
Daily Life Patterns, Psychophysical Conditions, and Immunity of Adolescents in the COVID-19 Era: A Mixed Research with Qualitative Interviews by a Quasi-Experimental Retrospective Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Ethical Approval
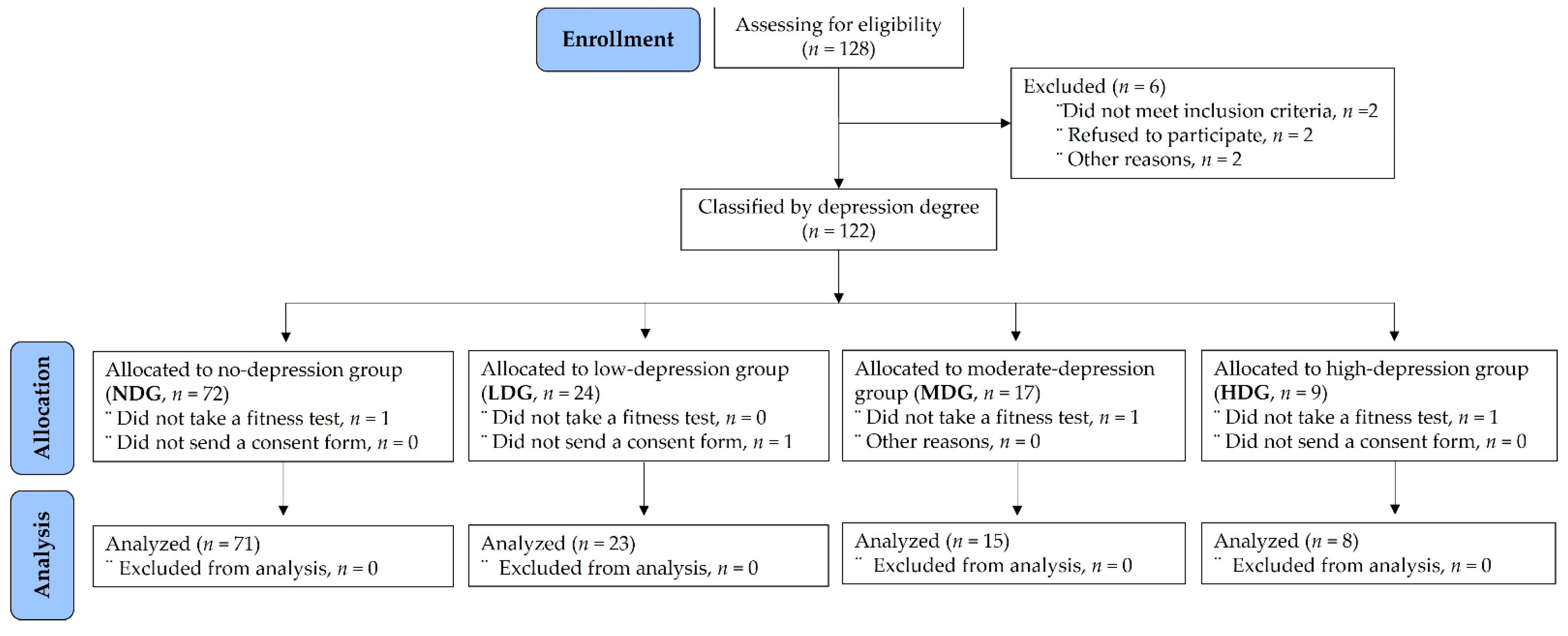
2.3. Subjects
2.4. Measurement Methods
2.4.1. Daily Life Pattern Questionnaire
2.4.2. CES-D Questionnaire Measures
2.4.3. Qualitative Interview Measures
First, are there any changes in your daily life due to the COVID-19 pandemic?
Second, are there any mental changes caused by the COVID-19 pandemic?
Third, are there any physical changes caused by the COVID-19 pandemic?
Lastly, how have you dealt with those changes?
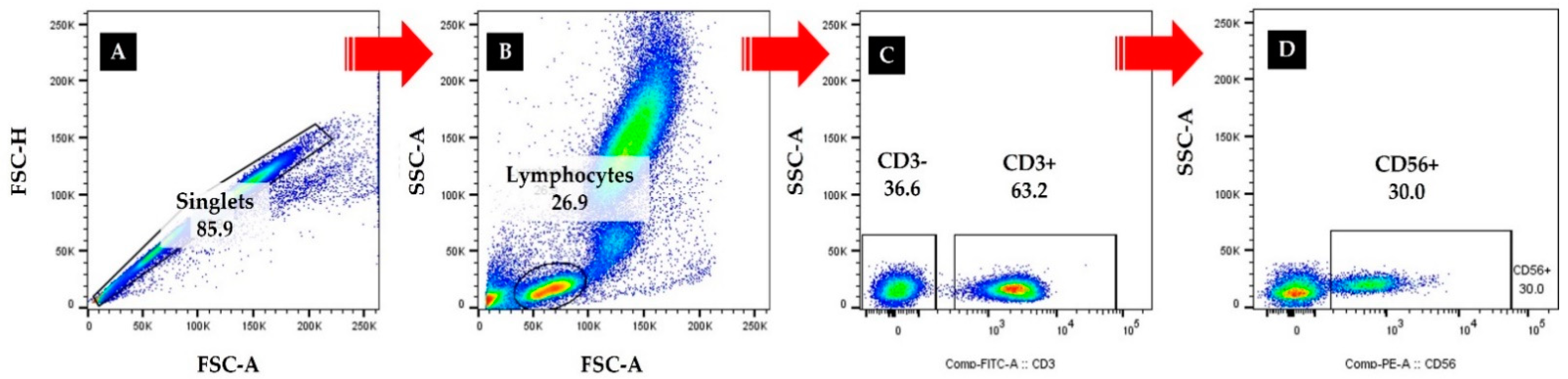
2.4.4. Immunocytes Measures
2.4.5. Body Composition Measures
2.4.6. Physical Fitness Measures
2.5. Sample Size and Data Analyses
3. Results
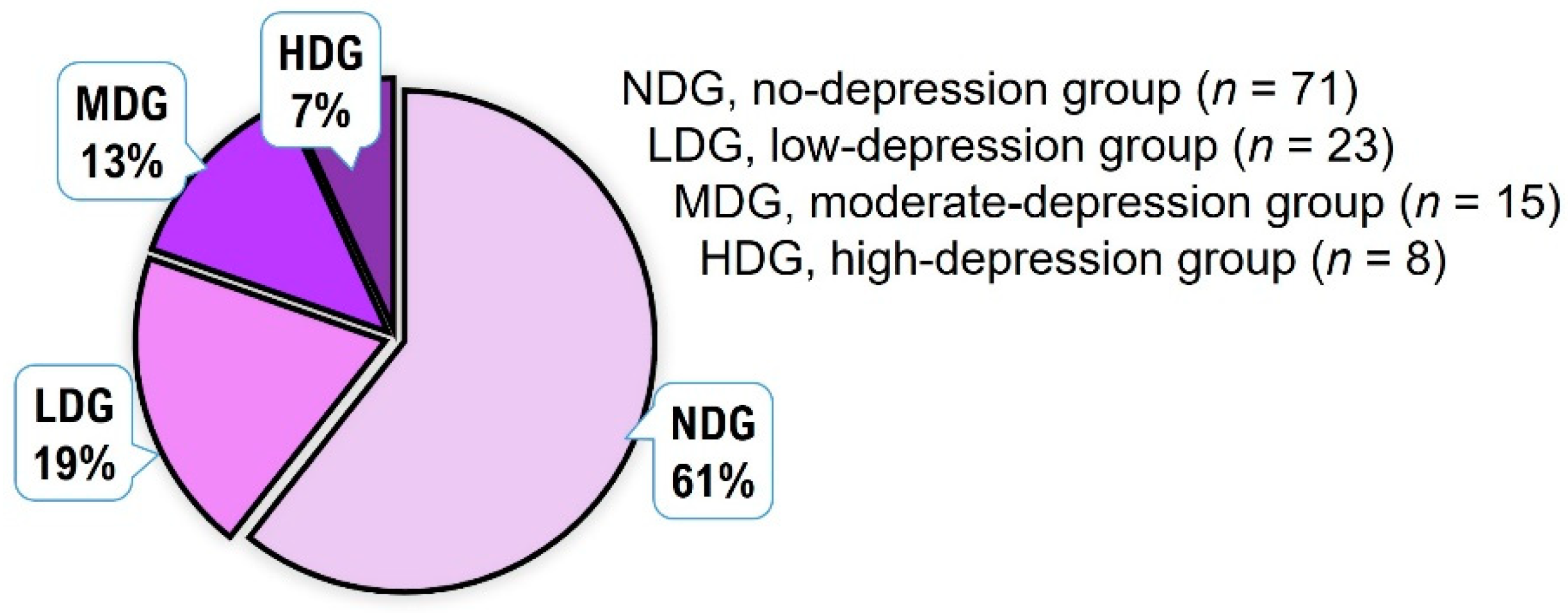
3.1. Frequency Analysis for Depression
3.2. Analysis of Daily Life Pattern
3.3. Analysis of Body Composition
3.4. Analysis of Psychological Condition
3.5. Analysis of Physical Fitness
3.6. Analysis of Immunocytes
4. Discussion
“Compared to pre-pandemic life, the situation has drastically changed because of online classes. I didn’t have to go to school, so I wasn’t nervous. During online classes, I couldn’t hear what they were talking about, so I just fell asleep.” Interview: a student (YOO)
“I slept a lot because I didn’t have to go to school. Of course, I slept even when it was time to eat. And, in the evening, I couldn’t sleep and had more time to play games. It seems that I ate ramen almost every day because I was hungry after playing games until dawn.” Interview: a student (KOO)
“At first, I didn’t go to school, so I felt good, and it was a different feeling. However, day by day, I became more anxious. I had to do something, but I did not know what to do”. Interview: a student (POO)
“When I first got into a lifestyle I wasn’t used to, I didn’t know what to do. As the number of corona patients continued to increase, I was afraid to go outside. When I saw the news, I was very afraid of the fact that the number of deaths was increasing while teenagers were not receiving vaccinations. That’s why I hated doing anything”. Interview: a student (LOO)
“The online exercise was fun, though it was difficult at first. After exercising, I slept well and woke up in the morning. I thought it was better than doing nothing, so I continued”. Interview: a student (POO)
“My friends and I had a good time following the teacher’s exercises on our smartphones. It was fun... Anyways, it was good that we were the only ones doing things that other school kids couldn’t... It was a fun time.” Interview: a student (COO)
“I walked on the playground with my parents wearing a mask. I felt a lot different than when I walked without a mask... I had to take care of my health, so I tried to exercise regularly... Anyway, I tried to keep doing it, thinking that it is better than not doing it”. Interview: a student (KOO)
“In fact, we thought Corona was like a cold, so we used to run around the playground. Of course, I used to wear a mask over my chin... Most of the other children didn’t even cover their noses and mouths with a mask... It was also very stuffy, and the mask was wet with sweat. But playing soccer with friends is fun, so it’s good to pass the time.” Interview: a student (COO)
“Because of the pandemic compared with the pre-COVID 19, I can’t go out often to meet my friends... I’m gaining more and more weight, my energy levels are low, and I don’t want to do anything.... Also, although it’s not Corona, I caught a cold easily and didn’t get better even if I took medicine...” Interview: a student (LOO)
“I couldn’t work out, so I tried to cut down on what I ate, but I gained weight. I need to study... I hate to do it... I fall asleep... but when I try to sleep, I can’t sleep.... Maybe it’s because I can’t move well... My fingers and knee joints are sore...” Interview: a student (POO)
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Viana, R.B.; de Lira, C.A.B. Exergames as coping strategies for anxiety disorders during the COVID-19 quarantine period. Games Health J. 2020, 9, 147–149. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 2 March 2022).
- Ko, C.H.; Yen, C.F.; Yen, J.Y.; Yang, M.J. Psychosocial impact among the public of the severe acute respiratory syndrome epidemic in Taiwan. Psychiatry Clin. Neurosci. 2006, 60, 397–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuch, F.B.; Stubbs, B.; Meyer, J.; Heissel, A.; Zech, P.; Vancampfort, D.; Rosenbaum, S.; Deenik, J.; Firth, J.; Ward, P.B.; et al. Physical activity protects from incident anxiety: A meta-analysis of prospective cohort studies. Depress. Anxiety 2019, 36, 846–858. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; De Leon, A.P.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef]
- Qu, Z.; Wang, C.W.; Zhang, X.; Ho, A.H.; Wang, X. Prevalence and determinants of depression among survivors 8 months after the Wenchuan earthquake. J. Nerv. Ment. Dis. 2014, 202, 275–279. [Google Scholar] [CrossRef]
- Barchard, K.A.; Grob, K.E.; Roe, M.J. Is sadness blue? The problem of using figurative language for emotions on psychological tests. Behav. Res. 2017, 49, 443–456. [Google Scholar] [CrossRef] [Green Version]
- Ehlers, A.; Clark, D.M. A cognitive model of posttraumatic stress disorder. Behav. Res. Ther. 2000, 38, 319–345. [Google Scholar] [CrossRef]
- Xu, W.; Fu, G.; An, Y.; Yuan, G.; Ding, X.; Zhou, Y. Mindfulness, posttraumatic stress symptoms, depression, and social functioning impairment in Chinese adolescents following a tornado: Mediation of posttraumatic cognitive change. Psychiatry Res. 2018, 259, 345–349. [Google Scholar] [CrossRef]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; Vancampfort, D.; Firth, J.; Stubbs, B.; Grabovac, I.; Willeit, P.; Tavares, V.D.O.; Calegaro, V.C.; et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Res. 2020, 292, 113339. [Google Scholar] [CrossRef]
- Min, S.K.; Son, W.H.; Choi, B.H.; Lee, H.J.; Ahn, C.Y.; Yoo, J.; Park, S.; Lee, J.W.; Jee, Y.S. Psychophysical condition of adolescents in coronavirus disease 2019. J. Exerc. Rehabil. 2021, 17, 112–119. [Google Scholar] [CrossRef]
- Heo, S.J.; Park, S.K.; Jee, Y.S. Detraining Effects of COVID-19 Pandemic on Physical Fitness, Cytokines, C-Reactive Protein and Immunocytes in Men of Various Age Groups. Int. J. Environ. Res. Public Health 2022, 19, 1845. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Jacob, L.; Butler, L.; Schuch, F.; Barnett, Y.; Grabovac, I.; Veronese, N.; Caperchione, C.; Lopez-Sanchez, G.F.; Meyer, J. Prevalence and correlates of physical activity in a sample of UK adults observing social distancing during the COVID-19 pandemic. BMJ Open Sport Exerc. Med. 2020, 6, e000850. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.; Khalesi, S.; Williams, S.; Alley, S.; Thwaite, T.; Fenning, A.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Hallgren, M.; Owen, N.; Vancampfort, D.; Dunstan, D.W.; Wallin, P.; Andersson, G.; Ekblom-Bak, E. Associations of sedentary behavior in leisure and occupational contexts with symptoms of depression and anxiety. Prev. Med. 2020, 133, 106021. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Lesser, I.A.; Nienhuis, C.P. The impact of COVID-19 on physical activity behavior and well-being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef] [PubMed]
- Kite, C.; Lagojda, L.; Clark, C.C.T.; Uthman, O.; Denton, F.; McGregor, G.; Harwood, A.E.; Atkinson, L.; Broom, D.R.; Kyrou, I.; et al. Changes in Physical Activity and Sedentary Behaviour Due to Enforced COVID-19-Related Lockdown and Movement Restrictions: A Protocol for a Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 5251. [Google Scholar] [CrossRef]
- Rogers, N.; Waterlow, N.; Brindle, H.; Enria, L.; Eggo, R.; Lees, S.; Roberts, C. Behavioural change towards reduced intensity physical activity is disproportionately prevalent among adults with serious health issues or self-perception of high risk during the UK COVID-19 lockdown. Front. Public Health 2020, 8, 575091. [Google Scholar] [CrossRef]
- Zhai, L.; Zhang, Y.; Zhang, D. Sedentary behaviour and the risk of depression: A meta-analysis. Br. J. Sports Med. 2015, 49, 705–709. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Spradley, J.P. Participant Observation; Holt, Rinehart and Winston: New York, NY, USA, 1980. [Google Scholar]
- Silverman, D. Interpreting Qualitative Research. In Methods for Analysing Talk, Text and Interaction, 2nd ed.; Sage: London, UK, 2001. [Google Scholar]
- Yoon, T.H.; Mun, Y.K.; Lee, J.S.; Min, S.K.; Jee, Y.S. Analysis for reliability and validity of gross motor function and health fitness tests for children with developmental disabilities. J. Exerc. Rehabil. 2019, 15, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Education Limited: London, UK, 2014. [Google Scholar]
- Korean Health Insurance Review and Assessment Service. Available online: https://www.hira.or.kr/dummy.do?ilnsCtgyNm=sixtyAge&pgmid=HIRAA030502030000&sortSno=46 (accessed on 6 April 2022).
- Jiao, W.Y.; Wang, L.N.; Liu, J.; Fang, S.F.; Jiao, F.Y.; Pettoello-Mantovani, M.; Somekh, E. Behavioral and emotional disorders in children during the COVID-19 epidemic. J. Pediatr. 2020, 221, 264–266.e1. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Pinto, A.J.; Dunstan, D.W.; Owen, N.; Bonfa, E.; Gualano, B. Combating physical inactivity during the COVID-19 pandemic. Nat. Rev. Rheumatol. 2020, 16, 347–348. [Google Scholar] [CrossRef]
- Xiang, M.; Zhang, Z.; Kuwahara, K. Impact of COVID-19 pandemic on children and adolescents’ lifestyle behavior larger than expected. Prog. Cardiovasc. Dis. 2020, 63, 531–532. [Google Scholar] [CrossRef]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19–related school closings and risk of weight gain among children. Obesity 2020, 28, 1008–1009. [Google Scholar] [CrossRef] [Green Version]
- Sharp, C.; Vanwoerden, S.; Wall, K. Adolescence as a Sensitive Period for the Development of Personality Disorder. Psychiatr. Clin. N. Am. 2018, 41, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Heo, S.J.; Hyun, G.S.; Park, S.K.; Cha, J.Y.; Jee, Y.S. Elbow plank exercise improves immunocyte function and physical fitness in an elderly male: A case study. J. Mens. Health 2022, 18, 084. [Google Scholar] [CrossRef]
- Park, S.K.; Lee, K.S.; Heo, S.J.; Jee, Y.S. Effects of high intensity plank exercise on physical fitness and immunocyte function in a middle-aged man: A case report. Medicina 2021, 57, 845. [Google Scholar] [CrossRef] [PubMed]
- Elliott, S.; Drummond, M.J.; Prichard, I.; Eime, R.; Drummond, C.; Mason, R. Understanding the impact of COVID-19 on youth sport in Australia and consequences for future participation and retention. BMC Public Health 2021, 21, 448. [Google Scholar] [CrossRef]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. Pandemic fear and COVID-19: Mental health burden and strategies. Braz. J. Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Mendoza-Muñoz, M.; Adsuar, J.C.; Pérez-Gómez, J.; Muñoz-Bermejo, L.; Garcia-Gordillo, M.Á.; Carlos-Vivas, J. Influence of body composition on physical fitness in adolescents. Medicina 2020, 56, 328. [Google Scholar] [CrossRef]
- Wind, A.E.; Takken, T.; Helders, P.J.; Engelbert, R.H. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur. J. Pediatr. 2010, 169, 281–287. [Google Scholar] [CrossRef]
- Peake, J.; Nosaka, K.K.; Suzuki, K. Characterization of inflammatory responses to eccentric exercise in humans. Exerc. Immunol. Rev. 2005, 11, 64–85. [Google Scholar] [PubMed]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2016, 444, 860–867. [Google Scholar] [CrossRef]
- Gruver, A.L.; Hudson, L.L.; Sempowski, G.D. Immunosenescence of ageing. J. Pathol. 2007, 211, 144–156. [Google Scholar] [CrossRef]
- Eagle, R.A.; Trowsdale, J. Promiscuity and the single receptor: NKG2D. Nat. Rev. Immunol. 2007, 7, 737–744. [Google Scholar] [CrossRef] [PubMed]
- Infante, J.R.; Peran, F.; Rayo, J.I.; Serrano, J.; Domínguez, M.L.; Garcia, L.; Duran, C.; Roldan, A. Levels of immune cells in transcendental meditation practitioners. Int. J. Yoga 2014, 7, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.J.; Campbell, J.P.; Gleeson, M.; Krüger, K.; Nieman, D.C.; Pyne, D.B.; Turner, J.E.; Walsh, N.P. Can exercise affect immune function to increase susceptibility to infection? Exerc. Immunol. Rev. 2020, 26, 8–22. [Google Scholar] [PubMed]
- Duggal, N.A.; Niemiro, G.; Harridge, S.D.R.; Simpson, R.J.; Lord, J.M. Can physical activity ameliorate immunosenescence and thereby reduce age-related multi-morbidity? Nat. Rev. Immunol. 2019, 19, 563–572. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | |||||||
|---|---|---|---|---|---|---|---|
| NDG | LDG | MDG | HDG | F | p | η² | |
| Q1. How healthy do you think you are? | 3.19 ± 1.39 a | 2.76 ± 1.22 b | 2.36 ± 0.93 b | 1.57 ± 0.79 c | 4.603 | 0.005 | 0.114 |
| Q2. Are you prone to respiratory diseases such as colds? | 3.59 ± 1.35 a | 3.05 ± 1.20 a | 2.36 ± 0.74 b | 1.43 ± 0.53 c | 9.463 | 0.001 | 0.210 |
| Q3. How many hours per day do you sleep on average? | 3.49 ± 0.97 | 3.39 ± 1.12 | 3.00 ± 1.13 | 2.63 ± 1.51 | 2.126 | 0.101 | 0.054 |
| Q4. What time do you usually sleep? | 3.93 ± 0.80 b | 3.83 ± 1.03 b | 4.60 ± 0.99 a | 4.75 ± 0.46 a | 4.720 | 0.004 | 0.112 |
| Q5. What time do you usually wake up? | 4.90 ± 0.59 | 4.78 ± 0.80 | 4.60 ± 0.51 | 4.63 ± 0.52 | 1.541 | 0.208 | 0.040 |
| Q6. How many meals do you eat per day? | 2.86 ± 0.62 b | 2.65 ± 0.57 b | 2.93 ± 0.80 b | 4.25 ± 0.71 a | 11.487 | 0.001 | 0.235 |
| Q7. How many days a week do you exercise for at least 30 min a day? | 3.41 ± 1.61 a | 2.87 ± 1.60 b | 2.67 ± 1.40 b | 1.38 ± 0.52 c | 6.393 | 0.001 | 0.146 |
| Groups | |||||||
|---|---|---|---|---|---|---|---|
| NDG | LDG | MDG | HDG | F | p | η² | |
| Height (cm) | 164.99 ± 13.97 | 163.67 ± 7.17 | 163.14 1 ± 8.17 | 167.15 ± 7.54 | 0.268 | 0.849 | 0.007 |
| Body weight (kg) | 60.04 ± 13.28 b | 57.85 ± 11.19 b,c | 54.12 ± 10.67 c | 71.76 ± 15.88 a | 5.505 | 0.018 | 0.085 |
| Muscle mass (kg) | 25.89 ± 6.31 a | 22.69 ± 4.82 b | 22.61 ± 5.60 b | 19.58 ± 5.06 c | 18.857 | 0.001 | 0.336 |
| Fat mass (kg) | 14.59 ± 5.06 d | 16.90 ± 5.63 b,c | 15.18 ± 6.50 b,c | 24.18 ± 11.13 a | 5.870 | 0.001 | 0.136 |
| BMI (kg/m²) | 21.29 ± 3.53 b | 21.34 ± 3.40 b | 21.17 ± 3.11 b | 26.10 ± 4.26 a | 4.691 | 0.004 | 0.112 |
| Percent fat (%) | 21.45 ± 7.09 c | 23.04 ± 4.76 b | 23.40 ± 6.95 b | 29.13 ± 4.15 a | 2.920 | 0.037 | 0.073 |
| WHR | 0.83 ± 0.05 c | 0.85 ± 0.06 b | 0.84 ± 0.06 b,c | 0.91 ± 0.07 a | 3.670 | 0.014 | 0.090 |
| Groups | |||||||
|---|---|---|---|---|---|---|---|
| NDG | LDG | MDG | HDG | F | p | η² | |
| Cardiorendurance (reps.) | 47.35 ± 19.95 a | 43.05 ± 17.73 b | 45.57 ± 19.96 a,b | 22.00 ± 10.91 c | 4.694 | 0.004 | 0.112 |
| Flexibility (cm) | 11.49 ± 9.50 | 12.55 ± 9.34 | 9.79 ± 15.11 | 5.30 ± 13.59 | 0.979 | 0.405 | 0.026 |
| Strength (kg) | 29.46 ± 9.73 a | 25.14 ± 6.94 b | 22.86 ± 5.76 b,c | 19.29 ± 4.99 c | 10.696 | 0.001 | 0.223 |
| Power (m) | 193.16 ± 27.64 a | 190.76 ± 35.62 a | 181.14 ± 31.75 b | 158.86 ± 22.84 c | 3.905 | 0.011 | 0.095 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, J.-E.; Eun, D.; Jee, Y.-S. Daily Life Patterns, Psychophysical Conditions, and Immunity of Adolescents in the COVID-19 Era: A Mixed Research with Qualitative Interviews by a Quasi-Experimental Retrospective Study. Healthcare 2022, 10, 1152. https://doi.org/10.3390/healthcare10061152
Yu J-E, Eun D, Jee Y-S. Daily Life Patterns, Psychophysical Conditions, and Immunity of Adolescents in the COVID-19 Era: A Mixed Research with Qualitative Interviews by a Quasi-Experimental Retrospective Study. Healthcare. 2022; 10(6):1152. https://doi.org/10.3390/healthcare10061152
Chicago/Turabian StyleYu, Ji-Eun, Denny Eun, and Yong-Seok Jee. 2022. "Daily Life Patterns, Psychophysical Conditions, and Immunity of Adolescents in the COVID-19 Era: A Mixed Research with Qualitative Interviews by a Quasi-Experimental Retrospective Study" Healthcare 10, no. 6: 1152. https://doi.org/10.3390/healthcare10061152