
Lactate and Lactate-to-Pyruvate Ratio in Critically Ill COVID-19 Patients: A Pilot Study

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
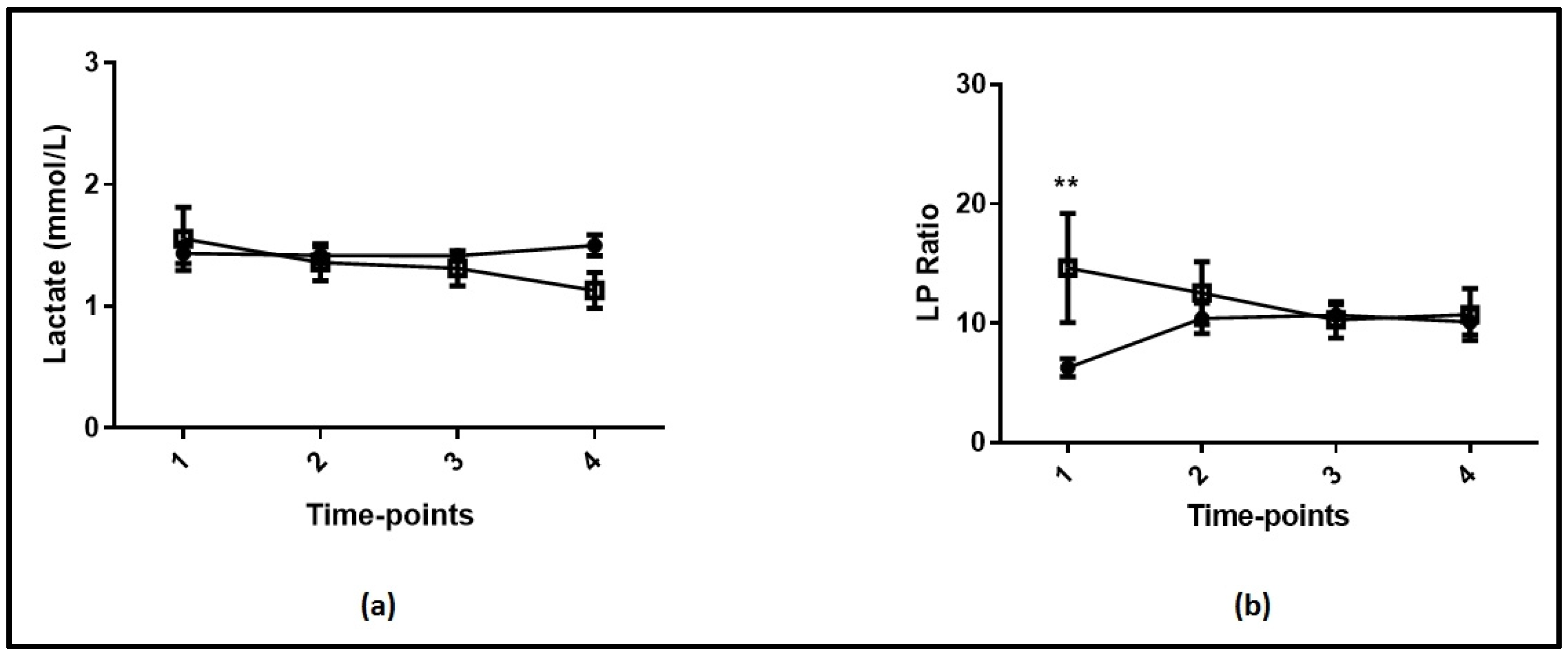
3.2. Lactate and Lactate-to-Pyruvate Ratio in COVID-19 and Non-COVID-19 Patients
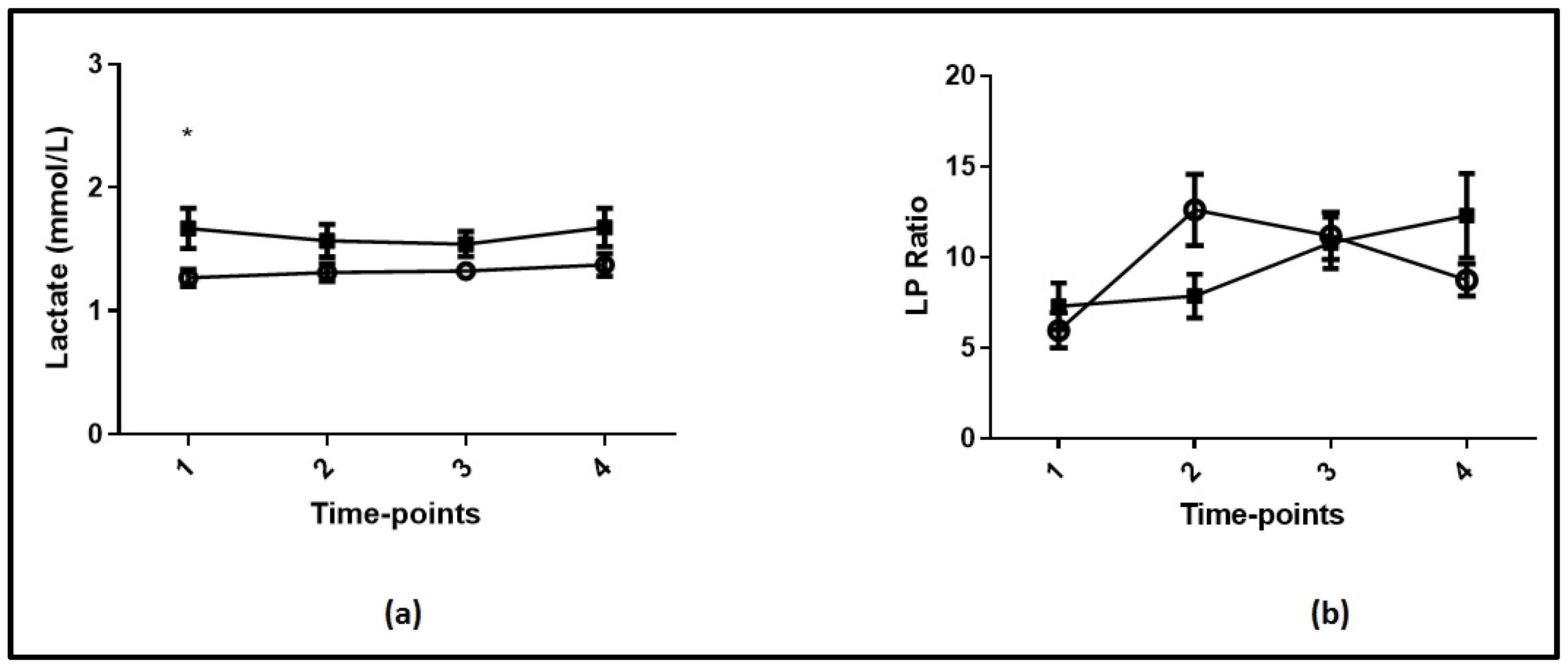
3.3. Lactate and Lactate-to-Pyruvate Ratio in COVID-19 Survivors and Non-Survivors
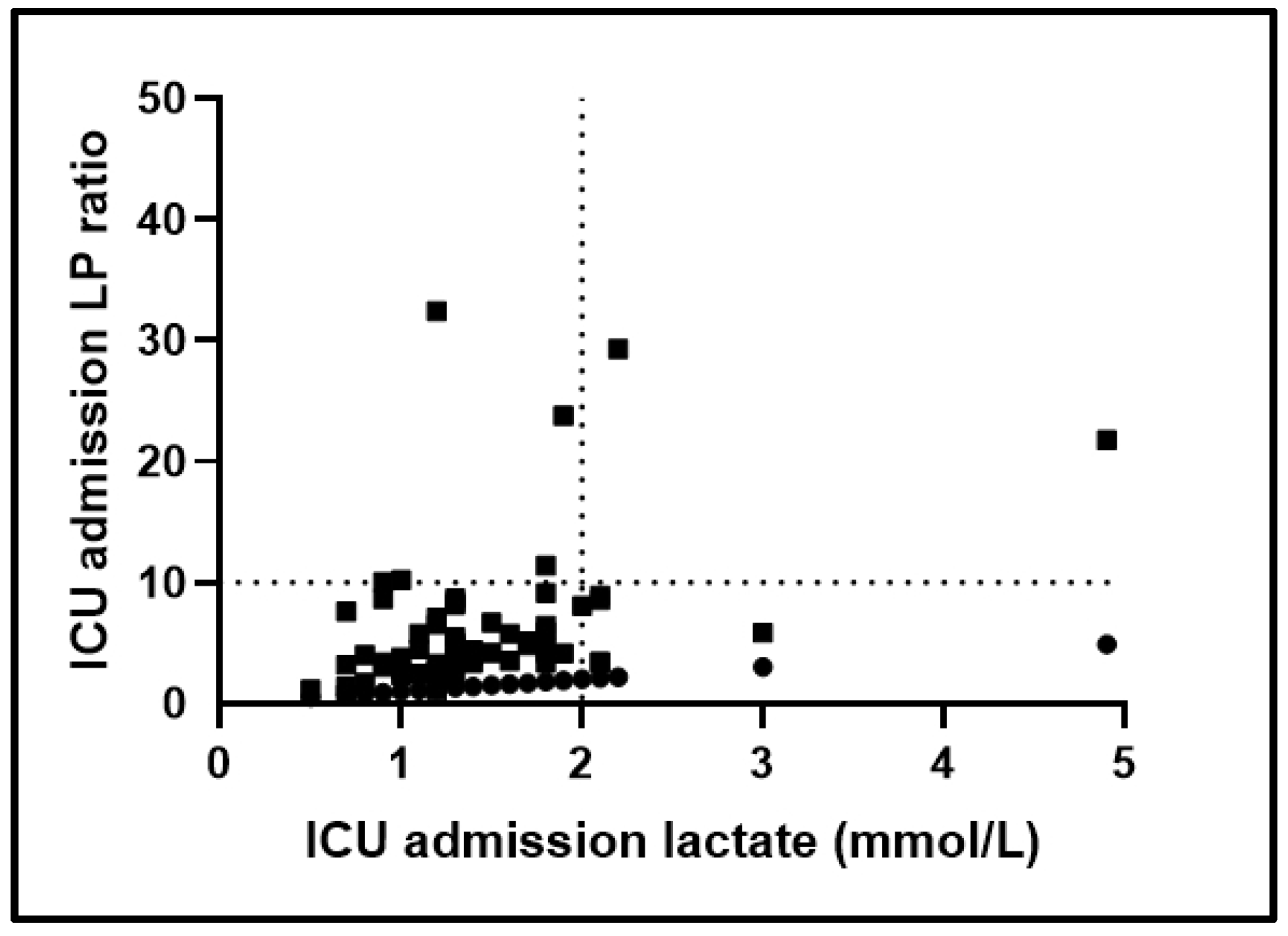
3.4. Metabolic Patterns in COVID-19 Patients and ICU Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Attaway, A.H.; Scheraga, R.G.; Bhimraj, A.; Biehl, M.; Hatipoğlu, U. Severe COVID-19 pneumonia: Pathogenesis and clinical management. BMJ 2021, 372, n436. [Google Scholar] [CrossRef] [PubMed]
- Singer, A.J.; Taylor, M.; Domingo, A.; Ghazipura, S.; Khorasonchi, A.; Thode, H.C., Jr.; Shapiro, N.I. Diagnostic characteristics of a clinical screening tool in combination with measuring bedside lactate level inemergency department patients with suspected sepsis. Acad. Emerg. Med. 2014, 21, 853–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, J.; Nijsten, M.W.; Jansen, T.C. Clinical use of lactate monitoring in critically ill patients. Ann. Intensive Care. 2013, 3, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Alvarez, M.; Marik, P.; Bellomo, R. Sepsis-associated hyper lactatemia. Crit. Care 2014, 18, 503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuzzo, E.; Berg, K.M.; Andersen, L.W.; Balkema, J.; Montissol, S.; Cocchi, M.N.; Liu, X.; Donnino, M.W. Pyruvate dehydrogenase activity is decreased in the peripheral blood mononuclear cells of patients with Sepsis: A prospective observational trial. Ann. Am. Thorac. Soc. 2015, 12, 1662–1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godinjak, A.; Jusufovic, S.; Rama, A.; Iglica, A.; Zvizdic, F.; Kukuljac, A.; Tancica, I.; Rozajac, S. Hyper lactatemia and the importance of repeated lactate measurements in critically ill patients. Med. Arch. 2017, 71, 404–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, B.; Sadoune, L.O.; Gelot, A.M.; Bollaert, P.E.; Nabet, P.; Larcan, A. Evolution of lactate/pyruvate and arterial ketone body ratios in the early course of catecholamine-treated septic shock. Crit. Care Med. 2000, 28, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Rimachi, R.; Bruzzide Carvahlo, F.; Orellano-Jimenez, C.; Cotton, F.; Vincent, J.L.; De Backer, D. Lactate/pyruvate ratio as a marker of tissue hypoxia in circulatory and septic shock. Anaesth. Intensive Care 2012, 40, 427–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suistomaa, M.; Ruokonen, E.; Kari, A.; Takala, J. Time-pattern of lactate and lactate to pyruvate ratio in the first 24 hours of intensive care emergency admissions. Shock 2000, 14, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weil, M.H.; Afifi, A.A. Experimental and clinical studies on lactate and pyruvate as indicators of the severity of acute circulatory failure (shock). Circulation 1970, 41, 989–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotchkiss, R.S.; Karl, I.E. Reevaluation of the role of cellular hypoxia and bioenergetic failure in sepsis. JAMA 1992, 267, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Cooper-smith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Vassiliou, A.G.; Jahaj, E.; Ilias, I.; Markaki, V.; Malachias, S.; Vrettou, C.; Ischaki, E.; Mastora, Z.; Douka, E.; Keskinidou, C.; et al. Lactate kinetics reflect organ dysfunction and are associated with adverse out-comes in intensive care unit patients with COVID-19 pneumonia: Preliminary results from a greek single-centre study. Metabolites 2020, 10, 386. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasonein hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Chioléro, R.L.; Revelly, J.P.; Leverve, X.; Gersbach, P.; Cayeux, M.C.; Berger, M.M.; Tappy, L. Effects of cardio genic shock on lactate and glucose metabolism after heart surgery. Crit. Care Med. 2000, 28, 3784–3791. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Critically-Ill COVID-19 | Critically-Ill Non-COVID-19 | p-Value | Effect Size |
|---|---|---|---|---|
| Number of patients, N | 63 | 17 | ||
| Age (years), (mean ± SD) | 63 ± 12 | 63 ± 12 | 0.97 | 0 |
| Sex, N (%) | 0.07 | 0.21 | ||
| Male | 48 (76.2%) | 9 (52.9%) | ||
| Female | 15 (23.8%) | 8 (47.1%) | ||
| BMI (kg/m2), (median, IQR) | 26.0 (24.5–27.8) | 26.0 (24.4–30.2) | 0.80 | 0.03 |
| Comorbidities, N (%) | 44 (69.8%) | 9 (52.9%) | 0.25 | 0.18 |
| Diagnosis, N (%) | <0.0001 * | 0.64 | ||
| Medical | 62 (98.4%) | 8 (47.1%) | ||
| Surgical/Trauma | 1 (1.6%) | 9 (52.9%) | ||
| Characteristics on ICU admission | ||||
| APACHE II score, (median, IQR) | 14 (12–17) | 19 (15–20) | 0.053 | 0.22 |
| SOFA score, (median, IQR) | 8 (7–8) | 8 (7–9) | 0.43 | 0.09 |
| ICU admission lactate (mmol/L), (median, IQR) | 1.30 (1.00–1.80) | 1.10 (0.85–1.85) | 0.60 | 0.06 |
| Mean lactate (mmol/L), (median, IQR) | 1.38 (1.13–1.68) | 1.25 (0.88–1.68) | 0.42 | 0.09 |
| Max lactate (mmol/L), (median, IQR) | 1.60 (1.30–2.00) | 1.50 (1.10–2.50) | 0.58 | 0.06 |
| ICU admission LP ratio, (median, IQR) | 4.72 (3.27–7.61) | 9.18 (5.55–16.50) | 0.005 * | 0.36 |
| Mean LP ratio, (median, IQR) | 8.57 (5.72–11.52) | 12.65 (6.31–16.25) | 0.22 | 0.14 |
| Max LP ratio, (median, IQR) | 14.58 (10.16–23.75) | 15.91 (9.85–27.62) | 0.58 | 0.06 |
| Mean vasopressor dose (µg/kg/min), (median, IQR) | 0.16 (0.04–0.30) | 0.28 (0.16–0.40) | 0.03 * | 0.25 |
| Max vasopressor dose (µg/kg/min), (median, IQR) | 0.25 (0.08–0.55) | 0.45 (0.31–0.78) | 0.01 * | 0.28 |
| Septic shock, N (%) | 14 (22.2%) | 5 (29.4) | 0.14 | 0.07 |
| Laboratory data | ||||
| pH, (mean ± SD) | 7.36 ± 0.09 | 7.34 ± 0.06 | 0.3 | 0.24 |
| Hemoglobin, (mean ± SD) | 11.7 ± 1.7 | 9.9 ± 2.0 | 0.001 * | 1.02 |
| Hematocrit, (mean ± SD) | 35.8 ± 4.7 | 30.1 ± 6.5 | <0.0001 * | 1.11 |
| Red blood cell count (million cells per μL), (median, IQR) | 4.13 (3.79–4.45) | 3.47 (3.14–4.07) | 0.003 * | 0.35 |
| White blood cell count (per μL), (median, IQR) | 10,300 (8200–13,200) | 14,910 (11,145–20,525) | 0.002 * | 0.34 |
| Platelets (per μL), (median, IQR) | 210,000 (164,000–270,000) | 208,000 (168,500–303,000) | 0.49 | 0.08 |
| Creatinine (mg/dL), (median, IQR) | 0.9 (0.8–1.2) | 0.7 (0.5–1.1) | 0.06 | 0.21 |
| Total bilirubin (mg/dL), (median, IQR) | 0.6 (0.4–0.8) | 0.6 (0.5–0.7) | 0.93 | 0.01 |
| CRP (mg/dL), (median, IQR) | 15.0 (8.9–21.2) | 14.6 (7.8–19.2) | 0.56 | 0.06 |
| LDH (U/L), (median, IQR) | 497 (379–702) | 254 (214–463) | 0.001 * | 0.36 |
| Na+ (mEq/L), (mean ± SD) | 139.5 ± 6.2 | 142.7 ± 10.0 | 0.10 | 0.45 |
| Cytokines | ||||
| IL-6 (pg/mL), (median, IQR) | 16.1 (8.3–42.8) | 36.6 (27.5–98.6) | 0.01 * | 0.28 |
| IL-8 (pg/mL), (median, IQR) | 54.7 (30.4–90.9) | 61.6 (17.2–94.6) | 0.85 | 0.02 |
| IL-10 (pg/mL), (median, IQR) | 11.4 (4.3–27.1) | 11.0 (1.3–25.6) | 0.50 | 0.19 |
| TNF-α (pg/mL), (median, IQR) | 49.1 (27.1–78.7) | 32.8 (26.0–37.9) | 0.12 | 0.18 |
| Outcomes | ||||
| LoS in the ICU (days), (median, IQR) | 24 (14–38) | 19 (9–32) | 0.21 | 0.14 |
| ICU mortality, N (%) | 26 (41.3%) | 5 (29.4%) | 0.42 | 0.1 |
| Characteristics | Survivors | Non-Survivors | p-Value | Effect Size |
|---|---|---|---|---|
| Number of patients, N | 37 | 26 | ||
| Age (years), (mean ± SD) | 60 ± 10 | 68 ± 11 | 0.006 * | 0.77 |
| Sex, N (%) | 0.24 | 0.17 | ||
| Male | 26 (70.3%) | 22 (84.6%) | ||
| Female | 11 (29.7%) | 4 (15.4%) | ||
| BMI (kg/m2), (median, IQR) | 25.7 (24.5–27.6) | 26.2 (24.43–28.65) | 0.38 | 0.11 |
| Comorbidities, N (%) | 26 (70.3%) | 20 (76.9%) | 0.77 | 0.07 |
| APACHE II score, (median, IQR) | 12 (11–16) | 16 (13–21) | 0.002 * | 0.38 |
| SOFA score, (median, IQR) | 8 (7–8) | 8 (7–9) | 0.15 | 0.23 |
| ICU admission lactate (mmol/L), (median, IQR) | 1.20 (0.90–1.65) | 1.45 (1.28–1898) | 0.01 * | 0.32 |
| ICU admission LP ratio, (median, IQR) | 4.04 (2.92–5.85) | 5.82 (3.79–8.60) | 0.056 | 0.24 |
| D-dimers (µg/mL), (median, IQR) | 1.09 (0.65–3.32) | 1.06 (0.74–3.38) | 0.71 | 0.05 |
| CRP (mg/dL), (median, IQR) | 14.5 (7.8–19.7) | 19.3 (9.1–23.5) | 0.10 | 0.21 |
| LDH (U/L), (median, IQR) | 513 (404–682) | 460 (339–705) | 0.39 | 0.11 |
| Variables | Univariate Model | Multivariate Model | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Age (years) | 1.071 | 1.017–1.127 | 0.010 * | 1.053 | 0.991–1.118 | 0.093 |
| APACHE II score | 1.190 | 1.048–1.352 | 0.007 * | 1.142 | 0.986–1.323 | 0.077 |
| ICU admission lactate (mmol/L) | 3.747 | 1.167–12.028 | 0.026 * | 1.968 | 0.420–9.217 | 0.390 |
| Metabolic pattern | ||||||
| Normal | Ref. value | Ref. value | ||||
| Abnormal | 6.447 | 1.216–34.173 | 0.029 * | 0.390 | 0.046–3.329 | 0.389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassiliou, A.G.; Tsipilis, S.; Keskinidou, C.; Vrettou, C.S.; Jahaj, E.; Gallos, P.; Routsi, C.; Orfanos, S.E.; Kotanidou, A.; Dimopoulou, I. Lactate and Lactate-to-Pyruvate Ratio in Critically Ill COVID-19 Patients: A Pilot Study. J. Pers. Med. 2022, 12, 171. https://doi.org/10.3390/jpm12020171
Vassiliou AG, Tsipilis S, Keskinidou C, Vrettou CS, Jahaj E, Gallos P, Routsi C, Orfanos SE, Kotanidou A, Dimopoulou I. Lactate and Lactate-to-Pyruvate Ratio in Critically Ill COVID-19 Patients: A Pilot Study. Journal of Personalized Medicine. 2022; 12(2):171. https://doi.org/10.3390/jpm12020171
Chicago/Turabian StyleVassiliou, Alice G., Stamatios Tsipilis, Chrysi Keskinidou, Charikleia S. Vrettou, Edison Jahaj, Parisis Gallos, Christina Routsi, Stylianos E. Orfanos, Anastasia Kotanidou, and Ioanna Dimopoulou. 2022. "Lactate and Lactate-to-Pyruvate Ratio in Critically Ill COVID-19 Patients: A Pilot Study" Journal of Personalized Medicine 12, no. 2: 171. https://doi.org/10.3390/jpm12020171