
Oxidative Stress and Inflammatory Biomarkers for the Prediction of Severity and ICU Admission in Unselected Patients Hospitalized with COVID-19

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics of the Studied Population
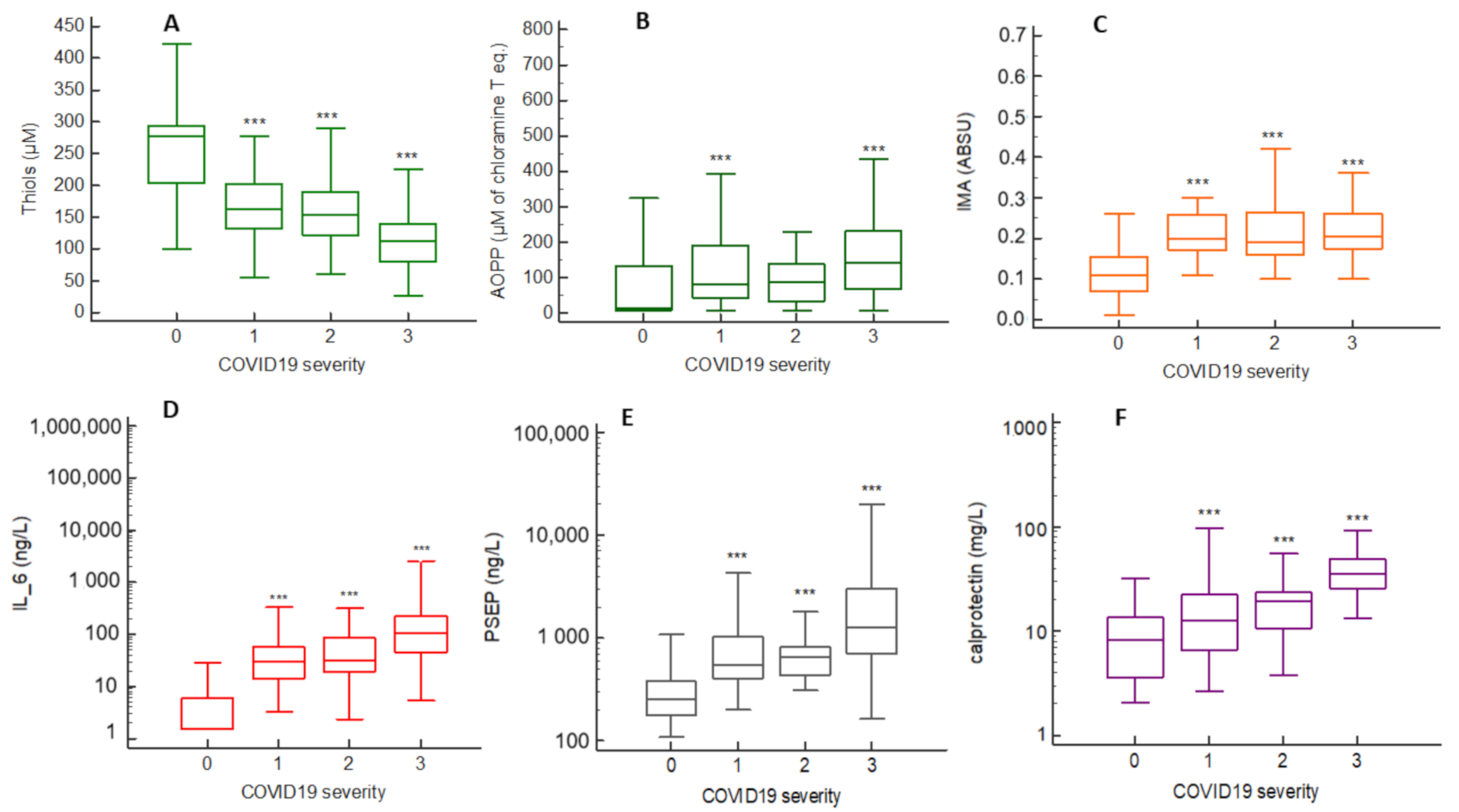
2.2. Oxidative Stress (OS), Inflammation and Cell-Activation Biomarkers Concentrations across COVID-19 Severity Stages
2.3. Correlations between Biomarkers
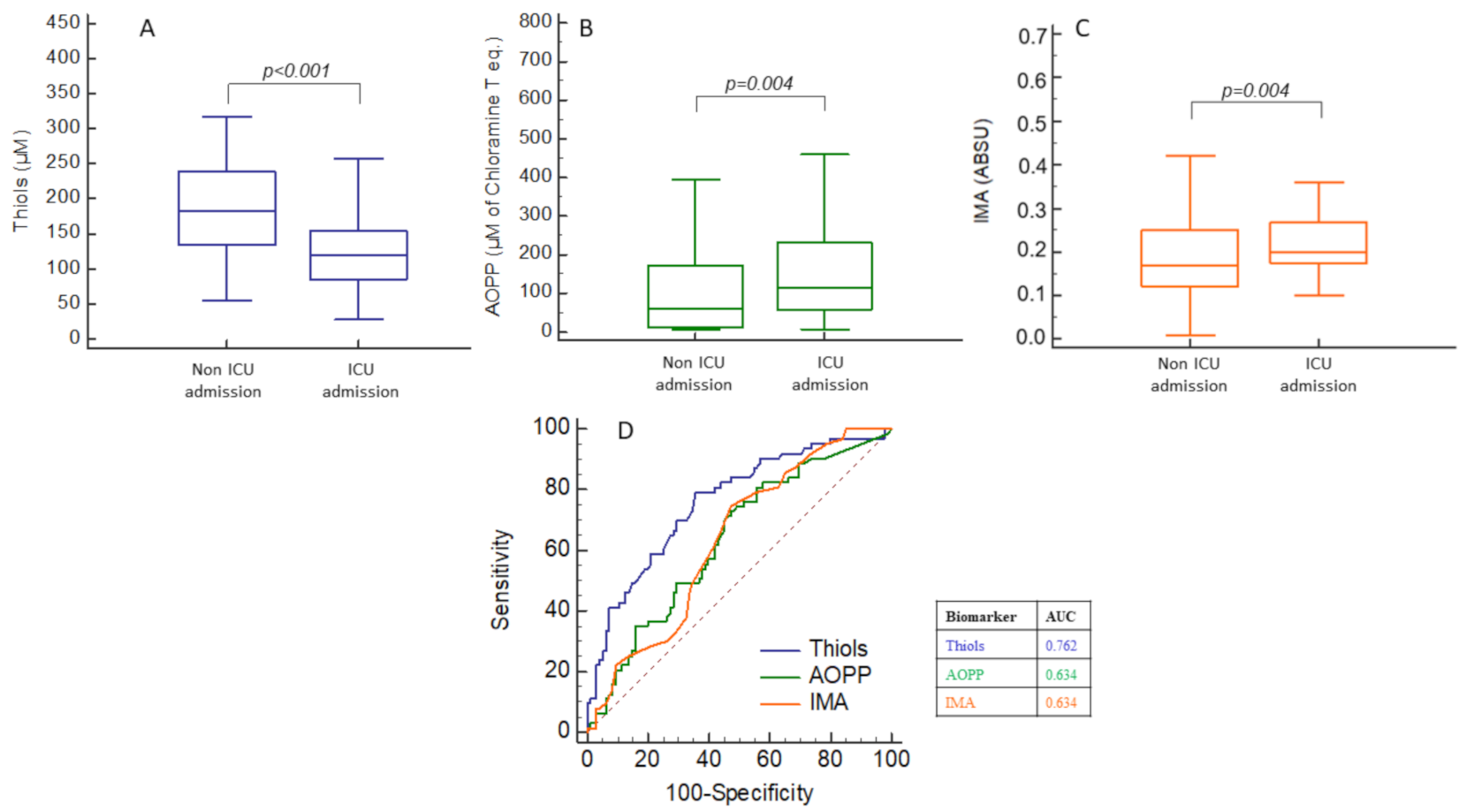
2.4. Oxidative Stress (OS), Inflammation and Cell-Activation Biomarkers Concentrations According to Increased O2 Needs
2.5. Prognostic Performances of OS, Inflammation and Cell-Activation Biomarkers for ICU Admission
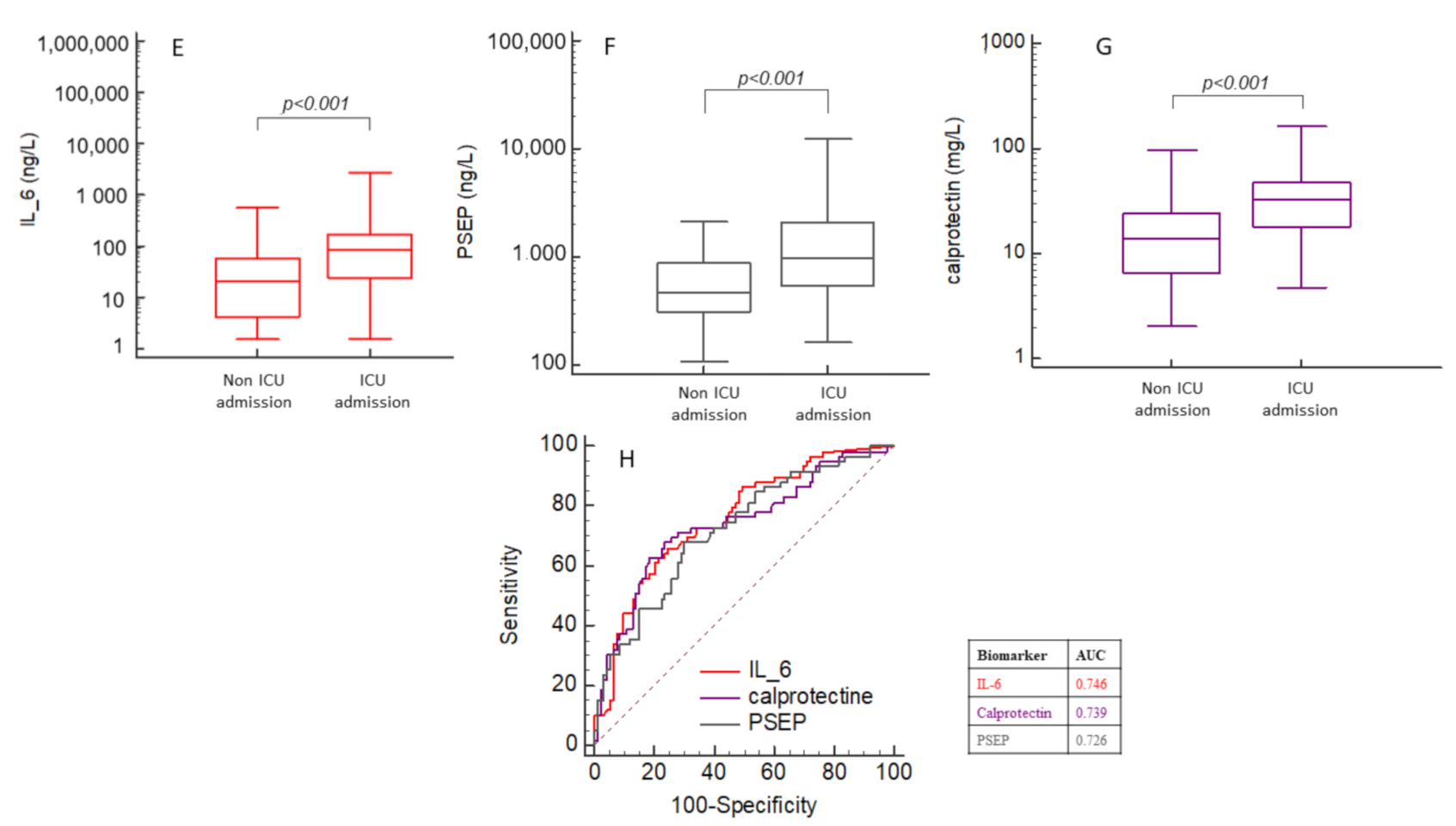
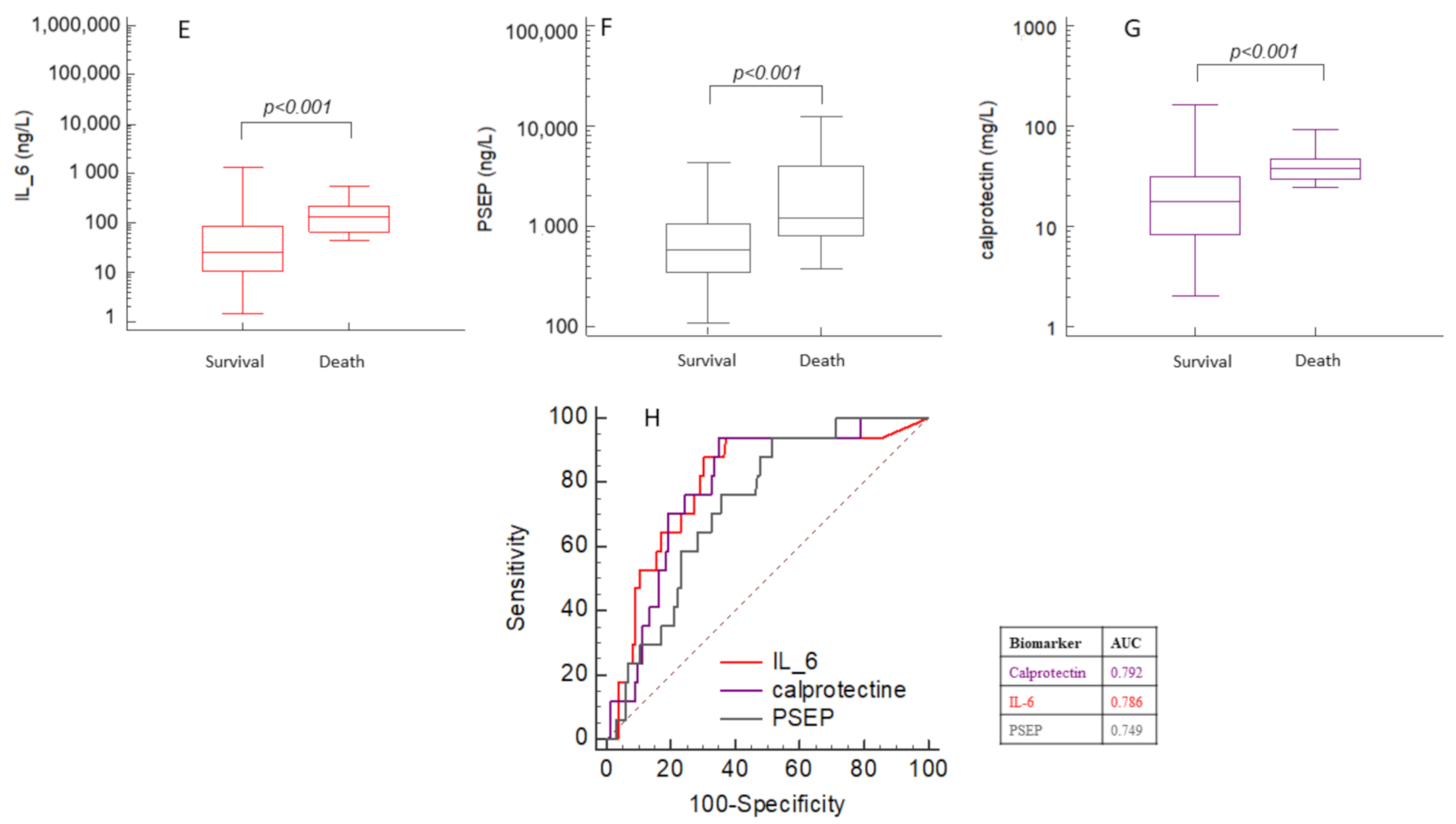
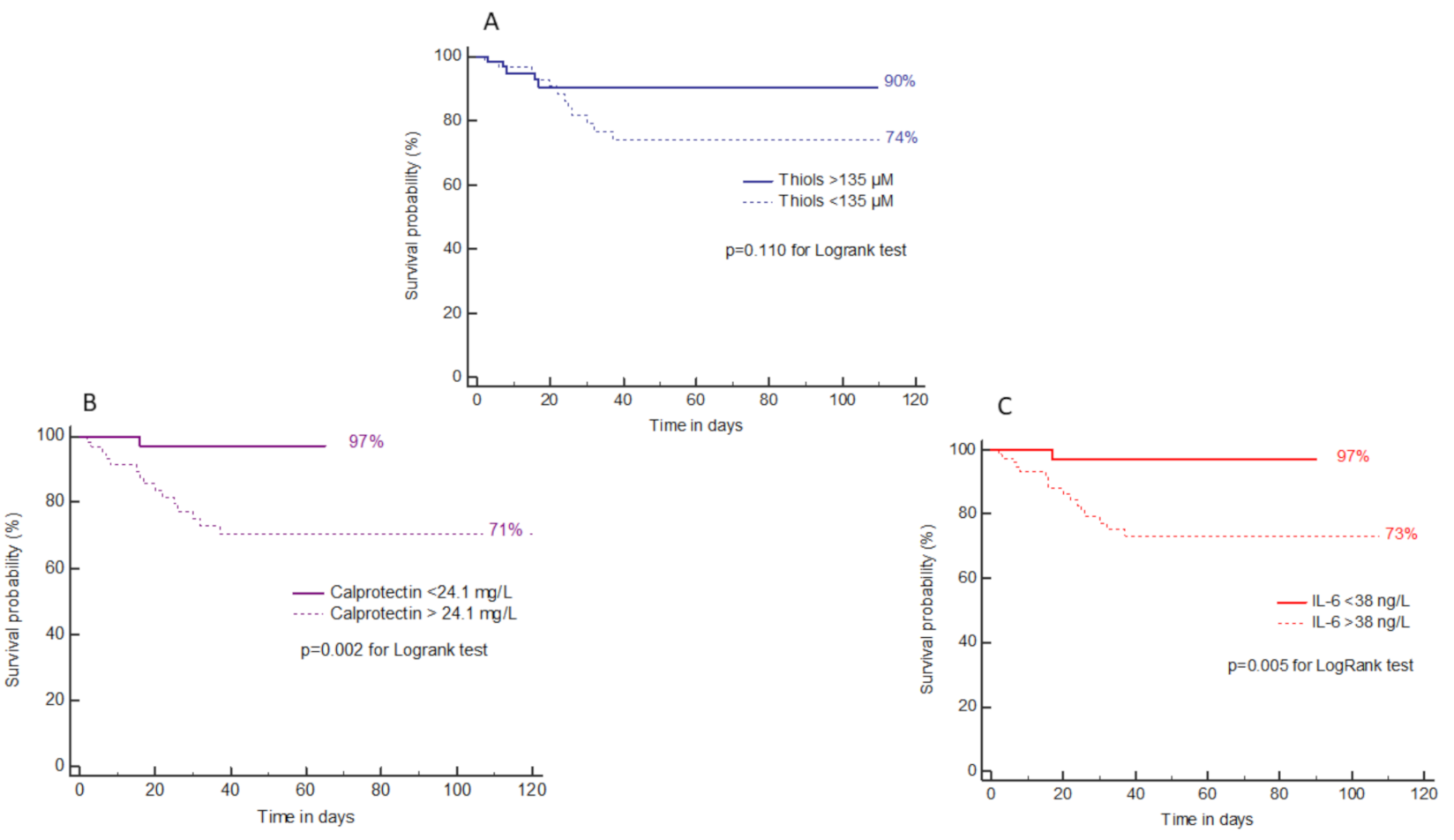
2.6. Prognostic Performances of OS, Inflammation and Cell-Activation Biomarkers for Death
3. Discussion
4. Limitations
5. Material and Methods
5.1. Population
5.2. Biomarkers Measurements
5.3. Statistical Analysis
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus Disease (COVID-19) Pandemic. Numbers at a Glance. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 26 March 2021).
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological Findings of COVID-19 Associated with Acute Respiratory Distress Syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Sies, H. Oxidative Stress: A Concept in Redox Biology and Medicine. Redox Biol. 2015, 4, 180–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derouiche, S. Oxidative Stress Associated with SARS-Cov-2 (COVID-19) Increases the Severity of the Lung Disease—A Systematic Review. J. Infect. Dis. Epidemiol. 2020, 6, 121–126. [Google Scholar]
- Cecchini, R.; Lourenço Cecchini, A. SARS-CoV-2 Infection Pathogenesis Is Related to Oxidative Stress as a Response to Aggression. Med. Hypotheses 2020, 143, 110102. [Google Scholar] [CrossRef]
- Komaravelli, N.; Casola, A. Respiratory Viral Infections and Subversion of Cellular Anti-oxidant Defenses. J. Pharm. Pharm. 2014, 5, 1000141. [Google Scholar]
- Laforge, M.; Elbim, C.; Frère, C.; Hemadi, M.; Massaad, C.; Nuss, P.; Benoliel, J.-J.; Becker, C. Tissue Damage from Neutrophil-Induced Oxidative Stress in COVID-19. Nat. Rev. Immunol. 2020, 20, 515–516. [Google Scholar] [CrossRef]
- Schönrich, G.; Raftery, M.J.; Samstag, Y. Devilishly Radical NETwork in COVID-19: Oxidative Stress, Neutrophil Extracellular Traps (NETs), and T Cell Suppression. Adv. Biol. Regul. 2020, 77, 100741. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Roche, L.; Mesta, F. Oxidative Stress as Key Player in Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Infection. Arch. Med. Res. 2020, 51, 384–387. [Google Scholar] [CrossRef]
- Chernyak, B.V.; Popova, E.N.; Prikhodko, A.S.; Grebenchikov, O.A.; Zinovkina, L.A.; Zinovkin, R.A.; Chernyak, B.V.; Popova, E.N.; Prikhodko, A.S.; Grebenchikov, O.A.; et al. COVID-19 and Oxidative Stress. Biochemistry 2020, 85, 1543–1553. [Google Scholar]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical Course and Risk Factors for Mortality of Adult In-patients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, J.; Yang, Y.; Ma, H.; Li, Z.; Zhang, J.; Cheng, J.; Zhang, X.; Zhao, Y.; Xia, Z.; et al. The role of interleukin-6 in monitoring severe case of coronavirus disease 2019. EMBO Mol. Med. 2020, 12, e12421. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Jiang, L.; Li, X.; Lin, F.; Wang, Y.; Li, B.; Jiang, T.; An, W.; Liu, S.; Liu, H.; et al. Clinical and Pathological Investigation of Patients with Severe COVID-19. JCI Insight 2020, 5, e138070. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Kong, J.; Wang, W.; Wu, M.; Yao, L.; Wang, Z.; Jin, J.; Wu, D.; Yu, X. The Clinical Implication of Dynamic Neutrophil to Lymphocyte Ratio and D-Dimer in COVID-19: A Retrospective Study in Suzhou China. Thromb. Res. 2020, 192, 3–8. [Google Scholar] [CrossRef]
- Bauer, W.; Diehl-Wiesenecker, E.; Ulke, J.; Galtung, N.; Havelka, A.; Hegel, J.K.; Tauber, R.; Somasundaram, R.; Kappert, K. Outcome Prediction by Serum Calprotectin in Patients with COVID-19 in the Emergency Department. J. Infect. 2021, 82, 84–123. [Google Scholar] [CrossRef] [PubMed]
- Silvin, A.; Chapuis, N.; Dunsmore, G.; Goubet, A.-G.; Dubuisson, A.; Derosa, L.; Almire, C.; Henon, C.; Kosmider, O.; Droin, N.; et al. Elevated Calprotectin and abnormal myeloid cell subsets discriminate severe from mild COVID-19. Cell 2020, 182, 1401–1418. [Google Scholar] [CrossRef]
- Pourbagheri-Sigaroodi, A.; Bashash, D.; Fateh, F.; Abolghasemi, H. Laboratory findings in COVID-19 diagnosis and prognosis. Clin. Chim. Acta 2020, 510, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Kalem, A.K.; Kayaaslan, B.; Neseliogliu, S.; Eser, F.; Hasanoglu, I.; Aypak, A.; Akinci, E.; Akca, H.N.; Erel, O.; Guner, R. A Useful and Sensitive Marker in the Prediction of COVID-19 and Disease Severity: Thiol. Free Radic. Biol. Med. 2021, 166, 11–17. [Google Scholar] [CrossRef]
- Turell, L.; Radi, R.; Alvarez, B. The Thiol Pool in Human Plasma: The Central Contribution of Albumin to Redox Processes. Free Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourdon, E.; Loreau, N.; Lagrost, L.; Blache, D. Differential effects of cysteine and methionine residues in the antioxidant activity of human serum albumin. Free Radic. Res. 2005, 39, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Anraku, M.; Chuang, V.T.G.; Maruyama, T.; Otagiri, M. Redox Properties of Serum Albumin. Biochim. Biophys. Acta 2013, 1830, 5465–5472. [Google Scholar] [CrossRef] [PubMed]
- Bar-Or, D.; Curtis, G.; Rao, N.; Bampos, N.; Lau, E. Characterization of the Co2+ and Ni2+ Binding Amino-Acid Residues of the N-Terminus of Human Albumin: An Insight into the Mechanism of a New Assay for Myocardial Ischemia. Eur. J. Biochem. 2001, 268, 42–47. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Antezana, J.P.E.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martínez, A.; et al. Clinical, Laboratory and Imaging Features of COVID-19: A Systematic Review and Meta-Analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Hati, S.; Bhattacharyya, S. Impact of Thiol–Disulfide Balance on the Binding of Covid-19 Spike Protein with Angiotensin-Converting Enzyme 2 Receptor. ACS Omega 2020, 5, 16292–16298. [Google Scholar] [CrossRef] [PubMed]
- Suhail, S.; Zajac, J.; Fossum, C.; Lowater, H.; McCracken, C.; Severson, N.; Laatsch, B.; Narkiewicz-Jodko, A.; Johnson, B.; Liebau, J.; et al. Role of Oxidative Stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) Infection: A Review. Protein J. 2020, 39, 644–656. [Google Scholar] [CrossRef]
- Management of COVID-19. Available online: https://www.COVID-19treatmentguidelines.nih.gov/overview/management-of-COVID-19 (accessed on 16 September 2020).
- Lemarechal, H.; Allanore, Y.; Chenevier-Gobeaux, C.; Ekindjian, O.G.; Kahan, A.; Borderie, D. High Redox Thioredoxin but Low Thioredoxin Reductase Activities in the Serum of Patients with Rheumatoid Arthritis. Clin. Chim. Acta 2006, 367, 156–161. [Google Scholar] [CrossRef]
- Witko-Sarsat, V.; Friedlander, M.; Capeillère-Blandin, C.; Nguyen-Khoa, T.; Nguyen, A.T.; Zingraff, J.; Jungers, P.; Descamps-Latscha, B. Advanced Oxidation Protein Products as a Novel Marker of Oxidative Stress in Uremia. Kidney Int. 1996, 49, 1304–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borderie, D.; Allanore, Y.; Meune, C.; Devaux, J.Y.; Ekindjian, O.G.; Kahan, A. High ischemia-modified albumin concentration reflects oxidative stress but not myocardial involvement in systemic sclerosis. Clin. Chem. 2004, 50, 2190–2193. [Google Scholar] [CrossRef] [Green Version]
- Åsberg, A.; Løfblad, L.; Felic, A.; Hov, G.G. Measuring calprotectin in plasma and blood with a fully automated turbidimetric assay. Scand. J. Clin. Lab. Investig. 2019, 79, 50–57. [Google Scholar] [CrossRef]
- Sharifpour, M.; Rangaraju, S.; Liu, M.; Alabyad, D.; Nahab, F.B.; Creel-Bulos, C.M.; Jabaley, C.S.; on behalf of the Emory COVID-19 Quality & Clinical Research Collaborative. C-Reactive protein as a prognostic indicator in hospitalized patients with COVID-19. PLoS ONE 2020, 15, e0242400. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | COVID-19 Patients According to Severity | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mild (Stage 0) | Moderate (Stage 1) | Severe (Stage 2) | Critical (Stage 3) | ||||||
| N | Value | N | Value | N | Value | N | Value | p | |
| Men—n (%) | 31 | 11 (35.5) | 36 | 20 (55.6) | 36 | 18 (50) | 57 | 43 (75.4) | <0.001 |
| Age—years (IQR) | 31 | 47.4 (32.4–57.1) | 36 | 63.9 (49.1–75.8) | 36 | 64.7 (58.5–74.9) | 57 | 61.9 (51.2–73.9) | <0.001 |
| Smoking—n (%) | 31 | 4 (12.9) | 36 | 9 (25.0) | 36 | 9 (25.0) | 57 | 12 (21.1) | 0.542 |
| Cardiovascular Disease—n (%) | 30 | 6 (20) | 34 | 19 (55.9) | 36 | 20 (55.6) | 53 | 30 (56.6) | 0.006 |
| Overweight/obesity—n (%) | 31 | 6 (19.4) | 36 | 17 (47.2) | 36 | 17 (47.2) | 57 | 42 (73.7) | <0.001 |
| Hypertension—n (%) | 30 | 3 (10) | 36 | 16 (44.4) | 36 | 16 (44.4) | 54 | 26 (48.1) | 0.003 |
| Diabetes—n (%) | 30 | 1 (3.3) | 36 | 10 (27.8) | 36 | 13 (36.1) | 54 | 13 (24.1) | 0.068 |
| Chronic kidney Disease—n (%) | 30 | 1 (3.3) | 36 | 7 (19.4) | 36 | 1 (2.8) | 53 | 7 (13.2) | 0.568 |
| Chronic Resp Failure—n (%) | 30 | 2 (6.7) | 36 | 1 (2.8) | 36 | 2 (5.6) | 54 | 3 (5.6) | 0.961 |
| Systemic autoimmune Disease—n (%) | 30 | 1 (3.3) | 35 | 4 (11.4) | 36 | 1 (2.8) | 54 | 3 (5.6) | 0.851 |
| Symptoms and Clinic at Admission: | |||||||||
| Temperature > 38 °C—n (%) | 31 | 9 (29.0) | 36 | 30 (83.3) | 35 | 30 (85.7) | 52 | 41 (78.8) | <0.001 |
| Cough—n (%) | 31 | 19 (61.3) | 36 | 24 (66.7) | 36 | 23 (63.9) | 54 | 31 (57.4) | 0.580 |
| Dyspnea—n (%) | 31 | 9 (29.0) | 36 | 17 (47.2) | 36 | 25 (69.4) | 55 | 44 (80) | <0.001 |
| Myalgias—n (%) | 31 | 14 (45.2) | 36 | 11 (30.6) | 36 | 13 (36.1) | 55 | 11 (20) | 0.026 |
| Fatigue—n (%) | 31 | 3 (9.7) | 36 | 21 (58.3) | 36 | 19 (52.8) | 55 | 21 (38.2) | 0.103 |
| Diarrhea—n (%) | 31 | 10 (32.3) | 36 | 10 (27.8) | 36 | 10 (27.8) | 55 | 10 (18.2) | 0.142 |
| Oxygenation—n (%) | 31 | 1 (3.2) | 36 | 28 (77.8) | 36 | 36 (100) | 57 | 57 (100) | <0.001 |
| Admission flow (L/min) | 1 | ND | 26 | 2.0 (1.0–2.0) | 35 | 4.0 (2.6–5.5) | 45 | 5 (3.0–15.0) | <0.001 |
| Extension at TDM: <10% 10–25% 25–50% 50–75% >75% | 31 3 3 3 3 3 | 5 (16.1) 2 (66.7) 0 (0) 1 (33.3) 0 (0) 0 (0) | 36 29 29 29 29 29 | 33 (91.7) 4 (13.8) 9 (31.0) 13 (44.8) 3 (10.3) 0 (0) | 36 33 33 33 33 33 | 35 (97.2) 0 (0) 6 (18.2) 14 (42.4) 10 (30.3) 3 (9.1) | 51 31 31 31 31 31 | 44 (86.3) 0 (0) 4 (12.9) 12 (38.7) 9 (29.0) 6 (19.4) | <0.001 <0.001 |
| O2 needs majoration —n (%) | 31 | 0 (0) | 36 | 10 (28) | 36 | 24 (67) | 57 | 55 (96) | <0.001 |
| Ventilation—n (%) | 31 | 0 (0) | 36 | 1 (2.8) | 36 | 13 (36.1) | 57 | 54 (94.7) | <0.001 |
| ICU Admission—n (%) | 31 | 1 (3.2) | 36 | 1 (2.8) | 36 | 10 (27.8) | 57 | 52 (91.2) | <0.001 |
| Length of stay—n (%) | 31 | 0 (0–0) | 36 | 7 (4–10) | 36 | 10 (7–19) | 56 | 26 (16–50) | <0.001 |
| Death—n (%) | 31 | 0 (0) | 36 | 0 (0) | 36 | 0 (0) | 57 | 17 (29.8) | <0.001 |
| Blood Routine Biomarkers at admission, when performed | |||||||||
| Albumin—g/L (IQR) | 6 | 38 (30–42) | 28 | 34.5 (31–37) | 28 | 32.5 (29–36) | 49 | 25 (22–30) | <0.001 |
| CRP—mg/L (IQR) | 14 | 1.8 (1.0–23.0) | 34 | 74.9 (28.8–118.3) | 34 | 98.4 (45.7–166.7) | 42 | 162 (48.6–234) | <0.001 |
| Fibrinogen—g/L (IQR) | 25 | 3.3 (2.7–3.8) | 25 | 6.2 (4.5–7.3) | 32 | 6.9 (5.5–7.9) | 47 | 6.6 (4.9–8.0) | <0.001 |
| Leukocytes—G/L (IQR) | 30 | 4.69 (4.04–6.10) | 35 | 5.08 (3.94–7.46) | 36 | 6.61 (4.75–9.23) | 57 | 9.35 (7.64–12.4) | <0.001 |
| Neutrophils—G/L (IQR) Neutrophils/Lymphocytes | 30 30 | 2.75 (2.30–3.62) 2.0 (1.5–2.3) | 34 34 | 3.65 (2.46–5.24) 3.7 (2.3–5.7) | 36 36 | 4.66 (3.39–6.87) 4.5 (3.4–9.2) | 56 56 | 7.55 (5.88–11.0) 8.5 (4.9–14.4) | <0.001 <0.001 |
| Biomarker | AUC | p | Optimal Threshold (*) | Sensibility in % [95% CI] | Specificity in % [95% CI] | Positive Predictive Value in % [95% CI] | Negative Predictive Value in % [95% CI] |
|---|---|---|---|---|---|---|---|
| For prediction of ICU admission | |||||||
| Thiols | 0.762 | <0.001 | <154 µmol/L | 79.7 [67.8–88.7] | 64.6 [54.2–74.1] | 58.8 [47.2–69.5] | 78.9 [68.1–86.9] |
| IL-6 | 0.746 | <0.001 | >60.9 ng/L | 59.4 [46.4–71.5] | 78.1 [68.5–85.9] | 62.3 [48.9–74.1] | 73.7 [63.7–81.8] |
| Calprotectin | 0.739 | <0.001 | >28.1 mg/L | 62.7 [49.1–75.0] | 81.7 [72.4–89.0] | 63.5 [50.4–75.0] | 78.7 [68.5–86.4] |
| PSEP | 0.726 | <0.001 | >721 ng/L | 68.3 [55.3–79.4] | 70.8 [60.7–79.7] | 60.6 [48.3–71.8] | 77.3 [66.9–85.3] |
| AOPP | 0.634 | 0.003 | >70 µmol/L | 73.0 [60.3–83.4] | 52.1 [41.6–62.4] | 50.0 [39.5–60.5] | 74.6 [62.2–84.1] |
| IMA | 0.634 | 0.002 | >0.17 ABSU | 74.6 [62.1–84.7] | 52.6 [42.1–63.0] | 51.1 [40.5–61.6] | 75.8 [63.4–85.1] |
| For prediction of mortality | |||||||
| Calprotectin | 0.792 | <0.001 | >24.1 mg/L | 94.1 [71.3–99.9] | 64.9 [56.2–73.0] | 97.1 [88.4–99.5] | 98.9 [93.0–99.9] |
| IL-6 | 0.786 | <0.001 | >37.6 ng/L | 94.4 [72.7–99.9] | 59.6 [51.0–67.7] | 23.0 [14.3–34.5] | 98.8 [92.7–99.9] |
| Thiols | 0.750 | <0.001 | <135 µmol/L | 83.3 [58.6–96.4] | 63.1 [54.6–71.1] | 21.0 [12.1–33.6] | 94.8 [87.8–98.1] |
| PSEP | 0.749 | <0.001 | >545 ng/L | 94.4 [72.7–99.9] | 49.3 [40.7–57.9] | 19.3 [12.0–29.4] | 98.6 [91.3–99.9] |
| AOPP | 0.620 | 0.027 | >88 µmol/L | 72.2 [46.5–90.3] | 53.2 [45.–62.0] | 16.7 [9.5–27.2] | 93.8 [85.4–97.7] |
| IMA | 0.534 | 0.599 | / | / | / | / | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ducastel, M.; Chenevier-Gobeaux, C.; Ballaa, Y.; Meritet, J.-F.; Brack, M.; Chapuis, N.; Pene, F.; Carlier, N.; Szwebel, T.-A.; Roche, N.; et al. Oxidative Stress and Inflammatory Biomarkers for the Prediction of Severity and ICU Admission in Unselected Patients Hospitalized with COVID-19. Int. J. Mol. Sci. 2021, 22, 7462. https://doi.org/10.3390/ijms22147462
Ducastel M, Chenevier-Gobeaux C, Ballaa Y, Meritet J-F, Brack M, Chapuis N, Pene F, Carlier N, Szwebel T-A, Roche N, et al. Oxidative Stress and Inflammatory Biomarkers for the Prediction of Severity and ICU Admission in Unselected Patients Hospitalized with COVID-19. International Journal of Molecular Sciences. 2021; 22(14):7462. https://doi.org/10.3390/ijms22147462
Chicago/Turabian StyleDucastel, Morgane, Camille Chenevier-Gobeaux, Yassine Ballaa, Jean-François Meritet, Michel Brack, Nicolas Chapuis, Frédéric Pene, Nicolas Carlier, Tali-Anne Szwebel, Nicolas Roche, and et al. 2021. "Oxidative Stress and Inflammatory Biomarkers for the Prediction of Severity and ICU Admission in Unselected Patients Hospitalized with COVID-19" International Journal of Molecular Sciences 22, no. 14: 7462. https://doi.org/10.3390/ijms22147462