
A Simple Prognostic Score for Critical COVID-19 Derived from Patients without Comorbidities Performs Well in Unselected Patients

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.1.1. Derivation Cohort: Unvaccinated Population without Comorbidities
2.1.2. Validation Cohorts
3. Statistical Analysis
4. Results
4.1. Laboratory Features on Admission Associated with Critical COVID-19 in the Absence of Comorbidities
4.2. Predictors of Critical COVID-19 in the Absence of Comorbidities
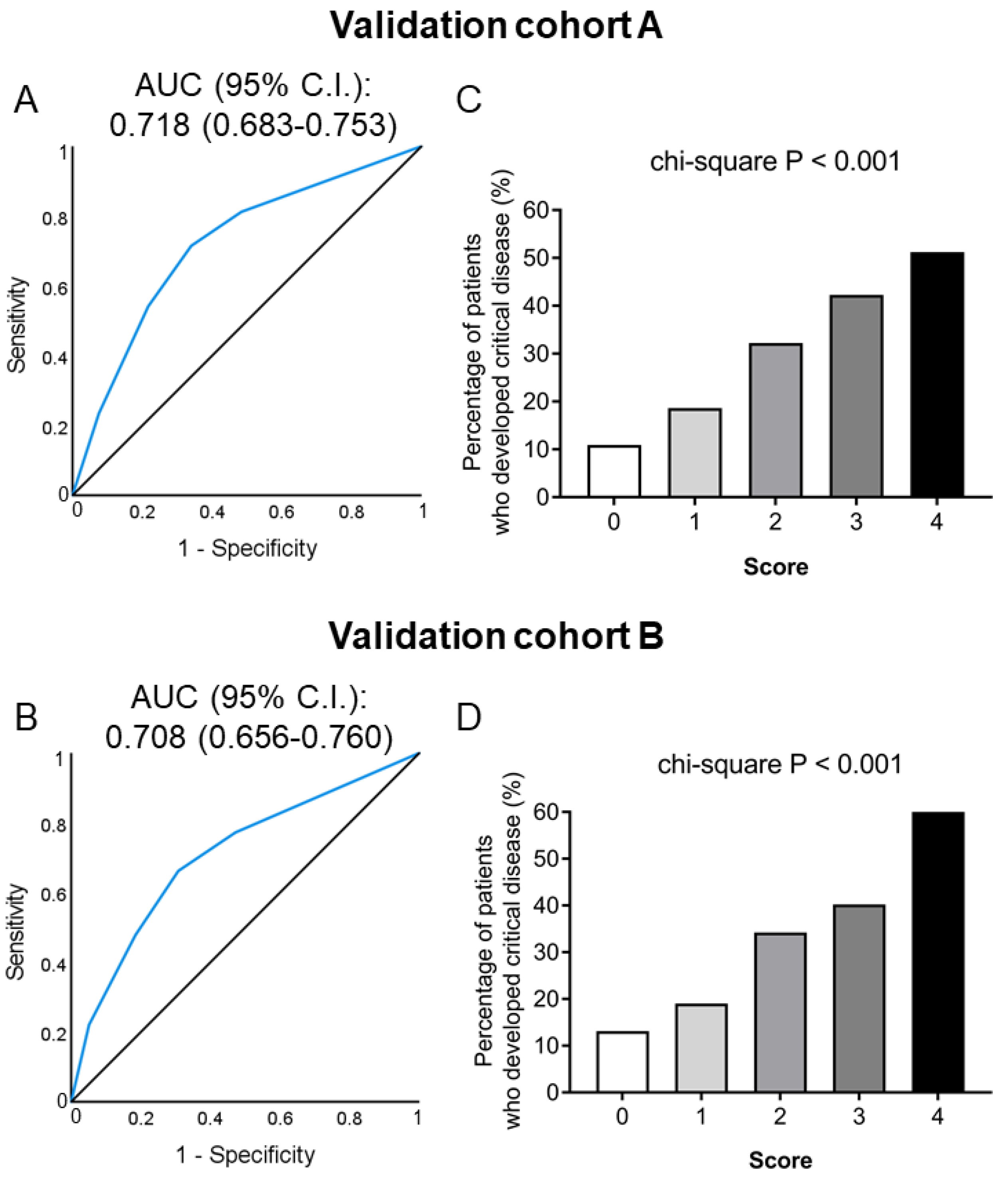
4.3. Development and Validation of a Simple Score for Critical COVID-19 Prediction
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 18 March 2022).
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk Stratification of Patients Admitted to Hospital with COVID-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Harrison, E.M.; Ho, A.; Docherty, A.B.; Knight, S.R.; van Smeden, M.; Abubakar, I.; Lipman, M.; Quartagno, M.; Pius, R.; et al. Development and Validation of the ISARIC 4C Deterioration Model for Adults Hospitalised with COVID-19: A Prospective Cohort Study. Lancet Respir. Med. 2021, 9, 349–359. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male Sex Identified by Global COVID-19 Meta-Analysis as a Risk Factor for Death and ITU Admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Li, S.; Yu, H.; Wang, P.; Zhang, Y.; Chen, Z.; Li, Y.; Cheng, L.; Li, W.; Jia, H.; et al. Epidemiological, Comorbidity Factors with Severity and Prognosis of COVID-19: A Systematic Review and Meta-Analysis. Aging 2020, 12, 12493–12503. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.Y.; Juthani, P.V.; Borges, K.A.; Shallow, M.K.; Gupta, A.; Price, C.; Won, C.H.; Chun, H.J. Severe Breakthrough COVID-19 Cases in the SARS-CoV-2 Delta (B.1.617.2) Variant Era. Lancet Microbe 2022, 3, e4–e5. [Google Scholar] [CrossRef]
- Macedo, A.; Gonçalves, N.; Febra, C. COVID-19 Fatality Rates in Hospitalized Patients: Systematic Review and Meta-Analysis. Ann. Epidemiol. 2021, 57, 14–21. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; Diab, W.; Wang, J.; Khanijo, S.; Mignatti, A.; Gianos, E.; Cohen, M.; Sharifova, G.; et al. Efficacy and Safety of Therapeutic-Dose Heparin vs Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-Risk Hospitalized Patients With COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1612–1620. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19-Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky, K.E.; Ferolito, B.R.; Figueroa Muñiz, M.J.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; Casas, J.P.; et al. Comparative Effectiveness of BNT162b2 and MRNA-1273 Vaccines in U.S. Veterans. N. Engl. J. Med. 2022, 386, 105–115. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G.; Stenehjem, E.; Grannis, S.; Ball, S.W.; Naleway, A.L.; Ong, T.C.; DeSilva, M.B.; Natarajan, K.; Bozio, C.H.; Lewis, N.; et al. Effectiveness of COVID-19 Vaccines in Ambulatory and Inpatient Care Settings. N. Engl. J. Med. 2021, 385, 1355–1371. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://eody.gov.gr/wp-content/uploads/2022/02/covid_19_algorithmos-nosileuomenon_20220217.pdf (accessed on 18 March 2022).
- Bone, R.C.; Balk, R.A.; Cerra, F.B.; Dellinger, R.P.; Fein, A.M.; Knaus, W.A.; Schein, R.M.; Sibbald, W.J. Definitions for Sepsis and Organ Failure and Guidelines for the Use of Innovative Therapies in Sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 1992, 101, 1644–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical Spectrum. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 27 January 2022).
- Li, X.; Marmar, T.; Xu, Q.; Tu, J.; Yin, Y.; Tao, Q.; Chen, H.; Shen, T.; Xu, D. Predictive Indicators of Severe COVID-19 Independent of Comorbidities and Advanced Age: A Nested Case-control Study. Epidemiol. Infect. 2020, 148, e255. [Google Scholar] [CrossRef]
- Ozturk, S.; Kurtulus Ozturk, E.; Yildiz Kaya, S. Clinical and Radiological Characteristics of COVID-19 Patients without Comorbidities. Wien. Klin. Wochenschr. 2021, 133, 875–881. [Google Scholar] [CrossRef]
- Wang, P.; Sha, J.; Meng, M.; Wang, C.; Yao, Q.; Zhang, Z.; Sun, W.; Wang, X.; Qie, G.; Bai, X.; et al. Risk Factors for Severe COVID-19 in Middle-Aged Patients without Comorbidities: A Multicentre Retrospective Study. J. Transl. Med. 2020, 18, 461. [Google Scholar] [CrossRef]
- Liu, W.; Yang, C.; Liao, Y.-G.; Wan, F.; Lin, L.; Huang, X.; Zhang, B.-H.; Yuan, Y.; Zhang, P.; Zhang, X.-J.; et al. Risk Factors for COVID-19 Progression and Mortality in Hospitalized Patients without Pre-Existing Comorbidities. J. Infect. Public Health 2021, 15, 13–20. [Google Scholar] [CrossRef]
- Espejo-Paeres, C.; Espliguero, R.A.; Uribarri, A.; Antón-Huguet, B.; Romero, R.; Fernández-Rozas, I.; Becerra-Muñoz, V.M.; Alfonso-Rodríguez, E.; Huang, J.; Ortega-Armas, M.E.; et al. Predictors of Poor Prognosis in Healthy, Young, Individuals with SARS-CoV-2 Infections. Clin. Microbiol. Infect. 2022, 28, 273–278. [Google Scholar] [CrossRef]
- Ronderos Botero, D.M.; Omar, A.M.S.; Sun, H.K.; Mantri, N.; Fortuzi, K.; Choi, Y.; Adrish, M.; Nicu, M.; Bella, J.N.; Chilimuri, S. COVID-19 in the Healthy Patient Population. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2764–2775. [Google Scholar] [CrossRef]
- Vlachogiannis, N.I.; Baker, K.F.; Georgiopoulos, G.; Lazaridis, C.; van der Loeff, I.S.; Hanrath, A.T.; Sopova, K.; Tual-Chalot, S.; Gatsiou, A.; Spyridopoulos, I.; et al. Clinical Frailty, and Not Features of Acute Infection, Is Associated with Late Mortality in COVID-19: A Retrospective Cohort Study. J. Cachexia Sarcopenia Muscle, 2022; online ahead of print. [Google Scholar] [CrossRef]
- Elmoheen, A.; Abdelhafez, I.; Salem, W.; Bahgat, M.; Elkandow, A.; Tarig, A.; Arshad, N.; Mohamed, K.; Al-Hitmi, M.; Saad, M.; et al. External Validation and Recalibration of the CURB-65 and PSI for Predicting 30-Day Mortality and Critical Care Intervention in Multiethnic Patients with COVID-19. Int. J. Infect. Dis. 2021, 111, 108–116. [Google Scholar] [CrossRef]
- Preti, C.; Biza, R.; Novelli, L.; Ghirardi, A.; Conti, C.; Galimberti, C.; Della Bella, L.; Memaj, I.; Di Marco, F.; Cosentini, R. Usefulness of CURB-65, Pneumonia Severity Index and MULBSTA in Predicting COVID-19 Mortality. Monaldi. Arch. Chest Dis. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Bradley, P.; Frost, F.; Tharmaratnam, K.; Wootton, D.G. NW Collaborative Organisation for Respiratory Research Utility of Established Prognostic Scores in COVID-19 Hospital Admissions: Multicentre Prospective Evaluation of CURB-65, NEWS2 and QSOFA. BMJ Open Respir. Res. 2020, 7, e000729. [Google Scholar] [CrossRef] [PubMed]
- Artero, A.; Madrazo, M.; Fernández-Garcés, M.; Muiño Miguez, A.; González García, A.; Crestelo Vieitez, A.; García Guijarro, E.; Fonseca Aizpuru, E.M.; García Gómez, M.; Areses Manrique, M.; et al. Severity Scores in COVID-19 Pneumonia: A Multicenter, Retrospective, Cohort Study. J. Gen. Intern. Med. 2021, 36, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex Differences in Immune Responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Giannis, D.; Allen, S.L.; Tsang, J.; Flint, S.; Pinhasov, T.; Williams, S.; Tan, G.; Thakur, R.; Leung, C.; Snyder, M.; et al. Postdischarge Thromboembolic Outcomes and Mortality of Hospitalized Patients with COVID-19: The CORE-19 Registry. Blood 2021, 137, 2838–2847. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Derivation Total Cohort (n = 241) | Non-Critical Course (n = 219) | Critical Course (n = 22) | p-Value * | |
|---|---|---|---|---|
| Demographics | ||||
| Male sex | 172 (71.4) | 155 (70.8) | 17 (77.3) | 0.626 |
| Age (years) | 49 (17) | 48 (17) | 57 (20) | 0.005 |
| Days from symptom onset to admission | 7 (4) | 7 (5) | 7 (4) | 0.164 |
| Symptoms and signs at admission | ||||
| Dyspnea (subjective) | 105 (43.6) | 90 (41.1) | 15 (68.2) | 0.022 |
| Cough | 104 (43.2) | 96 (43.8) | 8 (36.4) | 0.653 |
| Fever | 208 (86.3) | 188 (85.8) | 20 (90.9) | 0.747 |
| Fatigue | 30 (12.4) | 29 (13.2) | 1 (4.5) | 0.327 |
| Myalgia | 16 (6.6) | 15 (6.8) | 1 (4.5) | 1.000 |
| Headache | 21 (8.7) | 20 (9.1) | 1 (4.5) | 0.702 |
| Anosmia/Ageusia | 8 (3.3) | 8 (3.7) | 0 (0) | 1.000 |
| SpO2 < 94% at admission | 194 (80.5) | 172 (78.5) | 22 (100) | 0.010 |
| Laboratory parameters at admission | ||||
| Hemoglobin (g/dL) | 14.3 (2.1) | 14.3 (2.1) | 14.4 (1.3) | 0.622 |
| WBCs (K/μL) | 5.6 (3.4) | 5.5 (3.1) | 8.3 (4.2) | 0.001 |
| Neutrophils (K/μL) | 4.1 (3.0) | 3.9 (2.7) | 6.9 (4.1) | <0.001 |
| Lymphocytes (K/μL) | 1.05 (0.68) | 1.1 (0.7) | 0.93 (0.56) | 0.095 |
| Neutrophil/lymphocyte ratio | 3.8 (3.3) | 3.5 (3.0) | 7.2 (6.6) | <0.001 |
| Platelets (K/μL) | 192 (98) | 190 (93) | 218 (89.5) | 0.007 |
| D-dimers (μg/mL) | 0.72 (0.63) | 0.69 (0.61) | 0.97 (0.77) | 0.011 |
| Fibrinogen (mg/dL) | 528 (181) | 516 (169) | 690 (165) | <0.001 |
| Creatinine (mg/dL) | 0.85 (0.25) | 0.85 (0.25) | 0.87 (0.23) | 0.349 |
| AST (U/L) | 35 (24) | 34 (22) | 48 (28) | 0.001 |
| ALT (U/L) | 29 (28) | 28 (25) | 46 (51) | 0.012 |
| γ-GT (U/L) | 33 (47) | 31 (42) | 62 (112) | 0.002 |
| LDH (U/L) | 322 (166) | 311 (156) | 450 (251) | <0.001 |
| CRP (mg/L) | 41 (74) | 39 (66) | 112 (77) | <0.001 |
| Ferritin (ng/mL) | 507 (618) | 477 (591) | 764 (797) | 0.014 |
| Drug treatment | ||||
| LMWH | 237 (98.3) | 215 (98.2) | 22 (100) | 1.000 |
| Dexamethasone | 194 (80.5) | 172 (78.5) | 22 (100) | 0.010 |
| Remdesivir | 185 (77.1) | 163 (74.8) | 22 (100) | 0.003 |
| Tocilizumab | 21 (8.7) | 7 (3.2) | 14 (63.6) | <0.001 |
| OR (95% CI) * | p-Value | |
|---|---|---|
| Male sex | 1.40 (0.50–3.97) | 0.522 |
| Age (years) | 1.06 (1.02–1.10) | 0.003 |
| Time from symptom onset (days) | 1.11 (0.96–1.28) | 0.148 |
| Hemoglobin (g/dL) | 1.11 (0.82–1.50) | 0.488 |
| WBCs (K/μL) | 1.13 (1.02–1.24) | 0.018 |
| Neutrophils (K/μL) | 1.26 (1.11–1.43) | <0.001 |
| Lymphocytes (K/μL) | 0.47 (0.17–1.25) | 0.128 |
| Neutrophil/lymphocyte ratio | 1.21 (1.10–1.34) | <0.001 |
| Platelets (K/μL) | 1.004 (1.000–1.008) | 0.053 |
| D-dimers (μg/mL) | 1.11 (0.97–1.26) | 0.123 |
| Fibrinogen (mg/dL) | 1.009 (1.005–1.014) | <0.001 |
| Creatinine (mg/dL) | 1.57 (0.36–6.79) | 0.548 |
| AST (U/L) | 1.01 (0.999–1.024) | 0.080 |
| ALT (U/L) | 1.005 (0.998–1.012) | 0.178 |
| γ-GT (U/L) | 1.010 (1.004–1.016) | 0.001 |
| LDH (U/L) | 1.007 (1.004–1.010) | <0.001 |
| CRP (mg/L) | 1.014 (1.008–1.020) | <0.001 |
| Ferritin (ng/mL) | 1.001 (1.000–1.001) | 0.030 |
| OR (95% CI) * | p-Value | |
|---|---|---|
| WBCs (K/μL) | 1.13 (1.02–1.25) | 0.019 |
| Neutrophils (K/μL) | 1.23 (1.08–1.41) | 0.002 |
| Neutrophil/lymphocyte ratio | 1.20 (1.08–1.33) | 0.001 |
| Fibrinogen (mg/dL) | 1.008 (1.004–1.013) | <0.001 |
| γ-GT (U/L) | 1.010 (1.003–1.016) | 0.004 |
| LDH (U/L) | 1.007 (1.004–1.010) | <0.001 |
| CRP (mg/L) | 1.012 (1.006–1.019) | <0.001 |
| Ferritin (ng/mL) | 1.000 (0.9999–1.001) | 0.129 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgakopoulou, V.E.; Vlachogiannis, N.I.; Basoulis, D.; Eliadi, I.; Georgiopoulos, G.; Karamanakos, G.; Makrodimitri, S.; Samara, S.; Triantafyllou, M.; Voutsinas, P.M.; et al. A Simple Prognostic Score for Critical COVID-19 Derived from Patients without Comorbidities Performs Well in Unselected Patients. J. Clin. Med. 2022, 11, 1810. https://doi.org/10.3390/jcm11071810
Georgakopoulou VE, Vlachogiannis NI, Basoulis D, Eliadi I, Georgiopoulos G, Karamanakos G, Makrodimitri S, Samara S, Triantafyllou M, Voutsinas PM, et al. A Simple Prognostic Score for Critical COVID-19 Derived from Patients without Comorbidities Performs Well in Unselected Patients. Journal of Clinical Medicine. 2022; 11(7):1810. https://doi.org/10.3390/jcm11071810
Chicago/Turabian StyleGeorgakopoulou, Vasiliki E., Nikolaos I. Vlachogiannis, Dimitrios Basoulis, Irene Eliadi, Georgios Georgiopoulos, Georgios Karamanakos, Sotiria Makrodimitri, Stamatia Samara, Maria Triantafyllou, Pantazis M. Voutsinas, and et al. 2022. "A Simple Prognostic Score for Critical COVID-19 Derived from Patients without Comorbidities Performs Well in Unselected Patients" Journal of Clinical Medicine 11, no. 7: 1810. https://doi.org/10.3390/jcm11071810