
The HACOR Score Predicts Worse in-Hospital Prognosis in Patients Hospitalized with COVID-19

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
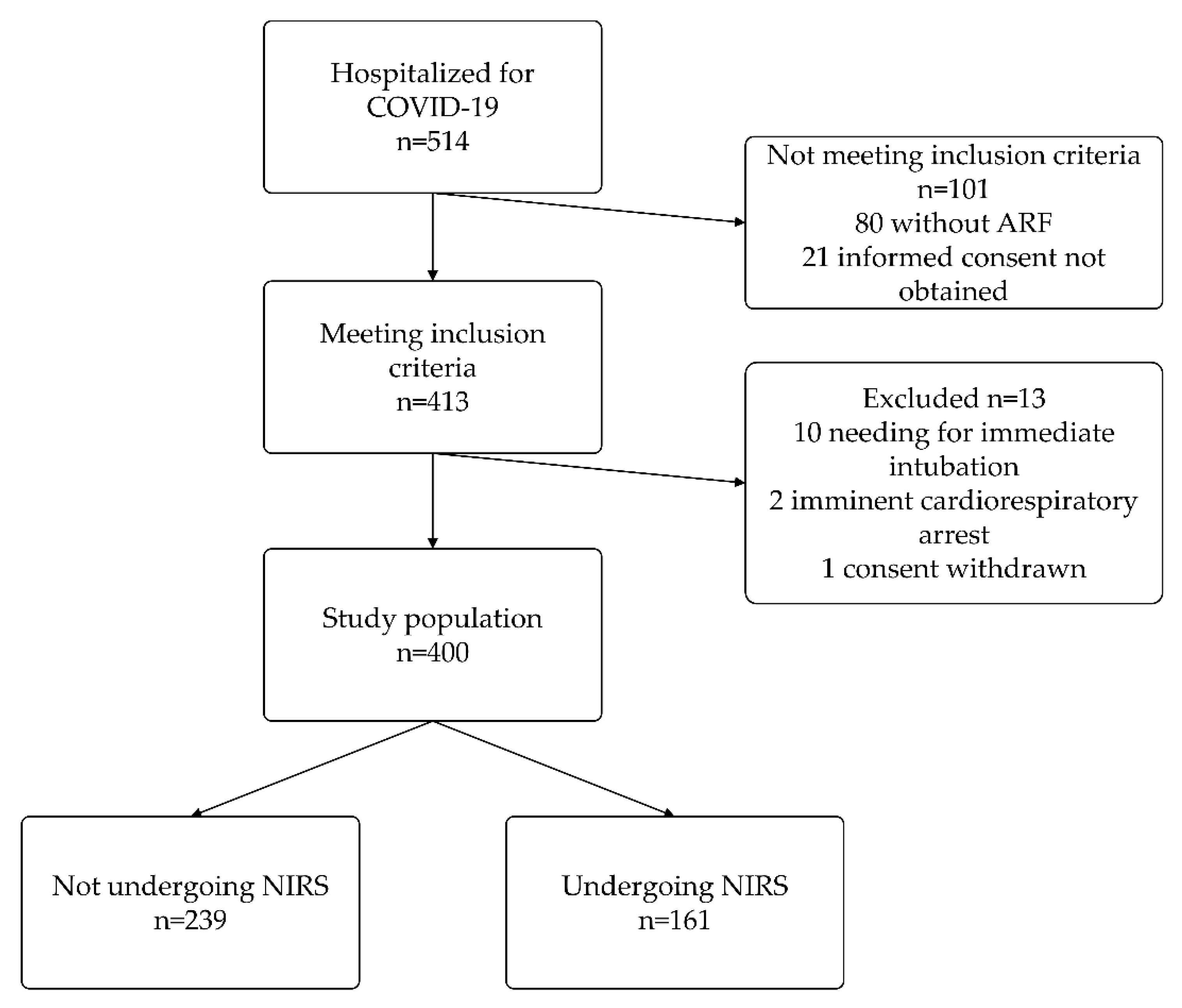
3. Results
4. Discussion
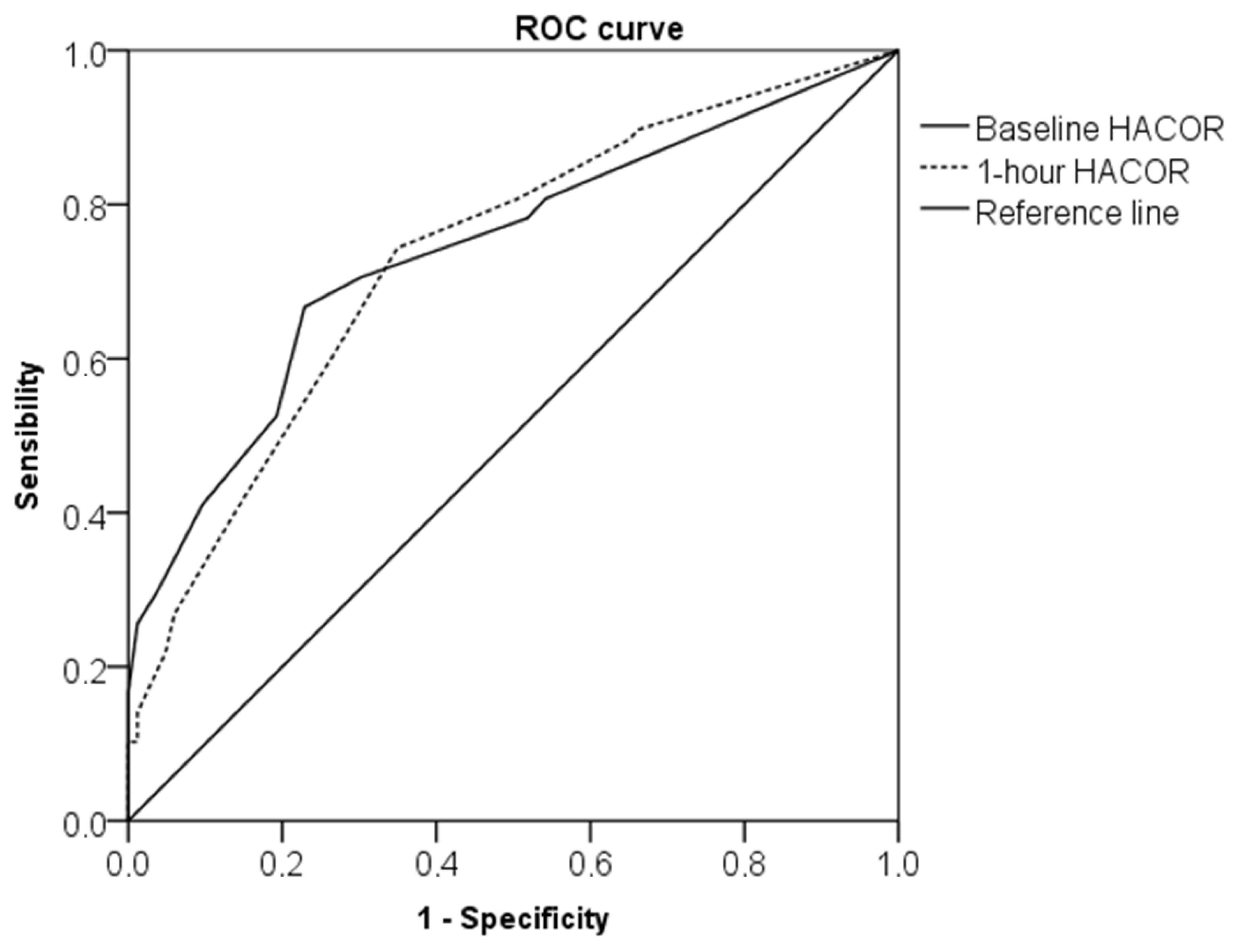
4.1. One-Hour HACOR Score as Predictor of NIRS Failure in COVID-19
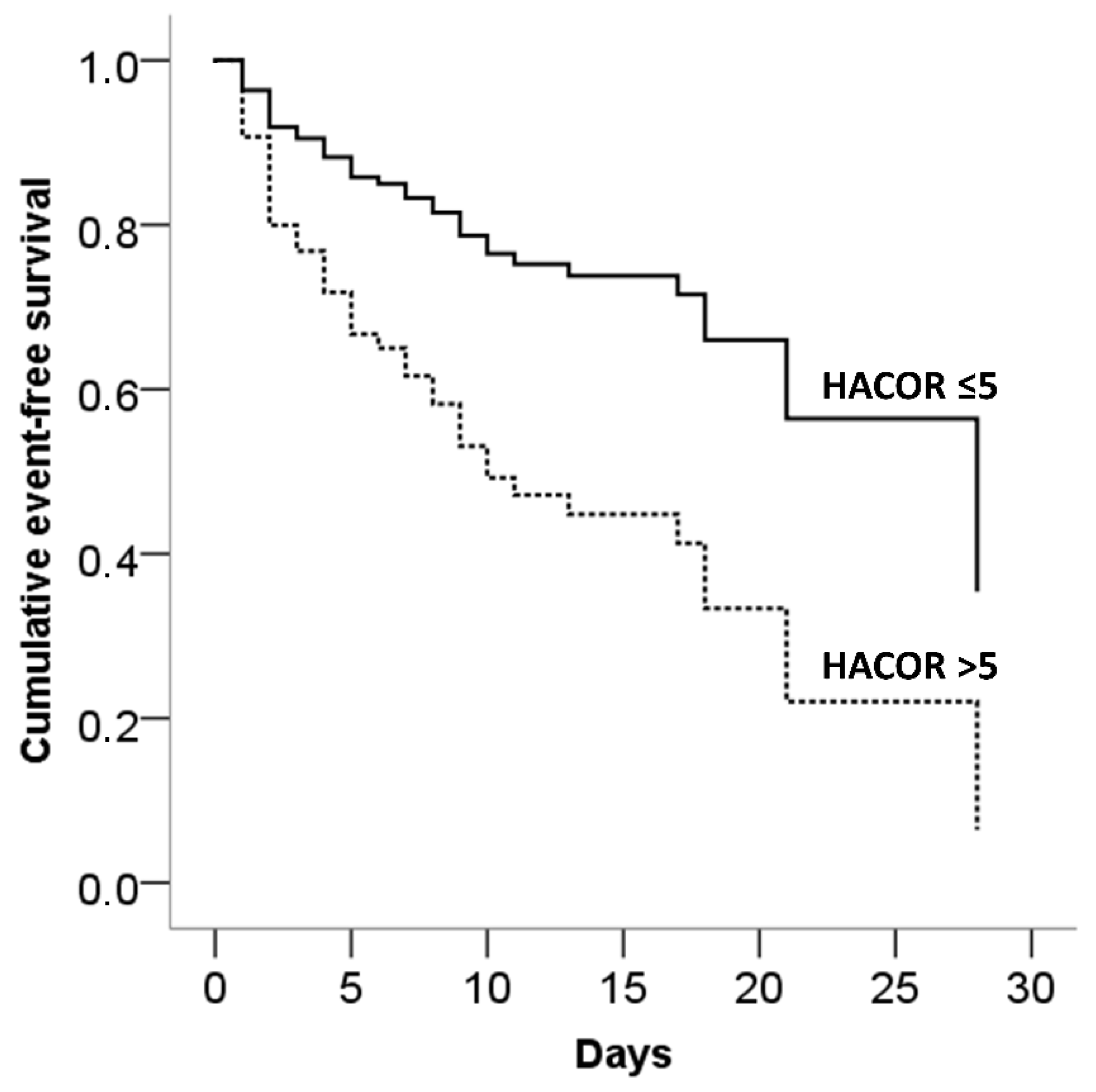
4.2. Baseline HACOR Score as Predictor of Adverse Outcome in COVID-19
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Lentz, S.; Roginski, M.A.; Montrief, T.; Ramzy, M.; Gottlieb, M.; Long, B. Initial Emergency Department Mechanical Ventilation Strategies for COVID-19 Hypoxemic Respiratory Failure and ARDS. Am. J. Emerg. Med. 2020, 38, 2194–2202. [Google Scholar] [CrossRef] [PubMed]
- Gorman, E.; Connolly, B.; Couper, K.; Perkins, G.D.; McAuley, D.F. Non-Invasive Respiratory Support Strategies in COVID-19. Lancet Respir. Med. 2021, 9, 553–556. [Google Scholar] [CrossRef]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the management of critically ill adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreyro, B.L.; Angriman, F.; Munshi, L.; Del Sorbo, L.; Ferguson, N.D.; Rochwerg, B.; Ryu, M.J.; Saskin, R.; Wunsch, H.; da Costa, B.R.; et al. Association of Noninvasive Oxygenation Strategies with All-Cause Mortality in Adults with Acute Hypoxemic Respiratory Failure. JAMA 2020, 324, 57. [Google Scholar] [CrossRef] [PubMed]
- Weerakkody, S.; Arina, P.; Glenister, J.; Cottrell, S.; Boscaini-Gilroy, G.; Singer, M.; Montgomery, H.E. Non-invasive respiratory support in the management of acute COVID-19 pneumonia: Considerations for clinical practice and priorities for research. Lancet Respir. Med. 2022, 10, 199–213. [Google Scholar] [CrossRef]
- Sullivan, Z.P.; Zazzeron, L.; Berra, L.; Hess, D.R.; Bittner, E.A.; Chang, M.G. Noninvasive respiratory support for COVID-19 patients: When, for whom, and how? J. Intensive Care 2022, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Han, X.; Bai, L.; Zhou, L.; Huang, S. Assessment of Heart Rate, Acidosis, Consciousness, Oxygenation, and Respiratory Rate to Predict Noninvasive Ventilation Failure in Hypoxemic Patients. Intensive Care Med. 2017, 43, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Innocenti, F.; Giordano, L.; Gualtieri, S.; Gandini, A.; Taurino, L.; Nesa, M.; Gigli, C.; Becucci, A.; Coppa, A.; Tassinari, I.; et al. Prediction of Mortality with the Use of Noninvasive Ventilation for Acute Respiratory Failure. Respir. Care 2020, 65, 1847–1856. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Han, X.; Bai, L.; Huang, S.; Duan, J. Impact of HACOR Score on Noninvasive Ventilation Failure in Non-COPD Patients with Acute-on-Chronic Respiratory Failure. Can. Respir. J. 2021, 2021, 9960667. [Google Scholar] [CrossRef] [PubMed]
- Guia, M.F.; Boléo-Tomé, J.P.; Imitazione, P.; Polistina, G.E.; Alves, C.; Ishikawa, O.; Ballenberger, M.; Mina, B.; Fiorentino, G.; Esquinas, A.; et al. Usefulness of the HACOR Score in Predicting Success of CPAP in COVID-19-Related Hypoxemia. Respir. Med. 2021, 187, 106550. [Google Scholar] [CrossRef] [PubMed]
- Valencia, C.F.; Lucero, O.D.; Castro, O.C.; Sanko, A.A.; Olejua, P.A. Comparison of ROX and HACOR Scales to Predict High-Flow Nasal Cannula Failure in Patients with SARS-CoV-2 Pneumonia. Sci. Rep. 2021, 11, 22559. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, A.; Lopez, A.; Carrillo, L.; Caldeira, V.; Guia, M.; Alonso, N.; Renedo, A.; Quintana, M.E.; Sanchez, J.M.; Esquinas, A. Validity of a Clinical Scale in Predicting the Failure of Non-Invasive Ventilation in Hypoxemic Patients. J. Crit. Care 2020, 60, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Van der Net, J.B.; Janssens, A.C.J.W.; Eijkemans, M.J.C.; Kastelein, J.J.P.; Sijbrands, E.J.G.; Steyerberg, E.W. Cox Proportional Hazards Models Have More Statistical Power than Logistic Regression Models in Cross-Sectional Genetic Association Studies. Eur. J. Hum. Genet. 2008, 16, 1111–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrillo, A.; Gonzalez-Diaz, G.; Ferrer, M.; Martinez-Quintana, M.E.; Lopez-Martinez, A.; Llamas, N.; Alcazar, M.; Torres, A. Non-Invasive Ventilation in Community-Acquired Pneumonia and Severe Acute Respiratory Failure. Intensive Care Med. 2012, 38, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Demoule, A.; Girou, E.; Richard, J.-C.; Taille, S.; Brochard, L. Benefits and Risks of Success or Failure of Noninvasive Ventilation. Intensive Care Med. 2006, 32, 1756–1765. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; Lam, E.C.; Astudillo, M.G.; Yang, D.; Miller, T.E.; Feldman, J.; Hauser, B.M.; Caradonna, T.M.; Clayton, K.L.; Nitido, A.D.; et al. COVID-19-Neutralizing Antibodies Predict Disease Severity and Survival. Cell 2021, 184, 476–488.e11. [Google Scholar] [CrossRef] [PubMed]
- Marin, B.G.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Values | Points |
|---|---|---|
| Heart rate, beats per minute | ≤120 | 0 |
| >120 | 1 | |
| pH | ≥7.35 | 0 |
| 7.30–7.34 | 2 | |
| 7.25–7.29 | 3 | |
| <7.25 | 4 | |
| Glasgow coma scale | 15 | 0 |
| 13–14 | 2 | |
| 11–12 | 5 | |
| ≤10 | 10 | |
| PaO2/FiO2 ratio | ≥201 | 0 |
| 176–200 | 2 | |
| 151–175 | 3 | |
| 126–150 | 4 | |
| 101–125 | 5 | |
| ≤100 | 6 | |
| Respiratory rate, breaths per minute | ≤30 | 0 |
| 31–35 | 1 | |
| 36–40 | 2 | |
| 41–45 | 3 | |
| ≥46 | 4 |
| Total (n = 400) | Baseline HACOR Score > 5 (n = 81) | Baseline HACOR Score ≤ 5 (n = 319) | p | |
|---|---|---|---|---|
| Age, mean (SD), years | 75 (14) | 82 (11) | 73 (15) | <0.001 |
| Male gender, No. (%) | 218 (55) | 44 (53) | 169 (55) | 0.775 |
| BMI, mean (SD), kg/m2 | 27 (8) | 25 (4) | 27 (8) | <0.001 |
| Current smoking, No. (%) | 54 (16) | 7 (7) | 55 (17) | 0.012 |
| Hypertension, No. (%) | 251 (63) | 51 (63) | 193 (63) | 0.965 |
| Type 2 diabetes, No. (%) | 79 (20) | 16 (20) | 62 (20) | 0.999 |
| Obesity, No. (%) | 125 (32) | 19 (22) | 105 (34) | 0.023 |
| CKD, No. (%) | 47 (12) | 9 (10) | 37 (12) | 0.538 |
| Previous CV event, No. (%) | 66 (17) | 15 (19) | 51 (16) | 0.654 |
| Active cancer, No. (%) | 33 (8) | 9 (11) | 22 (8) | 0.349 |
| Previous VTE, No. (%) | 13 (3) | 3 (4) | 9 (3) | 0.807 |
| AF, No. (%) | 58 (14) | 12 (17) | 42 (14) | 0.454 |
| COPD, No. (%) | 48 (12) | 10 (12) | 36 (12) | 0.916 |
| CCI, median (IQR) | 4 (3–6) | 5 (4–7) | 4 (2–6) | <0.001 |
| Anti-hypertensives, No. (%) | 260 (67) | 57 (70) | 203 (66) | 0.464 |
| Statins, No. (%) | 69 (18) | 14 (16) | 56 (18) | 0.680 |
| Anticoagulants, No. (%) | 127 (33) | 38 (46) | 90 (29) | 0.009 |
| Anti-platelets, No. (%) | 100 (25) | 26 (32) | 71 (23) | 0.123 |
| Insulin, No. (%) | 46 (12) | 9 (10) | 37 (12) | 0.703 |
| Oral hypoglycemic agents, No. (%) | 43 (11) | 9 (11) | 34 (10) | 0.841 |
| SBP, mean (SD), mmHg | 131 (20) | 125 (23) | 132 (19) | 0.012 |
| DBP, mean (SD), mmHg | 76 (11) | 74 (12) | 77 (11) | 0.072 |
| PaO2/FiO2, median (IQR) | 227 (156–276) | 119 (91–155) | 247 (195–284) | <0.001 |
| Hb, median (IQR), g/dL | 13.3 (11.9–14.5) | 13.1 (11.4–14.4) | 13.5 (12–14.5) | 0.364 |
| Leukocytes, median (IQR), ×103/μL | 7.5 (5.3–11.0) | 9.5 (6.6–13.2) | 7.1 (5–10.3) | <0.001 |
| Platelets, median (IQR), ×103/μL | 208 (154–270) | 212 (144–283) | 202 (154–264) | 0.825 |
| D-dimer, median (IQR), ng/mL | 936 (578–1788) | 1389 (724–2939) | 891 (571–1649) | 0.003 |
| hs-cTn, median (IQR), ng/L | 14.3 (7.6–32.7) | 28.3 (12.8–44) | 13 (7–26.6) | <0.001 |
| CRP, median (IQR), mg/dL | 7.6 (4–13.3) | 10.1 (4.6–16.9) | 7.3 (3.9–12.2) | 0.025 |
| Fasting glucose, median (IQR), mg/dL | 124 (106–154) | 132 (110–158) | 123 (106–154) | 0.263 |
| eGFR, mean (SD), mL/min | 69 (25) | 57 (26) | 72 (24) | <0.001 |
| LDH, median (IQR), UI/L | 323 (245–431) | 400 (255–474) | 313 (245–419) | 0.019 |
| SOFA score, median (IQR) | 3 (2–4) | 5 (4–6) | 2 (2–4) | <0.001 |
| NIRS, No. (%) | 161 (40) | 40 (49) | 121 (38) | 0.068 |
| PSV, No (%) | 90 (23) | 27 (33) | 63 (16) | 0.083 |
| CPAP, No (%) | 51 (13) | 9 (11) | 42 (13) | 0.298 |
| Helmet-CPAP, No (%) | 10 (3) | 2 (2) | 8 (3) | 0.716 |
| High flow nasal oxygenation, No (%) | 10 (3) | 1 (1) | 9 (3) | 0.157 |
| Number of Patients with Baseline HACOR ≤ 5 with/without Event | Number of Patients with Baseline HACOR > 5 with/without Event | Model 1 HR (95% CI) p Value | Model 2 HR (95% CI) p Value | Model 3 HR (95% CI) p Value | |
|---|---|---|---|---|---|
| Need for intubation/in-hospital death | |||||
| All patients | 70/249 | 55/26 | 3.62 (2.54, 5.16) p < 0.001 | 3.91 (2.62, 5.83) p < 0.001 | 4.32 (2.35, 7.92) p < 0.001 |
| NIRS | 46/75 | 32/8 | 2.76 (1.75, 4.34) p < 0.001 | 3.18 (1.88, 5.37) p < 0.001 | 5.17 (2.05, 13.02) p < 0.001 |
| No-NIRS | 24/174 | 23/18 | 4.75 (2.68, 8.43) p < 0.001 | 3.70 (1.99, 6.87) p < 0.001 | 7.87 (2.42, 25.63) p < 0.001 |
| In-hospital death | |||||
| All patients | 47/272 | 51/30 | 4.91 (3.30, 7.30) p < 0.001 | 4.03 (2.60, 6.22) p < 0.001 | 3.50 (1.83, 6.70) p < 0.001 |
| NIRS | 26/95 | 28/12 | 4.15 (2.43, 7.09) p < 0.001 | 3.70 (1.97, 6.95) p < 0.001 | 3.76 (1.24, 11.40) p = 0.019 |
| No-NIRS | 21/177 | 23/18 | 5.56 (3.07, 10.05) p < 0.001 | 3.77 (2.02, 7.04) p < 0.001 | 9.96 (2.86, 34.66) p < 0.001 |
| Number of Patients with 1-h HACOR ≤ 5 with/without Event | Number of Patients with 1-h HACOR > 5 with/without Event | Model 1 HR (95% CI) p Value | Model 2 HR (95% CI) p Value | Model 3 HR (95% CI) p Value | |
|---|---|---|---|---|---|
| Need for intubation/in-hospital death | 46/71 | 32/12 | 2.17 (1.38, 3.42) p < 0.001 | 2.50 (1.45, 4.30) p < 0.001 | 2.64 (1.05, 6.65) p = 0.039 |
| In-hospital death | 29/88 | 25/19 | 2.51 (1.46, 4.31) p < 0.001 | 2.23 (1.19, 4.19) p = 0.012 | 4.37 (1.34, 14.23) p = 0.014 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannarino, M.R.; Bianconi, V.; Cosentini, E.; Figorilli, F.; Natali, C.; Cellini, G.; Colangelo, C.; Giglioni, F.; Braca, M.; Pirro, M. The HACOR Score Predicts Worse in-Hospital Prognosis in Patients Hospitalized with COVID-19. J. Clin. Med. 2022, 11, 3509. https://doi.org/10.3390/jcm11123509
Mannarino MR, Bianconi V, Cosentini E, Figorilli F, Natali C, Cellini G, Colangelo C, Giglioni F, Braca M, Pirro M. The HACOR Score Predicts Worse in-Hospital Prognosis in Patients Hospitalized with COVID-19. Journal of Clinical Medicine. 2022; 11(12):3509. https://doi.org/10.3390/jcm11123509
Chicago/Turabian StyleMannarino, Massimo Raffaele, Vanessa Bianconi, Elena Cosentini, Filippo Figorilli, Costanza Natali, Giulia Cellini, Cecilia Colangelo, Francesco Giglioni, Marco Braca, and Matteo Pirro. 2022. "The HACOR Score Predicts Worse in-Hospital Prognosis in Patients Hospitalized with COVID-19" Journal of Clinical Medicine 11, no. 12: 3509. https://doi.org/10.3390/jcm11123509