
Decision Conflicts in Clinical Care during COVID-19: A Patient Perspective

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Development
2.2. Sample
2.3. Variables
2.4. Data Analysis
3. Results
3.1. Questionnaire Response
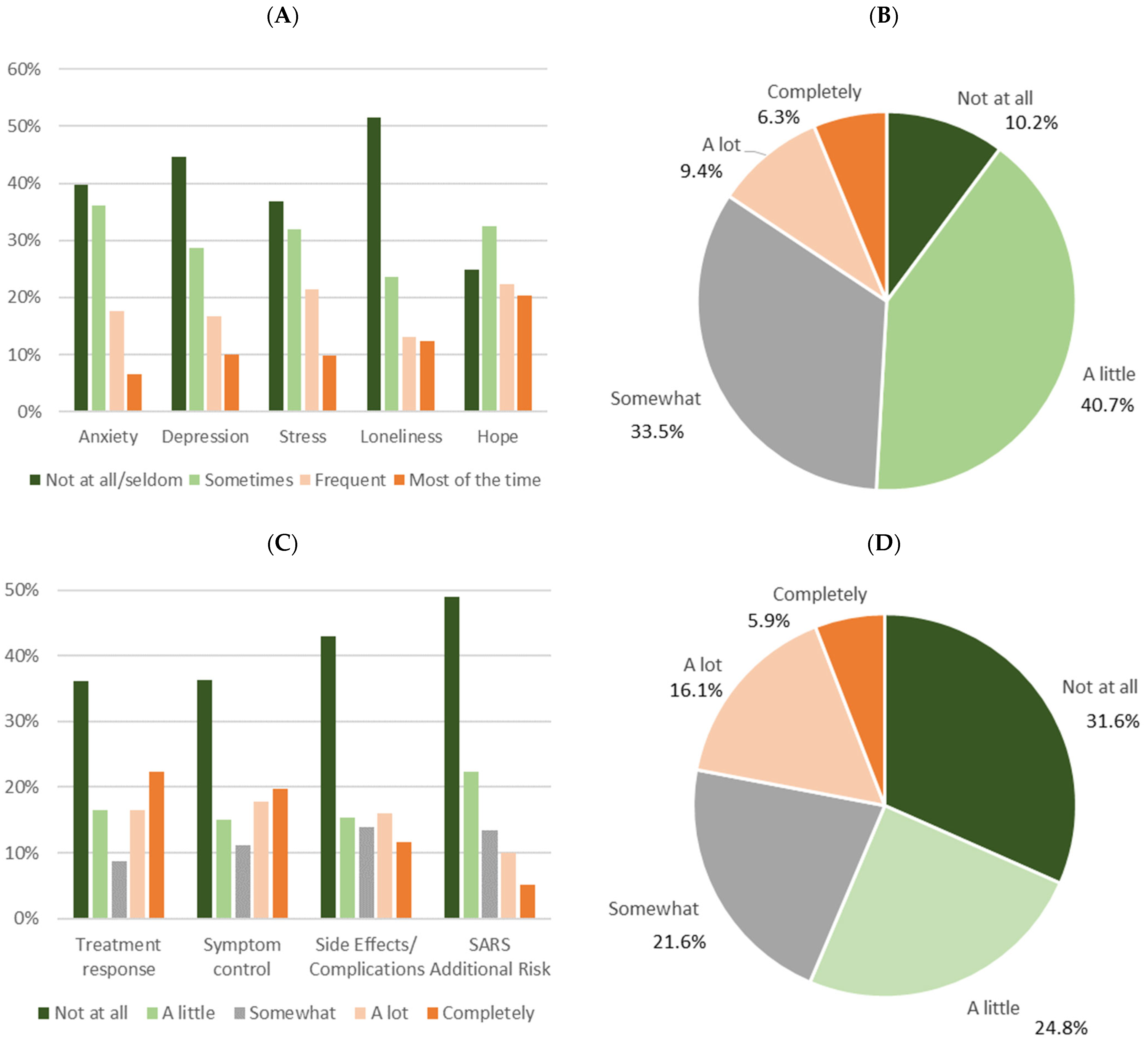
3.2. Decisional Uncertainty and Resulting Decisional Distress
3.3. Consequences of Decisional Uncertainty and Conflicts
3.4. Reasons and Vulnerability
4. Discussion
5. Conclusions
- Assessing the level of uncertainty and decisional burden in patients, especially additional effects of the pandemic;
- Considering potential modifications of decisional criteria in patients due to pandemic issues;
- Communicating one’s own decisional uncertainty with patients to ensure shared decision making;
- Organizing sufficient information management, especially when evidence deficits occur;
- Supporting specific groups of vulnerable patients in handling pandemic-related additional burden.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ho, A.; Huang, V. Unmasking the Ethics of Public Health Messaging in a Pandemic. J. Bioethical Inq. 2021, 18, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Romdhani, M.; Kohler, S.; Koskas, P.; Drunat, O. Ethical dilemma for healthcare professionals facing elderly dementia patients during the COVID-19 pandemic. L’encephale, 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Haier, J.; Beller, J.; Adorjan, K.; Bleich, S.; de Greck, M.; Griesinger, F.; Hein, A.; Hurlemann, R.; Mees, S.T.; Philipsen, A.; et al. Decision Conflicts in Oncological Care during COVID-19: A Multi-Perspective Inquiry. PLoS ONE, 2022; Under Review. [Google Scholar]
- Dhada, S.; Stewart, D.; Cheema, E.; Hadi, M.A.; Paudyal, V. Cancer Services during the COVID-19 Pandemic: Systematic Review of Patient’s and Caregiver’s Experiences. Cancer Manag. Res. 2021, 13, 5875–5887. [Google Scholar] [CrossRef] [PubMed]
- Ludwigson, A.; Huynh, V.; Myers, S.; Hampanda, K.; Christian, N.; Ahrendt, G.; Romandetti, K.; Tevis, S. Patient Perceptions of Changes in Breast Cancer Care and Well-Being during COVID-19: A Mixed Methods Study. Ann. Surg. Oncol. 2022, 29, 1649–1657. [Google Scholar] [CrossRef]
- Ivanyi, P.; Park-Simon, T.; Christiansen, H.; Gutzmer, R.; Vogel, A.; Heuser, M.; Golpon, H.; Hillemanns, P.; Haier, J. Protective measures for patients with advanced cancer during the SARS-CoV-2 pandemic: Quo vadis? Clin. Exp. Metastasis 2021, 38, 257–261. [Google Scholar] [CrossRef]
- Wamkpah, N.S.; Gerndt, S.P.; Kallogjeri, D.; Piccirillo, J.F.; Chi, J.J. Patients’ Views of Shared Decision-making and Decisional Conflict in Otolaryngologic Surgery during the COVID-19 Pandemic. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 879. [Google Scholar] [CrossRef]
- Al-Quteimat, O.M.; Amer, A.M. The Impact of the COVID-19 Pandemic on Cancer Patients. Am. J. Clin. Oncol. 2020, 43, 452–455. [Google Scholar] [CrossRef]
- Rashid, S.; Reeder, C.; Sahu, S.; Rashid, S. Psychological distress and moral injury to oncologists and their patients during COVID-19 pandemic. Curr. Psychol. 2021, 1–6. [Google Scholar] [CrossRef]
- Ruiz-Hornillos, J.; Suárez, P.H.; Martínez, J.M.M.; Beriain, D.M.; Vázquez, M.A.N.; Albert, M.; Abián, M.H.; Pacheco-Martínez, P.A.; Trasmontes, V.; Guillén-Navarro, E. Bioethical Concerns during the COVID-19 Pandemic: What Did Healthcare Ethics Committees and Institutions State in Spain? Front. Public Health 2021, 9, 737755. [Google Scholar] [CrossRef]
- Köther, A.K.; Siebenhaar, K.U.; Alpers, G.W. Shared Decision Making during the COVID-19 Pandemic. Med. Decis. Mak. 2021, 41, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Campi, R.; Tellini, R.; Grosso, A.A.; Amparore, D.; Mari, A.; Viola, L.; Cocci, A.; Polverino, P.; Checcucci, E.; Alessio, P.; et al. Deferring Elective Urologic Surgery during the COVID-19 Pandemic: The Patients’ Perspective. Urology 2021, 147, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Edge, R.; Mazariego, C.; Li, Z.; Canfell, K.; Miller, A.; Koczwara, B.; Shaw, J.; Taylor, N. Psychosocial impact of COVID-19 on cancer patients, survivors, and carers in Australia: A real-time assessment of cancer support services. Support. Care Cancer 2021, 29, 5463–5473. [Google Scholar] [CrossRef]
- Butow, P.; Havard, P.; Butt, Z.; Juraskova, L.; Sharpe, L.; Dhillon, H.; Beatty, L.; Beale, P.; Cigolini, M.; Kelly, B.; et al. The impact of COVID-19 on cancer patients, their carers and oncology health professionals: A qualitative study. Patient Educ. Couns. 2022. [Google Scholar] [CrossRef] [PubMed]
- Savard, J.; Jobin-Théberge, A.; Massicotte, V.; Banville, C. How did women with breast cancer experience the first wave of the COVID-19 pandemic? A qualitative study. Support. Care Cancer 2021, 29, 5721–5727. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Kilgour, H.M.; Haase, K.R. The Psychosocial Impact of COVID-19 on Older Adults with Cancer: A Rapid Review. Curr. Oncol. 2022, 29, 53. [Google Scholar] [CrossRef]
- Takeuchi, E.; Katanoda, K.; Cheli, S.; Goldzweig, G.; Tabuchi, T. Restrictions on healthcare utilization and psychological distress among patients with diseases potentially vulnerable to COVID-19; the JACSIS 2020 study. Health Psychol. Behav. Med. 2022, 10, 229–240. [Google Scholar] [CrossRef]
- Borsari, S.; Pampena, R.; Benati, M.; Raucci, M.; Mirra, M.; Lai, M.; Lombardi, M.; Pellacani, G.; Longo, C. Self-reported measure of subjective distress in response to COVID-19 pandemic in patients referred to our skin cancer unit during the first wave. Clin. Dermatol. 2022, 40, 93–99. [Google Scholar] [CrossRef]
- Beller, J.; Schäfers, J.; Geyer, S.; Haier, J.; Epping, J. Patterns of Changes in Oncological Care due to COVID-19: Results of a Survey of Oncological Nurses and Physicians from the Region of Hanover, Germany. Healthcare 2021, 10, 15. [Google Scholar] [CrossRef]
- Klaassen, Z.; Wallis, C.J. Assessing patient risk from cancer and COVID-19: Managing patient distress. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 243–246. [Google Scholar] [CrossRef]
- Koinig, K.A.; Arnold, C.; Lehmann, J.; Giesinger, J.; Köck, S.; Willenbacher, W.; Weger, R.; Holzner, B.; Ganswindt, U.; Wolf, D.; et al. The cancer patient’s perspective of COVID-19-induced distress—A cross-sectional study and a longitudinal comparison of HRQOL assessed before and during the pandemic. Cancer Med. 2021, 10, 3928–3937. [Google Scholar] [CrossRef] [PubMed]
- Hulbert-Williams, N.J.; Leslie, M.; Hulbert-Williams, L.; Smith, E.; Howells, L.; Pinato, D.J. Evaluating the impact of COVID-19 on supportive care needs, psychological distress and quality of life in UK cancer survivors and their support network. Eur. J. Cancer Care 2021, 30, e13442. [Google Scholar] [CrossRef] [PubMed]
- Lou, E.; Teoh, D.; Brown, K.; Blaes, A.; Holtan, S.G.; Jewett, P.; Parsons, H.; Mburu, E.W.; Thomaier, L.; Hui, J.Y.C.; et al. Perspectives of cancer patients and their health during the COVID-19 pandemic. PLoS ONE 2020, 15, e0241741. [Google Scholar] [CrossRef] [PubMed]
- Forner, D.; Murnaghan, S.; Porter, G.; Mason, R.; Hong, P.; Taylor, S.; Bentley, J.; Hirsch, G.; Noel, C.; Rigby, M.; et al. Psychosocial Distress in Adult Patients Awaiting Cancer Surgery during the COVID-19 Pandemic. Curr. Oncol. 2021, 28, 173. [Google Scholar] [CrossRef]
- Bäuerle, A.; Musche, V.; Schmidt, K.; Schweda, A.; Fink, M.; Weismüller, B.; Kohler, H.; Herrmann, K.; Tewes, M.; Schadendorf, D.; et al. Mental Health Burden of German Cancer Patients before and after the Outbreak of COVID-19: Predictors of Mental Health Impairment. Int. J. Environ. Res. Public Health 2021, 18, 2318. [Google Scholar] [CrossRef]
- Cona, M.S.; Rulli, E.; Dalu, D.; Galli, F.; Rota, S.; Ferrario, S.; Tosca, N.; Gambaro, A.; Filipazzi, V.; Piva, S.; et al. The emotional impact of the COVID-19 outbreak on cancer outpatients and their caregivers: Results of a survey conducted in the midst of the Italian pandemic. Support. Care Cancer 2022, 30, 1115–1125. [Google Scholar] [CrossRef]
- Gultekin, M.; Ak, S.; Ayhan, A.; Strojna, A.; Pletnev, A.; Fagotti, A.; Perrone, A.M.; Erzeneoglu, B.E.; Temiz, B.E.; Lemley, B.; et al. Perspectives, fears and expectations of patients with gynaecological cancers during the COVID-19 pandemic: A Pan-European study of the European Network of Gynaecological Cancer Advocacy Groups (ENGAGe). Cancer Med. 2021, 10, 208–219. [Google Scholar] [CrossRef]
- Wang, Y.; Duan, Z.; Ma, Z.; Mao, Y.; Li, X.; Wilson, A.; Qin, H.; Ou, J.; Peng, K.; Zhou, F.; et al. Epidemiology of mental health problems among patients with cancer during COVID-19 pandemic. Transl. Psychiatry 2020, 10, 263. [Google Scholar] [CrossRef]
- Dieperink, K.B.; Ikander, T.; Appiah, S.; Tolstrup, L.K. The cost of living with cancer during the second wave of COVID-19: A mixed methods study of Danish cancer patients’ perspectives. Eur. J. Oncol. Nurs. 2021, 52, 101958. [Google Scholar] [CrossRef]
- Toquero, P.; Fernández, C.B.; Martí, M.P.L.; Marín, B.H.; Cea, E.B.V.; García, A.G.; Carrascosa, E.M.; Torres, D.B.; Candil, O.D.; Sánchez-Torres, J.M.; et al. Emotional Distress in Cancer Patients during the First Wave of the COVID-19 Pandemic. Front. Psychol. 2021, 12, 755965. [Google Scholar] [CrossRef]
- Zomerdijk, N.; Jongenelis, M.; Short, C.E.; Smith, A.; Turner, J.; Huntley, K. Prevalence and correlates of psychological distress, unmet supportive care needs, and fear of cancer recurrence among haematological cancer patients during the COVID-19 pandemic. Support. Care Cancer 2021, 29, 7755–7764. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Feraca, M.; Nemesure, B. An Assessment of Distress Levels of Patients Undergoing Lung Cancer Treatment and Surveillance during the COVID-19 Pandemic. J. Nurse Pract. 2021, 17, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Turgeman, I.; Goshen-Lago, T.; Waldhorn, I.; Karov, K.; Groisman, L.; Benaim, A.R.; Almog, R.; Halberthal, M.; Ben-Aharon, I. Psychosocial perspectives among cancer patients during the coronavirus disease 2019 (COVID-19) crisis: An observational longitudinal study. Cancer Rep. 2021, 5, e1506. [Google Scholar] [CrossRef] [PubMed]
- Budisavljevic, A.; Kelemenic-Drazin, R.; Dedic Plavetic, N.; Kardum Fucak, I.; Silovski, T.; Telesmanic Dobric, V.; Nalbani, M.; Curic, Z.; Boric-Mikez, Z.; Ladenhauser, T.; et al. The First Wave of the COVID-19 Pandemic and Its Impact on the Level of Distress in Patients with Breast Cancer, a Multicentric Study. Psychiatry Danub. 2021, 33 (Suppl. 13), 341–349. [Google Scholar]
- Romito, F.; Dellino, M.; Loseto, G.; Opinto, G.; Silvestris, E.; Cormio, C.; Guarini, A.; Minoia, C. Psychological Distress in Outpatients With Lymphoma during the COVID-19 Pandemic. Front. Oncol. 2020, 10, 1270. [Google Scholar] [CrossRef] [PubMed]
- Bartmann, C.; Fischer, L.-M.; Hübner, T.; Müller-Reiter, M.; Wöckel, A.; McNeill, R.V.; Schlaiss, T.; Kittel-Schneider, S.; Kämmerer, U.; Diessner, J. The effects of the COVID-19 pandemic on psychological stress in breast cancer patients. BMC Cancer 2021, 21, 1356. [Google Scholar] [CrossRef] [PubMed]
- Kinghorn, A.; Mercer, S.; Yasin, T.; John, A.; Trickett, R. Is it safe yet? Patient readiness and perceptions about returning to hospital for planned orthopaedic care. Ann. R. Coll. Surg. Engl. 2021, 103, 332–336. [Google Scholar] [CrossRef]
- Logishetty, K.; Edwards, T.C.; Ponniah, H.S.; Ahmed, M.; Liddle, A.D.; Cobb, J.; Clark, C. How to prioritize patients and redesign care to safely resume planned surgery during the COVID-19 pandemic. Bone Jt. Open 2021, 2, 134–140. [Google Scholar] [CrossRef]
- Momenimovahed, Z.; Salehiniya, H.; Hadavandsiri, F.; Allahqoli, L.; Günther, V.; Alkatout, I. Psychological Distress Among Cancer Patients during COVID-19 Pandemic in the World: A Systematic Review. Front. Psychol. 2021, 12, 682154. [Google Scholar] [CrossRef]
- Musche, V.; Bäuerle, A.; Steinbach, J.; Schweda, A.; Hetkamp, M.; Weismüller, B.; Kohler, H.; Beckmann, M.; Herrmann, K.; Tewes, M.; et al. COVID-19-Related Fear and Health-Related Safety Behavior in Oncological Patients. Front. Psychol. 2020, 11, 1984. [Google Scholar] [CrossRef]
- Eckford, R.D.; Gaisser, A.; Arndt, V.; Baumann, M.; Kludt, E.; Mehlis, K.; Ubels, J.; Winkler, E.C.; Weg-Remers, S.; Schlander, M. The COVID-19 Pandemic and Cancer Patients in Germany: Impact on Treatment, Follow-Up Care and Psychological Burden. Front. Public Health 2022, 9, 788598. [Google Scholar] [CrossRef] [PubMed]
- Ballatore, Z.; Merloni, F.; Ranallo, N.; Bastianelli, L.; Vitarelli, F.; Cantini, L.; Ricci, G.; Ferretti, B.; Alessandroni, P.; Del Prete, M.; et al. Cancer patient perspective in the arena of COVID-19 pandemic. Psycho-Oncology 2021, 31, 39–45. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| (A) | |||||||
|---|---|---|---|---|---|---|---|
| Effect | −2 Log Likelihood for Reduced Model | Likelihood-Quotient Tests | |||||
| Chi² | dF | Significance | |||||
| Constant Term | 521.434 | 0.000 | 0 | ||||
| Decision Criteria SARS Additional Risk | 597.452 | 76.018 | 16 | 0.000 | |||
| Burden Infection Risk | 609.148 | 87.714 | 16 | 0.000 | |||
| Information Availability Own Provider | 592.611 | 71.178 | 16 | 0.000 | |||
| Education Level | 576.464 | 55.030 | 12 | 0.000 | |||
| Speciality Group | 586.717 | 65.283 | 4 | 0.000 | |||
| Distance Regulations | 582.071 | 60.638 | 16 | 0.000 | |||
| Decision Criteria Side Effects/Complications | 690.702 | 169.268 | 16 | 0.000 | |||
| Decision Criteria Treatment Response | 600.345 | 78.912 | 16 | 0.000 | |||
| Pandemic Own Risk | 570.796 | 49.363 | 16 | 0.000 | |||
| (B) | |||||||
| Observed | Predicted | ||||||
| Not at All | A Little | Somewhat | A Lot | Completely | % Correct | % Correct with Neighbor | |
| Not at all | 124 | 14 | 7 | 3 | 0 | 83.8% | 93.2% |
| A little | 31 | 27 | 5 | 7 | 0 | 38.6% | 90.0% |
| Somewhat | 11 | 6 | 19 | 5 | 0 | 46.3% | 73.2% |
| A lot | 13 | 6 | 5 | 22 | 0 | 47.8% | 58.7% |
| Completely | 0 | 0 | 0 | 0 | 16 | 100.0% | 100.0% |
| % Total | 55.8% | 16.5% | 11.2% | 11.5% | 5.0% | 64.8% | 85.4% |
| (A) | |||||||
|---|---|---|---|---|---|---|---|
| Effect | −2 Log Likelihood for Reduced Model | Likelihood-Quotient Tests | |||||
| Chi2 | dF | Significance | |||||
| Constant Term | 547.700 | 0.000 | 0 | ||||
| Information Availability Own Provider | 575.446 | 27.746 | 16 | 0.034 | |||
| Own Decisions | 588.645 | 40.945 | 16 | 0.001 | |||
| Decision Criteria Side Effects/Complications | 585.116 | 37.416 | 16 | 0.002 | |||
| Decision Criteria SARS Additional Risk | 571.083 | 23.383 | 16 | 0.104 | |||
| Burden Infection Risk | 596.564 | 48.864 | 16 | 0.000 | |||
| Decision Criteria Treatment Response | 581.926 | 34.226 | 16 | 0.005 | |||
| Pandemic Own Risk | 580.960 | 33.260 | 16 | 0.007 | |||
| Disease Stage | 582.082 | 34.382 | 16 | 0.005 | |||
| Age Groups | 579.589 | 31.889 | 8 | 0.000 | |||
| Education Level | 575.793 | 28.093 | 12 | 0.005 | |||
| Speciality Group | 555.719 | 8.019 | 4 | 0.091 | |||
| (B) | |||||||
| Observed | Predicted | ||||||
| NOT at All | A Little | Somewhat | A Lot | Completely | % Correct | % Correct with Neighbor | |
| Not at all | 88 | 14 | 6 | 3 | 1 | 78.6% | 91.1% |
| A little | 25 | 35 | 8 | 4 | 1 | 47.9% | 93.2% |
| Somewhat | 8 | 13 | 29 | 2 | 3 | 52.7% | 80.0% |
| A lot | 6 | 9 | 4 | 22 | 0 | 53.7% | 63.4% |
| Completely | 1 | 1 | 1 | 0 | 27 | 90.0% | 90.0% |
| % Total | 41.2% | 23.2% | 15.4% | 10.0% | 10.3% | 64.6% | 85.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haier, J.; Beller, J.; Adorjan, K.; Bleich, S.; De Greck, M.; Griesinger, F.; Hein, A.; Hurlemann, R.; Mees, S.T.; Philipsen, A.; et al. Decision Conflicts in Clinical Care during COVID-19: A Patient Perspective. Healthcare 2022, 10, 1019. https://doi.org/10.3390/healthcare10061019
Haier J, Beller J, Adorjan K, Bleich S, De Greck M, Griesinger F, Hein A, Hurlemann R, Mees ST, Philipsen A, et al. Decision Conflicts in Clinical Care during COVID-19: A Patient Perspective. Healthcare. 2022; 10(6):1019. https://doi.org/10.3390/healthcare10061019
Chicago/Turabian StyleHaier, Jörg, Johannes Beller, Kristina Adorjan, Stefan Bleich, Moritz De Greck, Frank Griesinger, Alexander Hein, René Hurlemann, Sören Torge Mees, Alexandra Philipsen, and et al. 2022. "Decision Conflicts in Clinical Care during COVID-19: A Patient Perspective" Healthcare 10, no. 6: 1019. https://doi.org/10.3390/healthcare10061019