Coronavirus Disease 2019 (COVID-19) in Italy: Double Reading of Chest CT Examination

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. CT Technique and Analysis
2.3. Statistical Analysis
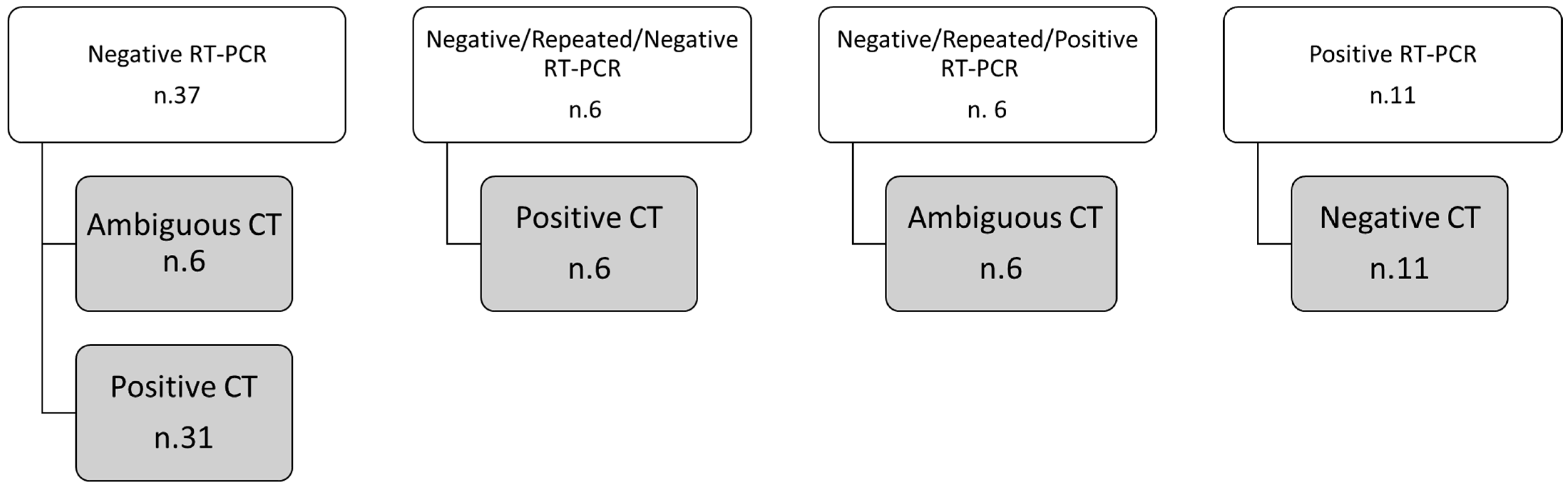
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Available online: https://www.who.int/health-topics/middle-east-respiratory-syndrome-coronavirus-mers#tab=tab_1 (accessed on 21 March 2020).
- World Health Organization. Naming the Coronavirus Disease (COVID-2019) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 21 March 2020).
- China National Health Commission. Diagnosis and Treatment of Pneumonitis Caused by New Coronavirus; Trial Version 5; National Health Commission: Beijing, China, 2020.
- Poon, L.L.; Chan, K.H.; Wong, O.K.; Cheung, T.K.; Ng, I.; Zheng, B.; Seto, W.H.; Yuen, K.Y.; Guan, Y.; Peirs, J.S.M. Detection of SARS coronavirus in patients with severe acute respiratory syndrome by conventional and real-time quantitative reverse transcription-PCR assays. Clin. Chem. 2004, 50, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, D.; Sabetta, E.; Ceriotti, D.; Motta, A.; Strollo, M.; Banfi, G.; Locatelli, M. Routine blood analysis greatly reduces the false-negative rate of RT-PCR testing for COVID-19. Acta Biomed. 2020, 91, e2020003. [Google Scholar] [PubMed]
- Rattan, A.; Ahmad, H. Can quantitative RT-PCR for SARS-coV-2 help in better management of patients and control of coronavirus disease 2019 pandemic. Indian J. Med. Microbiol. 2020, 38, 284–287. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology. ACR Recommendations for the Use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. Available online: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection (accessed on 21 March 2020).
- The Royal Australian and NewZeland College of Radiologists. COVID-19 Updates. Available online: https://www.ranzcr.com/our-work/coronavirus (accessed on 21 March 2020).
- The Royal College of Radiologists. The Role of CT in Patients Suspected with COVID-19 Infection. Available online: https://www.rcr.ac.uk/college/coronavirus-covid-19-what-rcr-doing/rcr-position-role-ct-patients-suspected-covid-19 (accessed on 21 March 2020).
- Canadian Association of Radiologists. Canadian Society of Thoracic Radiology and Canadian Association of Radiologists’ Statement on COVID-19. Available online: https://car.ca/news/canadian-society-of-thoracic-radiology-and-canadian-association-of-radiologists-statement-on-covid-19/ (accessed on 21 March 2020).
- See, K.C.; Ong, V.; Tan, Y.L.; Sahagun, J.; Taculod, J. Chest radiography versus lung ultrasound for identification of acute respiratory distress syndrome: A retrospective observational study. Crit. Care 2018, 22, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandirali, M.; Sconfienza, L.M.; Serra, R.; Brembilla, R.; Albano, D.; Pregliasco, F.; Messina, C. Chest Radiograph Findings in Asymptomatic and Minimally Symptomatic Quarantined Patients in Codogno, Italy during COVID-19 Pandemic. Radiology 2020, 295. [Google Scholar] [CrossRef] [Green Version]
- Zu, Z.Y.; Di Jiang, M.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.; Zhang, L.J. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanne, J.P.; Little, B.P.; Chung, J.H.; Elicker, B.M.; Ketai, L.H. Essentials for Radiologists on COVID-19: An Update—Radiology Scientific Expert Panel. Radiology 2020, 296, E113–E114. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Li, X.; Wang, Y.; Han, Y.; Wang, Y.; Wang, C.; Zhang, G.; Jin, J.; Jia, H.; Fan, F.; et al. Diagnostic value and key features of computed tomography in Coronavirus Disease 2019. Emerg. Microbes Infect. 2020, 9, 787–793. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Lei, J.; Li, J.; Li, X.; Qi, X. CT Imaging of the 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 2020, 295, 18. [Google Scholar] [CrossRef] [Green Version]
- Giovagnoni, A. Facing the COVID-19 emergency: We can and we do. Radiol. Med. 2020, 125, 337–338. [Google Scholar] [CrossRef] [Green Version]
- Agostini, A.; Floridi, C.; Borgheresi, A.; Badaloni, M.; Pirani, P.E.; Terilli, F.; Ottaviani, L.; Giovagnoni, A. Proposal of a low-dose, long-pitch, dual-source chest CT protocol on third-generation dual-source CT using a tin filter for spectral shaping at 100 kVp for CoronaVirus Disease 2019 (COVID-19) patients: A feasibility study. Radiol. Med. 2020, 125, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossa-Basha, M.; Meltzer, C.; Kim, D.C.; Tuite, M.J.; Kolli, K.P.; Tan, B.S. Radiology Department Preparedness for COVID-19: Radiology Scientific Expert Review Panel. Radiology 2020, 296, E106–E112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Società Italiana di Radiologia Medica e Interventistica. COVID-19: Il Referto Strutturato. Available online: https://www.sirm.org/2020/02/28/covid-19-il-referto-strutturato/ (accessed on 21 March 2020).
- Grassi, R.; Cappabianca, S.; Urraro, F.; Feragalli, B.; Montanelli, A.; Patelli, G.; Granata, V.; Giacobbe, G.; Russo, G.M.; Grillo, A.; et al. Chest CT Computerized Aided Quantification of PNEUMONIA Lesions in COVID-19 Infection: A Comparison among Three Commercial Software. Int. J. Environ. Res. Public Health 2020, 17, 6914. [Google Scholar] [CrossRef] [PubMed]
- Grassi, R.; Fusco, R.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; Urraro, F.; Petrillo, A.; Granata, V.; Sacco, P.; Mazzei, M.A.; et al. Coronavirus Disease 2019 (COVID-19) in Italy: Features on Chest Computed Tomography using a structured report system. Sci. Rep. 2020, 10, 17236. [Google Scholar] [CrossRef] [Green Version]
- Arevalo-Rodriguez, I.; Buitrago-Garcia, D.; Simancas-Racines, D.; Zambrano-Achig, P.; Del Campo, R.; Ciapponi, A.; Sued, O.; Martinez-García, L.; Rutjes, A.W.; Low, N.; et al. False-negative results of initial RT-PCR assays for COVID-19: A systematic review. PLoS ONE 2020, 15, e0242958. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Zhu, T.; Wang, Y.; Xia, L. Imaging features and evolution on CT in 100 COVID-19 pneumonia patients in Wuhan, China. Eur. Radiol. 2020, 1–9. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction-Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Ng, L.F.P.; Hiscox, J.A. Coronaviruses in animals and humans. BMJ 2020, 368. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Lee, E.Y.P.; Ng, M.Y.; Khong, P.L. COVID-19 pneumonia: What has CT taught us? Lancet Infect. Dis. 2020, 20, 384–385. [Google Scholar] [CrossRef]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, H.; Taha, M.S.; Askoura, A.; Aleem, M.; Omran, A.; Aboelela, S. Can chest CT improve sensitivity of COVID-19 diagnosis in comparison to PCR? A meta-analysis study. Egypt J. Otolaryngol. 2020, 36, 49, PMCID: PMC7649892. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (y) | Positive for COVID-19 upon RT-PCR Test | Negative for COVID-19 upon RT-PCR Test | p-Value | ||
|---|---|---|---|---|---|
| Median | 70.0 | 77.5 | >0.05 | ||
| Range | 29–93 | 32–89 | |||
| Tot | % | Tot | % | p-value | |
| Sex, no. (%) of patients | |||||
| Male | 226 | 68.9 | 31 | 62.0 | 0.01 |
| Female | 102 | 31.9 | 29 | 58.0 | |
| CT diagnosis at first CT reading | |||||
| Positive | 283 | 94.3 | 43 | 55.1 | <<0.001 |
| Negative | 17 | 5.7 | 35 | 44.9 | |
| CT diagnosis at second CT reading | |||||
| Positive | 292 | 97.3 | 36 | 46.2 | <<0.001 |
| Negative | 8 | 2.7 | 42 | 53.8 | |
| Cases with concordance between RT-PCR and CT diagnosis | |||||
| Median value of temporal windows between RT-PCR and CT execution | 0 | 0 | >0.05 | ||
| Range of temporal windows between RT-PCR and CT execution | −9–11 | −1–4 | |||
| Cases with discordance between RT-PCR and CT diagnosis | |||||
| Median value of temporal windows between RT-PCR and CT execution | 0 | 0 | >0.05 | ||
| Range of temporal windows between RT-PCR and CT execution | −2–4 | −8–4 | |||
| CT Findings in 50 patients with discordance between RT-PCR and CT diagnosis after second CT reading | |||||
| Presence of GGOs with consolidation | 2 | 12 | >0.05 | ||
| Presence of GGOs without consolidation | 5 | 20 | |||
| Presence of consolidation without GGOs | 1 | 4 | |||
| Diagnostic Confidence Level | CT Characteristics |
|---|---|
| High diagnostic confidence level | Bilateral multifocal GGO with predominantly peripheral distribution associated or not with septal thickening (crazy paving) and/or consolidations; multifocal GGO of rounded morphology associated or not with crazy paving and/or consolidations; multifocal GGO associated with findings of organizing pneumonia. |
| Intermediate diagnostic confidence level | GGO with diffuse distribution associated or not with crazy paving and/or consolidations; bilateral multifocal GGO and/or consolidations without a prevalent peripheral distribution and without rounded morphology; unilateral GGO with or without consolidation. |
| Low diagnostic confidence level | Isolated small areas of GGO and/or consolidations with non-rounded morphology were included in the low confidence level. |
| Negative for COVID-19 | Cases without the described alterations and with one or more of the following alterations were considered indicative of other diagnoses: isolated lobar or segmental consolidations, presence of solid or caveated nodules, presence of micro-nodules (centro-lobular micro-nodules and “tree in bud” pattern), smooth thickening of the interlobular septa with pleural effusion. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reginelli, A.; Grassi, R.; Feragalli, B.; Belfiore, M.P.; Montanelli, A.; Patelli, G.; La Porta, M.; Urraro, F.; Fusco, R.; Granata, V.; et al. Coronavirus Disease 2019 (COVID-19) in Italy: Double Reading of Chest CT Examination. Biology 2021, 10, 89. https://doi.org/10.3390/biology10020089
Reginelli A, Grassi R, Feragalli B, Belfiore MP, Montanelli A, Patelli G, La Porta M, Urraro F, Fusco R, Granata V, et al. Coronavirus Disease 2019 (COVID-19) in Italy: Double Reading of Chest CT Examination. Biology. 2021; 10(2):89. https://doi.org/10.3390/biology10020089
Chicago/Turabian StyleReginelli, Alfonso, Roberta Grassi, Beatrice Feragalli, Maria Paola Belfiore, Alessandro Montanelli, Gianluigi Patelli, Michelearcangelo La Porta, Fabrizio Urraro, Roberta Fusco, Vincenza Granata, and et al. 2021. "Coronavirus Disease 2019 (COVID-19) in Italy: Double Reading of Chest CT Examination" Biology 10, no. 2: 89. https://doi.org/10.3390/biology10020089