
Pathobiology of Cutaneous Manifestations Associated with COVID-19 and Their Management
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
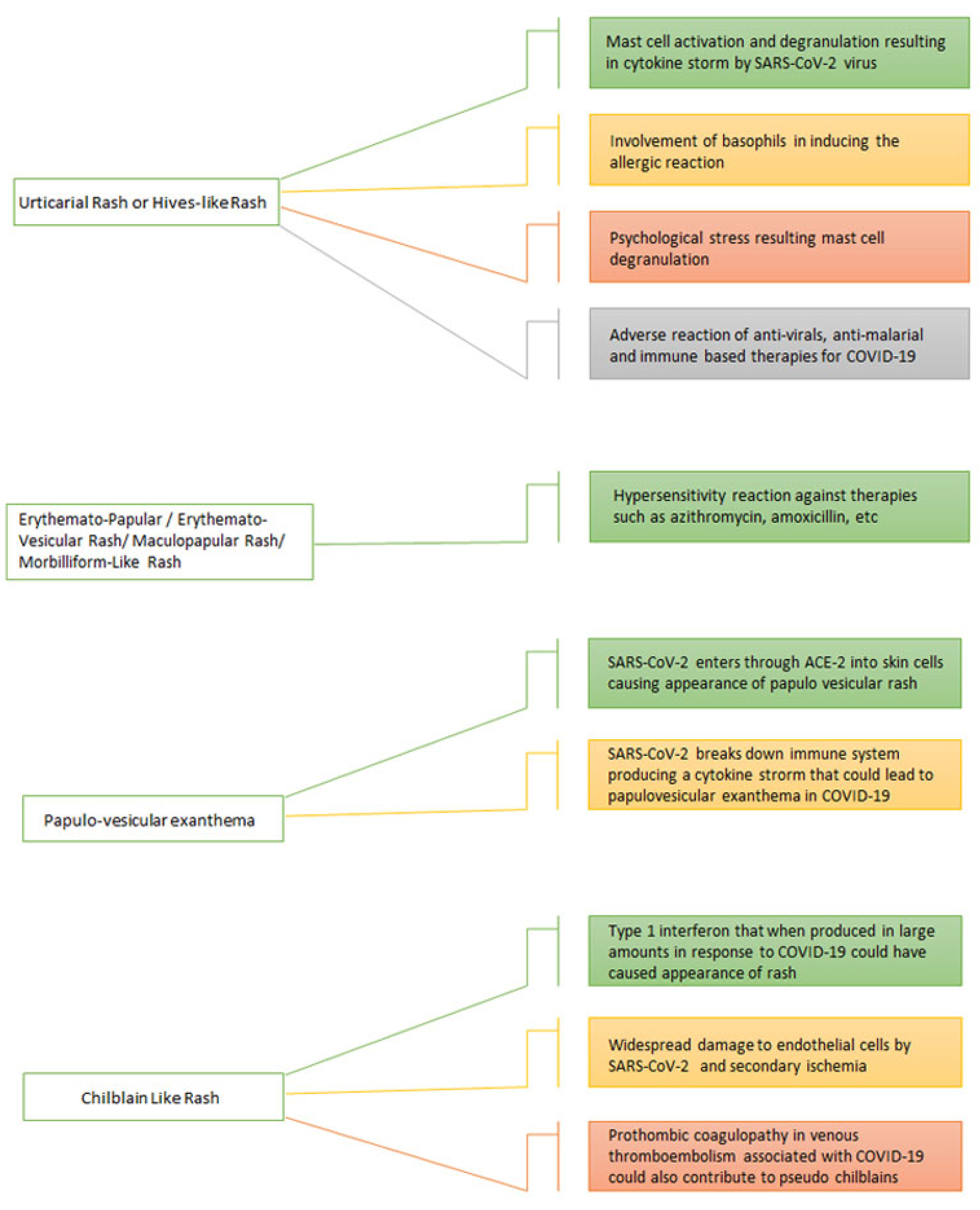
3.1. Urticarial Eruptions and COVID-19
3.1.1. Prevalence and Associated Clinical Features
3.1.2. Pathophysiology
Mast-Cell-Mediated Response
Eosinophils Infiltration
Basophils Infiltration
Stress-Induced Response
Drug Hypersensitivity
3.1.3. Management
3.2. Erythemato-Papular or Erythematous-Vesicular Rash or Maculopapular Rash or Morbilliform-like Rash
3.2.1. Prevalence and Associated Clinical Features
3.2.2. Pathophysiology
Drug Hypersensitivity
3.2.3. Management
3.3. Papulo-Vesicular Exanthema
3.3.1. Prevalence and Associated Clinical Features
3.3.2. Pathophysiology
3.3.3. Management
3.4. Chilblain-like Rash
3.4.1. Prevalence and Associated Clinical Features

{kind=link}
{kind=link}
| Type of Rash Associated with COVID-19 | Prevalence (%) | Mean Age (Years) | Gender Predominance (Male/Female) | Clinical Features | Associated Symptoms | Healing Duration | Treatment | Survival Rate (%) |
|---|---|---|---|---|---|---|---|---|
| Urticarial Rash [4,14] | 15–20% | 38 | Female | Red itchy elevated rash on trunk and limbs | Cough Dyspnea Fever Chills Angioedema | 24 h | Low dose corticosteriodAnti-histamines | 98% |
| Erythemato-Papular/Erythematous-Vesicular Rash/Maculopapular Rash/Morbilliform-like Rash [28] | 45% | 60 | Male | Erythematous pruritic rash having both flat and raised areas on trunk and limbs | cough fever pneumonia | 1 week | Oral and tropical steroids Triamcinolone | 100% |
| Papulo-vesicular exanthema [7] | 4–9% | 40–60 | Female | Widespread, varied sized polymorphic papules or vesicles Itchy, monomorphic vesicles on trunk | None | 8 days | Conservative/Observational | 98% |
| Chilblain-like rash [42] | 16–30% | 13–20 | Both | Red to purple, itchy, painful rash on toes and fingers | None | 1–2 weeks | Conservative/Observational Tropical corticosteroids | 98% |
3.4.2. Pathophysiology
Type 1 Interferon Response
Endothelial Cell Damage and Ischemia
Prothrombotic Coagulopathy
3.4.3. Management
3.5. Other Cutaneous Manifestations
3.6. Cutaneous Manifestations in Viral Variants of COVID-19
3.7. Cutaneous Findings in Long-Standing COVID-19 Patients
3.8. Skin Lesions in Vaccinated Individual
4. Conclusions
5. Strength and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID Live-Coronavirus Statistics-Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 26 December 2021).
- Behzad, S.; Aghaghazvini, L.; Radmard, A.R.; Gholamrezanezhad, A. Extrapulmonary manifestations of COVID-19: Radiologic and clinical overview. Clin. Imaging. 2020, 66, 35–41. [Google Scholar] [CrossRef]
- Torjesen, I. COVID-19: Omicron may be more transmissible than other variants and partly resistant to existing vaccines, scientists fear. BMJ 2021, 375, n2943. [Google Scholar] [CrossRef]
- Recalcati, S. Cutaneous manifestations in COVID-19: A first perspective. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e212–e213. [Google Scholar] [CrossRef]
- McMahon, D.E.; Gallman, A.E.; Hruza, G.J.; Rosenbach, M.; Lipoff, J.B.; Desai, S.R.; French, L.E.; Lim, H.; Cyster, J.G.; Fox, L.P.; et al. Long COVID in the skin: A registry analysis of COVID-19 dermatological duration. Lancet Infect. Dis. 2021, 21, 313–314. [Google Scholar] [CrossRef]
- Genovese, G.; Moltrasio, C.; Berti, E.; Marzano, A.V. Skin Manifestations Associated with COVID-19: Current Knowledge and Future Perspectives. Dermatology 2021, 237, 1–12. [Google Scholar] [CrossRef]
- Marzano, A.V.; Cassano, N.; Genovese, G.; Moltrasio, C.; Vena, G.A. Cutaneous manifestations in patients with COVID-19: A preliminary review of an emerging issue. Br. J. Dermatol. 2020, 183, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, P.; Hajikhani, B.; Mirsaeidi, M.; Vahidnezhad, H.; Dadashi, M.; Nasiri, M.J. Skin Manifestations in COVID-19 Patients: Are They Indicators for Disease Severity? A Systematic Review. Front. Med. 2021, 8, 634208. [Google Scholar] [CrossRef] [PubMed]
- Meiliani, P.D. ACE2 Receptor in the skin and Cutaneous Manifestations of SARS-CoV-2: A Review of the Literature. Biosci. Med. 2020, 5, 204–211. [Google Scholar] [CrossRef]
- Novembre, E.; Cianferoni, A.; Mori, F.; Barni, S.; Calogero, C.; Bernardini, R.; Di Grande, L.; Pucci, N.; Azzari, C.; Vierucci, A. Urticaria and urticaria related skin condition/disease in children. Eur. Ann. Allergy Clin. Immunol. 2007, 39, 253–258. [Google Scholar] [PubMed]
- Gonçalo, M.; Gimenéz-Arnau, A.; Al-Ahmad, M.; Ben-Shoshan, M.; Bernstein, J.A.; Ensina, L.F.; Fomina, D.; Galvàn, C.A.; Godse, K.; Grattan, C.; et al. The global burden of chronic urticaria for the patient and society. Br. J. Dermatol. 2021, 184, 226–236. [Google Scholar] [CrossRef]
- Galván Casas, C.; Català, A.; Carretero Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas Velasco, M.; et al. Classification of the cutaneous manifestations of COVID-19: A rapid prospective nationwide consensus study in Spain with 375 cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef]
- Freeman, E.E.; McMahon, D.E.; Lipoff, J.B.; Rosenbach, M.; Kovarik, C.; Desai, S.R.; Harp, J.; Takeshita, J.; French, L.E.; Lim, H.W.; et al. The spectrum of COVID-19–associated dermatologic manifestations: An international registry of 716 patients from 31 countries. J. Am. Acad. Dermatol. 2020, 83, 1118–1129. [Google Scholar] [CrossRef]
- Pagali, S.; Parikh, R.S. Severe urticarial rash as the initial symptom of COVID-19 infection. BMJ Case Rep. 2021, 14, e241793. [Google Scholar] [CrossRef]
- Tan, S.W.; Tam, Y.C.; Oh, C.C. Skin manifestations of COVID-19: A worldwide review. JAAD Int. 2021, 2, 119–133. [Google Scholar] [CrossRef]
- Dastoli, S.; Bennardo, L.; Patruno, C.; Nisticò, S.P. Are erythema multiforme and urticaria related to a better outcome of COVID-19? Dermatol. Ther. 2020, 33, e13681. [Google Scholar] [CrossRef]
- Zuberbier, T.; Aberer, W.; Asero, R.; Abdul Latiff, A.H.; Baker, D.; Ballmer-Weber, B.; Bernstein, J.A.; Bindslev-Jensen, C.; Brzoza, Z.; Buense Bedrikow, R.; et al. The EAACI/GA2LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy 2009, 64, 1417–1426. [Google Scholar] [CrossRef]
- Kocatürk, E.; Salman, A.; Cherrez-Ojeda, I.; Criado, P.R.; Peter, J.; Comert-Ozer, E.; Abuzakouk, M.; Agondi, R.C.; Al-Ahmad, M.; Altrichter, S.; et al. The global impact of the COVID-19 pandemic on the management and course of chronic urticaria. Allergy 2020, 76, 816–830. [Google Scholar] [CrossRef]
- Algaadi, S.A. Urticaria and COVID-19: A review. Dermatol. Ther. 2020, 33, e14290. [Google Scholar] [CrossRef]
- Zandifar, A.; Badrfam, R.; Yazdani, S.; Arzaghi, S.M.; Rahimi, F.; Ghasemi, S.; Khamisabadi, S.; Mohammadian Khonsari, N.; Qorbani, M. Prevalence and severity of depression, anxiety, stress and perceived stress in hospitalized patients with COVID-19. J. Diabetes Metab. Disord. 2020, 19, 1431–1438. [Google Scholar] [CrossRef]
- Baldwin, A.L. Mast Cell Activation by Stress. In Mast Cells; Humana Press: Totowa, NJ, USA, 2005; Volume 315, pp. 349–360. ISBN 978-1-59259-967-7. [Google Scholar]
- Singh, H.; Kaur, H.; Singh, K.; Sen, C.K. Cutaneous Manifestations of COVID-19: A Systematic Review. Adv. Wound Care 2021, 10, 51–80. [Google Scholar] [CrossRef]
- Schwartz, R.A.; Janniger, C.K. Generalized pustular figurate erythema: A newly delineated severe cutaneous drug reaction linked with hydroxychloroquine. Dermatol. Ther. 2020, 33, e13380. [Google Scholar] [CrossRef] [PubMed]
- Abadías-Granado, I.; Palma-Ruiz, A.M.; Cerro, P.A.; Morales-Callaghan, A.M.; Gómez-Mateo, M.C.; Gilaberte, Y.; Schwartz, R.A. Generalized pustular figurate erythema first report in two COVID-19 patients on hydroxychloroquine. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e5–e7. [Google Scholar] [CrossRef] [PubMed]
- Aktaş, H.; Hamidi, A.A. Urticaria in a patient with COVID-19: Therapeutic and diagnostic difficulties. Dermatol. Ther. 2020, 33, e13610. [Google Scholar] [CrossRef] [PubMed]
- Abuelgasim, E.; Dona, A.C.M.; Sondh, R.S.; Harky, A. Management of urticaria in COVID-19 patients: A systematic review. Dermatol. Ther. 2021, 34, e14328. [Google Scholar] [CrossRef]
- De Lorenzo Alvarez, A.; Revilla, Á.; Corbalán, T.; Villar, A.; Espinel, L.; Martins, J.; Cubas, A. Ischemic stroke and purpuric dermatitis as COVID-19-related complications in a peritoneal dialysis patient. CEN Case Rep. 2021, 10, 250–254. [Google Scholar] [CrossRef]
- Jimenez-Cauhe, J.; Ortega-Quijano, D.; Carretero-Barrio, I.; Suarez-Valle, A.; Saceda-Corralo, D.; Moreno-Garcia Del Real, C.; Fernandez-Nieto, D. Erythema multiforme-like eruption in patients with COVID-19 infection: Clinical and histological findings. Clin. Exp. Dermatol. 2020, 45, 892–895. [Google Scholar] [CrossRef]
- Caputo, V.; Metze, D.; Bonoldi, E.; Merli, M.; Rongioletti, F. Peculiar Histopathologic Feature of an Erythematous/Morbilliform Eruption in a COVID-19-Positive Patient. Am. J. Dermatopathol. 2021, 43, 962–964. [Google Scholar] [CrossRef]
- Zengarini, C.; Orioni, G.; Cascavilla, A.; Horna Solera, C.; Fulgaro, C.; Misciali, C.; Patrizi, A.; Gaspari, V. Histological pattern in COVID-19-induced viral rash. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e453–e454. [Google Scholar] [CrossRef]
- Najarian, D.J. Morbilliform exanthem associated with COVID-19. JAAD Case Rep. 2020, 6, 493–494. [Google Scholar] [CrossRef]
- Gianotti, R.; Veraldi, S.; Recalcati, S.; Cusini, M.; Ghislanzoni, M.; Boggio, F.; Fox, L.P. Cutaneous Clinico-Pathological Findings in three COVID-19-Positive Patients Observed in the Metropolitan Area of Milan, Italy. Acta. Derm. Venereol. 2020, 100, 1–2. [Google Scholar] [CrossRef]
- Ahouach, B.; Harent, S.; Ullmer, A.; Martres, P.; Bégon, E.; Blum, L.; Tess, O.; Bachmeyer, C. Cutaneous lesions in a patient with COVID-19: Are they related? Br. J. Dermatol. 2020, 183, e31. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Askin, O.; Altunkalem, R.N.; Altinisik, D.D.; Uzuncakmak, T.K.; Tursen, U.; Kutlubay, Z. Cutaneous manifestations in hospitalized patients diagnosed as COVID-19. Dermatol. Ther. 2020, 33, e13896. [Google Scholar] [CrossRef]
- Bouaziz, J.D.; Duong, T.A.; Jachiet, M.; Velter, C.; Lestang, P.; Cassius, C.; Arsouze, A.; Domergue Than Trong, E.; Bagot, M.; Begon, E.; et al. Vascular skin symptoms in COVID-19: A French observational study. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e451–e452. [Google Scholar] [CrossRef]
- De Giorgi, V.; Recalcati, S.; Jia, Z.; Chong, W.; Ding, R.; Deng, Y.; Scarfi, F.; Venturi, F.; Trane, L.; Gori, A.; et al. Cutaneous manifestations related to coronavirus disease 2019 (COVID-19): A prospective study from China and Italy. J. Am. Acad. Dermatol. 2020, 83, 674–675. [Google Scholar] [CrossRef]
- Fernandez-Nieto, D.; Ortega-Quijano, D.; Jimenez-Cauhe, J.; Burgos-Blasco, P.; Perosanz-Lobo, D.; Suarez-Valle, A.; Cortes-Cuevas, J.L.; Carretero, I.; Garcia-Del Real, C.; Fernandez-Guarino, M. Clinical and histological characterization of vesicular COVID-19 rashes: A prospective study in a tertiary care hospital. Clin. Exp. Dermatol. 2020, 45, 872–875. [Google Scholar] [CrossRef]
- Li, M.-Y.; Li, L.; Zhang, Y.; Wang, X.-S. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef]
- Gottlieb, M.; Long, B. Dermatologic manifestations and complications of COVID-19. Am. J. Emerg. Med. 2020, 38, 1715–1721. [Google Scholar] [CrossRef]
- Criado, P.R.; Abdalla, B.M.Z.; de Assis, I.C.; van Blarcum de Graaff Mello, C.; Caputo, G.C.; Vieira, I.C. Are the cutaneous manifestations during or due to SARS-CoV-2 infection/COVID-19 frequent or not? Revision of possible pathophysiologic mechanisms. Inflamm. Res. 2020, 69, 745–756. [Google Scholar] [CrossRef]
- Ladha, M.A.; Luca, N.; Constantinescu, C.; Naert, K.; Ramien, M.L. Approach to Chilblains During the COVID-19 Pandemic. J. Cutan. Med. Surg. 2020, 24, 504–517. [Google Scholar] [CrossRef]
- Massey, P.R.; Jones, K.M. Going viral: A brief history of Chilblain-like skin lesions (“COVID toes”) amidst the COVID-19 pandemic. Semin. Oncol. 2020, 47, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Kanitakis, J.; Lesort, C.; Danset, M.; Jullien, D. Chilblain-like acral lesions during the COVID-19 pandemic (“COVID toes”): Histologic, immunofluorescence, and immunohistochemical study of 17 cases. J. Am. Acad. Dermatol. 2020, 83, 870–875. [Google Scholar] [CrossRef] [PubMed]
- Freeman, E.E.; McMahon, D.E.; Lipoff, J.B.; Rosenbach, M.; Kovarik, C.; Takeshita, J.; French, L.E.; Thiers, B.H.; Hruza, G.J.; Fox, L.P. Pernio-like skin lesions associated with COVID-19: A case series of 318 patients from 8 countries. J. Am. Acad. Dermatol. 2020, 83, 486–492. [Google Scholar] [CrossRef]
- Burke, K.T.; McGinnis, K.S.; Petronic-Rosic, V. COVID toes: Pernio-like lesions. Clin. Dermatol. 2021, 39, 380–383. [Google Scholar] [CrossRef]
- Giavedoni, P.; Podlipnik, S.; Pericàs, J.M.; Fuertes de Vega, I.; García-Herrera, A.; Alós, L.; Carrera, C.; Andreu-Febrer, C.; Sanz-Beltran, J.; Riquelme-Mc Loughlin, C.; et al. Skin Manifestations in COVID-19: Prevalence and Relationship with Disease Severity. J. Clin. Med. 2020, 9, 3261. [Google Scholar] [CrossRef]
- Hernandez, C.; Bruckner, A.L. Focus on “COVID Toes”. JAMA Dermatol. 2020, 156, 1003. [Google Scholar] [CrossRef]
- Fabbrocini, G.; Vastarella, M.; Nappa, P.; Annunziata, M.C.; Camela, E.; Greco, V.; Gaudiello, F.; Alessio, M.; Pierri, L.; Catzola, A.; et al. A new dermoscopic pattern for chilblain-COVID-19–like skin lesions in adolescents. JAAD Case Rep. 2020, 6, 1271–1274. [Google Scholar] [CrossRef]
- Pavone, P.; Marino, S.; Marino, L.; Cacciaguerra, G.; Guarneri, C.; Nunnari, G.; Taibi, R.; Marletta, L.; Falsaperla, R. Chilblains-like lesions and SARS-CoV-2 in children: An overview in therapeutic approach. Dermatol. Ther. 2021, 34, e14502. [Google Scholar] [CrossRef]
- Rubio-Muniz, C.A.; Puerta-Peña, M.; Falkenhain-López, D.; Arroyo-Andrés, J.; Agud-Dios, M.; Rodriguez-Peralto, J.L.; Ortiz-Romero, P.L.; Rivera-Díaz, R. The broad spectrum of dermatological manifestations in COVID-19: Clinical and histopathological features learned from a series of 34 cases. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e574–e576. [Google Scholar] [CrossRef]
- Covid: 6 Omicron Skin Symptoms You Must Never Ignore|News.com.Au—Australia’s Leading News Site. Available online: https://www.news.com.au/world/coronavirus/health/six-covid-skin-symptoms-you-must-never-ignore/news-story/1e5c0be9e70b606ca275c9e87812de3a (accessed on 27 August 2022).
- Colmenero, I.; Santonja, C.; Alonso-Riaño, M.; Noguera-Morel, L.; Hernández-Martín, A.; Andina, D.; Wiesner, T.; Rodríguez-Peralto, J.L.; Requena, L.; Torrelo, A. SARS-CoV-2 endothelial infection causes COVID-19 chilblains: Histopathological, immunohistochemical and ultrastructural study of seven paediatric cases. Br. J. Dermatol. 2020, 183, 729–737. [Google Scholar] [CrossRef]
- Atzori, L.; Recalcati, S.; Ferreli, C.; Hoenig, L.J.; Rongioletti, F. COVID-19–related skin manifestations: Update on therapy. Clin. Dermatol. 2021, 39, 920–926. [Google Scholar] [CrossRef]
- Serafini, A.; Kurotschka, P.K.; Bertolani, M.; Riccomi, S. An itchy erythematous papular skin rash as a possible early sign of COVID-19: A case report. J. Med. Case Rep. 2020, 14, 216. [Google Scholar] [CrossRef]
- Birlutiu, V.; Feiereisz, A.I.; Oprinca, G.; Dobritoiu, S.; Rotaru, M.; Birlutiu, R.M.; Iancu, G.M. Cutaneous manifestations associated with anosmia, ageusia and enteritis in SARS-CoV-2 infection–A possible pattern? Observational study and review of the literature. Int. J. Infect. Dis. 2021, 107, 72–77. [Google Scholar] [CrossRef]
- Goren, A.; Vaño-Galván, S.; Wambier, C.G.; McCoy, J.; Gomez-Zubiaur, A.; Moreno-Arrones, O.M.; Shapiro, J.; Sinclair, R.D.; Gold, M.H.; Kovacevic, M.; et al. A preliminary observation: Male pattern hair loss among hospitalized COVID-19 patients in Spain-A potential clue to the role of androgens in COVID-19 severity. J. Cosmet Derm. 2020, 19, 1545–1547. [Google Scholar] [CrossRef]
- Veraldi, S.; Romagnuolo, M.; Benzecry, V. Pityriasis rosea-like eruption revealing COVID-19. Australas. J. Dermatol. 2021, 62, e333–e334. [Google Scholar] [CrossRef]
- Leerunyakul, K.; Pakornphadungsit, K.; Suchonwanit, P. Case Report: Pityriasis Rosea-Like Eruption Following COVID-19 Vaccination. Front. Med. 2021, 8, 752443. [Google Scholar] [CrossRef]
- Carballido Vázquez, A.M.; Morgado, B. Pityriasis rosea-like eruption after Pfizer-BioNTech COVID-19 vaccination. Br. J. Dermatol. 2021, 185, e34. [Google Scholar] [CrossRef]
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 21 August 2022).
- Visconti, A.; Murray, B.; Rossi, N.; Wolf, J.; Ourselin, S.; Spector, T.D.; Freeman, E.E.; Bataille, V.; Falchi, M. Cutaneous Manifestations of SARS-CoV-2 infection during the Delta and Omicron waves in 348,691 UK users of the UK ZOE COVID Study App. Br. J. Dermatol. 2022, bjd.21784. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. Comparison of Outcomes from COVID Infection in Pediatric and Adult Patients before and after the Emergence of Omicron. Infectious Diseases (except HIV/AIDS). medRxiv. [CrossRef]
- Venkatesan, P. NICE guideline on long COVID. Lancet Respir. Med. 2021, 9, 129. [Google Scholar] [CrossRef]
- Förster, C.; Colombo, M.G.; Wetzel, A.-J.; Martus, P.; Joos, S. Persisting symptoms after COVID-19. Dtsch. Ärzteblatt Int. 2022, 119, 167–174. [Google Scholar] [CrossRef]
- Desai, A.D.; Lavelle, M.; Boursiquot, B.C.; Wan, E.Y. Long-term complications of COVID-19. Am. J. Physiol. Cell Physiol. 2022, 322, C1–C11. [Google Scholar] [CrossRef]
- Fernández-Lázaro, D.; Garrosa, M. Identification, Mechanism, and Treatment of Skin Lesions in COVID-19: A Review. Viruses 2021, 13, 1916. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masood, W.; Ahmad, S.; Khan, N.A.; Shakir, A.; Rokni, G.R.; Gold, M.H.; Cockerell, C.J.; Schwartz, R.A.; Goldust, M. Pathobiology of Cutaneous Manifestations Associated with COVID-19 and Their Management. Viruses 2022, 14, 1972. https://doi.org/10.3390/v14091972
Masood W, Ahmad S, Khan NA, Shakir A, Rokni GR, Gold MH, Cockerell CJ, Schwartz RA, Goldust M. Pathobiology of Cutaneous Manifestations Associated with COVID-19 and Their Management. Viruses. 2022; 14(9):1972. https://doi.org/10.3390/v14091972
Chicago/Turabian StyleMasood, Waniyah, Shahzaib Ahmad, Noor Ayman Khan, Amaima Shakir, Ghasem Rahmatpour Rokni, Michael H. Gold, Clay J. Cockerell, Robert A. Schwartz, and Mohamad Goldust. 2022. "Pathobiology of Cutaneous Manifestations Associated with COVID-19 and Their Management" Viruses 14, no. 9: 1972. https://doi.org/10.3390/v14091972