
Effect of Immuno-Nutrition on Malnutrition, Inflammatory Response and Clinical Course of Semi-Critically Ill COVID-19 Patients: A Pilot Perspective Study
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Inclusion and Exclusion Criteria
2.3. Immune-Nutrition Administration Scheme
2.4. Nutritional Assessment
2.4.1. Mini Nutritional Assessment (MNA) Test
- -
- Screening (maximum score of 14 out of six variables): story of weight loss in the previous three months, food intake, motility, acute stress, cognitive status, and Body Mass Index (BMI) assessment. In particular, score of 0–7 is predictive of malnutrition, a score of 8–11 suggests that patients are at risk of malnutrition, and a score of 12–14 indicates that the person is well nourished and needs no further investigation. If the score is less than 11 it is strongly recommended to continue with the remaining test items.A MNA score higher than 24 indicates the patient is well-nourished, a score between 17–23.5 suggests a risk of malnutrition and scores lower than 17 clearly highlight malnutrition.
- -
- Self-Global Assessment (history of drugs assumption, food habits, fluid intake, residence place, and patient’s considerations on personal health status and on nutritional status).
2.4.2. Bioimpedance Vector Analysis
2.5. Data Collection
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lai, C.; Hsu, C.; Hsueh, S.; Yen, M.; Ko, W.; Hsueh, P. Multisystem inflammatory syndrome in adults: Characteristics, treatment, and outcomes. J. Med. Virol. 2022, 95, 28426. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Guo, L.; Feng, L. Interplay between swine enteric coronaviruses and host innate immune. Front. Veter Sci. 2022, 9, 1083605. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Leggeri, C.; Cinelli, G.; Tarsitano, M.G.; Caparello, G.; Carrano, E.; et al. COVID-19: Is there a role for immuno-nutrition in obese patient? J. Transl. Med. 2020, 18, 415. [Google Scholar] [CrossRef] [PubMed]
- Subedi, L.; Tchen, S.; Gaire, B.P.; Hu, B.; Hu, K. Adjunctive Nutraceutical Therapies for COVID-19. Int. J. Mol. Sci. 2021, 22, 1963. [Google Scholar] [CrossRef]
- Shakoor, H.; Feehan, J.; Al Dhaheri, A.S.; Ali, H.I.; Platat, C.; Ismail, L.C.; Apostolopoulos, V.; Stojanovska, L. Immune-boosting role of vitamins D; C; E; zinc; selenium and omega-3 fatty acids: Could they help against COVID-19? Maturitas 2021, 143, 1–9. [Google Scholar] [CrossRef]
- Derbyshire, E.; Delange, J. COVID-19: Is there a role for immuno-nutrition; particularly in the over 65s? BMJ Nutr. Prev. Health 2020, 3, 100–105. [Google Scholar] [CrossRef]
- Jovic, T.H.; Ali, S.R.; Ibrahim, N.; Jessop, Z.M.; Tarassoli, S.P.; Dobbs, T.D.; Holford, P.; Thornton, C.A.; Whitaker, I.S. Could Vitamins Help in the Fight Against COVID-19? Nutrients 2020, 12, 2550. [Google Scholar] [CrossRef]
- Grimble, R.F. Basics in clinical nutrition: Immuno-nutrition—Nutrients which influence immunity: Effect and mechanism of action. Eur. E-J. Clin. Nutr. Metab. 2009, 4, e10–e13. [Google Scholar] [CrossRef] [Green Version]
- Bae, M.; Kim, H. Mini-Review on the Roles of Vitamin C, Vitamin D, and Selenium in the Immune System against COVID-19. Molecules 2020, 25, 5346. [Google Scholar] [CrossRef]
- Scarcella, M.; Scarpellini, E.; Ascani, A.; Commissari, R.; Scorcella, C.; Zanetti, M.; Parisi, A.; Monti, R.; Milic, N.; Donati, A.; et al. Effect of Whey Proteins on Malnutrition and Extubating Time of Critically Ill COVID-19 Patients. Nutrients 2022, 14, 437. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19) Treatment Guidelines; National Institutes of Health (US): Bethesda, MD, USA, 2021.
- Matuszczyk, M.; Meglicka, M.; Landowski, P.; Czkwianianc, E.; Sordyl, B.; Szymańska, E.; Kierkuś, J. Oral exclusive enteral nutrition for induction of clinical remission, mucosal healing, and improvement of nutritional status and growth velocity in children with active Crohn’s disease—A prospective multicentre trial. Prz. Gastroenterol. 2021, 16, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E. Mini nutritional assessment. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Lundin, H.; Sääf, M.; Strender, L.E.; Mollasaraie, H.A.; Salminen, H. Mini nutritional assessment and 10-year mortality in free-living elderly women: A prospective cohort study with 10-year follow-up. Eur. J. Clin. Nutr. 2012, 66, 1050–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Chima, C.S.; Barco, K.; Dewitt, M.L.; Maeda, M.; Teran, J.; Mullen, K.D. Relationship of Nutritional Status to Length of Stay, Hospital Costs, and Discharge Status of Patients Hospitalized in the Medicine Service. J. Am. Diet. Assoc. 1997, 97, 975–978. [Google Scholar] [CrossRef] [PubMed]
- Gentile, S.; Lacroix, O.; Durand, A.C.; Cretel, E.; Alazia, M.; Sambuc, R.; Bonin-Guillaume, S. Malnutrition: A highly predictive risk factor of short-term mortality in elderly presenting to the emergency department. J. Nutr. Health Aging 2013, 17, 290–294. [Google Scholar] [CrossRef]
- Shidfar, F.; Babaii Darabkhani, P.; Yazdanpanah, L.; Karkheiran, S.; Noorollahi-Moghaddam, H.; Haghani, H. Assessment of nutritional status in patients with Parkinson’s disease and its relationship with severity of the disease. Med. J. Islam. Repub. Iran 2016, 30, 454. [Google Scholar]
- Bauer, J.M.; Kaiser, M.J.; Anthony, P.; Guigoz, Y.; Sieber, C.C. The Mini Nutritional Assessment—Its history; today’s practice; and future perspectives. Nutr. Clin. Pract. 2008, 23, 388–396. [Google Scholar] [CrossRef]
- Moonen, H.P.F.X.; Van Zanten, A.R.H. Bioelectric impedance analysis for body composition measurement and other potential clinical applications in critical illness. Curr. Opin. Crit. Care 2021, 27, 344–353. [Google Scholar] [CrossRef]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications; limitations; and opportunities. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef] [Green Version]
- Peacock, I.W.F. Use of Bioimpedance Vector Analysis in Critically Ill and Cardiorenal Patients. Contrib. Nephrol. 2010, 165, 226–235. [Google Scholar] [CrossRef] [Green Version]
- Niederer, L.E.; Miller, H.; Haines, K.L.; Molinger, J.; Whittle, J.; MacLeod, D.B.; McClave, S.A.; Wischmeyer, P.E. Prolonged progressive hypermetabolism during COVID-19 hospitalization undetected by common predictive energy equations. Clin. Nutr. ESPEN 2021, 45, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Alizadehsani, R.; Sani, Z.A.; Behjati, M.; Roshanzamir, Z.; Hussain, S.; Abedini, N.; Hasanzadeh, F.; Khosravi, A.; Shoeibi, A.; Roshanzamir, M.; et al. Risk factors prediction, clinical outcomes, and mortality in COVID-19 patients. J. Med. Virol. 2021, 93, 2307–2320. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, S.; Firoozi, D.; Dehghani, M.; Zare, M.; Mehrabi, Z.; Ghaseminasab-Parizi, M.; Masoumi, S.J. Evaluation of Nutritional Status of Intensive Care Unit COVID-19 Patients Based on the Nutritional Risk Screening 2002 Score. Int. J. Clin. Pract. 2022, 2022, 2448161. [Google Scholar] [CrossRef] [PubMed]
- Ting, T.H.Y.; Lo, T.H.M.; Lo, W.W.T.; Ding, Q.; Yuk, D.K.L.; Hui, E.; Tang, M.W.S. Inadequate energy and protein intake; underweight and malnutrition are associated with in-hospital mortality among COVID-19 rehabilitation patients during the omicron outbreak in Hong Kong. Aging Med. (Milton) 2022, 5, 204–210. [Google Scholar] [CrossRef]
- Vaezi, M.; Ravanshad, S.; Rad, M.A.; Zarrinfar, H.; Kabiri, M. The effect of synbiotic adjunct therapy on clinical and paraclinical outcomes in hospitalized COVID-19 patients: A randomized placebo-controlled trial. J. Med. Virol. 2023, 95, 28463. [Google Scholar] [CrossRef]
- Khani, N.; Soleimani, R.A.; Noorkhajavi, G.; Soleimani, A.A.; Abbasi, A.; Rad, A.H. Postbiotics as potential promising tools for SARS-CoV-2 disease adjuvant therapy. J. Appl. Microbiol. 2022, 132, 4097–4111. [Google Scholar] [CrossRef]
- Scarpellini, E.; Rinninella, E.; Basilico, M.; Colomier, E.; Rasetti, C.; Larussa, T.; Santori, P.; Abenavoli, L. From Pre- and Probiotics to Post-Biotics: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 19, 37. [Google Scholar] [CrossRef]
- Pimentel, R.F.W.; Silva, A.P.; Santana, A.I.C.; Silva, D.S.E.; Ramos, M.S.; Souza, M.C.; Suen, V.M.M.; Maduro, I.P.N.N.; Ribas Filho, D.; D’Oliveira Júnior, A.; et al. Effect of immuno-nutrition on serum levels of C-reactive protein and lymphocytes in patients with COVID-19: A ran-domized; controlled; double-blind clinical trial. Nutr. Hosp. 2022, 39, 20–26. [Google Scholar]
- Ruiz-León, A.M.; Lapuente, M.; Estruch, R.; Casas, R. Clinical Advances in Immuno-nutrition and Atherosclerosis: A Review. Front. Immunol. 2019, 10, 837. [Google Scholar] [CrossRef]
- Di Renzo, L.; Franza, L.; Monsignore, D.; Esposito, E.; Rio, P.; Gasbarrini, A.; Gambassi, G.; Cianci, R.; De Lorenzo, A. Vaccines; Microbiota and Immuno-nutrition: Food for Thought. Vaccines 2022, 10, 294. [Google Scholar] [CrossRef] [PubMed]
- Naghibi, T.; Shafigh, N.; Mazloomzadeh, S. Role of omega-3 fatty acids in the prevention of delirium in mechanically ventilated patients. J. Res. Med. Sci. 2020, 25, 10. [Google Scholar] [CrossRef] [PubMed]
- Reizine, F.; Lesouhaitier, M.; Gregoire, M.; Pinceaux, K.; Gacouin, A.; Maamar, A.; Painvin, B.; Camus, C.; Le Tulzo, Y.; Tattevin, P.; et al. SARS-CoV-2-Induced ARDS Associates with MDSC Expansion; Lymphocyte Dysfunction; and Arginine Shortage. J. Clin. Immunol. 2021, 41, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Fell, J.M. Control of systemic and local inflammation with transforming growth factor beta containing formulas. J. Parenter. Enteral. Nutr. 2005, 29, S126–S128. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IN COVID-19 pts (n = 34) | Control Group (n = 20) | p-Value | |
|---|---|---|---|
| Age (years) | 70.3 ± 5.4 | 68.0 ± 5.5 | NS |
| sex | 6 F | 8 F | 0.05 |
| BMI (kg/m2) | 27.0 ± 0.5 | 23.5 ± 0.6 | <0.05 |
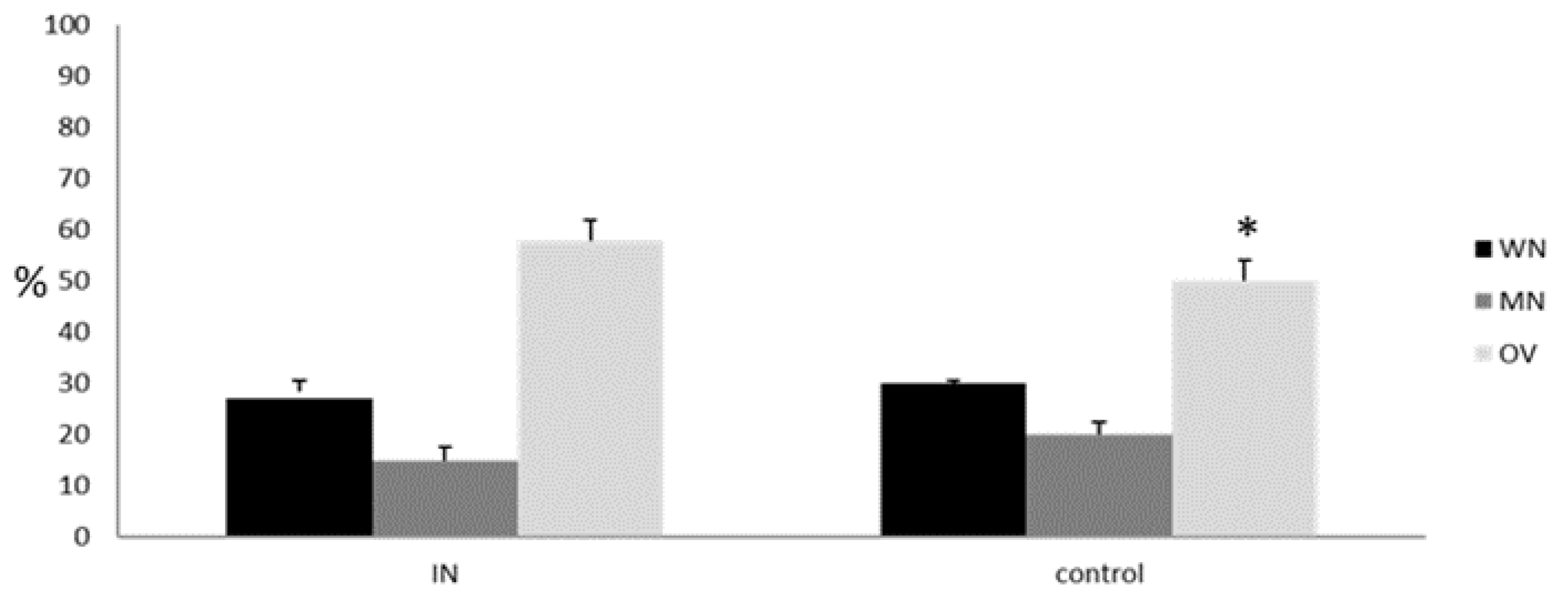
| MNA test (WN/MN/OV (%)) | 27/15/58 | 30/22/48 | <0.05 |
| PA (°) (WN/MN/OV) | 4.5/3.8/8.2 | 4.4/3.2/7.8 | <0.05 |
| CRP (mg/L) | 19 (5.6–31) | 20 (6–33) | NS |
| IL-6 (pg/mL) | 101 (35–133) | 103 (34–136) | NS |
| Semi-intensive unit stay (days) | 18.2 ± 0.4 | 18.6 ± 0.6 | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarcella, M.; Scarpellini, E.; Piergallini, S.; Rinninella, E.; Routhiaux, K.; Rasetti, C.; Abenavoli, L.; De Robertis, E.; Manzi, P.; Commissari, R.; et al. Effect of Immuno-Nutrition on Malnutrition, Inflammatory Response and Clinical Course of Semi-Critically Ill COVID-19 Patients: A Pilot Perspective Study. Nutrients 2023, 15, 1250. https://doi.org/10.3390/nu15051250
Scarcella M, Scarpellini E, Piergallini S, Rinninella E, Routhiaux K, Rasetti C, Abenavoli L, De Robertis E, Manzi P, Commissari R, et al. Effect of Immuno-Nutrition on Malnutrition, Inflammatory Response and Clinical Course of Semi-Critically Ill COVID-19 Patients: A Pilot Perspective Study. Nutrients. 2023; 15(5):1250. https://doi.org/10.3390/nu15051250
Chicago/Turabian StyleScarcella, Marialaura, Emidio Scarpellini, Sara Piergallini, Emanuele Rinninella, Karen Routhiaux, Carlo Rasetti, Ludovico Abenavoli, Edoardo De Robertis, Pietro Manzi, Rita Commissari, and et al. 2023. "Effect of Immuno-Nutrition on Malnutrition, Inflammatory Response and Clinical Course of Semi-Critically Ill COVID-19 Patients: A Pilot Perspective Study" Nutrients 15, no. 5: 1250. https://doi.org/10.3390/nu15051250