
Continuous Decline in Myocardial Infarction and Heart Failure Hospitalizations during the First 12 Months of the COVID-19 Pandemic in Israel

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Study Variables
2.3. Comparison Periods
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solomon, M.D.; McNulty, E.J.; Rana, J.S.; Leong, T.K.; Lee, C.; Sung, S.; Ambrosy, A.P.; Sidney, S.; Go, A.S. The COVID-19 Pandemic and the Incidence of Acute Myocardial infarction. N. Engl. J. Med. 2020, 383, 691–693. [Google Scholar] [CrossRef] [PubMed]
- Infarction. Available online: https://www.who.int/news/item/01-06-2020-covid-19-significantly-impacts-health-services-for-noncommunicable-diseases (accessed on 10 March 2022).
- Pessoa-Amorim, G.; Camm, C.F.; Gajendragadkar, P.; de Maria, G.L.; Arsac, C.; Laroche, C.; Zamorano, J.L.; Weidinger, F.; Achenbach, S.; Maggioni, A.P.; et al. Admission of patients with STEMI since the outbreak of the COVID-19 pandemic: A survey by the European Society of Cardiology. Guilherme Eur. Heart J. Qual. Care Clin. Outcomes 2020, 6, 210–216. [Google Scholar] [CrossRef] [PubMed]
- de Filippo, O.; D’Ascenzo, F.; Angelini, F.; Bocchino, P.P.; Conrotto, F.; Saglietto, A.; Secco, G.G.; Campo, G.; Gallone, G.; Verardi, R.; et al. Reduced Rate of Hospital Admissions for ACS during COVID-19 Outbreak in Northern Italy. N. Engl. J. Med. 2020, 383, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Severino, P.; D’Amato, A.; Saglietto, A.; D’Ascenzo, F.; Marini, C.; Schiavone, M.; Ghionzoli, N.; Pirrotta, F.; Troiano, F.; Cannillo, M.; et al. Reduction in heart failure hospitalization rate during coronavirus disease 19 pandemic outbreak. ESC Heart Fail. 2020, 7, 4182–4188. [Google Scholar] [CrossRef] [PubMed]
- Lavie, G.; Battat, E.; Saliba, W.; Flugelman, M.Y. Change in hospitalizations and 30-day mortality of patients with acute myocardial infarction during the first COVID-19 lockdown—A pure social isolation effect? Cardiovasc. Revasc. Med. 2021. [Google Scholar] [CrossRef]
- Mafham, M.M.; Spata, E.; Goldacre, R. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Wu, J.; Mamas, M.A.; de Belder, M.A.; Deanfield, J.E.; Gale, C.P. Second Decline in Admissions With Heart Failure and Myocardial Infarction During the COVID-19 Pandemic. J. Am. Coll. Cardiol. 2021, 77, 1141–1143. [Google Scholar] [CrossRef]
- Solomon, M.D.; Nguyen-Huynh, M.; Leong, T.K.; Alexander, J.; Rana, J.S.; Klingman, J.; Go, A.S. Changes in Patterns of Hospital Visits for Acute Myocardial Infarction or Ischemic Stroke During COVID-19 Surges. JAMA 2021, 326, 82–84. [Google Scholar] [CrossRef]
- Christensen, D.M.; Butt, J.H.; Fosbøl, E.; Køber, L.; Torp-Pedersen, C.; Gislason, G.; Phelps, M. Nationwide cardiovascular disease admission rates during a second COVID-19 lockdown. Am. Heart J. 2021, 241, 35–37. [Google Scholar] [CrossRef]
- Mohammad, M.A.; Koul, S.; Gale, C.P.; Alfredsson, J.; James, S.; Fröbert, O.; Omerovic, E.; Erlinge, D. The association of mode of location activity and mobility with acute coronary syndrome: A nationwide ecological study. J. Int. Med. 2021, 289, 247–254. [Google Scholar] [CrossRef]
- Sofi, F.; Dinu, M.; Reboldi, G.; Stracci, F.; Pedretti, R.F.E.; Valente, S.; Gensini, G.F.; Gibson, C.M.; Ambrosio, G. Worldwide differences of hospitalization for ST-segment elevation myocardial infarction during COVID-19: A systematic review and meta-analysis. Int. J. Cardiol. 2022, 347, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.; Rosamond, W.; Patel, M.D.; Waller, A.E. Statewide declines in myocardial infarction and stroke emergency department visits during COVID-19 restrictions in North Carolina. Am. J. Emerg. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, A.S.; Moscone, A.; McElrath, E.E.; Varshney, A.S.; Claggett, B.L.; Bhatt, D.L.; Januzzi, J.L.; Butler, J.; Adler, D.S.; Solomon, S.D.; et al. Fewer Hospitalizations for Acute Cardiovascular Conditions During the COVID-19 Pandemic. J. Am. Coll. Cardiol. 2020, 76, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, M.M.; D’Onofrio, G.; Paek, H.; Platts-Mills, T.F.; Soares, W.E.; Hoppe, J.A.; Genes, N.; Nath, B.; Melnick, E.R. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First Months of the COVID-19 Pandemic in the US. JAMA Intern. Med. 2020, 180, 1328–1333. [Google Scholar] [CrossRef]
- Ciofani, J.L.; Han, D.; Allahwala, U.K.; Asrress, K.N.; Bhindi, R. Internet search volume for chest pain during the COVID-19 pandemic. Am. Heart J. 2021, 231, 157–159. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or Avoidance of Medical Care Because of COVID-19-Related Concerns—United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250–1257. [Google Scholar] [CrossRef]
- Rind, I.A.; Cannata, A.; McDonaugh, B.; Cassimon, B.; Bannister, C.; Scott, P.A.; Piper, S.; Bromage, D.I.; McDonagh, T.A. Patients hospitalised with heart failure across different waves of the COVID-19 pandemic show consistent clinical characteristics and outcomes. Int. J. Cardiol. 2022, 350, 125–129. [Google Scholar] [CrossRef]
- D’Ascenzo, F.; de Filippo, O.; Borin, A.; Barbieri, L.; Adamo, M.; Morici, N.; Giachet, A.T.; Iannaccone, M.; Crimi, G.; Gaido, L.; et al. Impact of COVID-19 pandemic and infection on in hospital survival for patients presenting with acute coronary syndromes: A multicenter registry. Int. J. Cardiol. 2021, 332, 227–234. [Google Scholar] [CrossRef]
- Butt, J.H.; Østergaard, L.; Gerds, T.A.; Lauridsen, M.D.; Kragholm, K.; Schou, M.; Phelps, M.; Gislason, G.H.; Torp-Pedersen, C.; Køber, L.; et al. The association between cardiovascular disease admission rates and the coronavirus disease 2019 lockdown and reopening of a nation: A Danish nationwide cohort study. Eur. Heart J. Qual. Care Clin. Outcomes 2022, 8, 14–22. [Google Scholar] [CrossRef]
- Shoaib, A.; van Spall, H.G.C.; Wu, J.; Cleland, J.G.F.; McDonagh, T.A.; Rashid, M.; Mohamed, M.O.; Ahmed, F.Z.; Deanfield, J.; de Belder, M.; et al. Substantial decline in hospital admissions for heart failure accompanied by increased community mortality during COVID-19 pandemic. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 378–387. [Google Scholar] [CrossRef]
- Rao, V.N.; Kelsey, M.D.; Kelsey, A.M.; Russell, S.D.; Mentz, R.J.; Patel, M.R.; Fudim, M. Acute cardiovascular hospitalizations and illness severity before and during the COVID-19 pandemic. Clin. Cardiol. 2021, 44, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Cannatà, A.; Bromage, D.I.; Rind, I.A.; Gregorio, C.; Bannister, C.; Albarjas, M.; Piper, S.; Shah, A.M.; McDonagh, T.A. Temporal trends in decompensated heart failure and outcomes during COVID-19: A multisite report from heart failure referral centres in London. Eur. J. Heart Fail 2020, 22, 2219–2224. [Google Scholar] [CrossRef] [PubMed]
- Scholz, K.H.; Lengenfelder, B.; Thilo, C.; Jeron, A.; Stefanow, S.; Janssens, U.; Johann Bauersachs, P.; Schulze, C.; Winter, K.D.; Schröder, J.; et al. Impact of COVID-19 outbreak on regional STEMI care in Germany. Clin. Res. Cardiol. 2020, 109, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Cannata, A.; Watson, S.A.; Daniel, A.; Giacca, M.; Shah, A.M.; McDonagh, T.A.; Scott, P.A.; Bromage, D.I. Impact of the COVID-19 pandemic on in-hospital mortality in cardiovascular disease: A meta-analysis. Eur. J. Prev. Cardiol. 2021, zwab119. [Google Scholar] [CrossRef] [PubMed]
- König, S.; Hohenstein, S.; Meier-Hellmann, A.; Kuhlen, R.; Hindricks, G.; Bollmann, A. In-hospital care in acute heart failure during the COVID-19 pandemic: Insights from the German-wide Helios hospital network. Eur. J. Heart Fail. 2020, 22, 2190–2201. [Google Scholar] [CrossRef]
- Roy, C.M.; Bollman, E.B.; Carson, L.M.; Northrop, A.J.; Jackson, E.F.; Moresky, R.T. Assessing the indirect effects of COVID-19 on healthcare delivery, utilization and health outcomes: A scoping review. Eur. J. Public Health 2021, 31, 634–640. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | STEMI | non-STEMI | CHF | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yearly Average of 3 Baseline Years | Corona Year | p Value | Yearly Average of 3 Baseline Years | Corona Year | p Value | Yearly Average of 3 Baseline Years | Corona Year | p Value | Yearly Average of 3 Baseline Years | Corona Year | p Value | ||
| Total | N | 4,494,077 | 4,627,464 | 3187.3 | 2758 | 7353.3 | 6509 | 36,285 | 28,352 | ||||
| Age | Age < 60 years | 3,675,782 (82%) | 3,782,214 (82%) | 0.024 | 1089 (34%) | 974 (35%) | NS | 1482 (20%) | 1315 (20%) | NS | 3098 (9%) | 2377 (8%) | NS |
| >=60 years | 818,295 (18%) | 845,250 (18%) | 2098 (66%) | 1784 (65%) | 5872 (80%) | 5194 (80%) | 33,187 (91%) | 25,975 (92%) | |||||
| Sex | Male | 2,204,749 (49%) | 2,274,502 (49%) | 0.005 | 2430 (76%) | 2117 (77%) | NS | 4929 (67%) | 4439 (68%) | NS | 19,324 (53%) | 15,184 (54%) | NS |
| Female | 2,289,313 (51%) | 2,352,914 (51%) | 757 (24%) | 641 (23%) | 2424 (33%) | 2070 (32%) | 16,962 (47%) | 13,168 (46%) | |||||
| Charlson comorbidy index | CCI < 5 | 4,354,719 (97%) | 4,481,813 (97%) | <0.001 | 823 (26%) | 700 (25%) | NS | 1584 (22%) | 1312 (20%) | NS | 14,071 (39%) | 11,167 (39%) | NS |
| CCI >= 5 | 139,358 (3%) | 145,651 (3%) | 69 (2%) | 59 (2%) | 200 (3%) | 166 (3%) | 2221 (61%) | 17,185 (61%) | |||||
| Ethnicity | Arab | 1,210,338 (27%) | 1,248,746 (27%) | <0.001 | 2295 (72%) | 1999 (72%) | NS | 5568 (76%) | 5031 (77%) | NS | 7255 (20%) | 5546 (20%) | NS |
| Ultra-Orthodox | 253,545 (6%) | 273,004 (6%) | 2532 (79%) | 2233 (81%) | 4557 (62%) | 4071 (63%) | 1136 (3%) | 891 (3%) | |||||
| General | 3,013,349 (67%) | 3,090,087 (67%) | 655 (21%) | 525 (19%) | 2797 (38%) | 2438 (37%) | 27,885 (77%) | 21,913 (77%) | |||||
| Missing | 16,845 (0%) | 15,627 (0%) | |||||||||||
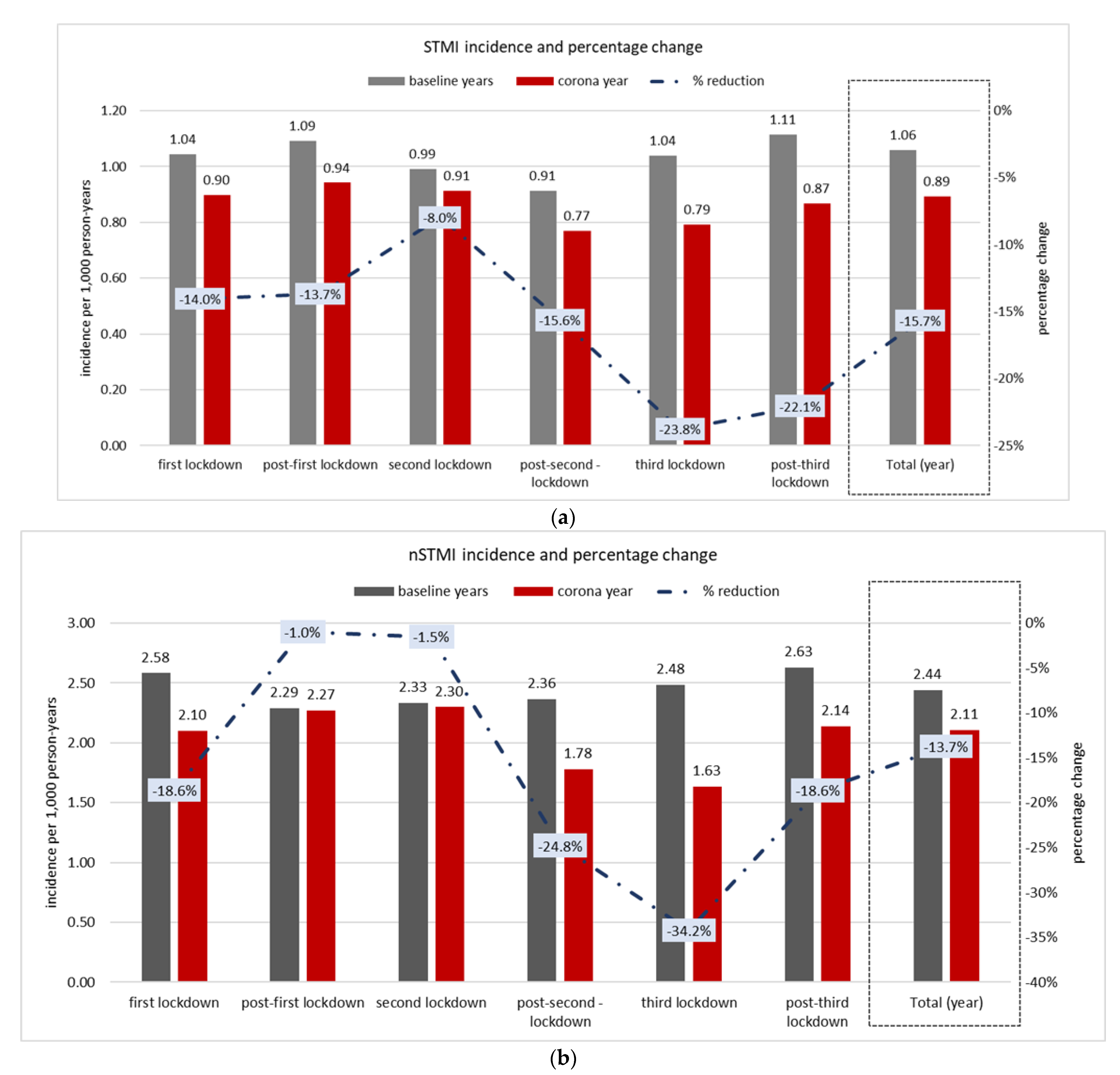
| STEMI | First Lockdown | Post-First Lockdown | Second Lockdown | Post-Second -Lockdown | Third Lockdown | Post-Third Lockdown | Total | |
|---|---|---|---|---|---|---|---|---|
| Calendar weeks | 10 to 15 | 16 to 36 | 37 to 41 | 42 to 51 | 52 to 6 | 7 to 10 | ||
| Baseline years | N of cases | 1068 | 3905 | 845 | 1556 | 1239 | 949 | 9562 |
| Total person-years | 1,022,379 | 3,578,329 | 851,983 | 1,703,966 | 1,192,777 | 851,983 | 9,031,021 | |
| Incidence per 1000 PY | 1.04 | 1.09 | 0.99 | 0.91 | 1.04 | 1.11 | 1.06 | |
| Corona year | N of cases | 314 | 1153 | 266 | 449 | 323 | 253 | 2758 |
| Total person-years | 349,688 | 1223,909 | 291,407 | 582,814 | 407,970 | 291,407 | 3,088,913 | |
| Incidence per 1000 PY | 0.90 | 0.94 | 0.91 | 0.77 | 0.79 | 0.87 | 0.89 | |
| % reduction | −14% | −13.7% | −8% | −15.6% | −23.8% | −22% | −15.7% | |
| 95% CI (upper, lower) | −11%, −17% | −11%, −17% | −5%, −11% | −13%, −19% | −21%, −27% | −19%, −25% | −13%, −19% | |
| Non-STEMI | First Lockdown | Post-First Lockdown | Second Lockdown | Post-Second-Lockdown | Third Lockdown | Post-Third Lockdown | Total | |
|---|---|---|---|---|---|---|---|---|
| Calendar weeks | 10 to 15 | 16 to 36 | 37 to 41 | 42 to 51 | 52 to 6 | 7 to 10 | ||
| Baseline years | N of cases | 2640 | 8201 | 1989 | 4027 | 2964 | 2239 | 22,060 |
| Total person-years | 1,022,379 | 3,578,329 | 851,983 | 1,703,966 | 1,192,777 | 851,983 | 9,031,021 | |
| Incidence per 1000 PY | 2.58 | 2.29 | 2.33 | 2.36 | 2.48 | 2.63 | 2.44 | |
| Corona year | N of cases | 735 | 2778 | 670 | 1036 | 667 | 623 | 6509 |
| Total person-years | 349,688 | 1,223,909 | 291,407 | 582,814 | 407,970 | 291,407 | 3,088,913 | |
| Incidence per 1000 PY | 2.10 | 2.27 | 2.30 | 1.78 | 1.63 | 2.14 | 2.11 | |
| % reduction | −18.6% | −1% | −1.5% | −24.8% | −34.2% | −18.6% | −13.7% | |
| 95% CI (upper, lower) | −16%, −22% | 2%, −4% | 1%, −5% | −22%, −28% | −31%, −37% | −16%, −22% | −11%, −17% |
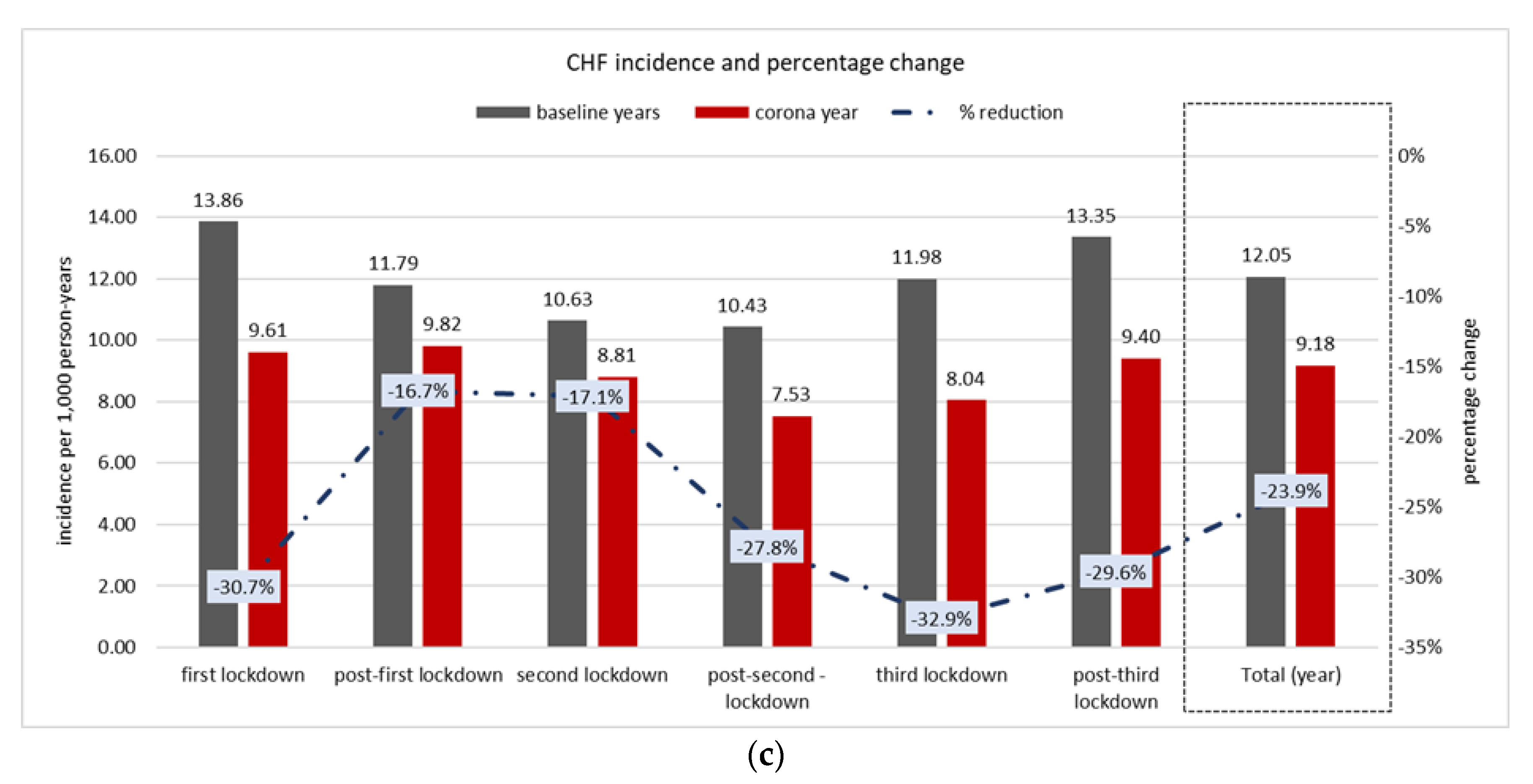
| CHF | First Lockdown | Post-First Lockdown | Second Lockdown | Post-Second–Lockdown | Third Lockdown | Post-Third Lockdown | Total (Year) | |
|---|---|---|---|---|---|---|---|---|
| calendar weeks | 10 to 15 | 16 to 36 | 37 to 41 | 42 to 51 | 52 to 6 | 7 to 10 | ||
| Baseline years | N of cases | 14,167 | 42,191 | 9058 | 17,771 | 14,295 | 11,374 | 108,856 |
| Total person-years | 1,022,379 | 3,578,329 | 8,51,983 | 1,703,966 | 1,192,777 | 851,983 | 9,031,021 | |
| Incidence per 1000 PY | 13.86 | 11.79 | 10.63 | 10.43 | 11.98 | 13.35 | 12.05 | |
| Corona year | N of cases | 3359 | 12018 | 2568 | 4387 | 3281 | 2739 | 28352 |
| Total person-years | 349,688 | 1,223,909 | 291,407 | 582,814 | 407,970 | 291,407 | 3,088,913 | |
| Incidence per 1000 PY | 9.61 | 9.82 | 8.81 | 7.53 | 8.04 | 9.40 | 9.18 | |
| % reduction | −30.7% | −16.7% | −17.1% | −27.8% | −32.9% | −29.6% | −23.9% | |
| 95% CI (upper, lower) | −28%, −34% | −14%, −20% | −14%, −20% | −25%, −31% | −30%, −36% | −27%, −33% | −21%, −27% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lavie, G.; Wolff Sagy, Y.; Hoshen, M.; Saliba, W.; Flugelman, M.Y. Continuous Decline in Myocardial Infarction and Heart Failure Hospitalizations during the First 12 Months of the COVID-19 Pandemic in Israel. J. Clin. Med. 2022, 11, 1577. https://doi.org/10.3390/jcm11061577
Lavie G, Wolff Sagy Y, Hoshen M, Saliba W, Flugelman MY. Continuous Decline in Myocardial Infarction and Heart Failure Hospitalizations during the First 12 Months of the COVID-19 Pandemic in Israel. Journal of Clinical Medicine. 2022; 11(6):1577. https://doi.org/10.3390/jcm11061577
Chicago/Turabian StyleLavie, Gil, Yael Wolff Sagy, Moshe Hoshen, Walid Saliba, and Moshe Y. Flugelman. 2022. "Continuous Decline in Myocardial Infarction and Heart Failure Hospitalizations during the First 12 Months of the COVID-19 Pandemic in Israel" Journal of Clinical Medicine 11, no. 6: 1577. https://doi.org/10.3390/jcm11061577