
Impact of the Organizational Model Adopted during the COVID-19 Pandemic on the Perceived Safety of Intensive Care Unit Staff

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Development, Design, and Conduction
2.2. Primary Outcome
- ⮚
- Perception of safety of staff working in the COVID-19 ICU.
2.3. Secondary Outcome
- ⮚
- Incidence of biohazard injuries, perception of training.
- ⮚
- Number of COVID-19+ cases in health care workers in the COVID-19 area found with regular screening after entering the COVID-19 ICU.
- ⮚
- Incidence of tendency to self-isolate in relation to the adopted organizational model.
- ⮚
- Incidence of additional requests for health surveillance interventions in health care personnel working in the COVID-19 area.
2.4. Statistical Analysis
- Age groups (20–30; 31–40; 41–50; over 50).
- Sex.
- Professional category.
- Years of ICU experience (>6 months; 6 months to 1 year); 1 to 3 years; <3 years).
- Exposure time in the COVID-19 ICU (<1 month; 1 to 3 months; 3 to 6 months; <6 months).
- Family and cohabiting settings.
3. Results
3.1. General Data
3.2. Health Surveillance
3.3. Training
3.4. Staff Risk Perception
3.5. Adherence to the Use of PPE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, X.; Lin, L.; Xuan, Z.; Xu, J.; Wan, Y.; Zhou, X. Risk communication on behavioral responses during COVID-19 among general population in China: A rapid national study. J. Infect. 2020, 81, 911–922. [Google Scholar] [CrossRef]
- Koh, Y.; Hegney, D.G.; Drury, V. Comprehensive Systematic review of healthcare workers’ perceptions of risk and use of coping strategies towards emerging respiratory infectious diseases. Int. J. Evid.-Based Healthc. 2011, 9, 403–419. [Google Scholar] [CrossRef]
- Bahrs, C.; Kimmig, A.; Weis, S.; Ankert, J.; Hagel, S.; Maschmann, J.; Stallmach, A.; Steiner, A.; Bauer, M.; Behringer, W.; et al. Prospective surveillance study in a 1,400-bed university hospital: COVID-19 Exposure at home was the main risk factor for SARS-CoV-2 point seroprevalence among hospital staff. Transbounding Emerg. Dis. 2021, 1–11. [Google Scholar] [CrossRef]
- Nasa, P.; Azoulay, E.; Chakrabarti, A.; Divatia, J.V.; Jain, R.; Rodrigues, C.; Rosenthal, V.D.; Alhazzani, W.; Arabi, Y.M.; Bakker, J.; et al. Infection control in the intensive care unit: Expert consensus statements for SARS-CoV-2 using a Delphi method. Lancet Infect. Dis. 2022, 22, e74–e87. [Google Scholar] [CrossRef]
- World Health Organization. For Survey Tool and Guidance: Rapid, Simple, Flexible Behavioural Insights on COVID-19; World Health Organization: Geneva, Switzerland, 2020; 40p. [Google Scholar]
- World Health Organization. Risk Assessment and Management of Exposure of Health Care Workers in the Context of COVID-19: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020; 6p. [Google Scholar]
- Carenzo, L.; Elli, D.; Mainetti, M.; Costantini, E.; Rendiniello, V.; Protti, A.; Sartori, F.; Cecconi, M. A Dedicated multidisciplinary safety briefing for the COVID-19 critical care. Intensive Crit. Care Nurs. 2020, 60, 102882. [Google Scholar] [CrossRef]
- Conoscenti, E.; Martucci, G.; Piazza, M.; Tuzzolino, F.; Ragonese, B.; Burgio, G.; Arena, G.; Blot, S.; Luca, A.; Arcadipane, A.; et al. Post-Crisis debriefing: A tool for improving quality in the medical emergency team system. Intensive Crit. Care Nurs. 2021, 63, 102977. [Google Scholar] [CrossRef] [PubMed]
- Conoscenti, E.; Blot, S.; Lombardo, R.; Campanella, M.; Luca, A. Good habits from the pandemic age to bring home: Effective communication and briefing tools. Intensive Crit. Care Nurs. 2021, 65, 103056. [Google Scholar] [CrossRef]
- Hildreth, B.A.; Panarello, G.; Martucci, G.; Tuzzolino, F.; Piacentini, A.; Occhipinti, G.; Giunta, A.; Genco, F.; Raffa, G.M.; Pilato, M.; et al. ECMO retrieval over the Mediterranean sea: Extending hospital arms. Membranes 2021, 11, 210. [Google Scholar] [CrossRef] [PubMed]
- Jansson, M.; Liao, X.; Rello, J. Strengthening ICU health security for a coronavirus epidemic. Intensive Crit. Care Nurs. 2020, 57, 102812. [Google Scholar] [CrossRef] [PubMed]
- Lormans, P.; Blot, S.; Amerlinck, S.; Devriendt, Y.; Dumoulin, A. COVID-19 acquisition risk among ICU nursing staff with patient-driven use of aerosol-generating respiratory procedures and optimal use of personal protective equipment. Intensive Crit. Care Nurs. 2021, 63, 102993. [Google Scholar] [CrossRef]
- Kelley, K. Good practice in the conduct and reporting of survey research. Int. J. Qual. Health Care 2003, 15, 261–266. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G. Improving the quality of web surveys: The checklist for reporting results of internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- Bhagavathula, A.S.; Raghavan, V.R.; Ahmadi, A.; Srirag, D.; Chattu, V.K. Frontline healthcare workers’ knowledge, perception and risk prevention practices regarding COVID-19 in afghanistan: A cross-sectional study. Med. Sci. 2021, 9, 2. [Google Scholar] [CrossRef]
- Arslanca, T.; Fidan, C.; Daggez, M.; Dursun, P. Knowledge, preventive behaviors and risk perception of the COVID-19 pandemic: A cross-sectional study in Turkish health care workers. PLoS ONE 2021, 16, e0250017. [Google Scholar] [CrossRef] [PubMed]
- Chu, E.; Lee, K.-M.; Stotts, R.; Benjenk, I.; Ho, G.; Yamane, D.; Mullins, B.; Heinz, E.R. Hospital-Based health care worker perceptions of personal risk related to COVID-19. J. Am. Board Fa Med. 2021, 34, S103–S112. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Vezzosi, L.; Balzarini, F.; Bragazzi, N.L. Inappropriate risk perception for SARS-CoV-2 infection among Italian HCWs in the Eve of COVID-19 pandemic. Acta Bio. Med. Atenei. Parm. 2020, 91, e2020040. [Google Scholar] [CrossRef]
- Erquicia, J.; Valls, L.; Barja, A.; Gil, S.; Miquel, J.; Leal-Blanquet, J.; Schmidt, C.; Checa, J.; Vega, D. Impacto emocional de la pandemia de COVID-19 en los trabajadores sanitarios de uno de los focos de contagio más importantes de Europa. Med. Clín. 2020, 155, 434–440. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structural and Training Procedural Elements Implemented for the Opening of the COVID-19 ICU Area | |
|---|---|
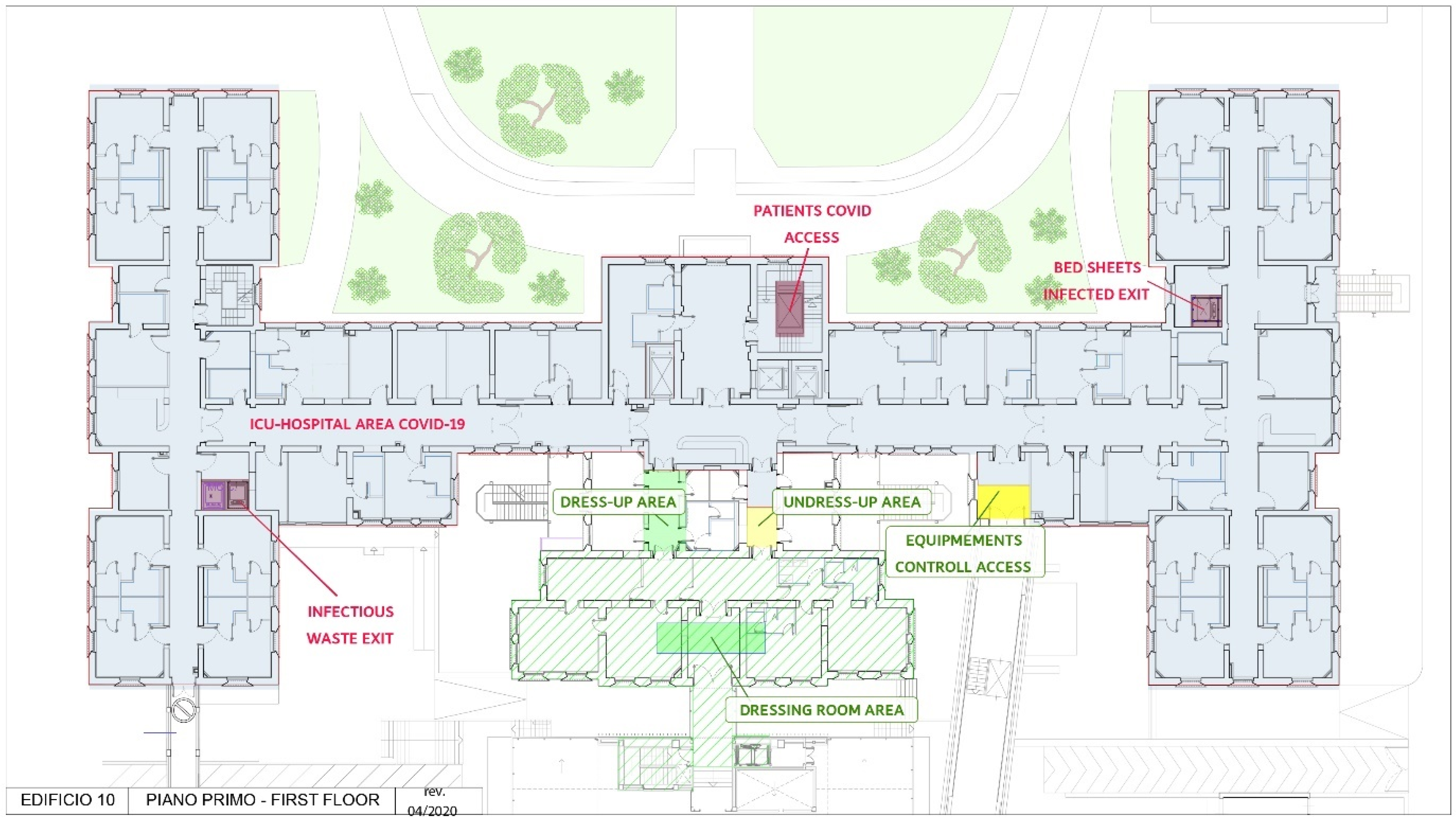
| Structural | Differentiated inbound and outbound routes from the COVID-19 area between personnel and materials. |
| Inbound and outbound filter areas. | |
| Refreshment area for staff. | |
| Implementation of shower in the changing room leaving the COVID-19 area. | |
| Negative pressure rooms/outpatient room to safely manage suspected patients. | |
| Triage point at the entrance of the hospital with thermoscanner. | |
| Personal and general protective equipment availability/hand sanitizer dispensers. | |
| Education | Hand hygiene. |
| Donning and doffing personal protective equipment. | |
| Education on differentiated inbound and outbound routes. | |
| Education on medical waste management, supplies and transport of biological samples. | |
| Theoretical and practical training for 23 nurses with no experience in critical nursing (2557 h). | |
| Experienced critical care nurse educators (2) assigned to the COVID-19 ICU. | |
| Policies and procedures | Infection control policies and procedures implementation. |
| Health surveillance | Evaluation by the occupational physician with the release of eligibility opinion for possible assignment to the COVID-19 ICU. |
| Serological tests, rapid or molecular antigenic swabs. | |
| Molecular swab every 14 days for dedicated COVID-19 staff. | |
| Molecular swab a week after completion of the service in the COVID-19 area. | |
| General | Modified working shifts. |
| Newly implemented work organizational briefing. | |
| General Data | Frequency | Percent | |
|---|---|---|---|
| Q1. Age. | 20–30 years | 27 | 17.65 |
| 31–40 years | 40 | 26.14 | |
| 41–50 years | 55 | 35.95 | |
| over 50 years | 31 | 20.26 | |
| Q2. Sex. | M | 86 | 56.21 |
| F | 67 | 43.79 | |
| Q3. Work/seniority in ICU settings. | <6 months | 40 | 26.14 |
| 6 months–1 year | 16 | 10.46 | |
| 1–3 years | 6 | 3.92 | |
| >3 years | 91 | 59.48 | |
| Q4. Professional role. | Nurse | 74 | 48.37 |
| Physician | 12 | 7.84 | |
| Physiotherapist | 11 | 7.19 | |
| Aide | 35 | 22.88 | |
| Radiology technician | 5 | 3.27 | |
| Housekeeping | 3 | 1.96 | |
| Other | 13 | 8.50 | |
| Q5. How long have you been working in the COVID-19 area? | <1 month | 42 | 27.45 |
| 1–3 months | 28 | 18.30 | |
| 3–6 months | 35 | 22.88 | |
| >6 months | 48 | 31.37 | |
| Clinical care tasks carried out on COVID-19 patients | |||
| Q6. Did you provide direct care to confirmed COVID-19 patients (e.g., CPR, intubation, extubation, circuit change, aerosol therapy, tracheotomy, bronchoscopy, patient hygiene, mobilization)? | Yes. | 98 | 67.12 |
| No. | 48 | 32.88 | |
| Q7. Did you have direct contact with the environment where confirmed COVID-19 patients were treated (e.g., bed, linen, medical equipment, restrooms, environmental hygiene)? | Yes. | 113 | 77.40 |
| No. | 33 | 22.60 | |
| Q8. During the activity in the COVID-19 area did you suffer any biological injury? | Yes, splashes of biological fluid/respiratory secretions in my mouth/nose mucosa. | 2 | 1.37 |
| Yes, splashes of biological fluid/respiratory secretions on intact skin. | 2 | 1.37 | |
| Yes, puncture/cut with material contaminated by biological fluid/respiratory secretions. | 0 | 0 | |
| No injury. | 142 | 97.26 | |
| Preventive measures implemented by the corporate organization | |||
| Q9. The organizational model adopted at ISMETT (e.g., dressing and undressing area, cafeteria, changing rooms and shower, training, health surveillance, in/out routes) made me feel safe while working in the COVID-19 ICU. | Strongly disagree | 0 | 0 |
| Disagree | 13 | 9.63 | |
| Irrelevant | 9 | 6.67 | |
| Agree | 58 | 42.96 | |
| Strongly agree | 55 | 40.74 | |
| Q10. Before entering the COVID-19 ICU, did you wear personal protection equipment (PPE) according to the corporate policies? | Yes. | 128 | 94.81 |
| I don’t think all PPEs are necessary. | 0 | 0 | |
| Not all PPEs are always available. | 4 | 2.96 | |
| Other (specify). | 3 | 2.22 | |
| Q11. Before and after contact with the patient or entering/leaving the room, did you disinfect the gloves with antiseptic gel? | Never | 2 | 1.48 |
| Sometimes | 0 | 0 | |
| Almost always | 6 | 4.44 | |
| Always | 127 | 94.07 | |
| Q12. Before and after contact with the surrounding environment (e.g., bed, door handle, infusion pump, ventilator, ECMO, monitor) of with a COVID-19 patient, did you disinfect the gloves with antiseptic gel? | Never | 3 | 2.22 |
| Sometimes | 1 | 0.74 | |
| Almost always | 12 | 8.89 | |
| Always | 119 | 88.15 | |
| Q13. The training and in-services (e.g., dressing/undressing, use of PPEs during shifts, work organization) made me confident to perform my tasks in the COVID-19 ICU. | Strongly disagree | 3 | 2.22 |
| Disagree | 10 | 7.41 | |
| Irrelevant | 7 | 5.19 | |
| Agree | 71 | 52.59 | |
| Strongly agree | 44 | 32.59 | |
| Q14. I received sufficient training/in-services on proper hand hygiene procedure. | Strongly disagree | 0 | 0 |
| Disagree | 3 | 2.22 | |
| Irrelevant | 6 | 4.44 | |
| Agree | 53 | 39.26 | |
| Strongly agree | 73 | 54.07 | |
| Q15. I received sufficient training on the correct sequence of COVID-19 dressing and undressing. | Strongly disagree | 2 | 1.48 |
| Disagree | 9 | 6.67 | |
| Irrelevant | 12 | 8.89 | |
| Agree | 65 | 48.15 | |
| Strongly agree | 47 | 34.81 | |
| Q16. The differentiated in/out pathways, both for staff and materials, made me feel safe while performing my tasks in the COVID-19 ICU. | Strongly disagree | 0 | 0 |
| Disagree | 4 | 2.96 | |
| Irrelevant | 7 | 5.19 | |
| Agree | 65 | 48.15 | |
| Strongly agree | 59 | 43.70 | |
| Q17. The health surveillance system made me feel safe during my work in the COVID-19 ICU. | Strongly disagree | 2 | 1.48 |
| Disagree | 11 | 8.15 | |
| Irrelevant | 10 | 7.41 | |
| Agree | 64 | 47.41 | |
| Strongly agree | 48 | 35.56 | |
| Q18. The areas provided for staff comfort and breaks made me feel safer working in the COVID-19 ICU. | Strongly disagree | 1 | 0.74 |
| Disagree | 8 | 5.93 | |
| Irrelevant | 17 | 12.59 | |
| Agree | 60 | 44.44 | |
| Strongly agree | 49 | 36.30 | |
| Q19. I believe taking a shower outside the COVID-19 area is an additional safety tool for health care providers. | Strongly disagree | 0 | 0 |
| Disagree | 1 | 0.74 | |
| Irrelevant | 7 | 5.19 | |
| Agree | 41 | 30.37 | |
| Strongly agree | 86 | 63.70 | |
| Staff risk perception | |||
| Q20. Composition of your family. | I live alone. | 19 | 14.29 |
| I live with children younger than 18 years of age. | 50 | 37.59 | |
| I live with people at greater COVID-19 risk (e.g., elderly, fragile). | 26 | 19.55 | |
| I live with people not included in the categories at risk. | 38 | 28.57 | |
| Q21. I’m afraid to transmit COVID-19 to my family or loved ones when I return home from work in the COVID-19 area. | Strongly disagree | 7 | 5.26 |
| Disagree | 11 | 8.27 | |
| Irrelevant | 10 | 7.52 | |
| Agree | 67 | 50.38 | |
| Strongly agree | 38 | 28.57 | |
| Q22. I consider myself among those at higher risk of contracting COVID-19 infection due to my activity in the COVID-19 ICU. | Strongly disagree | 15 | 11.28 |
| Disagree | 27 | 20.30 | |
| Irrelevant | 22 | 16.54 | |
| Agree | 50 | 37.59 | |
| Strongly agree | 19 | 14.29 | |
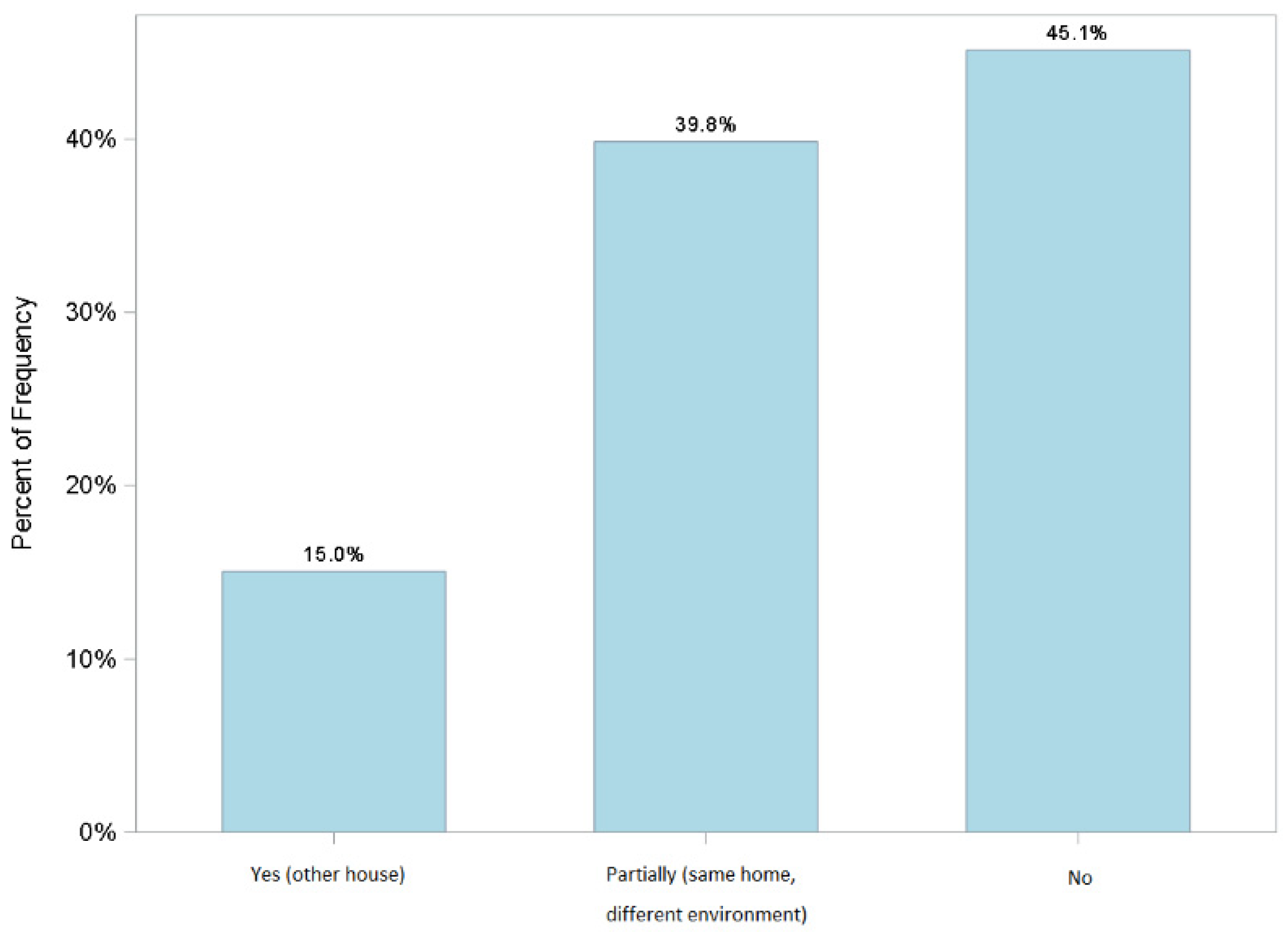
| Q23. In the first few days after your access to the COVID-19 area, did you take isolation measures upon returning home to protect your family? | Yes (another house). | 20 | 15.04 |
| Partially (same home, different environment). | 53 | 39.85 | |
| No. | 60 | 45.11 | |
| Q24. Did you return to your normal daily habits after a few days? | Yes | 55 | 75.34 |
| No | 18 | 24.66 | |
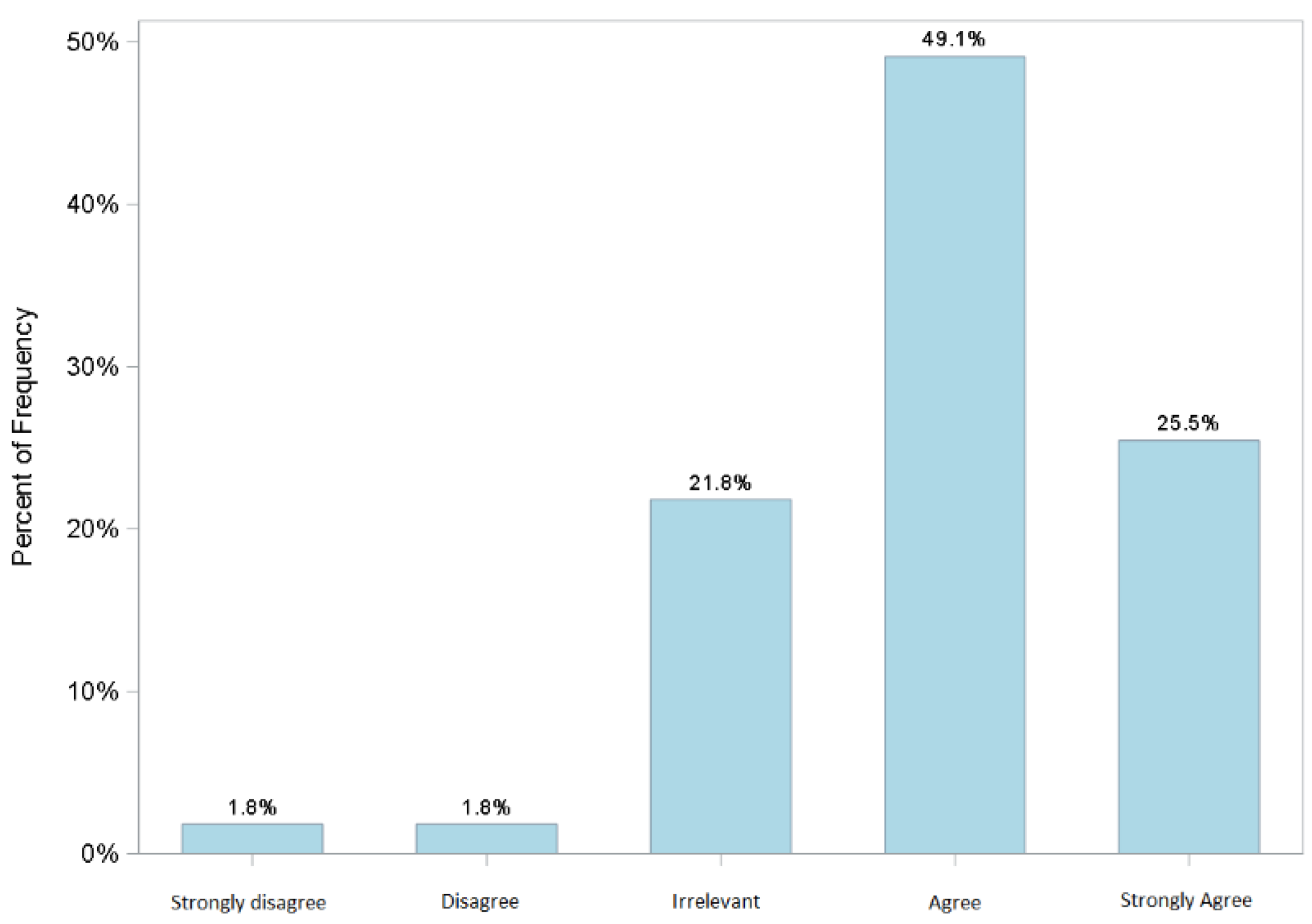
| Q25. I returned to normal daily habits because I felt sufficiently reassured by the implementation of the corporate organizational model. | Strongly disagree | 1 | 1.82 |
| Disagree | 1 | 1.82 | |
| Irrelevant | 12 | 21.82 | |
| Agree | 27 | 49.09 | |
| Strongly agree | 14 | 25.45 | |
| Q26. I think COVID-19 is a dangerous and deadly disease. | Strongly disagree | 0 | 0 |
| Disagree | 4 | 3.01 | |
| Irrelevant | 3 | 2.26 | |
| Agree | 61 | 45.86 | |
| Strongly agree | 65 | 48.87 | |
| Q27. COVID-19 changed my daily life habits (physical distancing, frequency of family meetings, social contacts). | Strongly disagree | 2 | 1.50 |
| Disagree | 3 | 2.26 | |
| Irrelevant | 3 | 2.26 | |
| Agree | 57 | 42.86 | |
| Strongly agree | 68 | 51.13 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conoscenti, E.; Campanella, M.; Sala, A.; Di Stefano, M.C.; Vinci, D.; Lombardo, R.; Arena, G.; Ginestra, A.; Fiolo, R.; Tuzzolino, F.; et al. Impact of the Organizational Model Adopted during the COVID-19 Pandemic on the Perceived Safety of Intensive Care Unit Staff. J. Clin. Med. 2022, 11, 1487. https://doi.org/10.3390/jcm11061487
Conoscenti E, Campanella M, Sala A, Di Stefano MC, Vinci D, Lombardo R, Arena G, Ginestra A, Fiolo R, Tuzzolino F, et al. Impact of the Organizational Model Adopted during the COVID-19 Pandemic on the Perceived Safety of Intensive Care Unit Staff. Journal of Clinical Medicine. 2022; 11(6):1487. https://doi.org/10.3390/jcm11061487
Chicago/Turabian StyleConoscenti, Elena, Maria Campanella, Antonino Sala, Maria Cristina Di Stefano, Dario Vinci, Rosario Lombardo, Giuseppe Arena, Angelo Ginestra, Rosario Fiolo, Fabio Tuzzolino, and et al. 2022. "Impact of the Organizational Model Adopted during the COVID-19 Pandemic on the Perceived Safety of Intensive Care Unit Staff" Journal of Clinical Medicine 11, no. 6: 1487. https://doi.org/10.3390/jcm11061487