
Adverse Collateral Effects of COVID-19 Public Health Restrictions on Physical Fitness and Cognitive Performance in Primary School Children

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Design
2.2. Anthropometric Characteristics and Body Composition
2.3. Executive Function
2.4. Physical Fitness
2.4.1. Cardiorespiratory Fitness
2.4.2. Upper-Body Muscular Strength
2.4.3. Lower-Body Muscular Strength
2.5. Implicit Activity Preferences
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef]
- Fu, Y.; Brusseau, T.A.; Hannon, J.C.; Burns, R.D. Effect of a 12-Week Summer Break on School Day Physical Activity and Health-Related Fitness in Low-Income Children from CSPAP Schools. J. Environ. Public Health 2017, 2017, 9760817. [Google Scholar] [CrossRef]
- Jackson, C.; Vynnycky, E.; Mangtani, P. The Relationship Between School Holidays and Transmission of Influenza in England and Wales. Am. J. Epidemiol. 2016, 184, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Paterson, D.C.; Ramage, K.; Moore, S.A.; Riazi, N.; Tremblay, M.S.; Faulkner, G. Exploring the impact of COVID-19 on the movement behaviors of children and youth: A scoping review of evidence after the first year. J. Sport Health Sci. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.M.; Yunker, A.G.; DeFendis, A.; Xiang, A.H.; Page, K.A. Associations between Affect, Physical Activity, and Anxiety Among US Children During COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Carriedo, A.; Cecchini, J.A.; Fernández-Río, J.; Méndez-Giménez, A. Resilience and physical activity in people under home isolation due to COVID-19: A preliminary evaluation. Ment. Health Phys. Act. 2020, 19, 100361. [Google Scholar] [CrossRef] [PubMed]
- Chouchou, F.; Augustini, M.; Caderby, T.; Caron, N.; Turpin, N.A.; Dalleau, G. The importance of sleep and physical activity on well-being during COVID-19 lockdown: Reunion island as a case study. Sleep Med. 2021, 77, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Ugbolue, U.; Duclos, M.; Urzeala, C.; Berthon, M.; Kulik, K.; Bota, A.; Thivel, D.; Bagheri, R.; Gu, Y.; Baker, J.; et al. An Assessment of the Novel COVISTRESS Questionnaire: COVID-19 Impact on Physical Activity, Sedentary Action and Psychological Emotion. J. Clin. Med. 2020, 9, 3352. [Google Scholar] [CrossRef] [PubMed]
- Werneck, A.O.; Silva, D.R.; Malta, D.C.; Souza-Júnior, P.R.B.; Azevedo, L.O.; Barros, M.B.A.; Szwarcwald, C.L. Changes in the clustering of unhealthy movement behaviors during the COVID-19 quarantine and the association with mental health indicators among Brazilian adults. Transl. Behav. Med. 2021, 11, 323–331. [Google Scholar] [CrossRef]
- Wahl-Alexander, Z.; Camic, C.L. Impact of COVID-19 on School-Aged Male and Female Health-Related Fitness Markers. Pediatr. Exerc. Sci. 2021, 33, 61–64. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Andersen, L.L.; Casaña, J.; Ezzatvar, Y.; Casajús, J.A.; Smith, L. Cardiorespiratory fitness in adolescents before and after the COVID-19 confinement: A prospective cohort study. Eur. J. Pediatr. 2021, 180, 2287–2293. [Google Scholar] [CrossRef]
- Jarnig, G.; Jaunig, J.; van Poppel, M.N.M. Association of COVID-19 Mitigation Measures With Changes in Cardiorespiratory Fitness and Body Mass Index Among Children Aged 7 to 10 Years in Austria. JAMA Netw. Open 2021, 4, e2121675. [Google Scholar] [CrossRef]
- Fearnbach, S.N.; Martin, C.K.; Heymsfield, S.B.; Staiano, A.E.; Newton, R.L.; Garn, A.C.; Finlayson, G. Validation of the Activity Preference Assessment: A tool for quantifying children’s implicit preferences for sedentary and physical activities. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 108. [Google Scholar] [CrossRef] [PubMed]
- Appelhans, B.M.; Thomas, A.S.; Roisman, G.I.; Booth-LaForce, C.; Bleil, M.E. Preexisting Executive Function Deficits and Change in Health Behaviors During the COVID-19 Pandemic. Int. J. Behav. Med. 2021, in press. [Google Scholar] [CrossRef]
- Chetty, R.; Friedman, J.N.; Hendren, N.; Stepner, M. How Did COVID-19 and Stabilization Policies Affect Spending and Employment?: A New Real-Time Economic Tracker Based on Private Sector Data; National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- The DELVE Initiative, Balancing the Risks of Pupils Returning to Schools. 2020. Available online: https://rs-delve.github.io/reports/2020/07/24/balancing-the-risk-of-pupils-returning-to-schools.html (accessed on 15 September 2021).
- Engzell, P.; Frey, A.; Verhagen, M.D. Learning loss due to school closures during the COVID-19 pandemic. Proc. Natl. Acad. Sci. USA 2021, 118, e2022376118. [Google Scholar] [CrossRef] [PubMed]
- McGinty, E.E.; Presskreischer, R.; Anderson, K.E.; Han, H.; Barry, C.L. Psychological Distress and COVID-19–Related Stressors Reported in a Longitudinal Cohort of US Adults in April and July 2020. JAMA 2020, 324, 2555–2557. [Google Scholar] [CrossRef]
- Shields, G.S.; Sazma, M.A.; Yonelinas, A.P. The effects of acute stress on core executive functions: A meta-analysis and comparison with cortisol. Neurosci. Biobehav. Rev. 2016, 68, 651–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, R.J.; Krystal, J.H.; Mathalon, D.H. Working memory overload: Fronto-limbic interactions and effects on subsequent working memory function. Brain Imaging Behav. 2010, 4, 96–108. [Google Scholar] [CrossRef] [Green Version]
- Esteban-Cornejo, I.; Reilly, J.; Ortega, F.B.; Matusik, P.; Mazur, A.; Erhardt, E.; Thivel, D. Paediatric obesity and brain functioning: The role of physical activity-A novel and important expert opinion of the European Childhood Obesity Group. Pediatr. Obes. 2020, 15, e12649. [Google Scholar] [CrossRef]
- Valkenborghs, S.; Noetel, M.; Hillman, C.H.; Nilsson, M.; Smith, J.J.; Ortega, F.B.; Lubans, D.R. The Impact of Physical Activity on Brain Structure and Function in Youth: A Systematic Review. Pediatrics 2019, 144, e20184032. [Google Scholar] [CrossRef]
- Freedman, D.S.; Katzmarzyk, P.T.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. Relation of body mass index and skinfold thicknesses to cardiovascular disease risk factors in children: The Bogalusa Heart Study. Am. J. Clin. Nutr. 2009, 90, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thivel, D.; Verney, J.; Miguet, M.; Masurier, J.; Cardenoux, C.; Lambert, C.; Pereira, B. The accuracy of bioelectrical impedance to track body composition changes depends on the degree of obesity in adolescents with obesity. Nutr. Res. 2018, 54, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Verney, J.; Metz, L.; Chaplais, E.; Cardenoux, C.; Pereira, B.; Thivel, D. Bioelectrical impedance is an accurate method to assess body composition in obese but not severely obese adolescents. Nutr. Res. 2016, 36, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Armitage, S.G. An analysis of certain psychological tests used for the evaluation of brain injury. Psychol. Monogr. 1946, 60, i-48. [Google Scholar] [CrossRef]
- Reitan, R.M. Trail making test results for normal and brain-damaged children. Percept. Mot. Skills 1971, 33, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Léger, L.A.; Lambert, J. A maximal multistage 20-m shuttle run test to predict VO2 max. Eur. J. Appl. Physiol. Occup. Physiol. 1982, 49, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Leger, L.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre Shuttle Run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C. Validation of two running tests as estimates of maximal aerobic power in children. Eur. J. Appl. Physiol. Occup. Physiol. 1986, 55, 503–506. [Google Scholar] [CrossRef]
- Mahar, M.T.; Rowe, D.A.; Parker, C.R.; Mahar, F.J.; Dawson, D.M.; Holt, J.E. Criterion-Referenced and Norm-Referenced Agreement Between the Mile Run/Walk and PACER. Meas. Phys. Educ. Exerc. Sci. 1997, 1, 245–258. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Aguilar-Soto, P.; Viciana, J. Criterion-Related Validity of the 20-M Shuttle Run Test for Estimating Cardiorespiratory Fitness: A Meta-Analysis. J. Sports Sci. Med. 2015, 14, 536–547. [Google Scholar]
- Beets, M.W.; Pitetti, K. Criterion-Referenced Reliability and Equivalency Between the PACER and 1-Mile Run/Walk for High School Students. J. Phys. Act. Health 2006, 3, S21–S33. [Google Scholar] [CrossRef]
- Ortega, F.B.; Artero, E.G.; Ruiz, J.R.; Vicente-Rodriguez, G.; Bergman, P.; Hagströmer, M.; Ottevaere, C.; Nagy, E.; Konsta, O.; Rey-Lopez, J.P.; et al. Reliability of health-related physical fitness tests in European adolescents. The HELENA Study. Int. J. Obes. 2008, 32, S49–S57. [Google Scholar] [CrossRef] [Green Version]
- Fernandez Santos, J.R.; Ruiz, J.R.; Gonzalez-Montesinos, J.L.; Castro-Piñero, J. Reliability and Validity of Field-Based Tests to Assess Upper-Body Muscular Strength in Children Aged 6–12 Years. Pediatr. Exerc. Sci. 2016, 28, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Kidokoro, T.; Edamoto, K. Improvements in Physical Fitness are Associated with Favorable Changes in Blood Lipid Concentrations in Children. J. Sports Sci. Med. 2021, 20, 404–412. [Google Scholar] [CrossRef]
- Holsgaard Larsen, A.; Caserotti, P.; Puggaard, L.; Aagaard, P. Reproducibility and relationship of single-joint strength vs. multi-joint strength and power in aging individuals. Scand. J. Med. Sci. Sports 2007, 17, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.H.; Cimbolic, K.; Armeli, S.R.; Hettler, T.R. Quantitative Assessment of Thriving. J. Soc. Issues 1998, 54, 323–335. [Google Scholar] [CrossRef]
- Altman, D.G. Statistics in the medical literature: 3. Stat. Med. 1999, 18, 487–490. [Google Scholar] [CrossRef]
- Chambonniere, C.; Lambert, C.; Fearnbach, N.; Tardieu, M.; Fillon, A.; Genin, P.; Larras, B.; Melsens, P.; Bois, J.; Pereira, B.; et al. Effect of the COVID-19 lockdown on physical activity and sedentary behaviors in French children and adolescents: New results from the ONAPS national survey. Eur. J. Integr. Med. 2021, 43, 101308. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Olds, T.S. Secular changes in pediatric aerobic fitness test performance: The global picture. Med. Sport Sci. 2007, 50, 46–66. [Google Scholar] [PubMed]
- Flanagan, E.W.; Beyl, R.A.; Fearnbach, S.N.; Altazan, A.D.; Martin, C.K.; Redman, L.M. The Impact of COVID-19 Stay-At-Home Orders on Health Behaviors in Adults. Obesity 2021, 29, 438–445. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| T0 | T1 | |||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p | ES | |
| Weight (kg) | 32.96 | 8.71 | 35.13 | 10.26 | 0.1862 | −0.22 [−0.56; 0.11] |
| BMI (kg/m2) | 17.23 | 3.51 | 18.20 | 3.94 | 0.1425 | −0.25 [−0.59; 0.09] |
| FM (%) | 24.23 | 7.20 | 24.41 | 6.85 | 0.9031 | −0.02 [−0.42; 0.37] |
| CMJ (cm) | 18.01 | 4.60 | 17.36 | 3.51 | 0.3213 | 0.15 [−0.15; 0.46] |
| SBJ (cm) | 169.87 | 142.57 | 135.23 | 31.40 | 0.0367 | 0.33 [0.01; 0.64] |
| Handgrip (N) | 14.30 | 3.54 | 14.02 | 3.04 | 0.5892 | 0.08 [−0.22; 0.39] |
| TMB (cm) | 297.28 | 81.11 | 249.06 | 52.13 | <0.0001 | 0.70 [0.38; 1.01] |
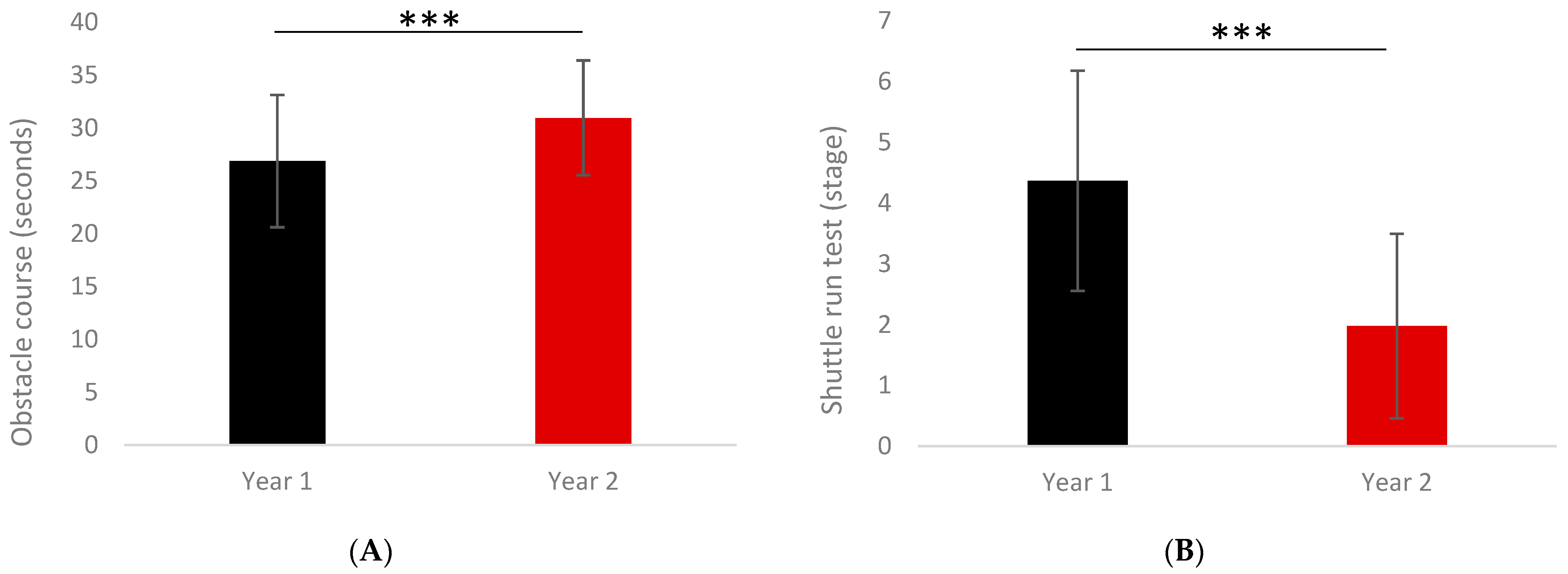
| Motor skills (s) | 26.88 | 6.26 | 30.97 | 5.43 | <0.0001 | −0.69 [−1.01; −0.37] |
| MAS (km/h) | 9.68 | 0.90 | 9.00 | 0.75 | <0.0001 | 0.80 [0.48; 1.12] |
| VO2max (mL/min/kg) | 45.66 | 4.25 | 43.05 | 3.69 | <0.0001 | 0.65 [0.33; 0.96] |
| Shuttle run stage | 4.37 | 1.81 | 1.98 | 1.52 | <0.0001 | 1.41 [1.06; 1.75] |
| TMT-A (s) | 79.69 | 26.47 | 95.60 | 32.36 | 0.0009 | −0.53 [−0.85; −0.22] |
| TMT-B (s) | 154.43 | 62.95 | 186.44 | 54.63 | 0.0008 | −0.53 [−0.85; −0.22] |
| TMT-Tot (s) | 234.12 | 77.90 | 293.24 | 80.98 | <0.0001 | −0.74 [−1.05; −0.41] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chambonnière, C.; Fearnbach, N.; Pelissier, L.; Genin, P.; Fillon, A.; Boscaro, A.; Bonjean, L.; Bailly, M.; Siroux, J.; Guirado, T.; et al. Adverse Collateral Effects of COVID-19 Public Health Restrictions on Physical Fitness and Cognitive Performance in Primary School Children. Int. J. Environ. Res. Public Health 2021, 18, 11099. https://doi.org/10.3390/ijerph182111099
Chambonnière C, Fearnbach N, Pelissier L, Genin P, Fillon A, Boscaro A, Bonjean L, Bailly M, Siroux J, Guirado T, et al. Adverse Collateral Effects of COVID-19 Public Health Restrictions on Physical Fitness and Cognitive Performance in Primary School Children. International Journal of Environmental Research and Public Health. 2021; 18(21):11099. https://doi.org/10.3390/ijerph182111099
Chicago/Turabian StyleChambonnière, Camille, Nicole Fearnbach, Léna Pelissier, Pauline Genin, Alicia Fillon, Audrey Boscaro, Line Bonjean, Mélina Bailly, Julie Siroux, Terry Guirado, and et al. 2021. "Adverse Collateral Effects of COVID-19 Public Health Restrictions on Physical Fitness and Cognitive Performance in Primary School Children" International Journal of Environmental Research and Public Health 18, no. 21: 11099. https://doi.org/10.3390/ijerph182111099