 2,200 binarized interactions. Data on 70 organisms are included, and most interactions refer to SARS-CoV-2 and SARS-CoV-human host.
By these studies, we deduced that, to define the biological keys of COVID-19 model, these are the main criteria to follow:
- (a)
to investigate SARS-CoV2 dynamics;
- (b)
to help the scientific community to identify knowledge gap and to guide specific experiments and interventions (“what if …”);
- (c)
to be based on a modular design, where each module is divided into one or more submodules;
- (d)
one or more functions refer to submodules.
The same working groups that previously carried out COVID-19 domain-based scoping review compared the modular design, as above defined, to the results of this review, underlying a direct correspondence between module and domain.
Applying main criteria above reported to define the biological keys of the COVID-19 model, the following critical components of the model framework were identified:
general model framework;
module (tissue/organ and/or physiopathological mechanism);
submodules that simulate critical process (receptor binding, cleavage and processing viral proteins, virus replication).
2.1.3. Step 3: Normalization of the Biological Model on the Hierarchical Model
In the previous steps, we collected the mechanistic knowledge scattered across scientific literature and bioinformatic databases and integrated it using a logical/conceptual model systems biology. A model should also allow a correlation among host, pathogen, and environment.
For this step, we referenced results of the short review: principles and referral concepts for modeling of infectious diseases. An extensive description of results of the short review was reported in
Supplement text. The aim was to identify through this short review a model framework that allows to describe infectious disease phenomena, considering possible variations through time and space at different scales. We identified methodology proposed by Garira, which incorporates events, such as pathogen replication, giving rise to transmission events in time and space. This methodology assumes that there are seven levels (cell, tissue, organ, microsystem, host, community, macrosystem), and within each level, there are two limiting adjacent scales of infection: microscale and macroscale. These levels hierarchically organized and make infectious disease dynamics at each level as a multiscale loop, involving the reciprocal influence of macroscale and microscale [
4,
5].
The main topics for building a disease model framework were:
- -
at any level of an infectious disease system, there is no privileged/absolute scale, which would determine disease dynamics, but only interactions between microscale and macroscale;
- -
at every level of an infectious disease system, the reciprocal influence between microscale and macroscale establishes a pathogen replication-transmission multiscale cycle;
- -
to use the conceptual diagram of the seven hierarchical levels of organization of an infectious disease system and the associated macroscale and microscale for each hierarchical level [
21].
Here, we performed an alignment between multiscale levels and modules/domains as biologically defined above, considering the results of the literature review. We attributed a hierarchical scale among levels, and we associated macroscale/microscale for each level. The hierarchical scale macro/micro was defined considering module/submodule/functions, as organized in biological models reported above, and assuming that domain is assimilated into the module.
At last, we verified if the model framework is compliant with reciprocal influence between macroscale and microscale, types of environmentally transmitted infectious disease, following the Garira method, which was suitably adapted.
3. Results
Considering domains and datasets above identified and scoping review results, the following issues were considered useful to build a logical disease model framework:
- -
Virus dissemination in epithelial tissue;
- -
Virus binding, endocytosis, replication, and exocytosis;
- -
Infected cell responses: changes of metabolism, secreted signals, death;
- -
Inflammatory response;
- -
Ramp up of the immune response (particularly in lymph nodes);
- -
Immune cell infiltration;
- -
Immune cell predation of infected and other cells;
- -
Tissue damage by death of cells due to infection or host response.
We therefore performed the modular design of the COVID-19 model framework, biologically based. The logical process was an overall tissue-scale model that integrates an array of submodels, which simulate critical processes. Each submodel is clearly specified to enable interoperability and to allow subteams to simultaneously develop and test the model components in parallel. As expected in methods, the working group that previously carried out the COVID-19 domain-based scoping review translated the results of this review into modular logic (module/submodule/functions) of this model framework, as below reported:
- -
Module A: cell infection and viral replication (submodules: tissue microenviroment; binding receptor on the cell’s membrane (ACE2 system); endocytosis process; viral replication; assembled virions exported from the cell by exocytosis);
- -
Module B: infected cell response (submodules: activation IFN type1 signal; cell death process);
- -
Module C: inflammatory and immune responses (submodules: pneumocytes and alveolar macrophages; innate immune response; endothelial damage and systemic; tissue damage and cytokines);
- -
Module D: inflammatory and clinical outcomes (phenotypes), (submodules: dysregulated amplified immune response and chemokines replications in the lower airways persistence; systemic disease: interactions of viral infection, cytokine production, immune response; clinical syndromes: haemophagocytosis, intravascular coagulation, ARDS, organ failure).
The modular logic of the biological model framework is detailed in
Table 2.
The main information about COVID-19 and SARS-CoV-2 infection were classified in four modules: cell infection and viral replication; infected cell response; inflammatory, adaptive, and innate immune responses; inflammatory, clinical outcome and phenotypes.
This setting, composed by module and submodules, allows to highlight multiple biological pathways in cells, tissues, organs, and define different COVID-19 phenotypes. However, this structure can provide a modular and ordered literature data but it cannot represent a framework for disease model, as levels (different point of view) and scales (within or between objects of analysis) are not provided.
Then, to consider possible variations at different scales for many levels, we first identified the macro/microscale attributions depending on the considered level, applying method logic of Garira.
Secondly, we considered the types of reciprocal influence among macroscale, microscale, and environment related to SARS-CoV-2 infection processes.
The Garira methodology assumes that the microscale and the macroscale influence each other at each hierarchical level of an infectious disease system through interactions of four key disease processes:
- -
infection/superinfection by pathogen;
- -
pathogen replication;
- -
pathogen shedding/excretion;
- -
pathogen transmission.
At each hierarchical level, disease dynamics involve a pathogen replication-transmission multiscale cycle. This happens because, at each of the hierarchical levels of organization of an infectious disease system, the characteristic scale at which pathogen replication and pathogen transmission occur often does not match.
Consequently, we distinguished two kinds of reciprocal influences between microscale and macroscale:
Type I: the microscale influences the macroscale through pathogen shedding/excretion: this involves the movement of pathogen from the microscale to the macroscale.
Type II: the macroscale influences the microscale also through super-infection.
(i.e., repeated infection before the host recovers from an infectious episode).
This condition involves the movement of the pathogen from the macroscale to the microscale. [
5].
Furthermore, following the logic of Garira method, considering host as unit exanimated, it was possible to identify three different types of environmentally transmitted infectious disease systems: Type A, where the pathogen does not replicate within-host (microscale); Type B, where the pathogen replicates only within-host (microscale); Type C, where the pathogen replicates both within-host and between-hosts (microscale and macroscale).
An extensive description of the methodology regarding the mutual influence between micro/macroscale and the types of environmentally transmitted infectious disease systems are reported in
Supplement text. Conceptual representation of mutual macro/micro scale influences and infections environmentally transmitted are in
Table S1.
As descripted in methods, the biological model framework was normalized on the hierarchical model, appropriately adapted following Garira methodology, as below reported:
- -
Level from I to V:
Cell level: module A and module B. Cell infection and viral replication and infected cell response;
Tissue level: module C. Inflammatory, innate, and adaptive immune response;
Organ/anatomical compartment level: module C + D. Inflammatory, innate, and adaptive immune response;
Microsystem level: module C + B + A. The three previous modules can contribute to describe functional interactions between human host and multi pathogens, both within and between specific anatomical districts;
Host/organism level: module D + A. Inflammatory and clinical outcome, and phenotypes of host, transmission risk in hospital and family; social distancing;
- -
Level VI and VII:
- VI.
Community level: epidemiological enquiries within community (familiar and hospital clusters, etc.) and between communities (restriction movement, etc.), global surveillance of infectious diseases;
- VII.
Macrosystem level: dynamics of functional interactions between human communities and multi pathogens, both within and between specific social and environmental context.
Alignment between the biological modules (as reported in
Table 2) and the hierarchical levels was implemented according to previous scheme (as illustrated in
Table 3).
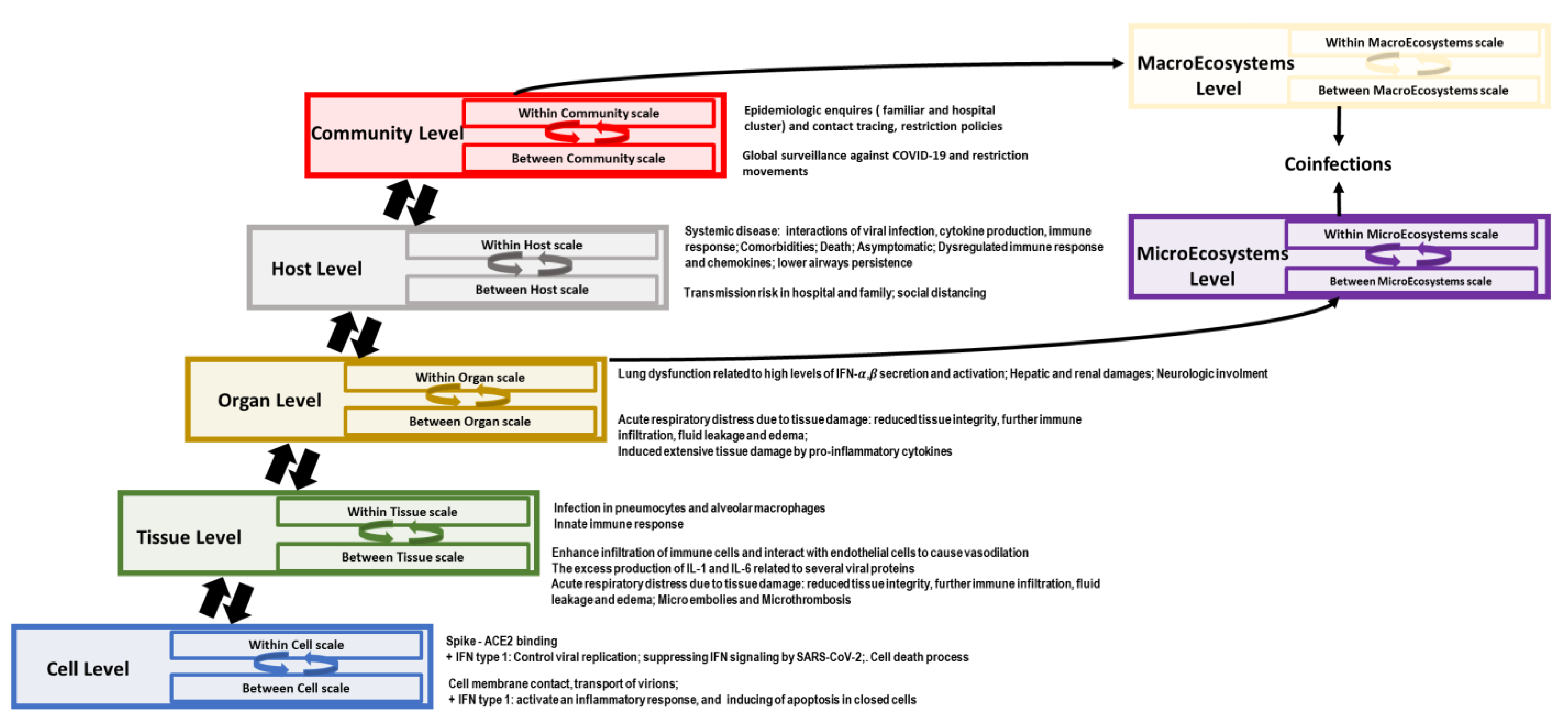
Finally, all this information was ordered in a framework diagram for level and scales (as illustrated in
Figure 1).
In fact, I-II-III levels contain structural information about viral biology, cell response, and damage in specific body districts, while V-VI-VII levels report descriptive information about clinical phenotypes, epidemiological dynamics, and social restrictions (as illustrated in
Figure 1)
Microecosystems and macroecosystems levels report all functional information about direct and indirect interactions among human host, SARS-CoV-2, other pathogens, or other SARS-CoV-2 strains, and environment. (as illustrated in
Table 3;
Figure 1). The point of view in these two levels is that the crucial aspect: microecosystems correspond to cell/tissue/organ system, while macroecosystems relate to host/community system. These two levels were not associated with any aspect of COVID-19 because of the lack of exhaustive data (as illustrated in
Figure 1).
Organically,
Table 4 represents the conceptual diagram of the seven hierarchical levels of organization of an infectious disease system related to SARS-CoV-2 infection processes as resulted from the domain-based scoping review, with the associated macroscale and microscale for each level and the types of reciprocal influences among macroscale, microscale, and environmental.
Such model framework can be enlarged with other and current information and detailed by adding new submodules, and it could be represented as a conceptual diagram of the seven hierarchical levels of organization of an infectious disease system, which could be applied also to other infection diseases.
4. Discussion
The molecular pathophysiology that links SARS-CoV-2 infection to COVID-19 clinical manifestations is complex and spans multiple biological pathways, cell types, and organs. To gain insights into this complex network, the biomedical research community needs to approach it from a systems perspective, collecting mechanistic knowledge scattered across scientific literature and bioinformatic databases and integrating it using formal systems biology standards.
COVID-19 Disease Map project represents a focal point to organize information about COVID-19 pathogenesis: it is an open-access collection of computational diagrams and models of molecular mechanisms of COVID-19, curated by biocurators, domain experts, modelers, and data analysts. The map is constantly evolving, and it is continuously refined, updated, analyzed, and shared. Currently, this repository reports 41 diagrams containing 1,836 interactions among 5,499 elements, supported by 617 publications and preprints [
17]. As part of this important experience, we suggest introducing new interactions into the existing diagrams [
16,
17].
Despite the increasing knowledge about COVID-19, there are many aspects still unclear and in need of further multiomics investigations, such as the pathophysiological pathways perturbed under comorbidities’ conditions and the degrees of severity.
The virus–host interactome is a network of virus–human protein–protein interactions (PPIs) that can help understanding COVID-19 mechanisms. It can be expanded by merging virus-host PPI data with human PPI and protein data to discover clusters of interactions indicating human mechanisms and pathways affected by SARS-CoV-2 [
11,
16].
Combined omics technologies could significantly contribute to improve the current understanding of COVID-19 pathology, as reported in our previous review on multiomics COVID-19 studies. However, the enormous amount of information available in the models, still needs to be integrated and harmonized. Thus, the development of disease models must rely on an active involvement and interpretation of domain experts.
Based on the above considerations, our modular design of conceptual disease model was built in analogy to the framework of two studies, chosen and evaluated by interdisciplinary working groups [
19].
In the
Table 2 are reported the key concepts of the framework and modular logic of a biological COVID-19 model. The modular design of this conceptual model framework was compared to the results of the domain-based scoping review (as reported in
Table 1), finding an almost complete overlap and a direct correspondence between module and domain.
This COVID-19 model framework was inspired by concept of infectious disease model system proposed by Garira. This theory considers the extension of the relativity principle in physics to the dynamic of the infectious diseases systems (“replication-transmission relativity theory”) and provides scientific basis for a systems level description of infectious diseases using multiscale modeling methods.
The Garira model allows to design every infectious disease as a multilevel and multiscale system organized into seven main hierarchical levels [
22]. In our work, we verified that the framework of the COVID-19 conceptual model is adaptable to Garira model. We also verified that in the model framework that was built, there is no privileged/absolute scale determining disease dynamics, and we identified only interactions among microscale, macroscale, and type of environmentally transmitted infections.
Such structural and functional information about cell response against virus and tissue/organ damages, as well as description of clinical phenotypes, epidemiological dynamics, and social restrictions are the scaffold to apply computation and mathematical model on biological and epidemiological systems [
23,
24,
25,
26].
We designed a conceptual diagram of the seven hierarchical levels, and the types of reciprocal influences between macroscale, microscale, and environment in relation to SARS-CoV-2 infection processes.
Finally, this model framework adapted and modified for COVID-19, allows a correlation among host, pathogen, and environment, developing a quantitative evaluation at different scales of the complex multiple biological pathways involved at different levels (cells, tissues, organs, etc.). From this point of view, the results of the scoping review represent the first experimental confirmation of this model, and otherwise, the model can be considered as validated by these results. Both the conceptual model framework and domain-based scoping review constitute a first operational result within an overall research project (i.e., It-IDRIN Project) whose main objective is an aggregation of clinical structures with “omics” competences in a collaborative network focused on pathology models.
In this context, although omics data could help to fill this model framework, providing signatures and pathways form specific phenotypes, they can give only a structural view, limited spatially and timely. Consequently, this model could be useful in research activities (experimental studies), finalizing it to design adaptive trails.
Thus, a network model of molecular interactions, based on omics data, can identify specific mechanisms of host–pathogen interactions, finding the degree of coherence in interactome with the hierarchical structure of the model. This computational approach could define whether an interaction is real, determining the molecular level involved, and correlating the cell/tissue/organ level involved.
Model simulations can help investigate a complete biological process instead of considering smaller segments or aspects, detail a segment of a process or simplify a very large one, suggest or even direct future experiments, and predict the behavior of a system under given conditions.
5. Conclusions
The development of disease model framework relies on an active involvement of domain experts. Multiscale modeling of infectious diseases aims to characterize the complexity of infectious disease systems.
The conclusive result is a methodology to design multiscale models of an infectious disease complex, integrating different kinds of data. This methodology is based on implementing a three-stage strategy in the research and development process for multiscale models of infectious disease systems. Further, such methodology could be applicable (with minor modifications) to multiscale modeling of other structurally organized complex systems beyond infectious disease systems.
This research and development process for multiscale models cannot be considered unique, complete, and final. Probably, it is bound to be improved, but it constitutes a good starting point, which may be useful as a basis for further refinement.
Supplementary Materials
The following are available online at
https://www.mdpi.com/article/10.3390/v13071309/s1, Table S1: key concepts, obtained by scoping review in Montaldo and colleagues, for the framework of a biological COVID-19 model. References [
3,
4,
5,
6,
16,
19,
20,
21,
22,
27,
28,
29,
30,
31,
32,
33] are cited in the Supplementary Materials.
Author Contributions
Conceptualization: F.M., F.N.L.; methodology: F.M., C.M., F.N.L.; investigation: F.M., C.M., E.G., F.N.L.; writing—original draft preparation: F.M., C.M., F.N.L.; writing—review and editing: E.G., I.A., M.A., V.B., G.M., A.S., G.M.F., M.P., M.R.C., F.N.L., G.I.; supervision: F.N.L., M.R.C., M.P., G.I. All authors have read and agreed to the published version of the manuscript.
Funding
National Institute for Infectious Diseases Lazzaro Spallanzani–IRCCS received financial support funded by Italian Ministry of Health, grants: Ricerca Corrente program 1- Emerging and re-emerging infections; It-IDRIN CCR-2017-23669075; and by projects COVID-2020-12371675 and COVID-2020-12371817. This work was supported also by Findus Italia, part of the Nomad Foods. Giuseppe Ippolito is co-Principal Investigator of the Pan-African Network on Emerging and Re-Emerging Infections (PANDORA-ID-NET–
https://www.pandora-id.net/ accessed on 24 May 2021) funded by the European and Developing Countries Clinical Trials Partnership the EU Horizon 2020 Framework Program.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data used to fill out this framework is reported in
Table S1.
Acknowledgments
We gratefully acknowledge collaborators members of COVID-19 scoping review working group. All the members of the COVID-19 INMI Network Medicine for IDs Study Group: Isabella Abbate, Manuela Antonioli, Veronica Bordoni, Alessandra Aiello, Fabiola Ciccosanti, Francesca Colavita, Chiara Farroni, Saeid Najafi Fard, Emanuela Giombini, Delia Goletti, Giulia Matusali, Gabriella Rozera, Martina Rueca, Alessandra Sacchi, Mauro Piacentini, Chiara Agrati, Gian Maria Fimia, Maria Rosaria Capobianchi, Chiara Montaldo, Francesco Messina, Francesco Nicola Lauria, and Giuseppe Ippolito. We gratefully thank also the COVID-19 INMI Network Medicine for IDs Study Group.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Saltelli, A.; Bammer, G.; Bruno, I.; Charters, E.; Di Fiore, M.; Didier, E.; Espeland, W.N.; Kay, J.; Lo Piano, S.; Mayo, D.; et al. Five ways to ensure that models serve society: A manifesto. Nature 2020, 582, 482–484. [Google Scholar] [CrossRef]
- Holmdahl, I.; Buckee, C. Wrong but Useful—What Covid-19 Epidemiologic Models Can and Cannot Tell Us. N. Engl. J. Med. 2020, 383, 303–305. [Google Scholar] [CrossRef]
- Karamanou, M.; Panayiotakopoulos, G.; Tsoucalas, G.; Kousoulis, A.A.; Androutsos, G. From miasmas to germs: A historical approach to theories of infectious disease transmission. Infez. Med. 2012, 20, 58–62. [Google Scholar]
- Garira, W. A primer on multiscale modelling of infectious disease systems. Infect. Dis. Model. 2018, 3, 176–191. [Google Scholar] [CrossRef]
- Garira, W. A complete categorization of multiscale models of infectious disease systems. J. Biol. Dyn. 2017, 11, 378–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garira, W. The research and development process for multiscale models of infectious disease systems. PLoS Comput. Biol. 2020, 16, e1007734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahni, N.; Yi, S.; Zhong, Q.; Jailkhani, N.; Charloteaux, B.; Cusick, M.E.; Vidal, M. Edgotype: A fundamental link between genotype and phenotype. Curr. Opin. Genet. Dev. 2013, 23, 649–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckhardt, M.; Hultquist, J.F.; Kaake, R.M.; Huttenhain, R.; Krogan, N.J. A systems approach to infectious disease. Nat. Rev. Genet. 2020, 21, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.F.; Xia, Y. Convergent perturbation of the human domain-resolved interactome by viruses and mutations inducing similar disease phenotypes. PLoS Comput. Biol. 2019, 15, e1006762. [Google Scholar] [CrossRef]
- Messina, F.; Giombini, E.; Agrati, C.; Vairo, F.; Bartoli, T.A.; Al Moghazi, S.; Piacentini, M.; Locatelli, F.; Kobinger, G.; Maeurer, M.; et al. COVID-19: Viral-host interactome analyzed by network based-approach model to study pathogenesis of SARS-CoV-2 infection. J. Transl. Med. 2020, 18, 233. [Google Scholar] [CrossRef] [PubMed]
- Messina, F.; Giombini, E.; Montaldo, C.; Sharma, A.; Zoccoli, A.; Sekaly, P.R.; Locatelli, F.; Zumla, A.; Maeurer, M.; Capobianchi, M.R.; et al. Looking for pathways related to COVID-19: Confirmation of pathogenic mechanisms by SARS-CoV-2—Host interactome. Cell Death Dis. 2021. [Google Scholar] [CrossRef]
- Navratil, V.; de Chassey, B.; Combe, C.R.; Lotteau, V. When the human viral infectome and diseasome networks collide: Towards a systems biology platform for the aetiology of human diseases. BMC Syst. Biol. 2011, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runge, J.; Nowack, P.; Kretschmer, M.; Flaxman, S.; Sejdinovic, D. Detecting and quantifying causal associations in large nonlinear time series datasets. Sci. Adv. 2019, 5, eaau4996. [Google Scholar] [CrossRef] [Green Version]
- Ostaszewski, M.; Gebel, S.; Kuperstein, I.; Mazein, A.; Zinovyev, A.; Dogrusoz, U.; Hasenauer, J.; Fleming, R.M.T.; Le Novere, N.; Gawron, P.; et al. Community-driven roadmap for integrated disease maps. Brief. Bioinform. 2019, 20, 659–670. [Google Scholar] [CrossRef]
- Mazein, A.; Ostaszewski, M.; Kuperstein, I.; Watterson, S.; Le Novere, N.; Lefaudeux, D.; De Meulder, B.; Pellet, J.; Balaur, I.; Saqi, M.; et al. Systems medicine disease maps: Community-driven comprehensive representation of disease mechanisms. NPJ Syst. Biol. Appl. 2018, 4, 21. [Google Scholar] [CrossRef]
- Gordon, D.E.; Jang, G.M.; Bouhaddou, M.; Xu, J.; Obernier, K.; White, K.M.; O’Meara, M.J.; Rezelj, V.V.; Guo, J.Z.; Swaney, D.L.; et al. A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 2020. [Google Scholar] [CrossRef]
- Ostaszewski, M.; Mazein, A.; Gillespie, M.E.; Kuperstein, I.; Niarakis, A.; Hermjakob, H.; Pico, A.R.; Willighagen, E.L.; Evelo, C.T.; Hasenauer, J.; et al. COVID-19 Disease Map, building a computational repository of SARS-CoV-2 virus-host interaction mechanisms. Sci. Data. 2020, 7, 136. [Google Scholar] [CrossRef]
- Ostaszewski, M.; Niarakis, A.; Mazein, A.; Kuperstein, I.; Phair, R.; Orta-Resendiz, A.; Singh, V.; Aghamiri, S.S.; Acencio, M.L.; Glaab, E.; et al. COVID-19 Disease Map, a computational knowledge repository of SARS-CoV-2 virus-host interaction mechanisms. bioRxiv 2020. [Google Scholar] [CrossRef]
- Wang, Y.; An, G.; Becker, A.; Cockrell, C.; Collier, N.; Craig, M.; Davis, C.L.; Faeder, J.; Versypt, A.N.F.; Gianlupi, J.F.; et al. Rapid community-driven development of a SARS-CoV-2 tissue simulator. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Perfetto, L.; Pastrello, C.; Del-Toro, N.; Duesbury, M.; Iannuccelli, M.; Kotlyar, M.; Licata, L.; Meldal, B.; Panneerselvam, K.; Panni, S.; et al. The IMEx coronavirus interactome: An evolving map of Coronaviridae-host molecular interactions. Database 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Garira, W. The Replication-Transmission Relativity Theory for Multiscale Modelling of Infectious Disease Systems. Sci. Rep. 2019, 9, 16353. [Google Scholar] [CrossRef] [PubMed]
- Netshikweta, R.; Garira, W. A Multiscale Model for the World’s First Parasitic Disease Targeted for Eradication: Guinea Worm Disease. Comput. Math. Methods Med. 2017, 2017, 1473287. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Owolabi, Y.; Li, A.; Lo, E.; Robinson, P.; Janies, D.; Lee, C.; Dulin, M. Patch dynamics modeling framework from pathogens’ perspective: Unified and standardized approach for complicated epidemic systems. PLoS ONE 2020, 15, e0238186. [Google Scholar] [CrossRef] [PubMed]
- Liang, K. Mathematical model of infection kinetics and its analysis for COVID-19, SARS and MERS. Infect. Genet. Evol. 2020, 82, 104306. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Coba, M.P.; Sun, F. Inference of domain-disease associations from domain-protein, protein-disease and disease-disease relationships. BMC Syst. Biol. 2016, 10 (Suppl. 1), 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawelek, K.A.; Salmeron, C.; Del Valle, S. Connecting within and between-hosts dynamics in the influenza infection-staged epidemiological models with behavior change. J. Coupled Syst. Multiscale Dyn. 2015, 3, 233–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Guo, M.; Tian, X.; Wang, X.; Yang, X.; Wu, P.; Liu, C.; Xiao, Z.; Qu, Y.; Yin, Y.; et al. Virus-Host Interactome and Proteomic Survey Reveal Potential Virulence Factors Influencing SARS-CoV-2 Pathogenesis. Med (N. Y.) 2021, 2, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Garira, W.; Mathebula, D.; Netshikweta, R. A mathematical modelling framework for linked within-host and between-host dynamics for infections with free-living pathogens in the environment. Math. Biosci. 2014, 256, 58–78. [Google Scholar] [CrossRef]
- Spicknall, I.H.; Koopman, J.S.; Nicas, M.; Pujol, J.M.; Li, S.; Eisenberg, J.N. Informing optimal environmental influenza interventions: How the host, agent, and environment alter dominant routes of transmission. PLoS Comput. Biol. 2010, 6, e1000969. [Google Scholar] [CrossRef]
- Beggs, C.B.; Noakes, C.J.; Sleigh, P.A.; Fletcher, L.A.; Siddiqi, K. The transmission of tuberculosis in confined spaces: An analytical review of alternative epidemiological models. Int. J. Tuberc. Lung Dis. 2003, 7, 1015–1026. [Google Scholar]
- Fung, I.C. Cholera transmission dynamic models for public health practitioners. Emerg. Themes Epidemiol. 2014, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chikerema, S.M.; Murwira, A.; Matope, G.; Pfukenyi, D.M. Spatial modelling of Bacillus anthracis ecological niche in Zimbabwe. Prev. Vet. Med. 2013, 111, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Breban, R.; Drake, J.M.; Rohani, P. A general multi-strain model with environmental transmission: Invasion conditions for the disease-free and endemic states. J. Theor. Biol. 2010, 264, 729–736. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}
