
The Role of Adolescents’ Personal and Social Resources in Achieving Desired Emotional and Behavioral Outcomes during an Anxiety-Provoking Pandemic Outbreak


Abstract
:1. Introduction
1.1. Why the COVID-19 Outbreak May Be Particularly Challenging for Adolescents
1.1.1. Pandemic-Related Anxiety
1.1.2. Handwashing
1.2. Adolescents’ Positive Resources during the COVID-19 Outbreak
1.2.1. Positivity Ratio
1.2.2. Self-Control
1.2.3. Hope
1.2.4. Peer Social Support
2. Method
2.1. Sample and Procedure
2.2. Measures
2.2.1. Self-Control Skills
2.2.2. Positivity Ratio
2.2.3. Perception of Handwashing (before and during the Outbreak)
2.2.4. Hope
2.2.5. Pandemic-Related Anxiety
2.2.6. Peer Social Support
2.3. Data Analysis
3. Results
3.1. Preliminary Analyses
3.2. Path Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andrews, J.L.; Foulkes, L.; Blakemore, S.-J. Peer influence in adolescence: Public-health implications for COVID-19. Trends Cogn. Sci. 2020, 24, 585–587. [Google Scholar] [CrossRef]
- Ayalon, L.; Chasteen, A.; Diehl, M.; Levy, B.; Neupert, S.D.; Rothermund, K.; Tesch-Römer, C.; Wahl, H.-W. Aging in times of the COVID-19 pandemic: Avoiding ageism and fostering intergenerational solidarity. J. Gerontol. Ser. B 2020, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Best, J.R.; Miller, P.H. A developmental perspective on executive function. Child Dev. 2010, 81, 1641–1660. [Google Scholar] [CrossRef] [Green Version]
- Blakemore, S.-J. Avoiding social risk in adolescence. Curr. Dir. Psychol. Sci. 2018, 27, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Bradburn, N.M. The Structure of Psychological Well-Being; Aldine: Chicago, IL, USA, 1969. [Google Scholar]
- Bukchin, S.; Kerret, D. Once you choose hope: Early adoption of green technology. Environ. Sci. Pollut. Res. 2019, 27, 3271–3280. [Google Scholar] [CrossRef]
- Bukchin, S.; Ronen, T. Linking positive components, anxiety and handwashing habits during the Coronavirus outbreak. 2021; Manuscript Submitted for Publication. [Google Scholar]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef] [PubMed]
- Choukas-Bradley, S.; Giletta, M.; Cohen, G.L.; Prinstein, M.J. Peer influence, peer status, and prosocial behavior: An experimental investigation of peer socialization of adolescents’ intentions to volunteer. J. Youth Adolesc. 2015, 44, 2197–2210. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.S.; Saucier, D.A.; Hafner, E. Meta-analysis of the relationships between social support and well-being in children and adolescents. J. Soc. Clin. Psychol. 2010, 29, 624–645. [Google Scholar] [CrossRef]
- Cirrincione, L.; Plescia, F.; Ledda, C.; Rapisarda, V.; Martorana, D.; Moldovan, R.E.; Theodoridou, K.; Cannizzaro, E. COVID-19 pandemic: Prevention and protection measures to be adopted at the workplace. Sustainability 2020, 12, 3603. [Google Scholar] [CrossRef]
- Cohn, M.A.; Fredrickson, B.L. Positive Emotions. In Oxford Library of Psychology. Oxford Handbook of Positive Psychology; Lopez, S.J., Snyder, C.R., Eds.; Oxford University Press: Oxford, UK, 2009; pp. 13–24. [Google Scholar] [CrossRef]
- Cooley, J.L.; Fite, P.J.; Rubens, S.L.; Tunno, A.M. Peer victimization, depressive symptoms, and rule-breaking behavior in adolescence: The moderating role of peer social support. J. Psychopathol. Behav. Assess. 2015, 37, 512–522. [Google Scholar] [CrossRef]
- Cramer, K.M.; Dyrkacz, L. Differential prediction of maladjustment scores with the Snyder hope subscales. Psychol. Rep. 1998, 83, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Dalton, L.; Rapa, E.; Stein, A. Protecting the psychological health of children through effective communication about COVID-19. Lancet Child Adolesc. Health 2020, 4, 346–347. [Google Scholar] [CrossRef]
- Daugherty, D.A.; Runyan, J.D.; Steenbergh, T.A.; Fratzke, B.J.; Fry, B.N.; Westra, E. Smartphone delivery of a hope intervention: Another way to flourish. PLoS ONE 2018, 13, e0197930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Barros Ahrens, R.; da Silva Lirani, L.; de Francisco, A.C. Construct validity and reliability of the work environment assessment instrument WE-10. Int. J. Environ. Res. Public Health 2020, 17, 7364. [Google Scholar] [CrossRef]
- De Ridder, D.T.; Lensvelt-Mulders, G. Taking stock of self-control: A meta-analysis of how trait self-control relates to a wide range of behaviors. In Self-Regulation and Self-Control; Baumeister, R., Ed.; Routledge: London, UK, 2018; pp. 221–274. [Google Scholar]
- Drach-Zahavy, A.; Somech, A. Coping with health problems: The distinctive relationships of hope sub-scales with constructive thinking and resource allocation. Personal. Individ. Differ. 2002, 33, 103–117. [Google Scholar] [CrossRef]
- Duckworth, A.L. The significance of self-control. Proc. Natl. Acad. Sci. USA 2011, 108, 2639–2640. [Google Scholar] [CrossRef] [Green Version]
- Duckworth, A.L.; Taxer, J.L.; Eskreis-Winkler, L.; Galla, B.M.; Gross, J.J. Self-control and academic achievement. Annu. Rev. Psychol. 2019, 70, 373–399. [Google Scholar] [CrossRef]
- Feldman, D.B.; Dreher, D.E. Can hope be changed in 90 minutes? Testing the efficacy of a single-session goal-pursuit intervention for college students. J. Happiness Stud. 2012, 13, 745–759. [Google Scholar] [CrossRef]
- Folkman, S. The case for positive emotions in the stress process. Anxiety Stress Coping 2008, 21, 3–14. [Google Scholar] [CrossRef]
- Foulkes, L.; Leung, J.T.; Fuhrmann, D.; Knoll, L.J.; Blakemore, S.J. Age differences in the prosocial influence effect. Dev. Sci. 2018, 21, e12666. [Google Scholar] [CrossRef] [Green Version]
- Frankl, V.E. Man’s Search for Meaning; Simon and Schuster: New York, NY, USA, 1985. [Google Scholar]
- Fredrickson, B.L. The broaden-and-build theory of positive emotions. Philos. Trans. R. Soc. B Biol. Sci. 2004, 359, 1367–1377. [Google Scholar] [CrossRef]
- Fredrickson, B.L. Positivity: Discover the Ratio That Tips Your Life toward Flourishing; Crown: New York, NY, USA, 2009. [Google Scholar]
- Fredrickson, B.L. Positive emotions broaden and build. In Advances in Experimental Social Psychology; Berkowitz, L., Ed.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 47, pp. 1–53. [Google Scholar]
- Fredrickson, B.L. Updated thinking on positivity ratios. Am. Psychol. 2013, 68, 814–822. [Google Scholar] [CrossRef]
- Fredrickson, B.L.; Tugade, M.M.; Waugh, C.E.; Larkin, G.R. What good are positive emotions in crisis? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J. Personal. Soc. Psychol. 2003, 4, 365. [Google Scholar] [CrossRef]
- Friedman, H.L.; Brown, N.J. Implications of debunking the “critical positivity ratio” for humanistic psychology: Introduction to special issue. J. Humanist. Psychol. 2018, 58, 239–261. [Google Scholar] [CrossRef] [Green Version]
- Garbarino, J. Foreword: Pathways from childhood trauma to adolescent violence and delinquency. J. Aggress. Maltreatment Trauma 2002, 6, xxv–xxxi. [Google Scholar]
- Gardner, M.; Steinberg, L. Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: An experimental study. Dev. Psychol. 2005, 41, 625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geraghty, A.W.; Wood, A.M.; Hyland, M.E. Dissociating the facets of hope: Agency and pathways predict dropout from unguided self-help therapy in opposite directions. J. Res. Personal. 2010, 44, 155–158. [Google Scholar] [CrossRef]
- Głąbska, D.; Skolmowska, D.; Guzek, D. Population-based study of the influence of the COVID-19 pandemic on hand hygiene behaviors—Polish Adolescents’ COVID-19 Experience (PLACE-19) Study. Sustainability 2020, 12, 4930. [Google Scholar] [CrossRef]
- Golberstein, E.; Wen, H.; Miller, B.F. Coronavirus disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatrics 2020, 174, 819–820. [Google Scholar] [CrossRef] [Green Version]
- Gomes, A.C.; Rebelo, M.A.B.; de Queiroz, A.C.; de Queiroz Herkrath, A.P.C.; Herkrath, F.J.; Vieira, J.M.R.; Pereira, J.V.; Vettore, M.V. Socioeconomic status, social support, oral health beliefs, psychosocial factors, health behaviours and health-related quality of life in adolescents. Qual. Life Res. 2020, 29, 141–151. [Google Scholar] [CrossRef]
- Gómez-Salgado, J.; Andrés-Villas, M.; Domínguez-Salas, S.; Díaz-Milanés, D.; Ruiz-Frutos, C. Related Health Factors of Psychological Distress During the COVID-19 Pandemic in Spain. Int. J. Environ. Res. Public Health 2020, 17, 3947. [Google Scholar] [CrossRef]
- Gottman, J.M. Principia Amoris: The New Science of Love; Routledge: London, UK, 2014. [Google Scholar]
- Greenberg, J.; Arndt, J. Terror management theory. Handb. Theor. Soc. Psychol. 2011, 1, 398–415. [Google Scholar]
- Groopman, J.E. The Anatomy of Hope: How You Can Find Strength in the Face of Illness; Pocket: San Francisco, CA, USA, 2004. [Google Scholar]
- Hamama, L.; Ronen, T.; Rahav, G. Self-control, self-efficacy, role overload, and stress responses among siblings of children with cancer. Health Soc. Work 2008, 33, 121–132. [Google Scholar] [CrossRef]
- Helsen, M.; Vollebergh, W.; Meeus, W. Social support from parents and friends and emotional problems in adolescence. J. Youth Adolesc. 2000, 29, 319–335. [Google Scholar] [CrossRef]
- Henneberger, A.K.; Mushonga, D.R.; Preston, A.M. Peer influence and adolescent substance use: A systematic review of dynamic social network research. Adolesc. Res. Rev. 2020, 6, 57–73. [Google Scholar] [CrossRef]
- Honken, N.; Ralston, P.A.; Tretter, T.R. Self-control and academic performance in engineering. Am. J. Eng. Educ. 2016, 7, 47–58. [Google Scholar] [CrossRef] [Green Version]
- Johnson, K.J.; Waugh, C.E.; Fredrickson, B.L. Smile to see the forest: Facially expressed positive emotions broaden cognition. Cogn. Emot. 2010, 24, 299–321. [Google Scholar] [CrossRef] [PubMed]
- Kerr, D.C.; Preuss, L.J.; King, C.A. Suicidal adolescents’ social support from family and peers: Gender-specific associations with psychopathology. J. Abnorm. Child Psychol. 2006, 34, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerret, D.; Orkibi, H.; Bukchin, S.; Ronen, T. Two for one: Achieving both pro-environmental behavior and subjective well-being by implementing environmental-hope-enhancing programs in schools. J. Environ. Educ. 2020, 51, 434–448. [Google Scholar] [CrossRef]
- Kerret, D.; Orkibi, H.; Ronen, T. Testing a model linking environmental hope and self-control with students’ positive emotions and environmental behavior. J. Environ. Educ. 2016, 47, 307–317. [Google Scholar] [CrossRef]
- Keyes, C.L. Mental health in adolescence: Is America’s youth flourishing? Am. J. Orthopsychiatry 2006, 76, 395–402. [Google Scholar] [CrossRef]
- Keyes, C.L. Mental Well-Being: International Contributions to the Study of Positive Mental Health; Springer Science & Business Media: Berlin, Germany, 2012. [Google Scholar]
- Kleres, J.; Wettergren, Å. Fear, hope, anger, and guilt in climate activism. Soc. Mov. Stud. 2017, 16, 507–519. [Google Scholar] [CrossRef]
- Klingman, A.; Sagi, A.; Raviv, A. The effect of war on Israeli children. In The Psychological Effects of War and Violence on Children; Leavitt, L.A., Fox, N.A., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1993; pp. 75–92. [Google Scholar]
- Kormos, C.; Gifford, R. The validity of self-report measures of proenvironmental behavior: A meta-analytic review. J. Environ. Psychol. 2014, 40, 359–371. [Google Scholar] [CrossRef]
- Kylmä, J.; Juvakka, T. Hope in parents of adolescents with cancer—: Factors endangering and engendering parental hope. Eur. J. Oncol. Nurs. 2007, 11, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Levendosky, A.A.; Leahy, K.L.; Bogat, G.A.; Davidson, W.S.; von Eye, A. Domestic violence, maternal parenting, maternal mental health, and infant externalizing behavior. J. Fam. Psychol. 2006, 20, 544. [Google Scholar] [CrossRef]
- Lorimer, K.; Knight, R.; Shoveller, J. Improving the health and social wellbeing of young people: Exploring the potential of and for collective agency. Crit. Public Health 2020, 1–8. [Google Scholar] [CrossRef]
- McGeer, V. The art of good hope. Ann. Am. Acad. Political Soc. Sci. 2004, 592, 100–127. [Google Scholar] [CrossRef]
- Muraven, M.; Baumeister, R.F.; Tice, D.M. Longitudinal improvement of self-regulation through practice: Building self-control strength through repeated exercise. J. Soc. Psychol. 1999, 139, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Neimiec, R.M. Character Strengths Interventions: A Field Guide for Practitioners; Hogrefe: Göttingen, Germany, 2017. [Google Scholar]
- Ong, A.D.; Van Dulmen, M.H. Oxford Handbook of Methods in Positive Psychology; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Orkibi, H.; Hamama, L.; Gavriel-Fried, B.; Ronen, T. Pathways to adolescents’ flourishing: Linking self-control skills and positivity ratio through social support. Youth Soc. 2018, 50, 3–25. [Google Scholar] [CrossRef]
- Orkibi, H.; Ronen, T. High self-control protects the link between social support and positivity ratio for Israeli students exposed to contextual risk. J. Sch. Psychol. 2015, 53, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Orkibi, H.; Ronen, T.; Assoulin, N. The subjective well-being of Israeli adolescents attending specialized school classes. J. Educ. Psychol. 2014, 106, 515. [Google Scholar] [CrossRef]
- Peterson, C.; Seligman, M.E. Character Strengths and Virtues: A Handbook and Classification; Oxford University Press: Oxford, UK, 2004; Volume 1. [Google Scholar]
- Preacher, K.; Hayes, A. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [Green Version]
- Pressley, M. Increasing children’s self-control through cognitive interventions. Rev. Educ. Res. 1979, 49, 319–370. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Redlich-Amirav, D.; Ansell, L.J.; Harrison, M.; Norrena, K.L.; Armijo-Olivo, S. Psychometric properties of Hope Scales: A systematic review. Int. J. Clin. Pract. 2018, 72, e13213. [Google Scholar] [CrossRef]
- Ronen, T.; Rahav, G.; Appel, N. Adolescent stress responses to a single acute stress and to continuous external stress: Terrorist attacks. J. Loss Trauma 2003, 8, 261–282. [Google Scholar] [CrossRef]
- Ronen, T.; Rahav, G.; Rosenbaum, M. Children’s reactions to a war situation as a function of age and sex. Anxiety Stress Coping 2003, 16, 59–69. [Google Scholar] [CrossRef]
- Ronen, T.; Rosenbaum, M. Developing learned resourcefulness in adolescents to help them reduce their aggressive behavior: Preliminary findings. Res. Soc. Work Pract. 2010, 20, 410–426. [Google Scholar] [CrossRef]
- Ronen, T.; Seeman, A. Subjective well being of adolescents in boarding schools under threat of war. J. Trauma. Stress 2007, 20, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, M. A schedule for assessing self-control behaviors: Preliminary findings. Behav. Ther. 1980, 11, 109–121. [Google Scholar] [CrossRef]
- Rosenbaum, M. The Role of Learned Resourcefulness in the Self-Control of Health Behavior; Springer Publishing Co.: New York, NY, USA, 1990. [Google Scholar]
- Rosenbaum, M. The three functions of self-control behaviour: Redressive, reformative and experiential. Work Stress 1993, 7, 33–46. [Google Scholar] [CrossRef]
- Rosenbaum, M. Chapter three the self-regulation of experience: Openness and construction. Coping Health Organ. 2000, 53, 51–67. [Google Scholar]
- Rosenbaum, M.; Ronen, T. Self-Control and Education for Self-Control: Development of Rating Scale. In Proceedings of the 25th anniversary meeting of the Association for Advancement of Behavior Therapy, New York, NY, USA, November 1991. [Google Scholar]
- Rosenbaum, M.; Ronen, T. Emotional well-being and self-control skills of children and adolescents: The Israeli perspective. In Mental Well-Being; Keyes, C., Ed.; Springer: Berlin, Germany, 2013; pp. 209–229. [Google Scholar] [CrossRef]
- Rosenbaum, M.; Ronen, T.; Abuelaish, I.; Orkibi, H.; Hamama, L. Positivity ratio links self-control skills to physical aggression and happiness in young Palestinians living in Gaza. Young 2018, 26 (Suppl. 4), 78S–95S. [Google Scholar] [CrossRef]
- RTI International. Tanzania Life Skills Assessment. 2018. Available online: https://www.unicef.org/tanzania/sites/unicef.org.tanzania/files/2019-07/Life%20Skills%20Assessment%20Report_final_2018_06_08.pdf (accessed on 10 April 2020).
- Rubens, S.L.; Vernberg, E.M.; Felix, E.D.; Canino, G. Peer deviance, social support, and symptoms of internalizing disorders among youth exposed to Hurricane Georges. Psychiatry Interpers. Biol. Process. 2013, 76, 169–181. [Google Scholar] [CrossRef] [Green Version]
- Russell, J.A.; Weiss, A.; Mendelsohn, G.A. Affect grid: A single-item scale of pleasure and arousal. J. Personal. Soc. Psychol. 1989, 57, 493. [Google Scholar] [CrossRef]
- Sarason, B.R.; Pierce, G.R.; Sarason, I.G. Social support: The sense of acceptance and the role of relationships. In Wiley Series on Personality Processes. Social Support: An Interactional View; Sarason, B., Sarason, I., Pierce, G., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 1990; pp. 97–128. [Google Scholar]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Sayeed, A.; Kundu, S.; Al Banna, H.; Hasan, M.T.; Begum, M.R.; Khan, S.I. Mental Health Outcomes during the COVID-19 and Perceptions towards the Pandemic: Findings from a Cross sectional Study among Bangladeshi Students. Child. Youth Serv. Rev. 2020, 119, 105658. [Google Scholar] [CrossRef] [PubMed]
- Schrank, B.; Stanghellini, G.; Slade, M. Hope in psychiatry: A review of the literature. Acta Psychiatr. Scand. 2008, 118, 421–433. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, J.B.; Nora, A.; Stage, F.K.; Barlow, E.A.; King, J. Reporting structural equation modeling and confirmatory factor analysis results: A review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Snyder, C.R. Hope theory: Rainbows in the mind. Psychol. Inq. 2002, 13, 249–275. [Google Scholar] [CrossRef]
- Snyder, C.R.; Harris, C.; Anderson, J.R.; Holleran, S.A.; Irving, L.M.; Sigmon, S.T.; Yoshinobu, L.; Gibb, J.; Langelle, C.; Harney, P. The will and the ways: Development and validation of an individual-differences measure of hope. J. Personal. Soc. Psychol. 1991, 60, 570. [Google Scholar] [CrossRef]
- Snyder, C.R.; Lopez, S.J.; Shorey, H.S.; Rand, K.L.; Feldman, D.B. Hope theory, measurements, and applications to school psychology. Sch. Psychol. Q. 2003, 18, 122. [Google Scholar] [CrossRef] [Green Version]
- Snyder, C.R.; Shorey, H.S.; Cheavens, J.; Pulvers, K.M.; Adams III, V.H.; Wiklund, C. Hope and academic success in college. J. Educ. Psychol. 2002, 94, 820–826. [Google Scholar] [CrossRef]
- Snyder, C.R.; Sympson, S.C.; Ybasco, F.C.; Borders, T.F.; Babyak, M.A.; Higgins, R.L. Development and validation of the State Hope Scale. J. Personal. Soc. Psychol. 1996, 70, 321–335. [Google Scholar] [CrossRef]
- Snyder, C.R.E. Handbook of Hope: Theory, Measures, and Applications; Academic Press: Cambridge, MA, USA, 2000. [Google Scholar]
- State of Israel Ministry of Health. News-Ministry of Health. 2020. Available online: https://www.gov.il/en/departments/news/?OfficeId=104cb0f4-d65a-4692-b590-94af928c19c0&skip=0&limit=10 (accessed on 4 April 2020).
- Steinberg, L. A social neuroscience perspective on adolescent risk-taking. Dev. Rev. 2008, 28, 78–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumerlin, J.R. Self-actualization and hope. J. Soc. Behav. Personal. 1997, 12, 1101. [Google Scholar]
- Tangney, J.P.; Boone, A.L.; Baumeister, R.F. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. In Self-Regulation and Self-Control: Selected Works of Roy F. Baumeister; Baumeister, R.F., Ed.; Routledge: London, UK, 2018; pp. 181–220. [Google Scholar]
- Thoits, P.A. Mechanisms linking social ties and support to physical and mental health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valle, M.F.; Huebner, E.S.; Suldo, S.M. An analysis of hope as a psychological strength. J. Sch. Psychol. 2006, 44, 393–406. [Google Scholar] [CrossRef]
- van Hoorn, J.; van Dijk, E.; Meuwese, R.; Rieffe, C.; Crone, E.A. Peer influence on prosocial behavior in adolescence. J. Res. Adolesc. 2016, 26, 90–100. [Google Scholar] [CrossRef]
- Vilaythong, A.P.; Arnau, R.C.; Rosen, D.H.; Mascaro, N. Humor and hope: Can humor increase hope? Humor: Int. J. Humor Res. 2003, 16, 79–90. [Google Scholar] [CrossRef]
- Vohs, K.D.; Baumeister, R.F. Handbook of Self-Regulation: Research, Theory, and Applications; Guilford Publications: New York, NY, USA, 2011. [Google Scholar]
- Vohs, K.D.; Schmeichel, B.J. What makes hope hopeful? The relationship between hope and self-regulation. Psychol. Inq. 2002, 13, 318–321. [Google Scholar]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Waslekar, R.S. The World Hope Index. J. Young Investig. 2018, 34, 56–62. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063. [Google Scholar] [CrossRef]
- World Health Organization [WHO]. Coronavirus. 2020. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 1 April 2020).
- Yeager, D.S.; Dahl, R.E.; Dweck, C.S. Why interventions to influence adolescent behavior often fail but could succeed. Perspect. Psychol. Sci. 2018, 13, 101–122. [Google Scholar] [CrossRef] [PubMed]
- Zambon, A.; Morgan, A.; Vereecken, C.; Colombini, S.; Boyce, W.; Mazur, J.; Lemma, P.; Cavallo, F. The contribution of club participation to adolescent health: Evidence from six countries. J. Epidemiol. Community Health 2010, 64, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, H.; Zeng, H.; Zhang, S.; Du, Q.; Jiang, T.; Du, B. The differential psychological distress of populations affected by the COVID-19 pandemic. Brain Behav. Immun. 2020, 87, 49–50. [Google Scholar] [CrossRef]
- Zhou, M.; Kam, C.C.S. Hope and general self-efficacy: Two measures of the same construct? J. Psychol. 2016, 150, 543–559. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Self-Control | Hope | Positivity Ratio | Pandemic-Related Anxiety | Social Support | Handwashing | ||
|---|---|---|---|---|---|---|---|
| Before the Pandemic | During the Pandemic | ||||||
| Range | −30–+70 | 10–64 | 0.36–3.80 | 8–53 | 12–72 | 0–12 | 0–13 |
| M | 14.19 | 45.79 | 1.49 | 25.39 | 49.88 | 4.77 | 6.72 |
| SD | 18.32 | 9.88 | 0.61 | 8.80 | 12.54 | 2.62 | 2.63 |
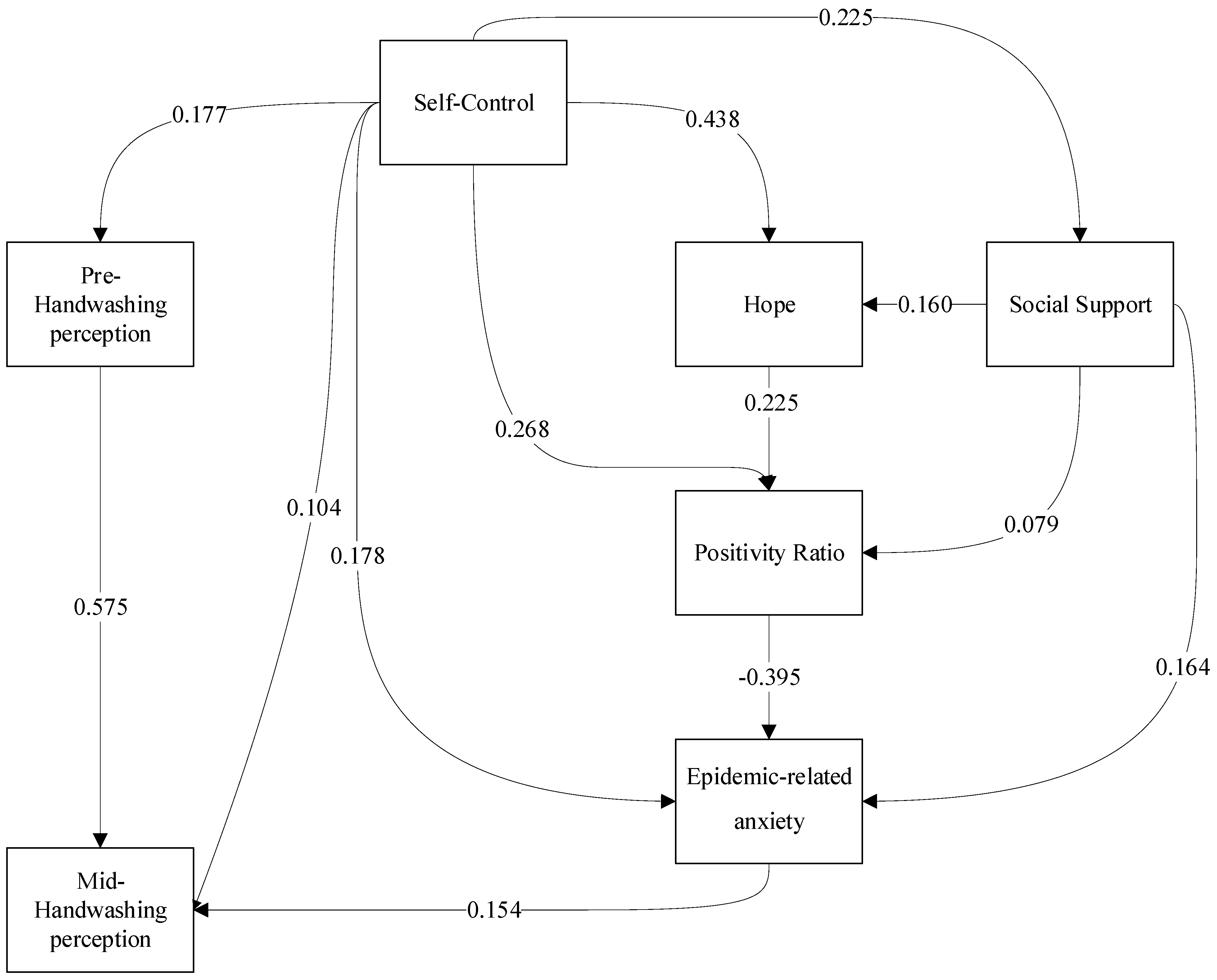
| Paths | Estimate | StandardError | CriticalRatio | p | ||
|---|---|---|---|---|---|---|
| Self-control | 🡢 | Social support | 0.225 | 0.038 | 5.876 | <0.001 |
| Self-control | 🡢 | Hope | 0.438 | 0.035 | 12.541 | <0.001 |
| Self-control | 🡢 | Mid-pandemic handwashing | 0.104 | 0.031 | 3.356 | <0.001 |
| Self-control | 🡢 | Pandemic-related anxiety | 0.178 | 0.040 | 4.462 | <0.001 |
| Self-control | 🡢 | Pre-pandemic handwashing | 0.177 | 0.039 | 4.589 | <0.001 |
| Self-control | 🡢 | Positivity ratio | 0.268 | 0.040 | 6.695 | <0.001 |
| Hope | 🡢 | Positivity ratio | 0.225 | 0.040 | 5.576 | <0.001 |
| Social support | 🡢 | Positivity ratio | 0.079 | 0.036 | 2.166 | 0.030 |
| Social support | 🡢 | Hope | 0.160 | 0.035 | 4.589 | <0.001 |
| Social support | 🡢 | Pandemic-related anxiety | 0.164 | 0.037 | 4.390 | <0.001 |
| Positivity ratio | 🡢 | Pandemic-related anxiety | −0.395 | 0.040 | −9.964 | <0.001 |
| Pandemic-related anxiety | 🡢 | Mid-pandemic handwashing | 0.154 | 0.030 | 5.056 | <0.001 |
| Pre-pandemic handwashing | 🡢 | Mid-pandemic handwashing | 0.575 | 0.031 | 18.601 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bukchin-Peles, S.; Ronen, T. The Role of Adolescents’ Personal and Social Resources in Achieving Desired Emotional and Behavioral Outcomes during an Anxiety-Provoking Pandemic Outbreak. Int. J. Environ. Res. Public Health 2021, 18, 6280. https://doi.org/10.3390/ijerph18126280
Bukchin-Peles S, Ronen T. The Role of Adolescents’ Personal and Social Resources in Achieving Desired Emotional and Behavioral Outcomes during an Anxiety-Provoking Pandemic Outbreak. International Journal of Environmental Research and Public Health. 2021; 18(12):6280. https://doi.org/10.3390/ijerph18126280
Chicago/Turabian StyleBukchin-Peles, Shira, and Tammie Ronen. 2021. "The Role of Adolescents’ Personal and Social Resources in Achieving Desired Emotional and Behavioral Outcomes during an Anxiety-Provoking Pandemic Outbreak" International Journal of Environmental Research and Public Health 18, no. 12: 6280. https://doi.org/10.3390/ijerph18126280