
Emotions, Stress and Coping among Healthcare Workers in a Reproductive Medicine Unit during the First and Second COVID-19 Lockdowns

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. The Questionnaire
- -
- Section 1: socio-demographic information and changes in work conditions;
- -
- Section 2: direct/indirect contact with COVID-19 (three items): this section aimed to collect information on infection and severe complications (or death) due to the virus, experienced personally or in one’s acquaintances;
- -
- Section 3: emotional reactions to the pandemic (nine items): the section explored the intensity experienced as a state of a range of positive and negative emotions (e.g., fear, sadness, anxiety, anger) experienced as a state (not as an emotional trait); the answers were rated on a seven-point Likert scale (1 = not at all, 7 = very much);
- -
- Section 4: stress symptoms (14 items): this section evaluated the occurrence of the main common signs of stress during the past two weeks (e.g., hypervigilance, avoidance, flashbacks, detachment); the answers were rated on a four-point Likert scale (1 = not at all to 4 = nearly every day);
- -
- Section 5: coping strategies (10 items): the section aimed at evaluating the tendency to use specific ways of coping (e.g., avoid conflicts, rely on others), rating the answers on a four-point Likert scale (1 = strongly disagree, 4 = strongly agree).
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics: Socio-Demographic and COVID-Related Information
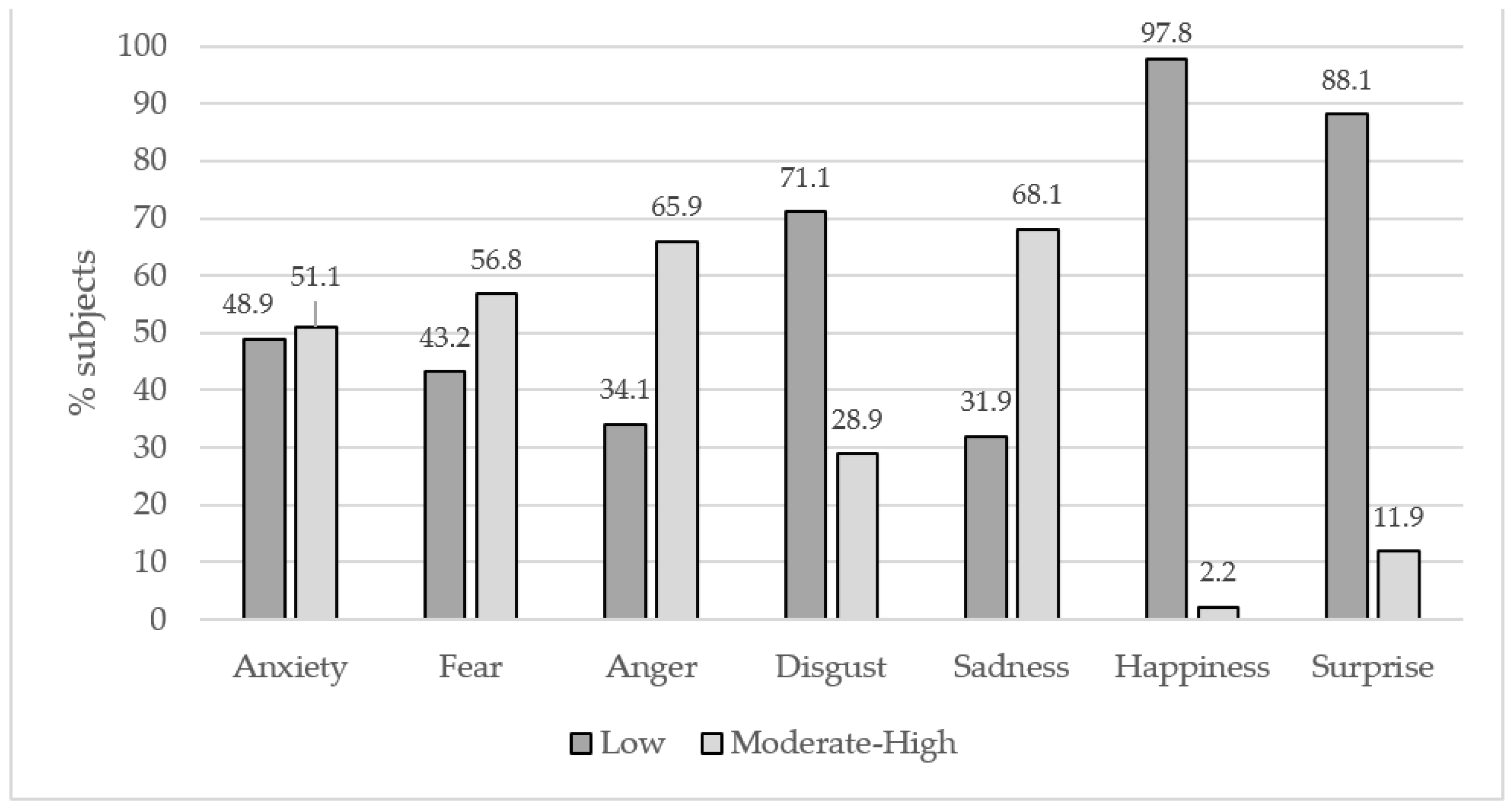
3.2. Emotional Reactions to the Pandemic
3.2.1. Stress Symptoms
3.2.2. Ways of Coping
3.3. Influence of Emotional States on Stress Symptoms
3.4. Influence of Emotional States on Ways of Coping
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marvaldi, M.; Mallet, J.; Dubertret, C.; Moro, M.R.; Guessoum, S.B. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 126, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Epifanio, M.S.; Andrei, F.; Mancini, G.; Agostini, F.; Piombo, M.A.; Spicuzza, V.; Riolo, M.; Lavanco, G.; Trombini, E.; La Grutta, S. The Impact of COVID-19 Pandemic and Lockdown Measures on Quality of Life among Italian General Population. J. Clin. Med. 2021, 10, 289. [Google Scholar] [CrossRef] [PubMed]
- Andrei, F.; Mancini, G.; Agostini, F.; Epifanio, M.S.; Piombo, M.A.; Riolo, M.; Spicuzza, V.; Neri, E.; Baido, R.L.; La Grutta, S.; et al. Quality of Life and Job Loss during the COVID-19 Pandemic: Mediation by Hopelessness and Moderation by Trait Emotional Intelligence. Int. J. Environ. Res. Public Health 2022, 19, 2756. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Carmassi, C.; Dell’Oste, V.; Bui, E.; Foghi, C.; Bertelloni, C.A.; Atti, A.R.; Buselli, R.; Di Paolo, M.; Goracci, A.; Malacarne, P.; et al. The interplay between acute post-traumatic stress, depressive and anxiety symptoms on healthcare workers functioning during the COVID-19 emergency: A multicenter study comparing regions with increasing pandemic incidence. J. Affect. Disord. 2022, 298, 209–216. [Google Scholar] [CrossRef]
- Neto, R.M.D.S.; Benjamim, C.J.R.; Carvalho, P.M.D.M.; Neto, M.L.R. Psychological effects caused by the COVID-19 pandemic in health professionals: A systematic review with meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 104, 110062. [Google Scholar] [CrossRef]
- Naldi, A.; Vallelonga, F.; Di Liberto, A.; Cavallo, R.; Agnesone, M.; Gonella, M.; Sauta, M.D.; Lochner, P.; Tondo, G.; Bragazzi, N.L.; et al. COVID-19 pandemic-related anxiety, distress and burnout: Prevalence and associated factors in healthcare workers of North-West Italy. BJPsych Open 2021, 7, e27. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Simonetti, V.; Durante, A.; Ambrosca, R.; Arcadi, P.; Graziano, G.; Pucciarelli, G.; Simeone, S.; Vellone, E.; Alvaro, R.; Cicolini, G. Anxiety, sleep disorders and self-efficacy among nurses during COVID-19 pandemic: A large cross-sectional study. J. Clin. Nurs. 2021, 30, 1360–1371. [Google Scholar] [CrossRef]
- CDC. Strategies to Mitigate Healthcare Personnel Staffing Shortages. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/mitigating-staff-shortages.html (accessed on 20 January 2022).
- Babore, A.; Lombardi, L.; Viceconti, M.L.; Pignataro, S.; Marino, V.; Crudele, M.; Candelori, C.; Bramanti, S.M.; Trumello, C. Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020, 293, 113366. [Google Scholar] [CrossRef] [PubMed]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Dif-ferences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef] [PubMed]
- Batra, K.; Singh, T.P.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the Psychological Impact of COVID-19 among Healthcare Workers: A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Pérez-García, E.; Ortega-Galán, M. Quality of Life in Nursing Professionals: Burnout, Fatigue, and Compassion Satisfaction. Int. J. Environ. Res. Public Health 2020, 17, 1253. [Google Scholar] [CrossRef] [Green Version]
- Walton, M.; Murray, E.; Christian, M.D. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 241–247. [Google Scholar] [CrossRef]
- Fernandez, R.; Sikhosana, N.; Green, H.; Halcomb, E.J.; Middleton, R.; Alananzeh, I.; Trakis, S.; Moxham, L. Anxiety and depression among healthcare workers during the COVID-19 pandemic: A systematic umbrella review of the global evidence. BMJ Open 2021, 11, e054528. [Google Scholar] [CrossRef]
- Mert, S.; Karatoprak, A.P.; Demirhan, Y.; Baydemir, C.; Çetinarslan, B.; Cantürk, Z.; Selek, A.; Aydin, L.; Sözen, M.; Gezer, E. COVID-19, Anxiety, and Hopelessness: Quality of Life Among Healthcare Workers in Turkey. Eval. Health Prof. 2021, 45, 97–107. [Google Scholar] [CrossRef]
- Mihaylova, T.; Koychev, A.; Stoyanova, S.; Dimitrov, T.; Todorova, D.; Ivantchev, N. Generalized anxiety in healthcare workers during the coronavirus pandemic. Biotechnol. Biotechnol. Equip. 2021, 35, 828–838. [Google Scholar] [CrossRef]
- Di Giuseppe, M.; Nepa, G.; Prout, T.; Albertini, F.; Marcelli, S.; Orrù, G.; Conversano, C. Stress, Burnout, and Resilience among Healthcare Workers during the COVID-19 Emergency: The Role of Defense Mechanisms. Int. J. Environ. Res. Public Health 2021, 18, 5258. [Google Scholar] [CrossRef]
- Canal-Rivero, M.; Armesto-Luque, L.; Rubio-García, A.; Rodriguez-Menéndez, G.; Garrido-Torres, N.; Capitán, L.; Luque, A.; Crespo-Facorro, B.; Ruiz-Veguilla, M. Trauma and stressor-related disorders among health care workers during COVID-19 pandemic and the role of the gender: A prospective longitudinal survey. J. Affect. Disord. 2022, 302, 110–122. [Google Scholar] [CrossRef]
- Gündoğmuş, I.; Ünsal, C.; Bolu, A.; Takmaz, T.; Ökten, S.B.; Aydın, M.B.; Uçar, H.; Gündüz, A.; Kul, A.T. The comparison of anxiety, depression and stress symptoms levels of healthcare workers between the first and second COVID-19 peaks. Psychiatry Res. 2021, 301, 113976. [Google Scholar] [CrossRef] [PubMed]
- Besirli, A.; Celik, S.; Atilgan, M.; Varlihan, A.; Habaci, M.F.; Yenieri, T.; Isler, A.C.; Kizileroglu, S.; Ozturk, G.; Ozer, O.A.; et al. The Relationship Between Anxiety and Depression Levels with Perceived Stress and Coping Strategies in Health Care Workers During The COVID-19 Pandemic. SiSli Etfal Häst. Tip Bulteni Med. Bull. Sisli Hosp. 2021, 55, 1–11. [Google Scholar] [CrossRef]
- Kilic, A.; Gurcan, M.B.; Aktura, B.; Sahin, A.R.; Kokrek, Z. Prevalence of Anxiety and Relationship of Anxiety with Coping Styles and Related Factors in Healthcare Workers During COVID-19 Pandemic. Psychiatr. Danub. 2021, 33, 161–171. [Google Scholar] [PubMed]
- Rus, M.; Matei, R.; Sandu, M.L.; Delcea, C.; Siserman, C. Emotional Distress and Coping Strategies of Health Care Workers During Covid-19 Pandemic. Rom. J. Leg. Med. 2020, 28, 442–450. [Google Scholar] [CrossRef]
- ESHRE. Coronavirus Covid-19: ESHRE Statement on Pregnancy and Conception. 2020. Available online: https://www.eshre.eu/Press-Room/ESHRE-News (accessed on 20 January 2022).
- Li, Y.; Zhao, R.; Zheng, S.; Chen, X.; Wang, J.; Sheng, X.; Zhou, J.; Cai, H.; Fang, Q.; Yu, F.; et al. Lack of Vertical Transmission of Severe Acute Respiratory Syndrome Coronavirus 2, China. Emerg. Infect. Dis. 2020, 26, 1335–1336. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.; Li, W.; Kang, Q.; Xiong, Z.; Wang, S.; Lin, X.; Liu, Y.; Xiao, J.; Liu, H.; Deng, D.; et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: A retrospective, single-centre, descriptive study. Lancet Infect. Dis. 2020, 20, 559–564. [Google Scholar] [CrossRef] [Green Version]
- Klonoff-Cohen, H.; Chu, E.; Natarajan, L.; Sieber, W. A prospective study of stress among women undergoing in vitro ferti-lization or gamete intrafallopian transfer. Fertil. Steril. 2001, 76, 675–687. [Google Scholar] [CrossRef]
- Slade, P.; O’Neill, C.; Simpson, A.J.; Lashen, H. The relationship between perceived stigma, disclosure patterns, support and distress in new attendees at an infertility clinic. Hum. Reprod. 2007, 22, 2309–2317. [Google Scholar] [CrossRef] [Green Version]
- Biviá-Roig, G.; Boldó-Roda, A.; Blasco-Sanz, R.; Serrano-Raya, L.; DelaFuente-Díez, E.; Múzquiz-Barberá, P.; Lisón, J.F. Impact of the COVID-19 Pandemic on the Lifestyles and Quality of Life of Women With Fertility Problems: A Cross-Sectional Study. Front. Public Health 2021, 9, 686115. [Google Scholar] [CrossRef]
- Boivin, J.; Harrison, C.; Mathur, R.; Burns, G.; Pericleous-Smith, A.; Gameiro, S. Patient experiences of fertility clinic closure during the COVID-19 pandemic: Appraisals, coping and emotions. Hum. Reprod. 2020, 35, 2556–2566. [Google Scholar] [CrossRef]
- Lablanche, O.; Salle, B.; Perie, M.-A.; Labrune, E.; Langlois-Jacques, C.; Fraison, E. Psychological effect of COVID-19 pandemic among women undergoing infertility care, a French cohort—PsyCovART Psychological effect of COVID-19: PsyCovART. J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102251. [Google Scholar] [CrossRef] [PubMed]
- Haham, L.M.; Youngster, M.; Shani, A.K.; Yee, S.; Ben-Kimhy, R.; Medina-Artom, T.R.; Hourvitz, A.; Kedem, A.; Librach, C. Suspension of fertility treatment during the COVID-19 pandemic: Views, emotional reactions and psychological distress among women undergoing fertility treatment. Reprod. Biomed. Online 2021, 42, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Streiner, D.L.; Norman, G.R. Correction for multiple testing: Is there a resolution? Chest 2011, 140, 16–18. [Google Scholar] [CrossRef] [PubMed]
- García-Fernández, L.; Romero-Ferreiro, V.; Padilla, S.; Lahera, G.; Rodriguez-Jimenez, R. Different emotional profile of health care staff and general population during the COVID-19 outbreak. Psychol. Trauma Theory Res. Pract. Policy 2022, 14, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Sima, R.-M.; Olaru, O.-G.; Cazaceanu, A.; Scheau, C.; Dimitriu, M.-T.; Popescu, M.; Ples, L. Stress and anxiety among physicians and nurses in Romania during the COVID-19 pandemic. J. Mind Med. Sci. 2021, 8, 252–258. [Google Scholar] [CrossRef]
- Şahin, C.U.; Kulakaç, N. Exploring anxiety levels in healthcare workers during COVID-19 pandemic: Turkey sample. Curr. Psychol. 2021, 41, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Franzoi, I.G.; Granieri, A.; Sauta, M.D.; Agnesone, M.; Gonella, M.; Cavallo, R.; Lochner, P.; Bragazzi, N.L.; Naldi, A. Anxiety, Post-Traumatic Stress, and Burnout in Health Professionals during the COVID-19 Pandemic: Comparing Mental Health Professionals and Other Healthcare Workers. Healthcare 2021, 9, 635. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Sadovyy, M.; Sanchez-Gomez, M.; Breso, E. COVID-19: How the stress generated by the pandemic may affect work perfor-mance through the moderating role of emotional intelligence. Pers. Individ. Dif. 2021, 180, 110986. [Google Scholar] [CrossRef]
- Lou, N.M.; Montreuil, T.; Feldman, L.S.; Fried, G.M.; Lavoie-Tremblay, M.; Bhanji, F.; Kennedy, H.; Kaneva, P.; Harley, J.M. Nurses’ and Physician’ Distress, Burnout, and Coping Strategies During COVID-19: Stress and Impact on Perceived Perfor-mance and Intentions to Quit. J. Contin. Educ. Health Prof. 2022, 42, e44–e52. [Google Scholar] [CrossRef]
- Guazzini, A.; Pesce, A.; Marotta, L.; Duradoni, M. Through the Second Wave: Analysis of the Psychological and Perceptive Changes in the Italian Population during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1635. [Google Scholar] [CrossRef] [PubMed]
- Subaşi, D.; Sümengen, A.A.; Şimşek, E.; Ocakçı, A.F. Healthcare workers’ anxieties and coping strategies during the COVID-19 pandemic in Turkey. Perspect. Psychiatr. Care 2021, 57, 1820–1828. [Google Scholar] [CrossRef] [PubMed]
- Marcolongo, F.; Ottaviani, M.; Romano, P.; Bonassi, S.; Garramone, A.; Infarinato, F.; Russo, P.; Tamburrano, A.; Tomino, C.; Prinzi, G. The role of resilience and coping among Italian healthcare workers during the COVID-19 pandemic. Med. Lav. 2021, 112, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Feng, X.L.; Wang, X.H.; Van Ijzendoorn, M.H. Coping with COVID-19: Exposure to COVID-19 and Negative Impact on Livelihood Predict Elevated Mental Health Problems in Chinese Adults. Int. J. Environ. Res. Public Health 2020, 17, 3857. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Rachman, S.T. Anxiety; Psychology Press: New York, NY, USA, 2014. [Google Scholar]
- Bolles, R.C.; Fanselow, M.S. A perceptual-defensive-recuperative model of fear and pain. Behav. Brain Sci. 1980, 3, 291–301. [Google Scholar] [CrossRef]
- Carlsson, K.; Andersson, J.; Petrovic, P.; Petersson, K.M.; Öhman, A.; Ingvar, M. Predictability modulates the affective and sensory-discriminative neural processing of pain. NeuroImage 2006, 32, 1804–1814. [Google Scholar] [CrossRef]
- Rhudy, J.L.; Meagher, M.W. Fear and anxiety: Divergent effects on human pain thresholds. Pain 2000, 84, 65–75. [Google Scholar] [CrossRef]
- Bassi, M.; Negri, L.; Delle Fave, A.; Accardi, R. The relationship between post-traumatic stress and positive mental health symptoms among health workers during COVID-19 pandemic in Lombardy, Italy. J. Affect. Disord. 2021, 280, 1–6. [Google Scholar] [CrossRef]
- al Falasi, B.; al Mazrouei, M.; al Ali, M.; al Dhamani, M.; al Ali, A.; al Kindi, M.; Dalkilinc, M.; al Qubaisi, M.; Campos, L.A.; al Tunaiji, H.; et al. Prevalence and Determinants of Immediate and Long-Term PTSD Consequences of Coronavirus-Related (CoV-1 and CoV-2) Pandemics among Healthcare Professionals: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 2182. [Google Scholar] [CrossRef]
- Gjerstad, C.L.; Bøe, H.J.; Falkum, E.; Nordstrand, A.E.; Tønnesen, A.; Reichelt, J.G.; Lystad, J.U. Caring for Coronavirus Healthcare Workers: Lessons Learned from Long-Term Monitoring of Military Peacekeepers. Front. Psychol. 2020, 11, 566199. [Google Scholar] [CrossRef]
- Del Piccolo, L.; Donisi, V.; Raffaelli, R.; Garzon, S.; Perlini, C.; Rimondini, M.; Uccella, S.; Cromi, A.; Ghezzi, F.; Ginami, M.; et al. The Psychological Impact of COVID-19 on Healthcare Providers in Obstetrics: A Cross-Sectional Survey Study. Front. Psychol. 2021, 12, 632999. [Google Scholar] [CrossRef] [PubMed]
- Cansiz, A.; Aydin, M.; Kandeger, A.; Tan, O.; Altinbas, K. Evaluation of the Relationships between State-Trait Anxiety, Coping Strategies and Perceived Social Support among Frontline and Non-Frontline Health Workers during the COVID-19 Pandemic in Turkey. Isr. J. Psychiatry Relat. Sci. 2021, 58, 10–18. [Google Scholar]


{kind=link}
| Total Sample (N = 47) | T1 Group (N = 25) | T2 Group (N = 22) | ||
|---|---|---|---|---|
| Age, mean ± SD (range) | 39.85 ± 6.76 (27–54) | 38.50 ± 7.68 (27–54) | 41.07 ± 5.75 (31–50) | |
| Gender (%) | Female | 93.2 | 95.8 | 90.0 |
| Job (%) | Biologist | 19.1 | 20 | 18.2 |
| Nurse | 34.0 | 36 | 31.8 | |
| Physician | 25.5 | 24 | 27.3 | |
| Healthcare assistant | 12.8 | 12 | 13.6 | |
| Other | 8.6 | 8.0 | 9.1 | |
| Education (%) | High school | 20.5 | 27.3 | 13.6 |
| Master’s degree | 27.3 | 27.3 | 27.3 | |
| Specialization | 45.5 | 40.9 | 50.0 | |
| Other | 6.7 | 4.5 | 9.1 | |
| Civil status (%) | Married/cohabiting | 80.8 | 76.0 | 86.3 |
| Single | 12.8 | 16.0 | 9.2 | |
| Other | 6.4 | 8.0 | 4.5 | |
| Total Sample (N = 47) | T1 Group (N = 25) | T2 Group (N = 22) | |
|---|---|---|---|
| Anxiety | 2.51 ± 0.80 (1–5) | 2.40 ± 0.71 (1–4) | 2.64 ± 0.91 (1–5) |
| Fear | 3.82 ± 1.76 (1–7) | 3.75 ± 1.80 (1–7) | 3.90 ± 1.74 (2–7) |
| Anger | 4.41 ± 2.27 (1–7) | 4.33 ± 2.46 (1–7) | 4.50 ± 2.10 (1–7) |
| Disgust | 2.74 ± 2.21 (1–7) | 2.33 ± 2.06 (1–7) | 3.18 ± 2.32 (1–7) |
| Sadness | 4.23 ± 2.02 (1–7) | 4.48 ± 1.94 (1–7) | 4.77 ± 1.57 (2–7) |
| Happiness | 1.30 ± 0.96 (1–7) | 1.25 ± 0.53 (1–3) | 1.36 ± 1.29 (1–7) |
| Surprise | 2.07 ± 0.53 (1–7) | 1.87 ± 1.33 (1–5) | 2.27 ± 1.72 (1–7) |
| Dimensions | Total Sample (N = 47) | T1 Group (N = 25) | T2 Group (N = 22) |
|---|---|---|---|
| Altered arousal | |||
| Irritability and anger | 2.18 ± 0.76 (1–4) | 2.20 ± 0.56 (1–4) | 2.22 ± 0.81 (1–4) |
| Problems with concentration | 1.67 ± 0.60 (1–4) | 1.67 ± 0.62 (1–4) | 1.67 ± 0.69 (1–4) |
| Hyperreactivity/physical reactions | 1.15 ± 0.56 (1–4) | 1.07 ± 0.26 (1–4) | 1.11 ± 0.47 (1–4) |
| Hypervigilance | 2.80 ± 1.04 (1–4) | 2.60 ± 0.99 (1–4) | 3.44 ± 0.78 (1–4) * |
| Intrusion symptoms | |||
| Intrusive thoughts | 2.19 ± 0.90 (1–4) | 1.93 ± 0.88 (1–4) | 2.33 ± 0.77 (1–4) * |
| Flashbacks | 1.64 ± 0.80 (1–4) | 1.53 ± 0.80 (1–4) | 1.61 ± 0.85 (1–4) |
| Distressing dreams and nightmares | 1.15 ± 0.47 (1–4) | 1.00 ± 0.00 (1–4) | 1.06 ± 0.24 (1–4) |
| Avoidance symptoms | |||
| Avoidance of external triggers | 1.53 ± 0.79 (1–4) | 1.53 ± 0.83 (1–4) | 1.33 ± 0.77 (1–4) * |
| Avoidance of thoughts and memories | 2.51 ± 0.92 (1–4) | 2.47 ± 0.83 (1–4) | 2.72 ± 1.02 (1–4) |
| Alterations in mood and cognition | |||
| Irritability/fearfulness | 1.74 ± 0.74 (1–4) | 1.47 ± 0.52 (1–4) | 2.11 ± 0.83 (1–4) * |
| Detachment/obnubilation | 1.54 ± 0.81 (1–4) | 1.40 ± 0.83 (1–4) | 1.67 ± 0.69 (1–4) * |
| Diminished interest/pleasure | 1.63 ± 0.68 (1–4) | 1.67 ± 0.49 (1–4) | 1.61 ± 0.78 (1–4) |
| Depression and hopelessness | 1.77 ± 0.73 (1–4) | 1.60 ± 063 (1–4) | 1.94 ± 0.87 (1–4) |
| Tiredness/low energy | 2.23 ± 0.84 (1–4) | 2.33 ± 0.62 (1–4) | 2.39 ± 1.09 (1–4) |
| Total Sample (N = 47) | T1 Group (N = 25) | T2 Group (N = 22) | |
|---|---|---|---|
| Emotion-focused coping | |||
| Worry and vent emotions | 2.74 ± 0.92 (1–4) | 3.00–0.69 (1–4) | 2.57–0.98 (1–4) |
| Try to see the positive side of a situation | 3.09 ± 0.93 (1–4) | 3.05–0.90 (1–4) | 3.00–1.00 (1–4) |
| Problem-focused coping | |||
| Ability to solve problems | 3.15 ± 0.66 (1–4) | 3.09–0.43 (1–4) | 3.19–0.81 (1–4) |
| Contribute to improve a situation | 3.20 ± 0.59 (2–4) | 3.00–0.54 (1–4) | 3.43–0.60 (1–4) * |
| Plan the time of the day | 3.30 ± 0.83 (1–4) | 3.27–0.73 (1–4) | 3.29–1.01 (1–4) |
| Avoidance-focused coping | |||
| Avoid conflicts | 3.02 ± 0.79 (1–4) | 2.91–0.75 (1–4) | 3.00–0.83 (1–4) |
| Suffer the situation | 2.20 ± 0.91 (1–4) | 2.27–0.88 (1–4) | 2.14–0.96 (1–4) |
| Support-focused coping | |||
| Rely on others | 2.43 ± 0.85 (1–4) | 2.41–0.66 (1–4) | 2.43–1.03 (1–4) |
| Can get help from others | 3.17 ± 0.70 (1–4) | 3.14–0.64 (1–4) | 3.14–0.79 (1–4) |
| Need of someone’s understanding and support | 2.72 ± 0.94 (1–4) | 2.64–0.90 (1–4) | 2.76–1.00 (1–4) |
| Anxiety | Fear | Anger | Sadness | |||||
|---|---|---|---|---|---|---|---|---|
| Low (n = 23) | Moderate–High (n = 24) | Low (n = 20) | Moderate–High (n = 27) | Low (n = 16) | Moderate–High (n = 31) | Low (n = 15) | Moderate–High (n = 32) | |
| Altered arousal | ||||||||
| Irritability and anger | 2.12 ± 0.49 | 2.29 ± 0.85 | 2.20 ± 0.67 | 2.17 ± 0.71 | 2.00 ± 0.00 | 2.23 ± 0.81 | 2.27 ± 0.64 | 2.17 ± 0.72 |
| Problems with concentration | 1.35 ± 0.49 | 2.00 ± 0.61 * | 1.60 ± 0.74 | 1.67 ± 0.49 | 1.70 ± 0.48 | 1.64 ± 0.66 | 1.64 ± 0.67 | 1.70 ± 0.64 |
| Hyperreactivity/physical reactions | 1.12 ± 0.49 | 1.06 ± 0.24 | 1.07 ± 2.26 | 1.11 ± 0.47 | 1.00 ± 0.00 | 1.14 ± 0.47 | 1.00 ± 0.00 | 1.13 ± 0.46 |
| Hypervigilance | 2.82 ± 1.02 | 3.24 ± 0.90 | 2.80 ± 1.01 | 3.17 ± 0.92 | 3.00 ± 0.94 | 3.00 ± 1.02 | 2.64 ± 0.81 | 3.22 ± 1.00 * |
| Intrusion symptoms | ||||||||
| Intrusive thoughts | 1.76 ± 0.66 | 2.47 ± 0.87 * | 2.07 ± 0.96 | 2.17 ± 0.79 | 1.90 ± 0.74 | 2.23 ± 0.92 | 1.91 ± 0.94 | 2.22 ± 0.80 |
| Flashbacks | 1.53 ± 0.80 | 1.59 ± 0.87 | 1.47 ± 0.83 | 1.67 ± 0.84 | 1.40 ± 0.70 | 1.64 ± 0.90 | 1.18 ± 0.41 | 1.74 ± 0.92 * |
| Distressing dreams and nightmares | 1.00 ± 0.00 | 1.06 ± 0.00 | 1.00 ± 0.00 | 1.06 ± 0.24 | 1.10 ± 0.32 | 1.00 ± 0.00 | 1.00 ± 0.00 | 1.04 ± 0.21 |
| Persistent avoidance | ||||||||
| Avoidance of external triggers | 1.71 ± 0.99 | 1.18 ± 0.39 | 1.60 ± 0.74 | 1.33 ± 0.84 | 1.80 ± 0.79 | 1.32 ± 0.78 * | 2.00 ± 0.78 | 1.17 ± 0.65 * |
| Avoidance of thoughts and memories | 2.65 ± 0.93 | 2.53 ± 0.94 | 2.53 ± 0.99 | 2.67 ± 0.91 | 2.70 ± 0.82 | 2.64 ± 0.95 | 2.45 ± 0.93 | 2.65 ± 0.94 |
| Alterations in mood and cognition | ||||||||
| Irritability/fearfulness | 1.41 ± 0.51 | 2.18 ± 0.81 * | 1.67 ± 0.82 | 1.89 ± 0.76 | 1.80 ± 0.79 | 1.73 ± 0.77 | 1.73 ± 0.79 | 1.83 ± 0.78 |
| Detachment/obnubilation | 1.41 ± 0.62 | 1.65 ± 0.86 | 1.67 ± 0.90 | 1.39 ± 0.61 | 1.40 ± 0.52 | 1.50 ± 0.80 | 1.27 ± 0.47 | 1.65 ± 0.83 |
| Diminished interest/pleasure | 1.41 ± 0.51 | 1.88 ± 0.70 * | 1.67 ± 0.62 | 1.67 ± 0.69 | 1.80 ± 0.79 | 1.64 ± 0.59 | 1.82 ± 0.60 | 1.57 ± 0.66 |
| Depression and hopelessness | 1.41 ± 0.62 | 2.18 ± 0.73 * | 1.87 ± 0.83 | 1.72 ± 0.75 | 1.70 ± 0.82 | 1.82 ± 0.80 | 1.82 ± 0.87 | 1.78 ± 0.74 |
| Tiredness/low energy | 1.91 ± 0.79 | 2.54 ± 0.78 * | 2.21 ± 0.98 | 2.24 ± 0.66 | 2.07 ± 0.70 | 2.21 ± 0.82 | 2.47 ± 0.74 | 2.13 ± 0.87 |
| Anxiety | Fear | Anger | Sadness | |||||
|---|---|---|---|---|---|---|---|---|
| Low (n = 23) | Moderate–High (n = 24) | Low (n = 20) | Moderate–High (n = 27) | Low (n = 16) | Moderate–High (n = 31) | Low (n = 15) | Moderate–High (n = 32) | |
| Emotion-focused coping | ||||||||
| Worry and vent emotions | 2.67 ± 0.80 | 2.91 ± 0.92 | 2.63 ± 0.83 | 2.95 ± 0.79 | 2.79 ± 0.80 | 2.70 ± 0.87 | 2.57 ± 0.85 | 2.90 ± 0.86 |
| Try to see the positive side of a situation | 3.19 ± 0.93 | 2.86 ± 0.94 | 3.21 ± 0.86 | 2.91 ± 0.92 | 3.00 ± 0.87 | 2.96 ± 0.98 | 2.93 ± 0.73 | 3.07 ± 1.03 |
| Problem-focused coping | ||||||||
| Ability to solve problems | 3.10 ± 0.70 | 3.18 ± 0.59 | 3.11 ± 0.57 | 3.23 ± 0.53 | 3.07 ± 0.27 | 3.11 ± 0.75 | 3.00 ± 0.55 | 3.21 ± 0.68 |
| Contribute to improve a situation | 3.14 ± 0.57 | 3.27 ± 0.63 | 3.16 ± 0.50 | 3.27 ± 0.63 | 3.21 ± 0.58 | 3.15 ± 0.60 | 3.14 ± 0.54 | 3.24 ± 0.64 |
| Plan the time of the day | 3.24 ± 0.94 | 3.32 ± 0.78 | 3.26 ± 0.87 | 3.36 ± 0.73 | 3.64 ± 0.50 | 3.04 ± 0.94 | 3.21 ± 0.98 | 3.31 ± 0.81 |
| Avoidance coping | ||||||||
| Avoid conflicts | 2.81 ± 0.87 | 3.09 ± 0.68 | 2.84 ± 0.83 | 3.09 ± 0.61 | 2.71 ± 0.83 | 3.00 ± 0.73 | 2.79 ± 0.80 | 3.03 ± 0.78 |
| Suffer the situation | 1.09 ± 0.83 | 2.50 ± 0.91 * | 2.32 ± 0.88 | 2.09 ± 0.87 | 2.21 ± 0.80 | 2.07 ± 0.87 | 2.14 ± 0.86 | 2.24 ± 0.95 |
| Support-focused coping | ||||||||
| Rely on others | 2.43 ± 0.74 | 2.41 ± 0.96 | 2.37 ± 0.76 | 2.45 ± 0.86 | 2.50 ± 0.76 | 2.26 ± 0.81 | 2.36 ± 0.63 | 2.45 ± 0.95 |
| Can get help from others | 3.24 ± 0.77 | 3.05 ± 0.65 | 3.26 ± 0.65 | 3.09 ± 0.61 | 3.43 ± 0.51 | 2.93 ± 0.73 | 3.07 ± 0.62 | 3.17 ± 0.76 |
| Need of someone’s understanding and support | 2.52 ± 0.93 | 2.86 ± 0.94 | 2.79 ± 0.86 | 2.64 ± 0.95 | 2.79 ± 0.89 | 2.56 ± 0.93 | 2.64 ± 1.01 | 2.72 ± 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paterlini, M.; Neri, E.; Nicoli, A.; Genova, F.; Villani, M.T.; Santi, S.; Agostini, F. Emotions, Stress and Coping among Healthcare Workers in a Reproductive Medicine Unit during the First and Second COVID-19 Lockdowns. Int. J. Environ. Res. Public Health 2022, 19, 5899. https://doi.org/10.3390/ijerph19105899
Paterlini M, Neri E, Nicoli A, Genova F, Villani MT, Santi S, Agostini F. Emotions, Stress and Coping among Healthcare Workers in a Reproductive Medicine Unit during the First and Second COVID-19 Lockdowns. International Journal of Environmental Research and Public Health. 2022; 19(10):5899. https://doi.org/10.3390/ijerph19105899
Chicago/Turabian StylePaterlini, Marcella, Erica Neri, Alessia Nicoli, Federica Genova, Maria Teresa Villani, Sara Santi, and Francesca Agostini. 2022. "Emotions, Stress and Coping among Healthcare Workers in a Reproductive Medicine Unit during the First and Second COVID-19 Lockdowns" International Journal of Environmental Research and Public Health 19, no. 10: 5899. https://doi.org/10.3390/ijerph19105899