
Comparing Humoral and Cellular Adaptive Immunity during Convalescent Phase of COVID-19 in Hemodialysis Patients and Kidney Transplant Recipients

 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- Age > 18 years,
- No clinical signs of COVID-19,
- If formerly tested positive for SARS-CoV-2, a minimum of 14 days must have passed since a positive test,
- Signed informed consent to participate in the study.
- Previous anti-SARS-CoV-2 vaccination,
- Symptoms of any infection or neoplasm at the time of recruitment and during the preceding 2 weeks,
- In the case of kidney transplant recipients—histological signs of allograft rejection at the time of evaluation and in the preceding 4 weeks prior to the study.
- They had tested positive in any former rRT-PCR SARS-CoV-2 test regardless of presentation with COVID-19 symptoms
- And/or they were anti-SARS-CoV-2 seropositive at the time of recruitment.
2.2. Routine Diagnostic Methods
2.3. SARS-CoV-2 rRT-PCR
2.4. SARS-CoV-2 Specific Antibodies
2.5. SARS-CoV-2 Cellular Response
2.6. Immune Cell Phenotypes
- Regulatory T cells—anti-CD25-FITC, anti-FOXP3-PE, anti-CD4-PerCP, and anti-CD3-APC; whole blood staining, lysed with BD FACS Lysing Solution, followed by Human FoxP3 Buffer Set fixation and permeabilization;
- Th and Tc lymphocytes—anti-CD57-FITC, anti-CD28-PE, anti-CD4-PerCP, anti-CD3-APC, anti-CD8-APC-Cy7; whole blood staining, lysed with BD FACS Lysing Solution and washed with BD Pharmingen Stain Buffer (FBS);
- Th1, Th2, and Th17—blood samples stimulated for 5 h with PMA and ionomycin in the presence of GolgiStop BD, followed by staining with Human Th1/Th2/Th17 Phenotyping Kit;
- B cells—anti-IgD-FITC, anti-CD24-PE, anti-CD27-PE-Cy7, anti-CD19-PerCP-Cy5.5, anti-CD38-APC, and anti-CD20-APC-H7); whole blood staining, lysed with BD FACS Lysing Solution and washed with BD Pharmingen Stain Buffer (FBS).
2.7. Statistical Analysis
3. Results
3.1. Anti-SARS-CoV-2 Antibodies in Convalescent Hemodialysis and Transplant Patients
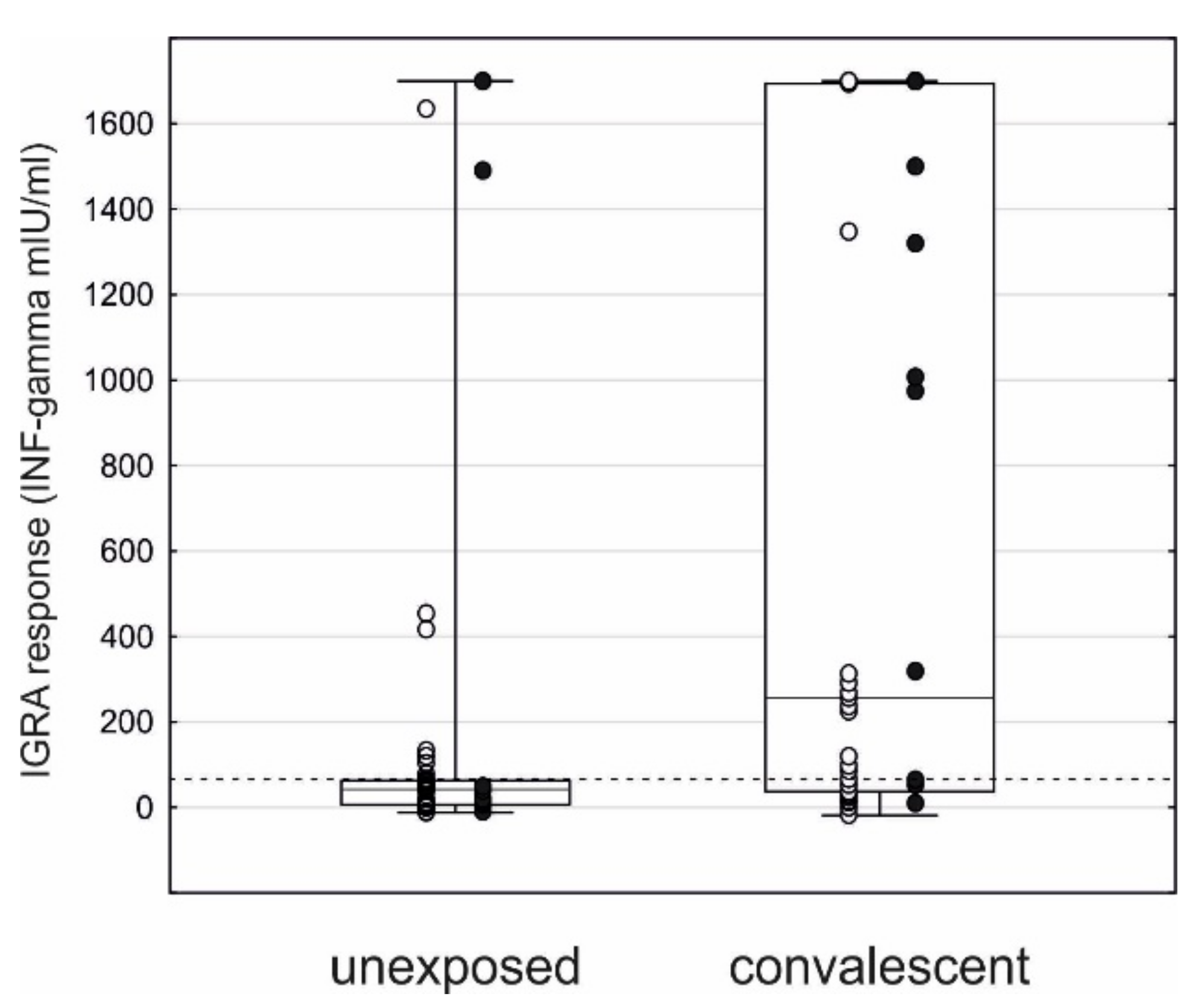
3.2. Anti-SARS-CoV-2 Cellular Response
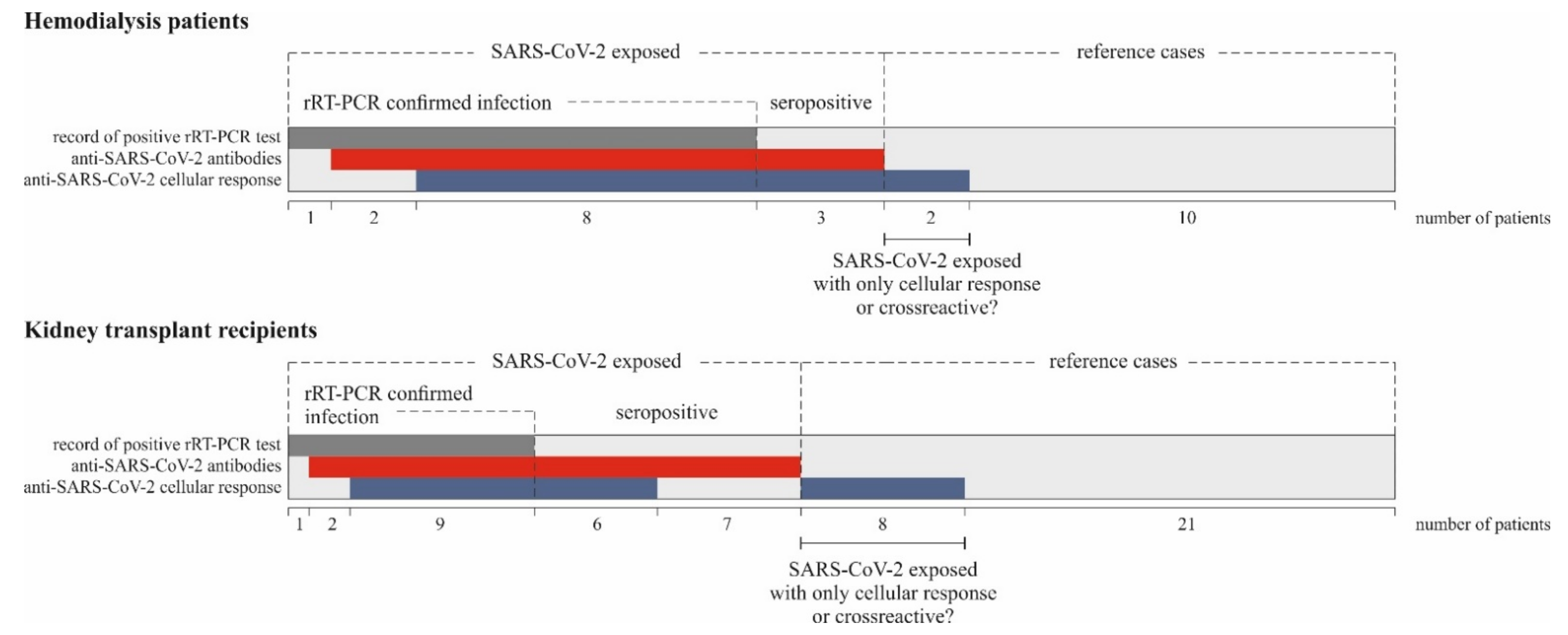
3.3. SARS-CoV-2 Specific Immune Characterization of the Patients
3.4. Analysis of Standard Laboratory Parameters and Inflammatory Markers in Relation to Convalescent SARS-CoV-2 Infection
3.5. Analysis of Lymphocyte Subpopulations
4. Discussion
Limitation of the Study
5. Conclusions
- Hemodialysis patients and kidney transplant recipients can induce both a humoral and cellular response after SARS-CoV-2 infection. The specific anti-SARS-CoV-2 IgG level is not different between the groups of patients, as opposed to SARS-CoV-2-reactive T cell response (IGRA), which is stronger in the hemodialysis patients compared to the transplant population.
- The SARS-CoV-2-specific IgG antibody level decreases with time, while IgA and the specific anti-SARS-CoV-2 cellular response is maintained for a longer time.
- The interferon-gamma release assay is a valuable test for the assessment of T cell-mediated immunity in immunocompromised KTR and HD patients.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 54, 536–544. [Google Scholar]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhong, X.; Wang, Y.; Zeng, X.; Luo, T.; Liu, Q. Clinical determinants of the severity of COVID-19: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0250602. [Google Scholar]
- Wang, B.; Luo, Q.; Zhang, W.; Yu, S.; Cheng, X.; Wang, L.; Chen, X.; Chen, Y. The Involvement of Chronic Kidney Disease and Acute Kidney Injury in Disease Severity and Mortality in Patients with COVID-19: A Meta-Analysis. Kidney Blood Press. Res. 2020, 46, 17–30. [Google Scholar] [PubMed]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef]
- McCafferty, K.; Davari, M.; Price, K.; Rajakariar, R.; Cove-Smith, A.; Forbes, S.H. COVID -19 prevalence and seroconversion in an urban hemodialysis unit in the United Kingdom. Hemodial. Int. 2021, 25, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Favà, A.; Donadeu, L.; Sabé, N.; Pernin, V.; González-Costello, J.; Lladó, L.; Meneghini, M.; Charmetant, X.; García-Romero, E.; Cachero, A.; et al. SARS-CoV-2-specific serological and functional T cell immune responses during acute and early COVID-19 convalescence in solid organ transplant patients. Am. J. Transplant. 2021, ajt.16570. [Google Scholar] [CrossRef]
- Burack, D.; Pereira, M.R.; Tsapepas, D.S.; Harren, P.; Farr, M.A.; Arcasoy, S.; Cohen, D.J.; Mohan, S.; Emond, J.C.; Hod, E.A.; et al. Prevalence and predictors of SARS-CoV-2 antibodies among solid organ transplant recipients with confirmed infection. Am. J. Transplant. 2021, 21, 2254–2261. [Google Scholar] [CrossRef]
- Ishigami, J.; Matsushita, K. Clinical epidemiology of infectious disease among patients with chronic kidney disease. Clin. Exp. Nephrol. 2019, 23, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Santeusanio, A.D.; Menon, M.C.; Liu, C.; Bhansali, A.; Patel, N.; Mahir, F.; Rana, M.; Tedla, F.; Mahamid, A.; Fenig, Y.; et al. Influence of patient characteristics and immunosuppressant management on mortality in kidney transplant recipients hospitalized with coronavirus disease 2019 (COVID-19). Clin. Transplant. 2021, 35, e14221. [Google Scholar]
- Caillard, S.; Chavarot, N.; Francois, H.; Matignon, M.; Greze, C.; Kamar, N.; Gatault, P.; Thaunat, O.; Legris, T.; Frimat, L.; et al. Is COVID-19 infection more severe in kidney transplant recipients? Am. J. Transplant. 2021, 21, 1295–1303. [Google Scholar] [CrossRef]
- Crespo, M.; Pérez-Sáez, M.J.; Redondo-Pachón, D.; Llinàs-Mallol, L.; Montero, M.M.; Villar-García, J.; Arias-Cabrales, C.; Buxeda, A.; Burballa, C.; Vázquez, S.; et al. COVID-19 in elderly kidney transplant recipients. Am. J. Transplant. 2020, 20, 2883–2889. [Google Scholar] [CrossRef]
- Goffin, E.; Candellier, A.; Vart, P.; Noordzij, M.; Arnol, M.; Covic, A.; Lentini, P.; Malik, S.; Reichert, L.J.; Sever, M.S.; et al. COVID-19 related mortality in kidney transplant and hemodialysis patients: A comparative, prospective registry based study. Nephrol. Dial. Transplant. 2021. [Google Scholar] [CrossRef] [PubMed]
- La Milia, V.; Tonolo, S.; Luzzaro, F.; Bonato, C.; Cavalli, A.; Foglieni, B.; Debiase, C.; Limardo, M.; Longhi, S.; Ravasi, C.; et al. The humoral immune response to SARS-CoV-2 mounts and is durable in symptomatic haemodialysis patients. Nephrol. Dial. Transplant. 2021, 36, 1132–1134. [Google Scholar] [CrossRef]
- De Vriese, A.S.; Reynders, M. IgG Antibody Response to SARS-CoV-2 Infection and Viral RNA Persistence in Patients on Maintenance Hemodialysis. Am. J. Kidney Dis. 2020, 76, 440. [Google Scholar] [CrossRef]
- Shaikh, A.; Zeldis, E.; Campbell, K.N.; Chan, L. Prolonged SARS-CoV-2 viral RNA shedding and IgG antibody response to SARS-CoV-2 in patients on hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 290–292. [Google Scholar] [CrossRef]
- Labriola, L.; Scohy, A.; Seghers, F.; Perlot, Q.; de Greef, J.; Desmet, C.; Romain, C.; Morelle, J.; Yombi, J.-C.; Kabamba, B.; et al. A Longitudinal, 3-Month Serologic Assessment of SARS-CoV-2 Infections in a Belgian Hemodialysis Facility. Clin. J. Am. Soc. Nephrol. 2020, 16, CJN.12490720. [Google Scholar] [CrossRef]
- Forbes, S.; Davari, M.; Gnanasampanthan, S.; Roth, N.; Young, G.; Rajakariar, R.; Cove-Smith, A.; Yaqoob, M.M.; Cutino-Moguel, T.; Mahalingasivam, V.; et al. Persistence of antibody response to SARS-CoV-2 in a cohort of haemodialysis patients with COVID-19. Nephrol. Dial. Transplant. 2021, 36, 1292–1297. [Google Scholar] [CrossRef]
- Alfano, G.; Fontana, F.; Morisi, N.; Giaroni, F.; Mori, G.; Guaraldi, G.; Magistroni, R.; Cappelli, G. One-year persistence of neutralizing anti-SARS-CoV-2 antibodies in dialysis patients recovered from COVID-19. Hemodial. Int. 2021, 25, E53–E56. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Bachmann, F.; Naik, M.G.; Duettmann, W.; Duerr, M.; Zukunft, B.; Schwarz, T.; Corman, V.M.; Liefeldt, L.; Budde, K.; et al. Low Seroprevalence of SARS-CoV-2 Antibodies during Systematic Antibody Screening and Serum Responses in Patients after COVID-19 in a German Transplant Center. J. Clin. Med. 2020, 9, 3401. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Vlad, G.; Vasilescu, E.R.; Husain, S.A.; Liu, Y.N.; Sun, W.Z.; Chang, M.F.; Suciu-Foca, N.; Mohan, S. Disparity between levels of anti-RBD IgG and anti-nucleocapsid protein IgG antibodies in COVID-19–recovered patients who received a kidney transplant. Kidney Int. 2021, 100, 240–241. [Google Scholar] [CrossRef]
- Hartzell, S.; Bin, S.; Benedetti, C.; Haverly, M.; Gallon, L.; Zaza, G.; Riella, L.V.; Menon, M.C.; Florman, S.; Rahman, A.H.; et al. Evidence of potent humoral immune activity in COVID-19-infected kidney transplant recipients. Am. J. Transplant. 2020, 20, 3149–3161. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Vargas, G.G.; Velay, A.; Wendling, M.J.; Perrin, P.; Fafi-Kremer, S.; Caillard, S. Persistence of SARS-CoV-2 antibodies in kidney transplant recipients. Am. J. Transplant. 2021, 21, 2307–2310. [Google Scholar] [CrossRef]
- Chavarot, N.; Leruez-Ville, M.; Scemla, A.; Burger, C.; Amrouche, L.; Rouzaud, C.; Lebreton, X.; Martinez, F.; Sberro-Soussan, R.; Legendre, C.; et al. Decline and loss of anti–SARS-CoV-2 antibodies in kidney transplant recipients in the 6 months following SARS-CoV-2 infection. Kidney Int. 2021, 99, 486–488. [Google Scholar] [CrossRef]
- Fernández-Ruiz, M.; Olea, B.; Giménez, E.; Laguna-Goya, R.; Trujillo, H.; Caravaca-Fontán, F.; Gutiérrez, E.; López-Medrano, F.; Remigia, M.J.; Almendro-Vazquez, P.; et al. SARS-CoV-2-Specific Cell-Mediated Immunity in Kidney Transplant Recipients Recovered from COVID-19. Transplantation 2021, 105, 1372–1380. [Google Scholar] [CrossRef]
- Crespo, M.; Barrilado-Jackson, A.; Padilla, E.; Eguía, J.; Echeverria-Esnal, D.; Cao, H.; Faura, A.; Folgueiras, M.; Solà-Porta, E.; Pascual, S.; et al. Negative immune responses to two-dose mRNA COVID-19 vaccines in renal allograft recipients assessed with simple antibody and interferon gamma release assay cellular monitoring. Am. J. Transplant. 2021. [Google Scholar] [CrossRef]
- Murugesan, K.; Jagannathan, P.; Pham, T.D.; Pandey, S.; Bonilla, H.F.; Jacobson, K.; Parsonnet, J.; Andrews, J.R.; Weiskopf, D.; Sette, A.; et al. Interferon-gamma release assay for accurate detection of SARS-CoV-2 T cell response. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Betjes, M.G.H.; Langerak, A.W.; van der Spek, A.; de Wit, E.A.; Litjens, N.H.R. Premature aging of circulating T cells in patients with end-stage renal disease. Kidney Int. 2011, 80, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Meijers, R.W.J.; Litjens, N.; De Wit, E.A.; Langerak, A.W.; Baan, C.; Betjes, M. Uremia-associated immunological aging is stably imprinted in the T-cell system and not reversed by kidney transplantation. Transpl. Int. 2014, 27, 1272–1284. [Google Scholar] [CrossRef] [PubMed]
- Zuo, J.; Dowell, A.C.; Pearce, H.; Verma, K.; Long, H.M.; Begum, J.; Aiano, F.; Amin-Chowdhury, Z.; Hallis, B.; Stapley, L.; et al. Robust SARS-CoV-2-specific T cell immunity is maintained at 6 months following primary infection. Nat. Immunol. 2021, 22, 620–626. [Google Scholar] [CrossRef]
- Clarke, C.L.; Prendecki, M.; Dhutia, A.; Gan, J.; Edwards, C.; Prout, V.; Lightstone, L.; Parker, E.; Marchesin, F.; Griffith, M.; et al. Longevity of SARS-CoV-2 immune responses in hemodialysis patients and protection against reinfection. Kidney Int. 2021, 99, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Thieme, C.J.; Anft, M.; Paniskaki, K.; Blazquez-Navarro, A.; Doevelaar, A.; Seibert, F.S.; Hoelzer, B.; Konik, M.J.; Meister, T.L.; Pfaender, S.; et al. The Magnitude and Functionality of SARS-CoV-2 Reactive Cellular and Humoral Immunity in Transplant Population Is Similar to the General Population Despite Immunosuppression. Transplantation 2021, 105, 2156. [Google Scholar] [CrossRef] [PubMed]
- Candon, S.; Guerrot, D.; Drouot, L.; Lemoine, M.; Lebourg, L.; Hanoy, M.; Boyer, O.; Bertrand, D. T cell and antibody responses to SARS-CoV-2: Experience from a French transplantation and hemodialysis center during the COVID-19 pandemic. Am. J. Transplant. 2021, 21, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Danthu, C.; Hantz, S.; Dahlem, A.; Duval, M.; Ba, B.; Guibbert, M.; el Ouafi, Z.; Ponsard, S.; Berrahal, I.; Achard, J.-M.; et al. Humoral Response after SARS-CoV-2 mRNA Vaccination in a Cohort of Hemodialysis Patients and Kidney Transplant Recipients. J. Am. Soc. Nephrol. 2021, 32, 2153–2158. [Google Scholar] [CrossRef] [PubMed]
- Dęborska-Materkowska, D.; Kamińska, D. The Immunology of SARS-CoV-2 Infection and Vaccines in Solid Organ Transplant Recipients. Viruses 2021, 13, 1879. [Google Scholar] [CrossRef]
- Swai, J.; Gui, M.; Long, M.; Wei, Z.; Hu, Z.; Liu, S. Humoral and cellular immune response to severe acute respiratory syndrome coronavirus-2 vaccination in hemodialysis and kidney transplant patients. Nephrology 2021. [Google Scholar] [CrossRef]
- Broseta, J.J.; Rodríguez-Espinosa, D.; Rodríguez, N.; Mosquera, M.d.; Marcos, M.Á.; Egri, N.; Pascal, M.; Soruco, E.; Bedini, J.L.; Bayés, B.; et al. Humoral and Cellular Responses to mRNA-1273 and BNT162b2 SARS-CoV-2 Vaccines Administered to Hemodialysis Patients. Am. J. Kidney Dis. 2021, 78, 571–581. [Google Scholar] [CrossRef]
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501.e15. [Google Scholar] [CrossRef] [PubMed]
- Echeverría, G.; Guevara, Á.; Coloma, J.; Ruiz, A.M.; Vasquez, M.M.; Tejera, E.; de Waard, J.H. Pre-existing T-cell immunity to SARS-CoV-2 in unexposed healthy controls in Ecuador, as detected with a COVID-19 Interferon-Gamma Release Assay. Int. J. Infect. Dis. 2021, 105, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Pahl, M.V.; Gollapudi, S.; Sepassi, L.; Gollapudi, P.; Elahimehr, R.; Vaziri, N.D. Effect of end-stage renal disease on B-lymphocyte subpopulations, IL-7, BAFF and BAFF receptor expression. Nephrol. Dial. Transplant. 2010, 25, 205–212. [Google Scholar] [CrossRef]
- Yang, A.-P.; Liu, J.-P.; Tao, W.-Q.; Li, H.-M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef]
- Dávila-Collado, R.; Jarquín-Durán, O.; Solís-Vallejo, A.; Nguyen, M.; Espinoza, J. Elevated Monocyte to Lymphocyte Ratio and Increased Mortality among Patients with Chronic Kidney Disease Hospitalized for COVID-19. J. Pers. Med. 2021, 11, 224. [Google Scholar] [CrossRef] [PubMed]
- Nithya, G.; Lamech, T.M.; Arumugam, V.; Dineshkumar, T.; Gopalakrishnan, N.; Aiswarya, D.; Shaji, S.; Sastry, B.V.R.H.; Solomon, D.; Kannan, B.S.; et al. A clinical study on the changing dynamics of disease severity, management strategies and outcomes of COVID-19 in patients requiring haemodialysis. J. Nephrol. 2021, 34, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, X.; Wang, S.; Li, H. High Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Are Associated with Poor Survival in Patients with Hemodialysis. BioMed Res. Int. 2021, 2021, 9958081. [Google Scholar] [PubMed]
- Zinellu, A.; Sotgia, S.; Carru, C.; Mangoni, A.A. B-Type Natriuretic Peptide Concentrations, COVID-19 Severity, and Mortality: A Systematic Review and Meta-Analysis With Meta-Regression. Front. Cardiovasc. Med. 2021, 8, 690790. [Google Scholar] [CrossRef]
- Mathew, D.; Giles, J.R.; Baxter, A.E.; Oldridge, D.A.; Greenplate, A.R.; Wu, J.E.; Alanio, C.; Kuri-Cervantes, L.; Pampena, M.B.; D’Andrea, K.; et al. Deep immune profiling of COVID-19 patients reveals distinct immunotypes with therapeutic implications. Science 2020, 369, eabc8511. [Google Scholar] [CrossRef] [PubMed]
- Orologas-Stavrou, N.; Politou, M.; Rousakis, P.; Kostopoulos, I.V.; Ntanasis-Stathopoulos, I.; Jahaj, E.; Tsiligkeridou, E.; Gavriatopoulou, M.; Kastritis, E.; Kotanidou, A.; et al. Peripheral blood immune profiling of convalescent plasma donors reveals alterations in specific immune subpopulations even at 2 months post SARS-cov-2 infection. Viruses 2021, 13, 26. [Google Scholar] [CrossRef] [PubMed]
- Krajewska, M.; Kościelska-Kasprzak, K.; Kamińska, D.; Żabińska, M.; Myszka-Kozłowska, M.; Gomułkiewicz, A.; Dzięgiel, P.; Klinger, M. Kidney Transplant Outcome Is Associated with Regulatory T Cell Population and Gene Expression Early after Transplantation. J. Immunol. Res. 2019, 2019, 7452019. [Google Scholar] [CrossRef]
- Overgaard, N.H.; Jung, J.-W.; Steptoe, R.; Wells, J.W. CD4+/CD8+double-positive T cells: More than just a developmental stage? J. Leukoc. Biol. 2015, 97, 31–38. [Google Scholar] [CrossRef]
- Corey, L.; Beyrer, C.; Cohen, M.S.; Michael, N.L.; Bedford, T.; Rolland, M. SARS-CoV-2 Variants in Patients with Immunosuppression. N. Engl. J. Med. 2021, 385, 562–566. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| KTR | HD | |
|---|---|---|
| Number of patients | 54 | 26 |
| Gender (F/M) | 27/27 | 17/9 |
| Age (years) | 52.9 ± 11.4; 54, 45–62 | 58.4 ± 13.7; 61, 46–70 |
| BMI (kg/m2) | 25.6 ± 4.1; 26, 24–28 | 26.8 ± 5.6; 26, 22–31 |
| Blood type | ||
| 0 | 17 | 12 |
| A | 17 | 9 |
| B | 15 | 4 |
| AB | 5 | 1 |
| Duration of HD therapy (months) | - | 43.2 ± 37.3; 52; 5–64 |
| Time since KTx (months) | 68.9 ± 70.0; 47, 20–102 | - |
| Living/deceased donor | 5/49 | - |
| 1st/2nd/3rd transplant | 46/7/1 | - |
| Current IS | ||
| Steroids | 53 | 0 |
| Tacrolimus/Cyclosporine A | 49/5 | 1/0 |
| MPA/Azathioprine/mTOR/none | 39/1/4/10 | 0/0/0/0 |
| Induction of IS | ||
| Anti-IL-2R | 17 | - |
| Anti-CD3 | 2 | - |
| Comorbidities | ||
| Cardiovascular disease or atrial fibrillation or heart failure | 13 | 17 |
| Hypertension | 49 | 25 |
| diabetes mellitus | 13 | 8 |
| Lung disease | 0 | 1 |
| Chronic liver disease | 13 | 9 |
| Malignancy in history | 3 | 5 |
| Graft function | ||
| Serum creatinine (mg/dL) | 1.42 ± 0.47; 1.3, 1.2–1.6 | - |
| eGFR (mL/min/1.73 m2, MDRD) | 53.5 ± 15.1; 55, 44–59 | - |
| Other medications | ||
| ACEI/ARB | 4 | 8 |
| Statins | 17 | 7 |
| vitamin D | 10 | 22 |
| Smoking | 5 | 0 |
| rRT-PCR-Confirmed | Unconfirmed | p-Value | |
|---|---|---|---|
| Number of IgG positive samples | 11 | 13 | |
| IgG (BAU/mL) | 821.1 ± 1113.9 369, 207–746 | 256.5 ± 409.5 111, 64–207 | 0.016 |
| Number of IgA positive samples | 11 | 12 | |
| IgA (ratio to the cutoff) | 28.91 ± 43.34 12.5, 6.3–33.5 | 13.47 ± 16.58 6.4, 3.4–15.9 | 0.247 |
| Number of IgM positive samples | 0 | 3 | |
| IgM (ratio to the cutoff) | 1.51; 1.92; 3.06 | – |
| rRT-PCR-Confirmed | Unconfirmed | |
|---|---|---|
| Number of IgG positive samples | 10 | 3 |
| IgG (BAU/mL) | 551.3 ± 483.8 529, 51–967 | 106; 534; 635 |
| Number of IgA positive samples | 10 | 3 |
| IgA (ratio to the cutoff) | 28.64 ± 46.25 5.4, 3.7–44.3 | 2.6; 6.2; 19.9 |
| Number of IgM positive samples | 1 | 1 |
| IgM (ratio to the cutoff) | 11.5 | 10.4 |
| Patients Group | IGRA Response | rRT-PCR-Confirmed | rRT-PCR-Unconfirmed | p-Value |
|---|---|---|---|---|
| HD | mIU/mL * | 975.0 ± 736.7 1008, 64–1700 | 1320; 1700; 1700 | 0.291 |
| >64 mIU/mL % (positive/total cases) | 72.7% (8/11) | 100% (3/3) | ||
| KTR | mIU/mL | 617.1 ± 744.7 241, 61–1520 | 222.1 ± 457.4 53, 23–236 | 0.207 |
| >64 mIU/mL % (positive/total cases) | 75.0% (9/12) | 46.2% (6/13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamińska, D.; Augustyniak-Bartosik, H.; Kościelska-Kasprzak, K.; Żabińska, M.; Bartoszek, D.; Poznański, P.; Kuriata-Kordek, M.; Kusztal, M.; Mazanowska, O.; Krajewska, M. Comparing Humoral and Cellular Adaptive Immunity during Convalescent Phase of COVID-19 in Hemodialysis Patients and Kidney Transplant Recipients. J. Clin. Med. 2021, 10, 4833. https://doi.org/10.3390/jcm10214833
Kamińska D, Augustyniak-Bartosik H, Kościelska-Kasprzak K, Żabińska M, Bartoszek D, Poznański P, Kuriata-Kordek M, Kusztal M, Mazanowska O, Krajewska M. Comparing Humoral and Cellular Adaptive Immunity during Convalescent Phase of COVID-19 in Hemodialysis Patients and Kidney Transplant Recipients. Journal of Clinical Medicine. 2021; 10(21):4833. https://doi.org/10.3390/jcm10214833
Chicago/Turabian StyleKamińska, Dorota, Hanna Augustyniak-Bartosik, Katarzyna Kościelska-Kasprzak, Marcelina Żabińska, Dorota Bartoszek, Paweł Poznański, Magdalena Kuriata-Kordek, Mariusz Kusztal, Oktawia Mazanowska, and Magdalena Krajewska. 2021. "Comparing Humoral and Cellular Adaptive Immunity during Convalescent Phase of COVID-19 in Hemodialysis Patients and Kidney Transplant Recipients" Journal of Clinical Medicine 10, no. 21: 4833. https://doi.org/10.3390/jcm10214833