
Seroprevalence of SARS-CoV-2 Antibodies among Vaccinated and Non-Vaccinated Adults in the West Bank: Results of a Repeated Cross-Sectional Study



Abstract: Background
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. SARS-CoV-2 Antibody Testing
2.4. Statistical Analysis
3. Results
Sample Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2021; Available online: https://covid19.who.int/table (accessed on 12 March 2022).
- Cheng, M.P.; Papenburg, J.; Desjardins, M.; Kanjilal, S.; Quach, C.; Libman, M.; Dittrich, S.; Yansouni, C.P. Diagnostic Testing for Severe Acute Respiratory Syndrome-Related Coronavirus 2: A Narrative Review. Ann. Intern. Med. 2020, 172, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Lieberman-Cribbin, W.; Tuminello, S.; Flores, R.M.; Taioli, E. Disparities in COVID-19 Testing and Positivity in New York City. Am. J. Prev. Med. 2020, 59, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Buitrago-Garcia, D.; Egli-Gany, D.; Counotte, M.J.; Hossmann, S.; Imeri, H.; Ipekci, A.M.; Salanti, G.; Low, N. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis. PLoS Med. 2020, 17, e1003346. [Google Scholar] [CrossRef] [PubMed]
- Busch, M.P.; Stone, M. Serosurveillance for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Incidence Using Global Blood Donor Populations. Clin. Infect. Dis. 2021, 72, 254–256. [Google Scholar] [CrossRef] [PubMed]
- Havers, F.P.; Reed, C.; Lim, T.; Montgomery, J.M.; Klena, J.D.; Hall, A.J.; Hand, J.; Jain, S.; Lindquist, S.; Thornburg, N.J.; et al. Seroprevalence of Antibodies to SARS-CoV-2 in 10 Sites in the United States, March 23–May 12, 2020. JAMA Intern. Med. 2020, 180, 1576–1586. [Google Scholar] [CrossRef] [PubMed]
- Bajema, K.L.; Wiegand, R.E.; Cuffe, K.; Patel, S.V.; Iachan, R.; Lim, T.; Lee, A.; Moyse, D.; Havers, F.P.; Edens, C.; et al. Estimated SARS-CoV-2 Seroprevalence in the US as of September 2020. JAMA Intern. Med. 2021, 181, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhang, X.; Zhang, X.; Wei, Z.; Zhang, L.; Xu, J.; Liang, P.; Xu, Y.; Zhang, C.; Xu, A.; et al. Rapid asymptomatic transmission of COVID-19 during the incubation period demonstrating strong infectivity in a cluster of youngsters aged 16–23 years outside Wuhan and characteristics of young patients with COVID-19: A prospective contact-tracing study. J. Infect. 2020, 80, e1–e13. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, C.C.; Doll, M.K.; Morrison, K.T.; McLaughlin, W.L.; O’Connor, T.; Sholukh, A.M.; Bossard, E.L.; Phasouk, K.; Ford, E.S.; Corey, L.; et al. High Community SARS-CoV-2 Antibody Seroprevalence in a Ski Resort Community, Blaine County, Idaho, US. Preliminary Results. medRxiv 2020. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Arora, R.K.; Cao, C.; Boucher, E.; Liu, M.; Donnici, C.; Yanes-Lane, M.; Whelan, M.; Perlman-Arrow, S.; Cheng, M.P.; et al. Global seroprevalence of SARS-CoV-2 antibodies: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0252617. [Google Scholar]
- Worldometer. State of Palestine: Coronovirus Cases. 2022. Available online: https://www.worldometers.info/coronavirus/country/state-of-palestine (accessed on 17 March 2022).
- Qutob, N.; Awartani, F.; Salah, Z.; Asia, M.; Khader, I.A.; Herzallah, K.; Balqis, N.; Sallam, H. Seroprevalence of SARS-CoV-2 in Palestine: A cross-sectional seroepidemiological study. medRxiv 2020. [Google Scholar] [CrossRef]
- Maraqa, B.; Basha, W.; Khayyat, R.; Abdul-Hadi, A.R.; Jabareen, J.; Al-Shakhra, K.; Al-Kaila, M.; Nazzal, Z. Prevalence of SARS-CoV-2 antibodies in the Palestinian population: A primary health center-based cross-sectional study. PLoS ONE 2021, 16, e0258255. [Google Scholar] [CrossRef] [PubMed]
- Rayan, I.; Qaddomi, S.E.; Najjar, O.; Abbas, S.; Mousa, K.; Iraqi, L.; Aly, E.A.; Khader, K.A.; Barakat, A.; Salman, R. Seroprevalence of COVID-19 in Palestine in 2020. medRxiv 2021. [Google Scholar] [CrossRef]
- Sauré, D.; O’Ryan, M.; Torres, J.P.; Zuniga, M.; Santelices, E.; Basso, L.J. Dynamic IgG seropositivity after rollout of CoronaVac and BNT162b2 COVID-19 vaccines in Chile: A sentinel surveillance study. Lancet Infect. Dis. 2021, 22, 56–63. [Google Scholar] [CrossRef]
- Bellizzi, S.; Alsawalha, L.; Ali, S.S.; Sharkas, G.; Muthu, N.; Ghazo, M.; Aly, E.; Rashidian, A.; Al Ariqi, L.; Hayajneh, W.; et al. A three-phase population based sero-epidemiological study: Assessing the trend in prevalence of SARS-CoV-2 during COVID-19 pandemic in Jordan. One Health 2021, 13, 100292. [Google Scholar] [CrossRef] [PubMed]
- Clarke, K.E.; Jones, J.M.; Deng, Y.; Nycz, E.; Lee, A.; Iachan, R.; Gundlapalli, A.V.; Hall, A.J.; MacNeil, A. Seroprevalence of Infection-Induced SARS-CoV-2 Antibodies—United States, September 2021–February 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 606–608. [Google Scholar] [CrossRef] [PubMed]
- Hampshire, A.; Chatfield, D.A.; Phil, A.M.M.; Jolly, A.; Trender, W.; Hellyer, P.J.; del Giovane, M.; Newcombe, V.F.J.; Outtrim, J.G.; Warne, B.; et al. Multivariate profile and acute-phase correlates of cognitive deficits in a COVID-19 hospitalised cohort. eClinicalMedicine 2022, 47, 101417. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Location | Number of Households in each cluster(census tract) | Cumulative |
|---|---|---|
| L1 | X1 | C1 = X1 |
| L2 | X2 | C2 = X1 + X2 |
| L3 | X3 | C3 = X1 + X2 + X3 |
| Lk-1 | Xk-1 | Ck-1 = X1 + X2 + … + Xk-1 |
| Lk | Xk | Ck = X1 + X2 + … + Xk |
| Background Variable | N | % | |
|---|---|---|---|
| Gender | Male | 737 | 50.8% |
| Female | 714 | 49.2% | |
| Marital Status | Never married | 377 | 26.0% |
| Engaged | 33 | 2.3% | |
| Married | 935 | 64.4% | |
| Divorced | 21 | 1.4% | |
| Widowed | 81 | 5.6% | |
| Separated | 5 | 0.3% | |
| Highest Degree Obtained | Illiterate | 57 | 3.9% |
| Knows how to read and write | 68 | 4.7% | |
| Elementary | 216 | 14.9% | |
| Preparatory | 396 | 27.3% | |
| Secondary | 336 | 23.2% | |
| Two or one-year diploma | 81 | 5.6% | |
| Bachelor | 273 | 18.8% | |
| Higher diploma | 2 | 0.2% | |
| Masters | 18 | 1.3% | |
| Ph.D. | 3 | 0.2% | |
| Refugee Status | Registered refugee | 357 | 24.6% |
| Unregistered refugee | 15 | 1.0% | |
| Not a refugee | 1078 | 74.3% | |
| Age category in years | 18–29 | 561 | 38.6% |
| 30–49 | 568 | 39.2% | |
| 50+ | 322 | 22.2% | |
| Gender | Total | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| Antibodies test result | Negative | Count | 114 | 105 | 219 |
| % within Gender | 25.8% | 22.4% | 24.1% | ||
| Positive | Count | 328 | 363 | 691 | |
| % within Gender | 74.2% | 77.6% | 75.9% | ||
| Total | Count | 442 | 468 | 910 | |
| % within Gender | 100.0% | 100.0% | 100.0% | ||
| Chi-Square Tests | |||||
| Value | Df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |
| Pearson Chi-Square | 1.401 a | 1 | 0.237 | ||
| Continuity Correction b | 1.223 | 1 | 0.269 | ||
| Likelihood Ratio | 1.401 | 1 | 0.237 | ||
| Fisher’s Exact Test | 0.245 | 0.134 | |||
| Linear-by-Linear Association | 1.399 | 1 | 0.237 | ||
| N of Valid Cases | 910 | ||||
| Antibodies Test Results by Protein Type and Gender Crosstabulation | |||||
|---|---|---|---|---|---|
| Gender | Total | ||||
| Male | Female | ||||
| Antibody Test Results | Negative | Count | 114 | 105 | 219 |
| % within Gender | 25.8% | 22.4% | 24.1% | ||
| N-Protein Positive | Count | 186 | 289 | 475 | |
| % within Gender | 42.1% | 61.8% | 52.2% | ||
| S-Protein Positive and N-protein Negative | Count | 142 | 74 | 216 | |
| % within Gender | 32.1% | 15.8% | 23.7% | ||
| Total | Count | 442 | 468 | 910 | |
| % within Gender | 100.0% | 100.0% | 100.0% | ||
| Chi-Square Tests | |||||
| Value | df | Asymptotic Significance (2-sided) | |||
| Pearson Chi-Square | 43.405 a | 2 | 0.000 | ||
| Likelihood Ratio | 43.916 | 2 | 0.000 | ||
| Linear-by-Linear Association | 0.345 | 1 | 0.557 | ||
| N of Valid Cases | 910 | ||||
| Age Category in Years | Total | |||||
|---|---|---|---|---|---|---|
| 18–29 | 30–49 | 50+ | ||||
| Antibodies test result | Negative | Count | 113 | 71 | 35 | 219 |
| % within Age category in years | 30.8% | 22.0% | 15.8% | 24.1% | ||
| Positive | Count | 254 | 251 | 186 | 691 | |
| % within Age category in years | 69.2% | 78.0% | 84.2% | 75.9% | ||
| Total | Count | 367 | 322 | 221 | 910 | |
| % within Age category in years | 100.0% | 100.0% | 100.0% | 100.0% | ||
| Chi-Square Tests | ||||||
| Value | df | Asymptotic Significance (2-sided) | ||||
| Pearson Chi-Square | 17.986 a | 2 | 0.000 | |||
| Likelihood Ratio | 18.297 | 2 | 0.000 | |||
| Linear-by-Linear Association | 17.789 | 1 | 0.000 | |||
| N of Valid Cases | 910 | |||||
| Antibodies Test Result | Total | ||||
|---|---|---|---|---|---|
| Negative | Positive | ||||
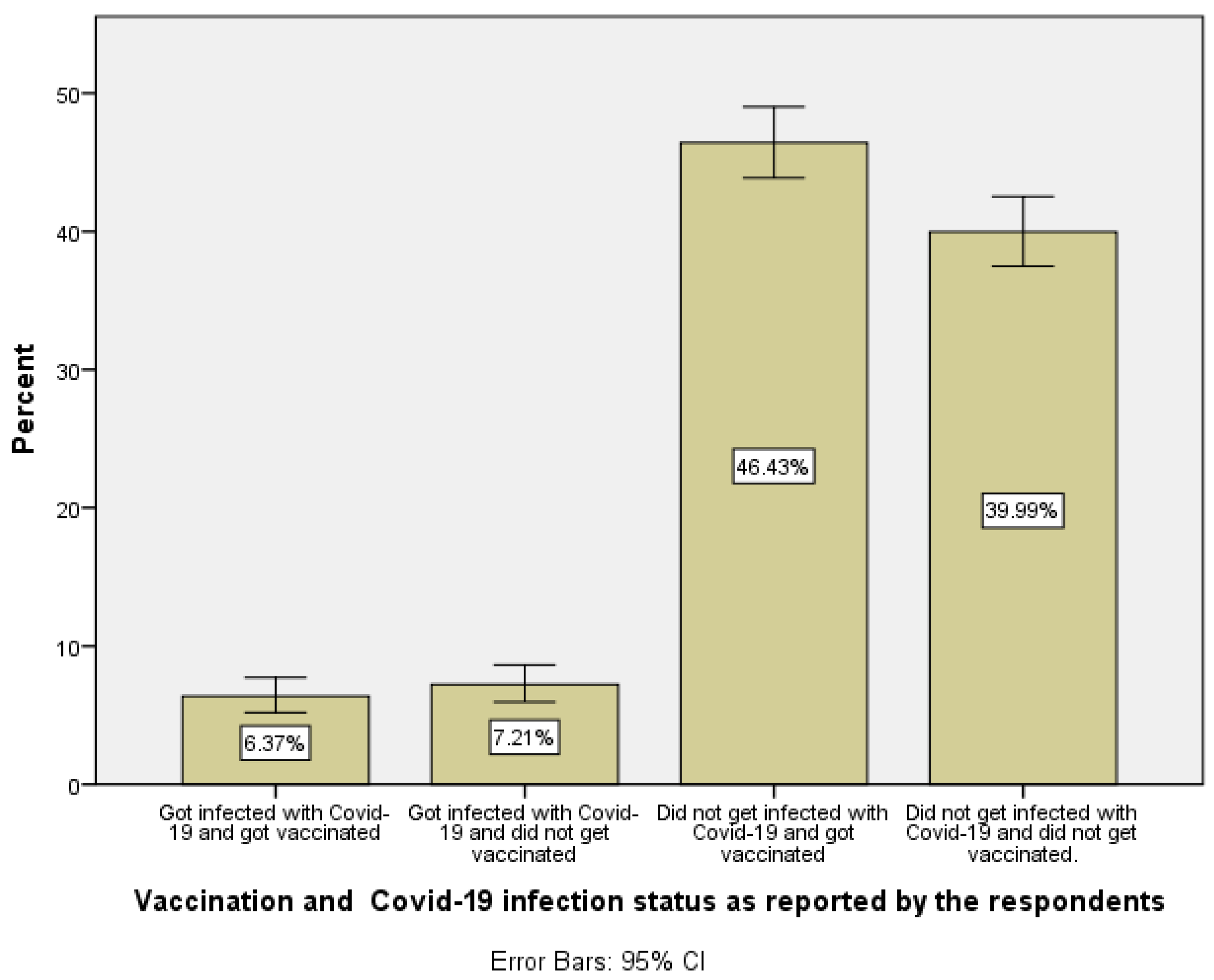
| Vaccination and COVID-19 infection status as reported by the respondents | Became infected with COVID-19 and got vaccinated | Count | 1 | 59 | 60 |
| 1.7% | 98.3% | 100.0% | |||
| Became infected with COVID-19 and did not get vaccinated | Count | 4 | 67 | 71 | |
| 5.6% | 94.4% | 100.0% | |||
| Did not become infected with COVID-19 and got vaccinated | Count | 26 | 410 | 436 | |
| 6.0% | 94.0% | 100.0% | |||
| Did not become infected with COVID-19 and did not get vaccinated. | Count | 188 | 155 | 343 | |
| 54.8% | 45.2% | 100.0% | |||
| Total | Count | 219 | 691 | 910 | |
| 24.1% | 75.9% | 100.0% | |||
| Chi-Square Tests | |||||
| Value | df | Asymptotic Significance (2-sided) | |||
| Pearson Chi-Square | 285.275 a | 3 | 0.000 | ||
| Likelihood Ratio | 294.040 | 3 | 0.000 | ||
| Linear-by-Linear Association | 62.356 | 1 | 0.000 | ||
| N of Valid Cases | 910 | ||||
| Crosstab | |||||
|---|---|---|---|---|---|
| Gender | Total | ||||
| Male | Female | ||||
| Have you been vaccinated against COVID-19? | Yes | Count | 474 | 292 | 766 |
| % within Gender | 64.3% | 40.9% | 52.8% | ||
| No | Count | 263 | 422 | 685 | |
| % within Gender | 35.7% | 59.1% | 47.2% | ||
| Total | Count | 737 | 714 | 1451 | |
| % within Gender | 100.0% | 100.0% | 100.0% | ||
| Chi-Square Tests | |||||
| Value | Df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |
| Pearson Chi-Square | 79.805 a | 1 | 0.000 | ||
| Continuity Correction b | 78.868 | 1 | 0.000 | ||
| Likelihood Ratio | 80.540 | 1 | 0.000 | ||
| Fisher’s Exact Test | 0.000 | 0.000 | |||
| Linear-by-Linear Association | 79.750 | 1 | 0.000 | ||
| N of Valid Cases | 1451 | ||||
| Crosstab | |||||
|---|---|---|---|---|---|
| Gender | Total | ||||
| Male | Female | ||||
| Name of vaccine | Pfizer | Count | 244 | 153 | 397 |
| % within Gender | 51.4% | 52.4% | 51.8% | ||
| Sputnik | Count | 12 | 7 | 19 | |
| % within Gender | 2.5% | 2.4% | 2.5% | ||
| AstraZeneca | Count | 28 | 18 | 46 | |
| % within Gender | 5.9% | 6.2% | 6.0% | ||
| Sputnik Light | Count | 120 | 87 | 207 | |
| % within Gender | 25.3% | 29.8% | 27.0% | ||
| Moderna | Count | 44 | 14 | 58 | |
| % within Gender | 9.3% | 4.8% | 7.6% | ||
| Sinopharm | Count | 19 | 12 | 31 | |
| % within Gender | 4.0% | 4.1% | 4.0% | ||
| Others | Count | 8 | 1 | 9 | |
| % within Gender | 1.7% | 0.3% | 1.2% | ||
| Total | Count | 475 | 292 | 767 | |
| % within Gender | 100.0% | 100.0% | 100.0% | ||
| Chi-Square Tests | |||||
| Value | df | Asymptotic Significance (2-sided) | |||
| Pearson Chi-Square | 9.002 a | 6 | 0.173 | ||
| Likelihood Ratio | 9.853 | 6 | 0.131 | ||
| Linear-by-Linear Association | 0.779 | 1 | 0.377 | ||
| N of Valid Cases | 767 | ||||
| Antibody Test Result by Gender Crosstabulation | |||||
|---|---|---|---|---|---|
| Gender | Total | ||||
| Male | Female | ||||
| Antibody Test Result | Negative | Count | 114 | 105 | 219 |
| % within Gender | 25.7% | 22.4% | 24.0% | ||
| positive due to infection with COVID-19 | Count | 88 | 193 | 281 | |
| % within Gender | 19.9% | 41.2% | 30.8% | ||
| positive due to vaccination | Count | 241 | 170 | 411 | |
| % within Gender | 54.4% | 36.3% | 45.1% | ||
| Total | Count | 443 | 468 | 911 | |
| % within Gender | 100.0% | 100.0% | 100.0% | ||
| Chi-Square Tests | |||||
| Value | df | Asymptotic Significance (2-sided) | |||
| Pearson Chi-Square | 51.222 a | 2 | 0.000 | ||
| Likelihood Ratio | 52.214 | 2 | 0.000 | ||
| Linear-by-Linear Association | 7.673 | 1 | 0.006 | ||
| N of Valid Cases | 911 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Awartani, F.; Qutob, N.M.; Asia, M.R. Seroprevalence of SARS-CoV-2 Antibodies among Vaccinated and Non-Vaccinated Adults in the West Bank: Results of a Repeated Cross-Sectional Study. Vaccines 2022, 10, 1332. https://doi.org/10.3390/vaccines10081332
Awartani F, Qutob NM, Asia MR. Seroprevalence of SARS-CoV-2 Antibodies among Vaccinated and Non-Vaccinated Adults in the West Bank: Results of a Repeated Cross-Sectional Study. Vaccines. 2022; 10(8):1332. https://doi.org/10.3390/vaccines10081332
Chicago/Turabian StyleAwartani, Faisal, Nouar Mohammad Qutob, and Mohammad Rajab Asia. 2022. "Seroprevalence of SARS-CoV-2 Antibodies among Vaccinated and Non-Vaccinated Adults in the West Bank: Results of a Repeated Cross-Sectional Study" Vaccines 10, no. 8: 1332. https://doi.org/10.3390/vaccines10081332