
Use of Quantitative Dried Blood Spots to Evaluate the Post-Vaccination Level of Neutralizing Antibodies against SARS-CoV-2


Abstract
:1. Introduction
2. Material and Methods
2.1. Blood Samples
2.2. Sample Preparation
2.3. SARS-CoV-2 S Immunoassay
2.4. Data Interpretation
2.5. Adaptation of the Elecsys® Anti-SARS-CoV-2 S Immunoassay to DBS
2.6. Clinical Study Performed to Follow the Development and Stability of the Antibodies Produced after Vaccination against SARS-CoV-2
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheng, H.; Peng, Z.; Luo, W.; Si, S.; Mo, M.; Zhou, H.; Xin, X.; Liu, H.; Yu, Y. Efficacy and Safety of COVID-19 Vaccines in Phase III Trials: A Meta-Analysis. Vaccines 2021, 9, 582. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Zeng, J.; Yan, J. COVID-19 mRNA vaccines. J. Genet Genom. 2021, 48, 107–114. [Google Scholar] [CrossRef]
- Secchi, M.; Bazzigaluppi, E.; Brigatti, C.; Marzinotto, I.; Tresoldi, C.; Rovere-Querini, P.; Poli, A.; Castagna, A.; Scarlatti, G.; Zangrillo, A.; et al. COVID-19 survival associates with the immunoglobulin response to the SARS-CoV-2 spike receptor binding domain. J. Clin. Investig. 2020, 130, 6366–6378. [Google Scholar] [CrossRef] [PubMed]
- Dispinseri, S.; Secchi, M.; Pirillo, M.F.; Tolazzi, M.; Borghi, M.; Brigatti, C.; De Angelis, M.L.; Baratella, M.; Bazzigaluppi, E.; Venturi, G.; et al. Neutralizing antibody responses to SARS-CoV-2 in symptomatic COVID-19 is persistent and critical for survival. Nat. Commun. 2021, 12, 2670. [Google Scholar] [CrossRef] [PubMed]
- Chia, W.N.; Zhu, F.; Ong, S.W.X.; Young, B.E.; Fong, S.W.; Le Bert, N.; Tan, C.W.; Tiu, C.; Zhang, J.; Tan, S.Y.; et al. Dynamics of SARS-CoV-2 neutralising antibody responses and duration of immunity: A longitudinal study. Lancet Microbe 2021, 2, e240–e249. [Google Scholar] [CrossRef]
- Tea, F.; Ospina Stella, A.; Aggarwal, A.; Ross Darley, D.; Pilli, D.; Vitale, D.; Merheb, V.; Lee, F.X.Z.; Cunningham, P.; Walker, G.J.; et al. SARS-CoV-2 neutralizing antibodies: Longevity, breadth, and evasion by emerging viral variants. PLoS Med. 2021, 18, e1003656. [Google Scholar] [CrossRef]
- Misset, B.; Hoste, E.; Donneau, A.F.; Grimaldi, D.; Meyfroidt, G.; Moutschen, M.; Compernolle, V.; Gothot, A.; Desmecht, D.; Garigliany, M.; et al. A multicenter randomized trial to assess the efficacy of CONvalescent plasma therapy in patients with Invasive COVID-19 and acute respiratory failure treated with mechanical ventilation: The CONFIDENT trial protocol. BMC Pulm Med. 2020, 20, 317. [Google Scholar] [CrossRef]
- Callegaro, A.; Borleri, D.; Farina, C.; Napolitano, G.; Valenti, D.; Rizzi, M.; Maggiolo, F. Antibody response to SARS-CoV-2 vaccination is extremely vivacious in subjects with previous SARS-CoV-2 infection. J. Med. Virol. 2021, 93, 4612–4615. [Google Scholar] [CrossRef]
- Tan, E.; Frew, E.; Cooper, J.; Humphrey, J.; Holden, M.; Mand, A.R.; Li, J.; Anderson, S.; Bi, M.; Hatler, J.; et al. Use of Lateral Flow Immunoassay to Characterize SARS-CoV-2 RBD-Specific Antibodies and Their Ability to React with the UK, SA and BR P.1 Variant RBDs. Diagnostics 2021, 11, 1190. [Google Scholar] [CrossRef]
- Sekirov, I.; Barakauskas, V.E.; Simons, J.; Cook, D.; Bates, B.; Burns, L.; Masud, S.; Charles, M.; McLennan, M.; Mak, A.; et al. SARS-CoV-2 serology: Validation of high-throughput chemiluminescent immunoassay (CLIA) platforms and a field study in British Columbia. J. Clin. Virol. 2021, 142, 104914. [Google Scholar] [CrossRef]
- Yel, L.; Rabbat, C.J.; Cunningham-Rundles, C.; Orange, J.S.; Torgerson, T.R.; Verbsky, J.W.; Wang, Y.; Fu, M.; Robins, T.S.; Edwards, M.S.; et al. A Novel Targeted Screening Tool for Hypogammaglobulinemia: Measurement of Serum Immunoglobulin (IgG, IgM, IgA) Levels from Dried Blood Spots (Ig-DBS Assay). J. Clin. Immunol. 2015, 35, 573–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velghe, S.; Delahaye, L.; Stove, C.P. Is the hematocrit still an issue in quantitative dried blood spot analysis? J. Pharm. Biomed. Anal. 2019, 163, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Roxhed, N.; Bendes, A.; Dale, M.; Mattsson, C.; Hanke, L.; Dodig-Crnkovic, T.; Christian, M.; Meineke, B.; Elsasser, S.; Andrell, J.; et al. Multianalyte serology in home-sampled blood enables an unbiased assessment of the immune response against SARS-CoV-2. Nat. Commun. 2021, 12, 3695. [Google Scholar] [CrossRef] [PubMed]
- Elecsys® Anti-SARS-CoV-2 S Immunoassay for the Quantitative Determination of Antibodies to the SARS-CoV-2 Spike Protein. 2021. Available online: https://diagnostics.roche.com/global/en/products/params/elecsys-anti-SARS-CoV-2-s.html (accessed on 10 October 2021).
- McAndrews, K.M.; Dowlatshahi, D.P.; Dai, J.; Becker, L.M.; Hensel, J.; Snowden, L.M.; Leveille, J.M.; Brunner, M.R.; Holden, K.W.; Hopkins, N.S.; et al. Heterogeneous antibodies against SARS-CoV-2 spike receptor binding domain and nucleocapsid with implications for COVID-19 immunity. JCI Insight 2020, 5, e142386. [Google Scholar] [CrossRef]
- Case, J.B.; Rothlauf, P.W.; Chen, R.E.; Liu, Z.; Zhao, H.; Kim, A.S.; Bloyet, L.M.; Zeng, Q.; Tahan, S.; Droit, L.; et al. Neutralizing Antibody and Soluble ACE2 Inhibition of a Replication-Competent VSV-SARS-CoV-2 and a Clinical Isolate of SARS-CoV-2. Cell Host Microbe 2020, 28, 475–485.e5. [Google Scholar] [CrossRef]
- Meyer, B.; Torriani, G.; Yerly, S.; Mazza, L.; Calame, A.; Arm-Vernez, I.; Zimmer, G.; Agoritsas, T.; Stirnemann, J.; Spechbach, H.; et al. Validation of a commercially available SARS-CoV-2 serological immunoassay. Clin. Microbiol. Infect. 2020, 26, 1386–1394. [Google Scholar] [CrossRef]
- Marchand, A.; Roulland, I.; Semence, F.; Ericsson, M. Adaptation of Elecsys((R)) anti-severe acute respiratory syndrome coronavirus-2 immunoassay to dried blood spots: Proof of concept. Bioanalysis 2021, 13, 161–167. [Google Scholar] [CrossRef]
- Morley, G.L.; Taylor, S.; Jossi, S.; Perez-Toledo, M.; Faustini, S.E.; Marcial-Juarez, E.; Shields, A.M.; Goodall, M.; Allen, J.D.; Watanabe, Y.; et al. Sensitive Detection of SARS-CoV-2-Specific Antibodies in Dried Blood Spot Samples. Emerg Infect. Dis. 2020, 26, 2970–2973. [Google Scholar] [CrossRef]
- Thevis, M.; Knoop, A.; Schaefer, M.S.; Dufaux, B.; Schrader, Y.; Thomas, A.; Geyer, H. Can dried blood spots (DBS) contribute to conducting comprehensive SARS-CoV-2 antibody tests? Drug Test Anal. 2020, 12, 994–997. [Google Scholar] [CrossRef]
- Toh, Z.Q.; Higgins, R.A.; Anderson, J.; Mazarakis, N.; Do, L.A.H.; Rautenbacher, K.; Ramos, P.; Dohle, K.; Tosif, S.; Crawford, N.; et al. The use of dried blood spots for the serological evaluation of SARS-CoV-2 antibodies. J. Public Health (Oxf.) 2021, 1–4, online ahead of print. [Google Scholar] [CrossRef]
- Beyerl, J.; Rubio-Acero, R.; Castelletti, N.; Paunovic, I.; Kroidl, I.; Khan, Z.N.; Bakuli, A.; Tautz, A.; Oft, J.; Hoelscher, M.; et al. A dried blood spot protocol for high throughput analysis of SARS-CoV-2 serology based on the Roche Elecsys anti-N assay. EBioMedicine 2021, 70, 103502. [Google Scholar] [CrossRef]
- Sancilio, A.E.; D’Aquila, R.T.; McNally, E.M.; Velez, M.P.; Ison, M.G.; Demonbreun, A.R.; McDade, T.W. A surrogate virus neutralization test to quantify antibody-mediated inhibition of SARS-CoV-2 in finger stick dried blood spot samples. Sci. Rep. 2021, 11, 15321. [Google Scholar] [CrossRef]
- Turgeon, C.T.; Sanders, K.A.; Granger, D.; Nett, S.L.; Hilgart, H.; Matern, D.; Theel, E.S. Detection of SARS-CoV-2 IgG antibodies in dried blood spots. Diagn. Microbiol. Infect. Dis. 2021, 101, 115425. [Google Scholar] [CrossRef]
- Brinc, D.; Biondi, M.J.; Li, D.; Sun, H.; Capraru, C.; Smookler, D.; Zahoor, M.A.; Casey, J.; Kulasingam, V.; Feld, J.J. Evaluation of Dried Blood Spot Testing for SARS-CoV-2 Serology Using a Quantitative Commercial Assay. Viruses 2021, 13, 962. [Google Scholar] [CrossRef]
- Higgins, V.; Fabros, A.; Kulasingam, V. Quantitative Measurement of Anti-SARS-CoV-2 Antibodies: Analytical and Clinical Evaluation. J. Clin. Microbiol. 2021, 59, e03149-20. [Google Scholar] [CrossRef]
- Cavalcanti, E.; Isgro, M.A.; Rea, D.; Di Capua, L.; Trillo, G.; Russo, L.; Botti, G.; Miscio, L.; Buonaguro, F.M.; Bianchi, A.A.M. Vaccination strategy and anti-SARS-CoV-2 S titers in healthcare workers of the INT-IRCCS “Fondazione Pascale” Cancer Center (Naples, Italy). Infect Agent Cancer 2021, 16, 32. [Google Scholar] [CrossRef]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Marculescu, R.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Anti-Spike Protein Assays to Determine SARS-CoV-2 Antibody Levels: A Head-to-Head Comparison of Five Quantitative Assays. Microbiol. Spectr. 2021, 9, e0024721. [Google Scholar] [CrossRef]
- Lo Sasso, B.; Giglio, R.V.; Vidali, M.; Scazzone, C.; Bivona, G.; Gambino, C.M.; Ciaccio, A.M.; Agnello, L.; Ciaccio, M. Evaluation of Anti-SARS-CoV-2 S-RBD IgG Antibodies after COVID-19 mRNA BNT162b2 Vaccine. Diagnostics 2021, 11, 1135. [Google Scholar] [CrossRef]
- Muller, L.; Andree, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 COVID-19 vaccination. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Furlong, A.; Deutsch, J. A Country-by-Country Guide to Coronavirus Vaccine Booster Plans. 2021. Available online: https://www.politico.eu/article/vaccine-booster-coronavirus-COVID-19-europe-delta-varian-who/ (accessed on 10 October 2021).
- Singapore Ministry of Health. Expert Committee on COVID-19 Vaccination Recommends an Additional Dose of Mrna COVID-19 Vaccine for Immunocompromised and Seniors. Available online: https://www.moh.gov.sg/news-highlights/details/expert-committee-on-COVID-19-vaccination-recommends-an-additional-dose-of-mrna-COVID-19-vaccine-for-immunocompromised-and-seniors_3Sep2021 (accessed on 10 October 2021).
- Weisblum, Y.; Schmidt, F.; Zhang, F.; DaSilva, J.; Poston, D.; Lorenzi, J.C.; Muecksch, F.; Rutkowska, M.; Hoffmann, H.H.; Michailidis, E.; et al. Escape from neutralizing antibodies by SARS-CoV-2 spike protein variants. eLife 2020, 9, e61312. [Google Scholar] [CrossRef]
- Wang, Z.; Schmidt, F.; Weisblum, Y.; Muecksch, F.; Barnes, C.; Finkin, S.; Muecksch, F.; Schaefer-Babajew, D.; Cipola, M.; Gaebler, C.; et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nature 2021, 592, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Tretyn, A.; Szczepanek, J.; Skorupa, M.; Jarkiewicz-Tretyn, J.; Sandomierz, D.; Dejewska, J.; Ciechanowska, K.; Jarkiewicz-Tretyn, A.; Koper, W.; Palgan, K.; et al. Differences in the concentration of Anti-SARS-CoV-2 IgG Post-COVID-19 recovery or Post-Vaccination. Cells 2021, 10, 1952. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plasma Values (U/mL) | DBS Results | Day 1 | Day 2 | Day 5 | Day 8 | Day 13 | Day 13/ Day 1 (%) |
|---|---|---|---|---|---|---|---|
| C1: 14.8 | C1 | 0.477 | 0.426 | <0.400 | <0.400 | <0.400 | |
| 0.439 | 0.414 | 0.431 | <0.400 | <0.400 | |||
| 0.417 | 0.416 | <0.400 | |||||
| 0.445 | 0.453 | 0.415 | |||||
| mean | 0.445 | 0.427 | 0.411 | <0.400 | <0.400 | ND | |
| CV% | 5.6% | 4.2% | ND | ND | ND | ||
| C3: 129.1 | C3 | 2.99 | 3.21 | 2.84 | 2.76 | 2.85 | |
| 3.17 | 3.32 | 2.89 | 2.89 | 2.84 | |||
| 3.15 | 3.18 | 2.94 | |||||
| 3.14 | 3.22 | 2.92 | |||||
| mean | 3.11 | 3.233 | 2.898 | 2.825 | 2.845 | 91.4% | |
| CV% | 2.7% | 1.9% | 1.5% | 3.3% | 3.2% | ||
| C4: 59.8 | C4 | 1.680 | 1.63 | 1.52 | 1.66 | 1.49 | |
| 1.560 | 1.64 | 1.53 | 1.47 | 1.46 | |||
| 1.600 | 1.59 | 1.44 | |||||
| 1.650 | 1.58 | 1.55 | |||||
| mean | 1.623 | 1.610 | 1.510 | 1.565 | 1.475 | 90.9% | |
| CV% | 3.3% | 1.8% | 3.2% | 8.6% | 1.4% |
| Test before Vaccination | 2 Weeks after First Dose (Pfizer) | Fold Plasma/Capitainer | 4 Weeks after First Dose | Fold Plasma/Capitainer | 4 Weeks after First Dose | Fold Plasma/Capitainer | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CODE | Plasma | DBS | Plasma | DBS | Plasma | DBS | Plasma | DBS | |||
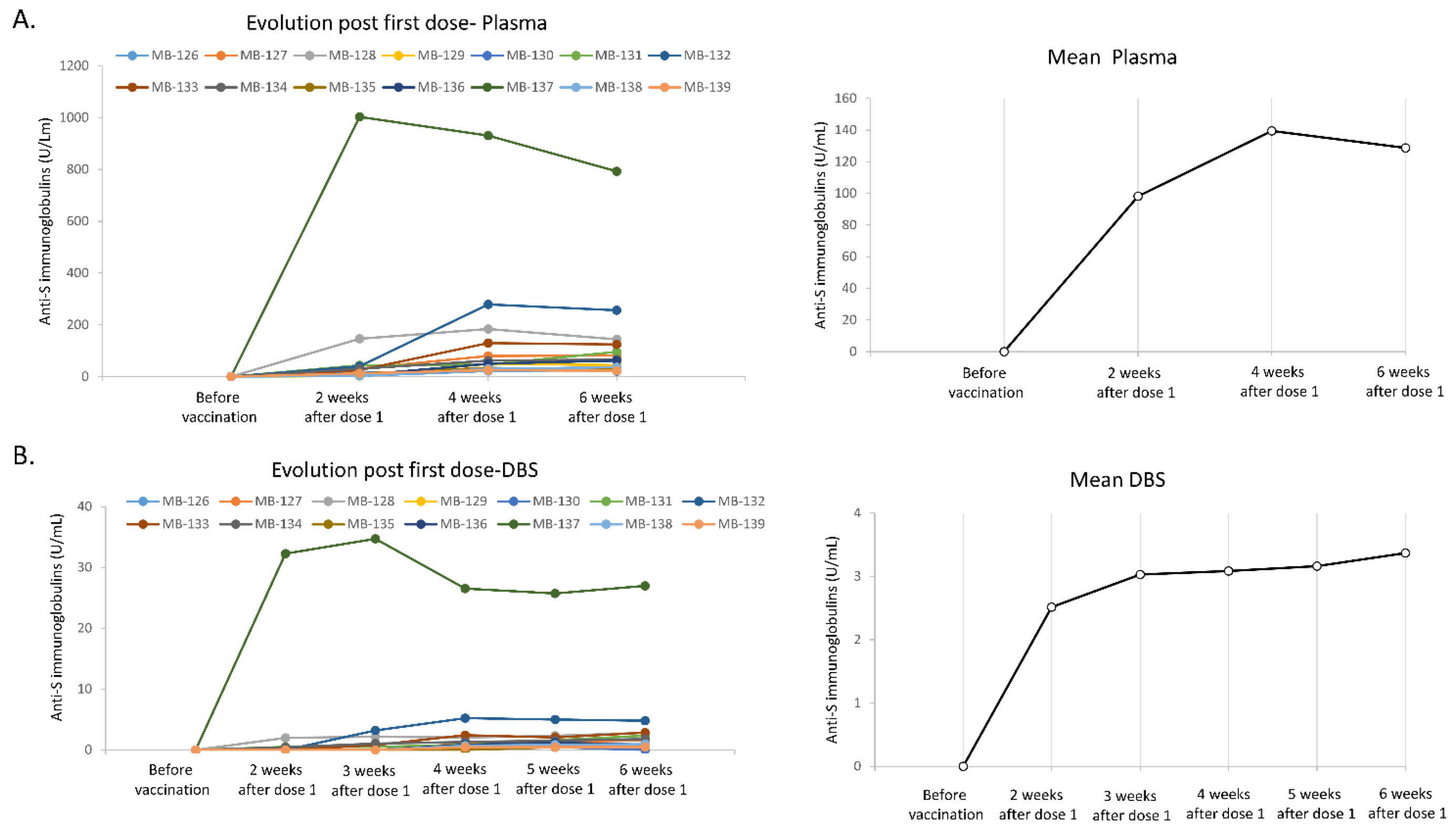
| MB-126 | <0.4 | <0.4 | 3.52 | <0.4 | 22.15 | 0.441 | 50.2 | 26.16 | 0.54 | 48.4 | |
| MB-127 | <0.4 | <0.4 | 30.9 | <0.4 | 80.14 | 1.03 | 77.8 | 81.77 | 1.55 | 52.8 | |
| MB-128 | <0.4 | <0.4 | 146.7 | 1.99 | 73.7 | 183.7 | 2.04 | 90.0 | 144.1 | 2.8 | 51.5 |
| MB-129 | <0.4 | <0.4 | 2.69 | <0.4 | 49.58 | 0.922 | 53.8 | 44.47 | 0.793 | 56.1 | |
| MB-130 | <0.4 | <0.4 | 14.45 | <0.4 | 29.94 | 0.466 | 64.2 | 21.42 | <0.4 | ND | |
| MB-131 | <0.4 | <0.4 | 43.82 | 0.494 | 88.7 | 46.93 | 0.832 | 56.4 | 95.88 | 2.32 | 41.3 |
| MB-132 | <0.4 | <0.4 | 39.94 | <0.4 | 279.3 | 5.23 | 53.4 | 256.4 | 4.81 | 53.3 | |
| MB-133 | <0.4 | <0.4 | 25.2 | <0.4 | 129.6 | 2.42 | 53.6 | 124.8 | 2.85 | 43.8 | |
| MB-134 | <0.4 | <0.4 | 30.24 | 0.44 | 68.7 | 62.05 | 1.31 | 47.4 | 65.47 | 1.78 | 36.8 |
| MB-135 | <0.4 | <0.4 | 12.15 | <0.4 | 33.85 | <0.4 | ND | 28.94 | 0.463 | 62.5 | |
| MB-136 | <0.4 | <0.4 | 5.86 | <0.4 | 49.88 | 0.844 | 59.1 | 61.65 | 0.894 | 69.0 | |
| MB-137 | <0.4 | <0.4 | 1003 | 32.27 | 31.1 | 930.8 | 26.53 | 35.1 | 793 | 26.98 | 29.4 |
| MB-138 | <0.4 | <0.4 | 3.21 | <0.4 | 30.6 | 0.698 | 43.8 | 36.3 | 0.95 | 38.2 | |
| MB-139 | <0.4 | <0.4 | 13.25 | <0.4 | 24.92 | 0.442 | 56.4 | 22.76 | 0.456 | 49.9 | |
| 1 Week after Dose 2 | 2 Weeks after Dose 2 | Fold Plasma/DBS | 3 Weeks after Dose 2 | 4 Weeks after Dose 2 | Fold Plasma/DBS | 5 Weeks after Dose 2 | 6 Weeks after Dose 2 | Fold Plasma/ DBS | 2 Months after Dose 2 | Fold Plasma/ DBS | 3 Months after Dose 2 | Fold Plasma/ DBS | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CODE | DBS | Plasma | DBS | DBS | Plasma | DBS | DBS | Plasma | DBS | Plasma | DBS | Plasma | DBS | |||||
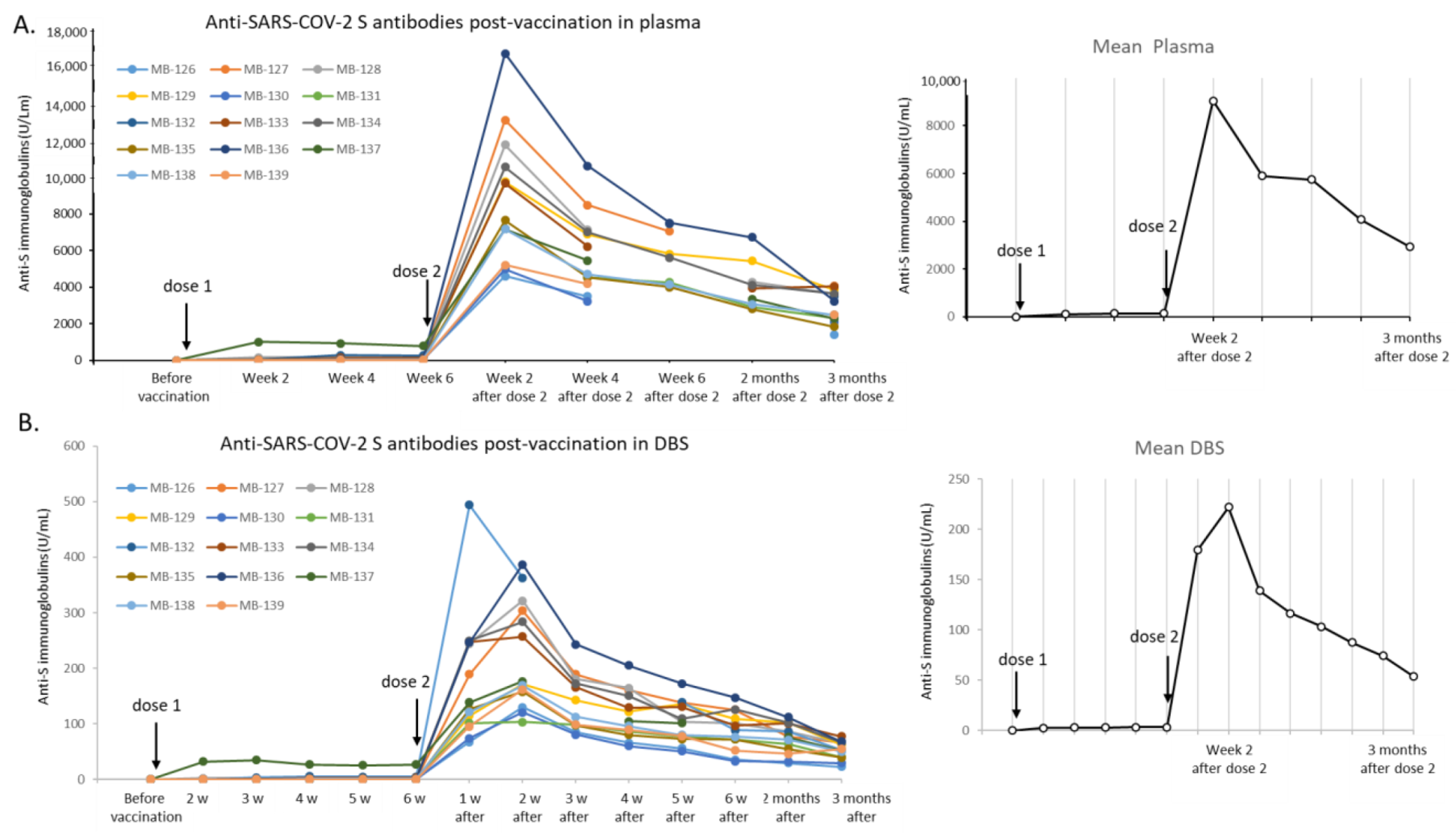
| MB-126 | 67.1 | 4605 | 129.7 | 35.5 | 85.3 | 3505 | 66.4 | 52.8 | 56.0 | 35.7 | ND | 29.3 | ND | 1418 | 22.6 | 62.7 | ||
| MB-127 | 188.9 | 13,149 | 304.0 | 43.3 | 189.2 | 8498 | 160.3 | 53.0 | 137.8 | 7055 | 125.2 | 56.3 | 77.5 | ND | 4055 | 66.9 | 60.6 | |
| MB-128 | 244.5 | 11,800 | 321.9 | 36.7 | 180.8 | 7135 | 164.6 | 43.3 | 104.3 | 101.5 | ND | 4290 | 86.9 | 49.4 | 3662 | 64.0 | 56.4 | |
| MB-129 | 114.7 | 9765 | 171.2 | 57.0 | 142.8 | 6900 | 122.0 | 56.6 | 135.1 | 5830 | 109.6 | 53.2 | 5440 | 102.5 | 53.1 | 3856 | 63.0 | 61.3 |
| MB-130 | 74.1 | 4988 | 120.8 | 41.3 | 80.4 | 3230 | 60.4 | 53.5 | 50.8 | 32.6 | ND | 32.3 | ND | 2101 | 29.4 | 71.6 | ||
| MB-131 | 101.3 | 103.6 | ND | 98.2 | 4541 | 86.4 | 52.5 | 76.9 | 4258 | 72.4 | 58.8 | 2925 | 64.1 | 45.6 | 2329 | 40.4 | 57.7 | |
| MB-132 | 494.3 | 362.9 | ND | ND | 139.5 | 7465 | 88.5 | 53.1 | 86.0 | ND | 3506 | 53.6 | 65.4 | |||||
| MB-133 | 247.9 | 9685 | 256.8 | 37.7 | 165.8 | 6235 | 129.4 | 48.2 | 130.7 | 96.9 | ND | 3940 | 100.4 | 39.2 | 4033 | 77.6 | 52.0 | |
| MB-134 | 249.5 | 10,583 | 283.7 | 37.3 | 172.4 | 7012 | 150.5 | 46.6 | 109.1 | 5627 | 126 | 44.7 | 4120 | 102.0 | 40.4 | 3639 | 66.4 | 54.8 |
| MB-135 | 126.9 | 7665 | 158.2 | 48.5 | 97.4 | 4532 | 79.8 | 56.8 | 72.7 | 3998 | 72.0 | 55.5 | 2815 | 54.9 | 51.3 | 1845 | 39.5 | 46.8 |
| MB-136 | 246.8 | 16,785 | 387.2 | 43.4 | 243.4 | 10,635 | 205.1 | 51.9 | 172.8 | 7526 | 147.5 | 51.0 | 6732 | 112.0 | 60.1 | 3228 | 68.2 | 47.3 |
| MB-137 | 138.3 | 7172 | 176.9 | 40.5 | 5465 | 104.6 | 52.2 | 101.2 | ND | 3353 | 76.2 | 44.0 | 2290 | 52.3 | 43.8 | |||
| MB-138 | 121.0 | 7185 | 169.2 | 42.5 | 113 | 4714 | 96.2 | 49.0 | 80.3 | 4153 | 76.6 | 54.2 | 3080 | 71.2 | 43.3 | 2491 | 50.0 | 49.8 |
| MB-139 | 95.5 | 5213 | 161.8 | 32.2 | 98.4 | 4178 | 89.4 | 46.7 | 77.8 | 52.3 | ND | 45.9 | ND | 2490 | 55.0 | 45.3 | ||
| Mean | 179.3 | 9049.4 | 222.0 | 41.3 | 138.9 | 5890.7 | 116.5 | 51.0 | 103.2 | 5738.8 | 87.4 | 53.4 | 4077.2 | 74.4 | 47.4 | 2925 | 53.5 | 55.4 |
| PFIZER VACCINE | 7 Weeks after Dose 2 | 3 Months after Dose 2 | ||||
|---|---|---|---|---|---|---|
| Hospitalized for COVID-19 in November 2020-Final vaccination March 2021 (dose 2) | Plasma | DBS | Fold Plasma/DBS | Plasma | DBS | Fold Plasma/DBS |
| 100 166 | 1817 | 55.1 | 47 710 | 944.7 | 50.5 | |
| PFIZER VACCINE Final vaccination April 2021 | 5 Weeks after Dose 2 | 3 Months after Dose 2 | ||||
| Plasma | DBS | Fold Plasma/DBS | Plasma | DBS | Fold Plasma/DBS | |
| 4987 | 91.38 | 54.6 | 2854.5 | 50.24 | 56.8 | |
| ASTRAZENECA VACCINE Final vaccination June 2021 | 3 Weeks after Dose 2 | 5 Weeks after Dose 2 | ||||
| DBS | DBS | |||||
| 45.3 | 37.94 | |||||
| ASTRAZENECA VACCINE Final vaccination July 2021 | 1 Day after Dose 2 | 3 Weeks after Dose 2 | ||||
| DBS | DBS | |||||
| 0.822 | 88.24 | |||||
| JANSSEN VACCINE Final vaccination May 2021 | 7 Weeks after the Dose | |||||
| DBS | ||||||
| 1.96 | ||||||
| Sex | Age | Sample Number | Plasma | DBS | Fold Change Plasma/DBS |
|---|---|---|---|---|---|
| F | 85 | 4 | <0.4 | <0.4 | ND |
| M | 32 | 6 | <0.4 | <0.4 | ND |
| M | 39 | 7 | <0.4 | <0.4 | ND |
| F | 76 | 38 | <0.4 | <0.4 | ND |
| F | 18 | 12 | <0.4 | <0.4 | ND |
| F | 10 | 39 | <0.4 | <0.4 | ND |
| F | 15 | 20 | <0.4 | <0.4 | ND |
| M | 48 | 40 | <0.4 | <0.4 | ND |
| M | 33 | 23 | <0.4 | <0.4 | ND |
| M | 13 | 57 | <0.4 | <0.4 | ND |
| M | 77 | 60 | <0.4 | <0.4 | ND |
| M | 73 | 70 | <0.4 | <0.4 | ND |
| F | 59 | 74 | <0.4 | <0.4 | ND |
| M | 19 | 121 | <0.4 | <0.4 | ND |
| M | 77 | 168 | <0.4 | <0.4 | ND |
| F | 33 | 37 | <0.4 | <0.4 | ND |
| ? | ? | 64 | <0.4 | <0.4 | ND |
| F | 26 | 79 | <0.4 | <0.4 | ND |
| F | 7 | 88 | <0.4 | <0.4 | ND |
| M | 61 | 90 | <0.4 | <0.4 | ND |
| F | 15 | 98 | <0.4 | <0.4 | ND |
| F | 15 | 159 | <0.4 | <0.4 | ND |
| M | 27 | 161 | <0.4 | <0.4 | ND |
| F | 48 | 172 | <0.4 | <0.4 | ND |
| F | 18 | 199 | <0.4 | <0.4 | ND |
| M | 33 | 103 | 0.41 | <0.4 | ND |
| F | 30 | 102 | 1.1 | <0.4 | ND |
| F | 41 | 165 | 1.8 | <0.4 | ND |
| M | 72 | 95 | 1.9 | <0.4 | ND |
| F | 34 | 51 | 6.0 | <0.4 | ND |
| M | 88 | 36 | 6.1 | <0.4 | ND |
| M | 69 | 50 | 6.3 | <0.4 | ND |
| F | 38 | 134 | 7.2 | <0.4 | ND |
| F | 33 | 133 | 12.2 | <0.4 | ND |
| F | 73 | 96 | 13.5 | 0.46 | 29.0 |
| M | 73 | 124 | 16.5 | <0.4 | ND |
| M | 60 | 191 | 18.3 | 0.48 | 38.6 |
| F | 31 | 116 | 18.4 | <0.4 | ND |
| M | 39 | 181 | 18.7 | 0.65 | 28.7 |
| F | 86 | 108 | 19.1 | <0.4 | ND |
| F | 79 | 160 | 19.4 | 0.65 | 30.1 |
| F | 89 | 128 | 25.0 | <0.4 | ND |
| F | 79 | 80 | 25.3 | 0.62 | 40.7 |
| F | 78 | 132 | 32.0 | <0.4 | ND |
| F | 40 | 99 | 32.7 | 0.81 | 40.6 |
| F | 34 | 114 | 33.4 | <0.4 | ND |
| F | 48 | 152 | 34.7 | 1.06 | 32.7 |
| M | 94 | 197 | 39.0 | 1.05 | 37.2 |
| M | 46 | 187 | 40.3 | 1.42 | 28.4 |
| F | 75 | 61 | 44.0 | 0.99 | 44.6 |
| M | 46 | 97 | 48.2 | 1.48 | 32.6 |
| F | 97 | 10 | 53.7 | 2.10 | 25.6 |
| M | 74 | 143 | 55.8 | 1.36 | 41.1 |
| F | 52 | 101 | 61.8 | 1.49 | 41.5 |
| F | 50 | 94 | 64.9 | 2.03 | 32.0 |
| M | 79 | 56 | 66.9 | 2.22 | 30.1 |
| F | 21 | 3 | 72.6 | 1.84 | 39.4 |
| F | 32 | 52 | 75.8 | 1.99 | 38.1 |
| M | 44 | 142 | 80.0 | 0.92 | 86.6 |
| M | 81 | 140 | 80.1 | 0.48 | 168.0 |
| F | 69 | 126 | 92.7 | 2.62 | 35.4 |
| F | 34 | 22 | 110 | 1.87 | 58.9 |
| M | 31 | 100 | 117 | 2.02 | 57.7 |
| F | 68 | 146 | 120 | 2.99 | 40.0 |
| F | 48 | 145 | 122 | 1.94 | 63.0 |
| F | 11 | 138 | 126 | <0.4 | ND |
| F | 82 | 2 | 128 | 3.56 | 36.0 |
| F | 45 | 87 | 129.2 | 3.98 | 32.5 |
| M | 55 | 13 | 138.2 | 4.86 | 28.4 |
| M | 90 | 125 | 143 | 4.11 | 34.8 |
| M | 54 | 75 | 148.5 | 4.96 | 29.9 |
| F | 81 | 18 | 150.1 | 1.97 | 76.2 |
| F | 87 | 137 | 156.5 | 1.8 | 86.9 |
| F | 62 | 48 | 157 | 8.74 | 18.0 |
| F | 36 | 171 | 158.1 | 2.78 | 56.9 |
| F | 41 | 164 | 160.9 | 4.28 | 37.6 |
| F | 83 | 9 | 161.9 | 3.94 | 41.1 |
| M | 18 | 67 | 176.6 | 4.17 | 42.4 |
| F | 85 | 163 | 183.6 | 5.09 | 36.1 |
| M | 81 | 89 | 195.5 | 2.89 | 67.6 |
| M | 66 | 58 | 205.7 | 5.56 | 37.0 |
| F | 66 | 104 | 213.4 | 5.57 | 38.3 |
| M | 38 | 54 | 226.9 | 5.63 | 40.3 |
| M | 28 | 55 | 229.4 | 2.27 | 101.1 |
| F | 34 | 107 | 241.2 | 5.72 | 42.2 |
| F | 39 | 49 | 273 | 13.43 | 20.3 |
| M | 75 | 43 | 279 | 16.24 | 17.2 |
| M | 89 | 34 | 368 | 11.03 | 33.4 |
| F | 28 | 17 | 418 | 7.45 | 56.1 |
| F | 74 | 11 | 452 | 8.44 | 53.6 |
| F | 81 | 112 | 454 | 7.12 | 63.8 |
| F | 13 | 30 | 484 | 7.85 | 61.7 |
| F | 88 | 35 | 486 | 13.25 | 36.7 |
| F | 39 | 27 | 495 | 9.05 | 54.7 |
| M | 87 | 26 | 515 | 7.72 | 66.7 |
| F | 70 | 85 | 536 | 8.49 | 63.1 |
| M | 75 | 83 | 556 | 10.53 | 52.8 |
| F | 68 | 44 | 558 | 13.3 | 42.0 |
| M | 74 | 82 | 575 | 9.74 | 59.0 |
| M | 47 | 93 | 663 | 13.09 | 50.6 |
| M | 86 | 117 | 664 | 10.47 | 63.4 |
| F | 71 | 72 | 727 | 9.39 | 77.4 |
| M | 52 | 148 | 820 | 11.35 | 72.2 |
| F | 29 | 65 | 827 | 14.29 | 57.9 |
| F | 74 | 42 | 842 | 16.05 | 52.5 |
| F | 84 | 92 | 863 | 16.38 | 52.7 |
| F | 75 | 81 | 889 | 13.44 | 66.1 |
| M | 72 | 186 | 937 | 21.83 | 42.9 |
| F | 89 | 15 | 1081 | 21.64 | 50.0 |
| M | 86 | 122 | 1104 | 21.38 | 51.6 |
| F | 89 | 111 | 1147 | 22.31 | 51.4 |
| M | 13 | 8 | 1166 | 45.84 | 25.4 |
| F | 83 | 162 | 1254 | 24.79 | 50.6 |
| F | 41 | 175 | 1259 | 22.51 | 55.9 |
| F | 67 | 115 | 1295 | 24.45 | 53.0 |
| F | 57 | 200 | 1396 | 24.51 | 57.0 |
| M | 22 | 130 | 1398 | 9.26 | 151.0 |
| M | 25 | 156 | 1436 | 23.78 | 60.4 |
| F | 32 | 178 | 1514 | 24.38 | 62.1 |
| M | 57 | 157 | 1618 | 27.62 | 58.6 |
| F | 60 | 123 | 1621 | 29.58 | 54.8 |
| F | 70 | 105 | 1740 | 33.85 | 51.4 |
| F | 92 | 177 | 1762 | 32.11 | 54.9 |
| F | 91 | 141 | 1766 | 32.74 | 53.9 |
| M | 33 | 131 | 1768 | 44.67 | 39.6 |
| F | 70 | 113 | 1788 | 33.44 | 53.5 |
| M | 63 | 127 | 1806 | 32.82 | 55.0 |
| M | 63 | 71 | 1837 | 25.63 | 71.7 |
| F | 70 | 106 | 1884 | 36.34 | 51.8 |
| F | 83 | 68 | 1910 | 30.45 | 62.7 |
| M | 22 | 77 | 1961 | 27.44 | 71.5 |
| F | 56 | 120 | 2038 | 29.21 | 69.8 |
| M | 46 | 45 | 2281 | 92.63 | 24.6 |
| F | 87 | 5 | 2328 | 45.56 | 51.1 |
| M | 49 | 47 | 2331 | 112.6 | 20.7 |
| F | 79 | 14 | 2375 | 37.23 | 63.8 |
| M | 69 | 144 | 2716 | 68.05 | 39.9 |
| M | 54 | 147 | 2722 | 39.05 | 69.7 |
| F | 49 | 32 | 2990 | 51.63 | 57.9 |
| M | 60 | 29 | 3007 | 47.19 | 63.7 |
| M | 63 | 189 | 3075 | 45.94 | 66.9 |
| F | 53 | 169 | 3095 | 54.46 | 56.8 |
| M | 74 | 153 | 3107 | 54.19 | 57.3 |
| F | 50 | 78 | 3163 | 49.34 | 64.1 |
| F | 43 | 110 | 3170 | 51.24 | 61.9 |
| F | 47 | 86 | 3295 | 57.18 | 57.6 |
| M | 59 | 198 | 3448 | 60.56 | 56.9 |
| M | 59 | 194 | 3639 | 60.27 | 60.4 |
| M | 69 | 33 | 3661 | 62.67 | 58.4 |
| F | 60 | 69 | 3960 | 49.95 | 79.3 |
| F | 76 | 91 | 4024 | 59.12 | 68.1 |
| M | 65 | 136 | 4249 | 70.44 | 60.3 |
| M | 41 | 139 | 4794 | 88.54 | 54.1 |
| M | 29 | 84 | 4798 | 79.75 | 60.2 |
| F | 68 | 180 | 5253 | 93.19 | 56.4 |
| F | 71 | 149 | 6048 | 89.64 | 67.5 |
| M | 25 | 174 | 6450 | 93.17 | 69.2 |
| F | 19 | 25 | 6547 | 119.6 | 54.7 |
| F | 27 | 192 | 6597 | 111.2 | 59.3 |
| M | 56 | 188 | 6747 | 99.29 | 68.0 |
| F | 71 | 76 | 6794 | 98.5 | 69.0 |
| F | 42 | 46 | 7312 | 1023 | 7.1 |
| F | 38 | 16 | 7751 | 119.4 | 64.9 |
| F | 39 | 176 | 7803 | 172.2 | 45.3 |
| M | 50 | 53 | 8630 | 98.05 | 88.0 |
| M | 42 | 31 | 8684 | 141.7 | 61.3 |
| M | 53 | 193 | 8945 | 150.1 | 59.6 |
| F | 52 | 118 | 9036 | 149.9 | 60.3 |
| F | 23 | 155 | 9234 | 173.3 | 53.3 |
| F | 45 | 158 | 9473 | 172 | 55.1 |
| M | 34 | 185 | 9646 | 147.5 | 65.4 |
| F | 70 | 41 | 10,470 | 1216 | 8.6 |
| F | 81 | 173 | 11,910 | 238.3 | 50.0 |
| M | 63 | 170 | 11,960 | 177 | 67.6 |
| F | 38 | 184 | 13,000 | 201.9 | 64.4 |
| M | 25 | 195 | 13,220 | 189.5 | 69.8 |
| M | 40 | 135 | 13,240 | 223.3 | 59.3 |
| M | 43 | 62 | 14,710 | 180.3 | 81.6 |
| F | 55 | 59 | 14,890 | 211.5 | 70.4 |
| F | 30 | 154 | 15,070 | 227.1 | 66.4 |
| F | 41 | 150 | 15,640 | 199.7 | 78.3 |
| F | 29 | 151 | 15,880 | 248.7 | 63.9 |
| M | 34 | 24 | 18,260 | 675 | 27.1 |
| F | 43 | 196 | 18,870 | 714 | 26.4 |
| M | 38 | 21 | 18,950 | 706 | 26.8 |
| F | 63 | 167 | 19,110 | 794 | 24.1 |
| F | 28 | 183 | 19,370 | 832 | 23.3 |
| F | 43 | 179 | 20,040 | 838 | 23.9 |
| F | 61 | 109 | 20,070 | 639 | 31.4 |
| F | 40 | 1 | 20,880 | 852 | 24.5 |
| F | 83 | 119 | 22,870 | 730 | 31.3 |
| M | 23 | 182 | 24,160 | 818 | 29.5 |
| M | 32 | 28 | 31,210 | 760 | 41.1 |
| F | 48 | 190 | 31,990 | 964 | 33.2 |
| F | 57 | 166 | 36,430 | 1479 | 24.6 |
| M | 52 | 63 | 47,210 | 1126 | 41.9 |
| M | 42 | 129 | 59,340 | 1345 | 44.1 |
| F | 81 | 73 | 87,400 | 2141 | 40.8 |
| F | 53 | 19 | 92,820 | 2896 | 32.1 |
| F | 85 | 66 | 98,290 | 2551 | 38.5 |
| Mean fold-change | 51.3 | ||||
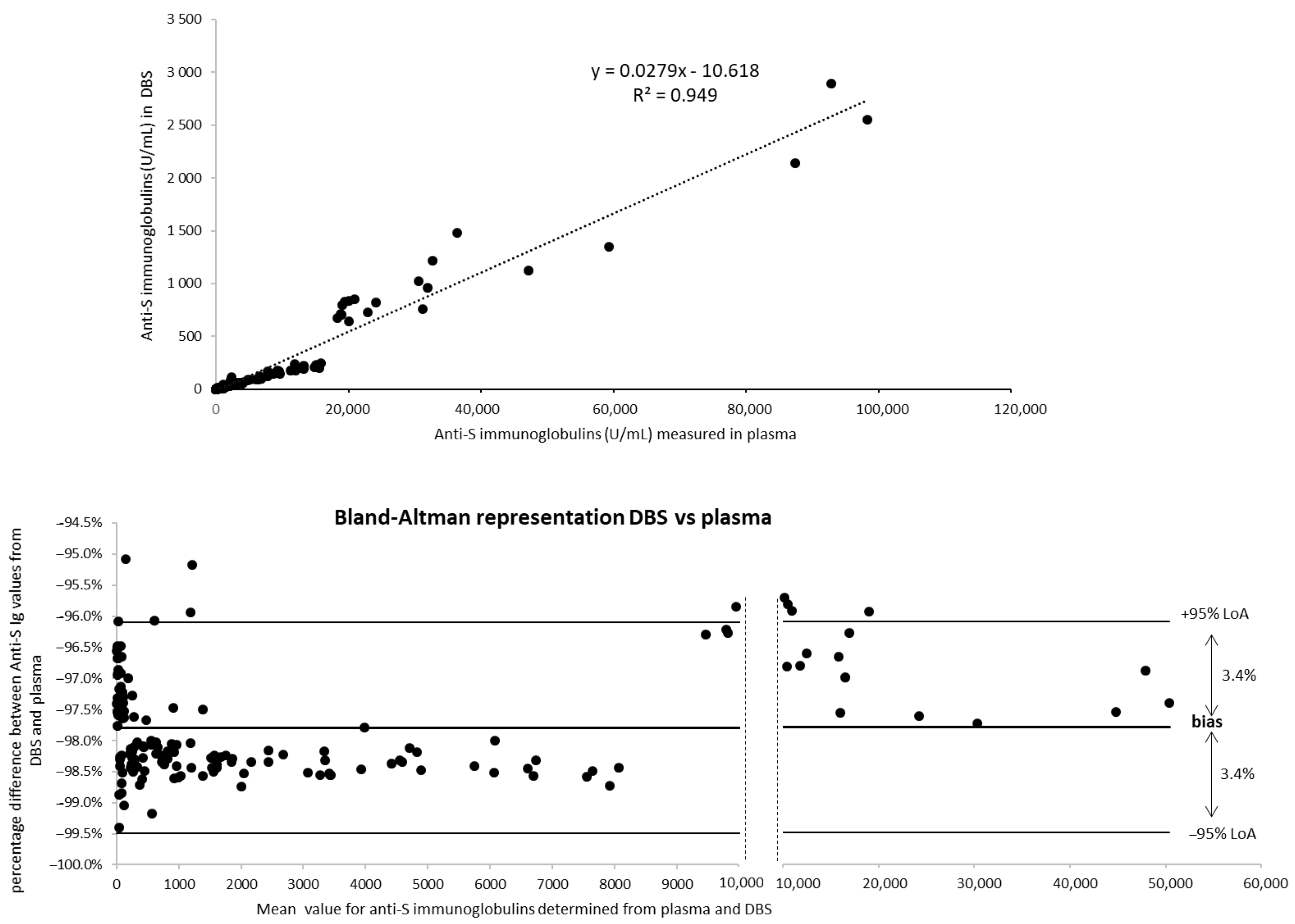
| Anti-S Ig below the Assay LOD (<0.4) | Anti-S Ig between 0.4 and 0.8 U/mL | Anti-S Ig (Value ≥0.8 for Plasma or ≥0.4 for DBS) | |||
| Plasma | 25 | 1 | 174 | ||
| qDBS | 41 | 5 | 159 | ||
| Discordant plasma-DBS results | |||||
| Plasma ≥0.8 and <0.4 by DBS | 15 | ||||
| Plasma <0.8 and DBS ≥0.4) | 0 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchand, A.; Roulland, I.; Semence, F.; Beck, O.; Ericsson, M. Use of Quantitative Dried Blood Spots to Evaluate the Post-Vaccination Level of Neutralizing Antibodies against SARS-CoV-2. Life 2021, 11, 1125. https://doi.org/10.3390/life11111125
Marchand A, Roulland I, Semence F, Beck O, Ericsson M. Use of Quantitative Dried Blood Spots to Evaluate the Post-Vaccination Level of Neutralizing Antibodies against SARS-CoV-2. Life. 2021; 11(11):1125. https://doi.org/10.3390/life11111125
Chicago/Turabian StyleMarchand, Alexandre, Ingrid Roulland, Florian Semence, Olof Beck, and Magnus Ericsson. 2021. "Use of Quantitative Dried Blood Spots to Evaluate the Post-Vaccination Level of Neutralizing Antibodies against SARS-CoV-2" Life 11, no. 11: 1125. https://doi.org/10.3390/life11111125