
Analysis of Perception, Reasons, and Motivations for COVID-19 Vaccination in People with Diabetes across Sub-Saharan Africa: A Mixed-Method Approach

 , , , , , ,
, , , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Approval
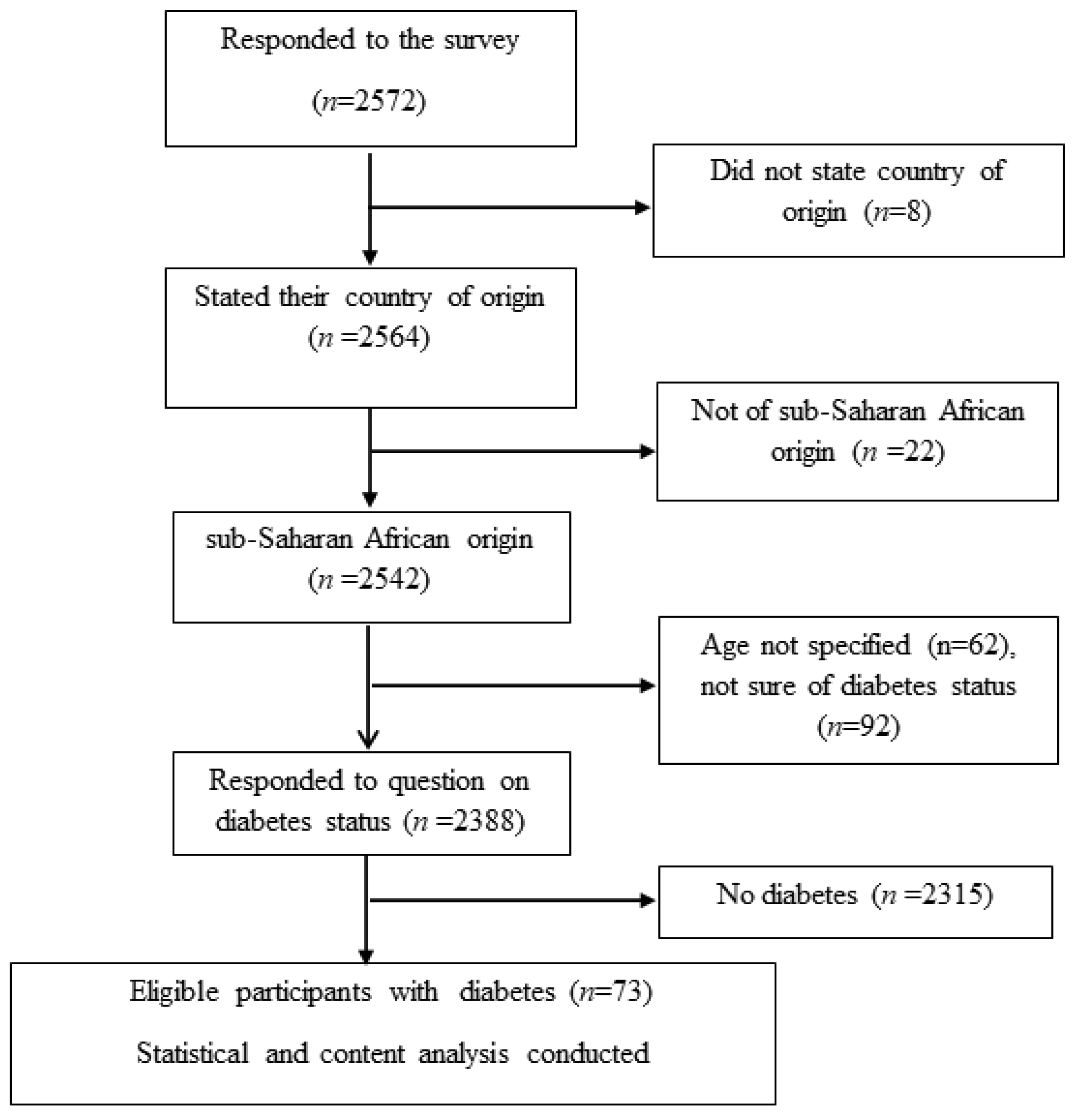
2.3. Participants
2.4. Data Collection
2.5. Qualitative Responses
2.6. Statistical Analysis
3. Results
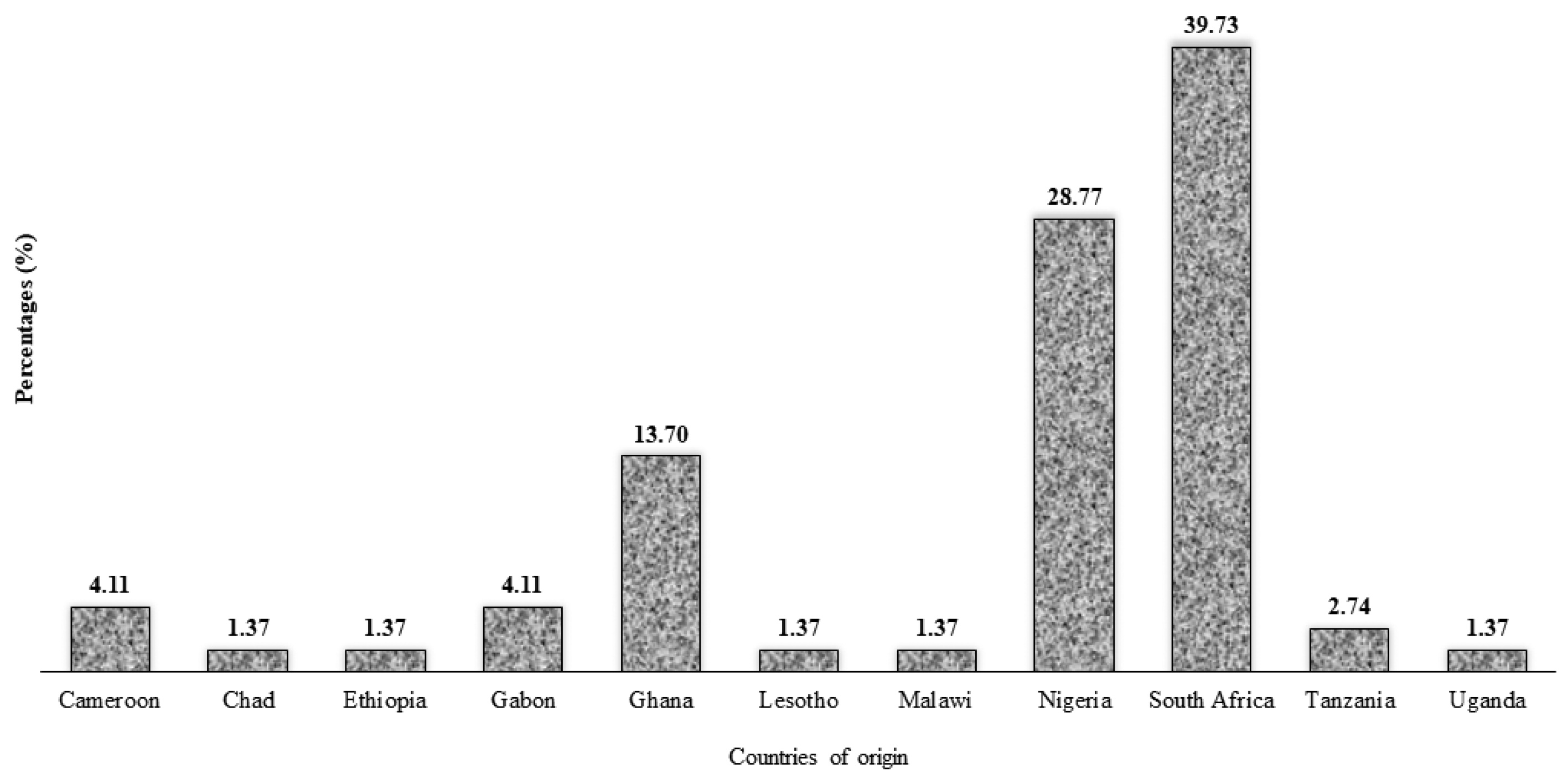
3.1. Characteristics of the Study Population
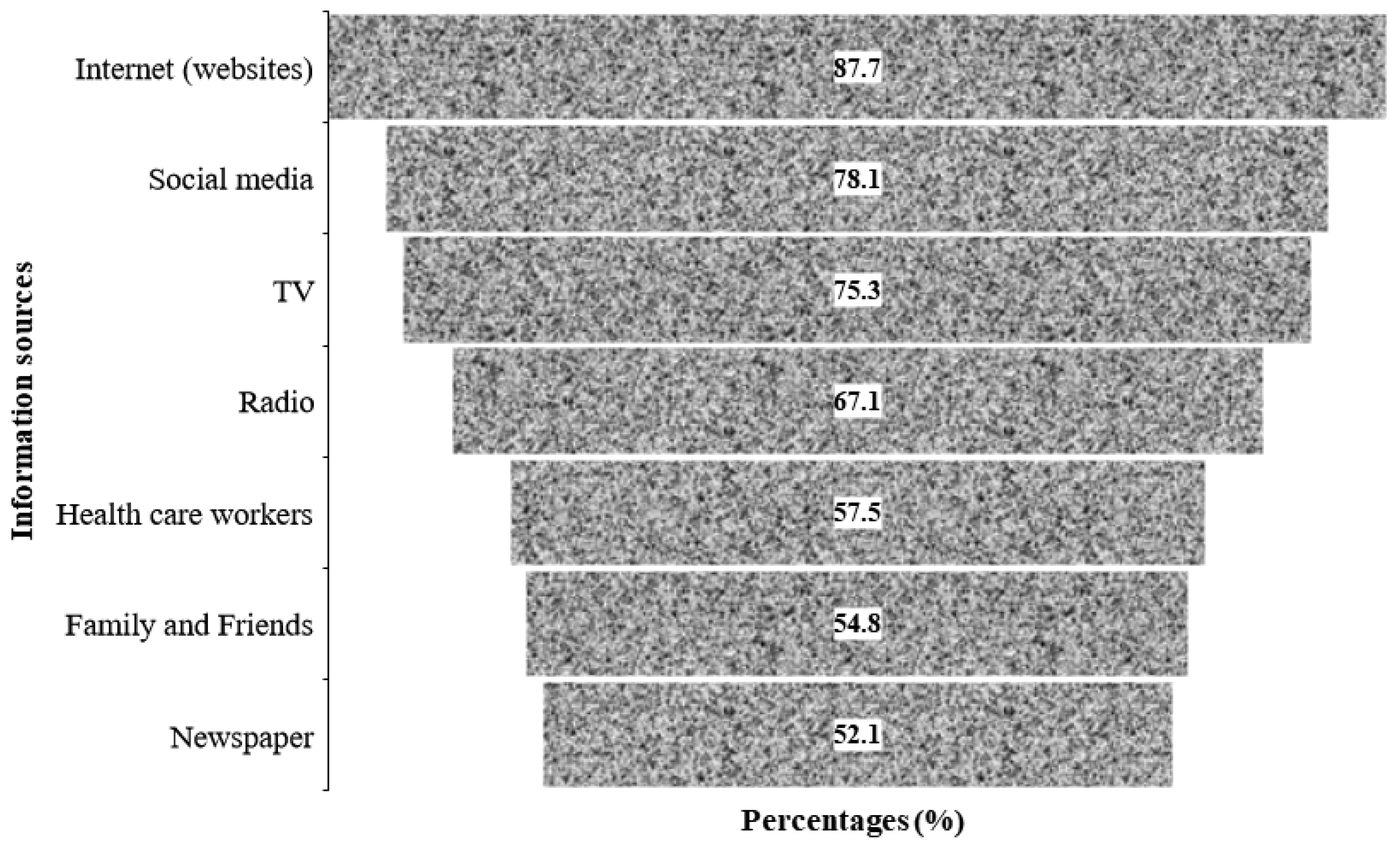
3.2. Information Related to COVID 19 and Vaccination Uptake
3.3. Association between Hesitancy or Refusal towards COVID-19 Vaccine and the Study Variables
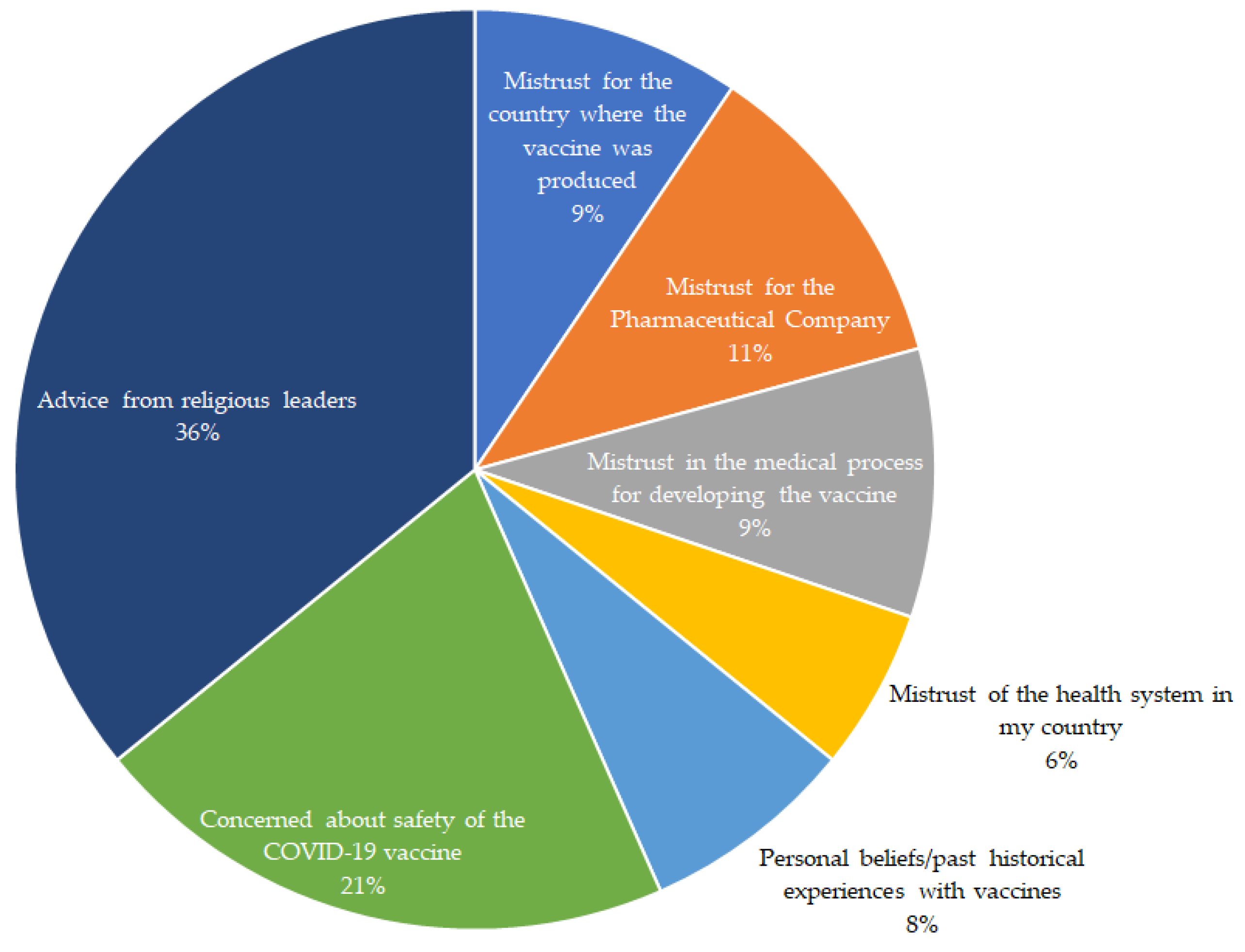
3.4. Reasons for COVID-19 Vaccine Hesitancy or Refusal among Participants
3.5. Factors That Would Encourage Uptake of Vaccination in People with DM
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atlas, D. International diabetes federation. In IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- Atlas, I.D. Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar]
- Kengne, A.P.; June-Rose McHiza, Z.; Amoah, A.G.; Mbanya, J.C. Cardiovascular diseases and diabetes as economic and developmental challenges in Africa. Prog. Cardiovasc. Dis. 2013, 56, 302–313. [Google Scholar] [CrossRef]
- Kengne, A.P.; Amoah, A.G.; Mbanya, J.C. Cardiovascular complications of diabetes mellitus in Sub-Saharan Africa. Circulation 2005, 112, 3592–3601. [Google Scholar] [CrossRef] [Green Version]
- Jakovljevic, M.B.; Milovanovic, O. Growing Burden of Non-Communicable Diseases in the Emerging Health Markets: The Case of BRICS. Front. Public Health 2015, 3, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Institute of Health and Welfare; Holdenson, Z. A Picture of Diabetes in Overseas-Born Australians; Australian Institute of Health and Welfare: Darlinghurst, Australia, 2003.
- Dzinamarira, T.; Dzobo, M.; Chitungo, I. COVID-19: A perspective on Africa’s capacity and response. J. Med. Virol. 2020, 92, 2465–2472. [Google Scholar] [CrossRef]
- Nwaeze, O.; Langsi, R.; Osuagwu, U.L.; Oloruntoba, R.; Ovenseri-Ogbomo, G.O.; Abu, E.K.; Charwe, D.D.; Ekpenyong, B.; Mashige, K.P.; Goson, P.C. Factors affecting willingness to comply with public health measures during the pandemic among sub-Sahara Africans. Afr. Health Sci. 2021, 21, 1629–1639. [Google Scholar] [CrossRef]
- Basak, P.; Abir, T.; Al Mamun, A.; Zainol, N.R.; Khanam, M.; Haque, M.R.; Milton, A.H.; Agho, K.E. A Global Study on the Correlates of Gross Domestic Product (GDP) and COVID-19 Vaccine Distribution. Vaccines 2022, 10, 266. [Google Scholar] [CrossRef]
- Bonora, E.; Fedeli, U.; Schievano, E.; Trombetta, M.; Saia, M.; Scroccaro, G.; Tacconelli, E.; Zoppini, G. SARS-CoV-2 and COVID-19 in diabetes mellitus. Population-based study on ascertained infections, hospital admissions and mortality in an Italian region with ~5 million inhabitants and ~250,000 diabetic people. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2612–2618. [Google Scholar] [CrossRef]
- Silverii, G.A.; Monami, M.; Cernigliaro, A.; Vigneri, E.; Guarnotta, V.; Scondotto, S.; Allotta, V.A.; Conti, M.; Giordano, C.; Mannucci, E. Are diabetes and its medications risk factors for the development of COVID-19? Data from a population-based study in Sicily. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 396–398. [Google Scholar] [CrossRef]
- Gao, Y.d.; Ding, M.; Dong, X.; Zhang, J.j.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.l.; Fu, W.; Li, W. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Conferenza Permanente per i Rapporti tra lo Stato, le Regioni e le Province Autonome di Trento e Bolzano. 2016, Volume 20. Available online: http://www.statoregioni.it/Documenti/DOC_044351_82%20CSR%20PUNTO (accessed on 20 March 2022).
- MacDonald, N. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Guaraldi, F.; Montalti, M.; Di Valerio, Z.; Mannucci, E.; Nreu, B.; Monami, M.; Gori, D. Rate and predictors of hesitancy toward SARS-CoV-2 vaccine among type 2 diabetic patients: Results from an Italian survey. Vaccines 2021, 9, 460. [Google Scholar] [CrossRef] [PubMed]
- Aldossari, K.K.; Alharbi, M.B.; Alkahtani, S.M.; Alrowaily, T.Z.; Alshaikhi, A.M.; Twair, A.A. COVID-19 vaccine hesitancy among patients with diabetes in Saudi Arabia. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102271. [Google Scholar] [CrossRef]
- Cooper, S.; van Rooyen, H.; Wiysonge, C.S. COVID-19 vaccine hesitancy in South Africa: How can we maximize uptake of COVID-19 vaccines? Expert Rev. Vaccines 2021, 20, 921–933. [Google Scholar] [CrossRef] [PubMed]
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19): Herd Immunity, Lockdowns and COVID-19; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Klekotka, R.B.; Mizgała, E.; Król, W. The etiology of lower respiratory tract infections in people with diabetes. Adv. Respir. Med. 2015, 83, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Alguwaihes, A.M.; Al-Sofiani, M.E.; Megdad, M.; Albader, S.S.; Alsari, M.H.; Alelayan, A.; Alzahrani, S.H.; Sabico, S.; Al-Daghri, N.M.; Jammah, A.A. Diabetes and COVID-19 among hospitalized patients in Saudi Arabia: A single-centre retrospective study. Cardiovasc. Diabetol. 2020, 19, 205. [Google Scholar] [CrossRef]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Pecorelli, S. Assessing COVID-19 vaccine literacy: A preliminary online survey. Hum. Vaccines Immunother. 2021, 17, 1304–1312. [Google Scholar] [CrossRef]
- Buzasi, K. Linguistic situation in twenty Sub-Saharan African countries: A survey-based approach. Afr. Stud. 2016, 75, 358–380. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes Metab. Res. Rev. 2020, 36, e3319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of theCytokine Storm’in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- CDC. People with Certain Medical Conditions; CDC: Atlanta, GA, USA, 2022. [Google Scholar]
- WHO. COVID-19 Advice for the Public: Getting Vaccinated; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- WHO. WHO Coronavirus (COVID-19) Dashboard; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- WHO. Africa’s COVID-19 Vaccine Uptake Increases by 15%; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Gregory, J.M.; Slaughter, J.C.; Duffus, S.H.; Smith, T.J.; LeStourgeon, L.M.; Jaser, S.S.; McCoy, A.B.; Luther, J.M.; Giovannetti, E.R.; Boeder, S. COVID-19 severity is tripled in the diabetes community: A prospective analysis of the pandemic’s impact in type 1 and type 2 diabetes. Diabetes Care 2021, 44, 526–532. [Google Scholar] [CrossRef] [PubMed]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn, L.A.; McAllister, D.A.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A. Risks of and risk factors for COVID-19 disease in people with diabetes: A cohort study of the total population of Scotland. Lancet Diabetes Endocrinol. 2021, 9, 82–93. [Google Scholar] [CrossRef]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: A whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- Chen, X.; Hu, W.; Ling, J.; Mo, P.; Zhang, Y.; Jiang, Q.; Ma, Z.; Cao, Q.; Deng, L.; Song, S.; et al. Hypertension and Diabetes Delay the Viral Clearance in COVID-19 Patients. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Cariou, B.; Hadjadj, S.; Wargny, M.; Pichelin, M.; Al-Salameh, A.; Allix, I.; Amadou, C.; Arnault, G.; Baudoux, F.; Bauduceau, B. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: The CORONADO study. Diabetologia 2020, 63, 1500–1515. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High rates of COVID-19 vaccine hesitancy and its association with conspiracy beliefs: A study in Jordan and Kuwait among other Arab countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; MacDonald, N.; Bocquier, A.; Peretti-Watel, P.; Verger, P. Underlying factors impacting vaccine hesitancy in high income countries: A review of qualitative studies. Expert Rev. Vaccines 2018, 17, 989–1004. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Alfageeh, E.I.; Alshareef, N.; Angawi, K.; Alhazmi, F.; Chirwa, G.C. Acceptability of a COVID-19 Vaccine among the Saudi Population. Vaccines 2021, 9, 226. [Google Scholar] [CrossRef]
- Hilverda, F.; Vollmann, M. The Role of Risk Perception in Students’ COVID-19 Vaccine Uptake: A Longitudinal Study. Vaccines 2021, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Allen, E.M.; Lee, H.Y.; Pratt, R.; Vang, H.; Desai, J.R.; Dube, A.; Lightfoot, E. Facilitators and barriers of cervical cancer screening and human papilloma virus vaccination among Somali refugee women in the United States: A qualitative analysis. J. Transcult. Nurs. 2019, 30, 55–63. [Google Scholar] [CrossRef]
- Wiley, K.E.; Massey, P.D.; Cooper, S.C.; Wood, N.J.; Ho, J.; Quinn, H.E.; Leask, J. Uptake of influenza vaccine by pregnant women: A cross-sectional survey. Med. J. Aust. 2013, 198, 373–375. [Google Scholar] [CrossRef] [Green Version]
- Dilley, S.E.; Peral, S.; Straughn, J.M., Jr.; Scarinci, I.C. The challenge of HPV vaccination uptake and opportunities for solutions: Lessons learned from Alabama. Prev. Med. 2018, 113, 124–131. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Lu, P.; Meador, S.; Hung, M.-C.; Kahn, K.; Hoehner, J.; Razzaghi, H.; Black, C.; Singleton, J.A. Comparison of COVID-19 Vaccination Coverage Estimates from the Household Pulse Survey, Omnibus Panel Surveys, and COVID-19 Vaccine Administration Data, United States, March 2021; CDC: Atlanta, GA, USA, 2021. [Google Scholar]
- Adane, M.; Ademas, A.; Kloos, H. Knowledge, attitudes, and perceptions of COVID-19 vaccine and refusal to receive COVID-19 vaccine among healthcare workers in northeastern Ethiopia. BMC Public Health 2022, 22, 128. [Google Scholar] [CrossRef]
- Katoto, P.D.M.C.; Parker, S.; Coulson, N.; Pillay, N.; Cooper, S.; Jaca, A.; Mavundza, E.; Houston, G.; Groenewald, C.; Essack, Z.; et al. Predictors of COVID-19 Vaccine Hesitancy in South African Local Communities: The VaxScenes Study. Vaccines 2022, 10, 353. [Google Scholar] [CrossRef]
- Ruijs, W.L.M.; Hautvast, J.L.A.; Kerrar, S.; van der Velden, K.; Hulscher, M.E.J.L. The role of religious leaders in promoting acceptance of vaccination within a minority group: A qualitative study. BMC Public Health 2013, 13, 511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viskupič, F.; Wiltse, D.L. The Messenger Matters: Religious Leaders and Overcoming COVID-19 Vaccine Hesitancy. PS Political Sci. Politics 2022, 55, 504–509. [Google Scholar] [CrossRef]
- Hjort, J.; Poulsen, J. The arrival of fast internet and employment in Africa. Am. Econ. Rev. 2019, 109, 1032–1079. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency n (%) |
|---|---|
| Demography | |
| Age category in years | |
| <35 | 10 (13.7) |
| ≥35 | 63 (86.3) |
| Sex | |
| Males | 48 (65.8) |
| Females | 25 (34.2) |
| Place of residenceǂ | |
| Local | 62 (84.9) |
| Diaspora | 9 (12.3) |
| SSA region of origin | |
| Central Africa | 7 (9.6) |
| East Africa | 5 (6.8) |
| Southern Africa | 30 (41.1) |
| West Africa | 31 (42.5) |
| Marital status | |
| Not married | 20 (27.4) |
| Married/de facto | 53 (72.6) |
| Highest level of education | |
| Secondary or less | 6 (8.2) |
| University/diploma | 35 (48.0) |
| Postgraduate (master’s/PhD) | 32 (43.8) |
| Employment statusǂ | |
| Unemployed | 14 (19.2) |
| Employed | 58 (79.5) |
| Religion | |
| Non-Christians | 16 (21.9) |
| Christians | 57 (78.1) |
| Occupationǂ | |
| Nonhealthcare sector | 48 (65.8) |
| Healthcare sector | 23 (31.5) |
| Smoking status | |
| Current smoker | 9 (12.3) |
| Ex-smoker | 11 (15.1) |
| Nonsmoker | 53 (72.6) |
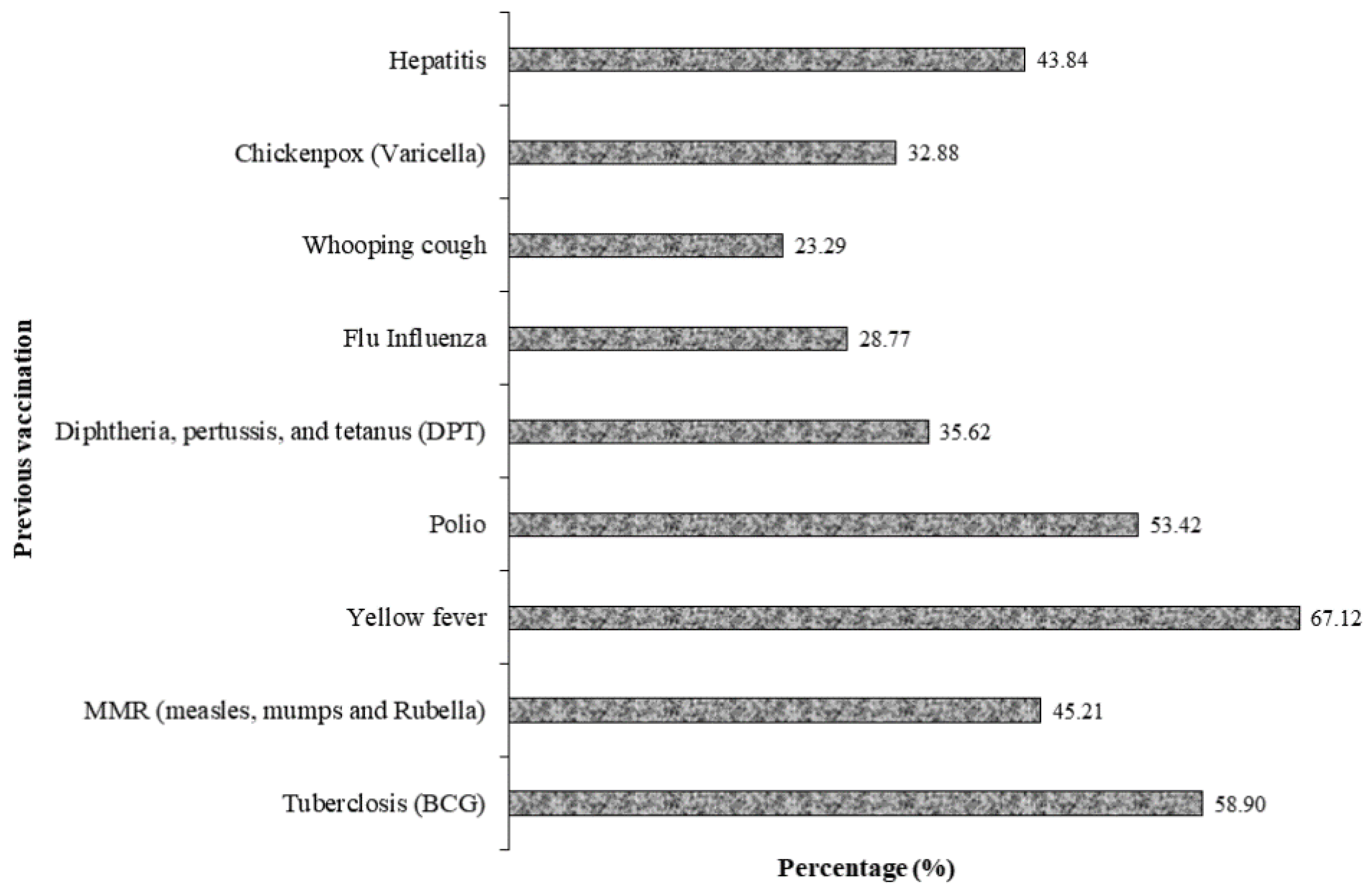
| Previous vaccination | |
| Yes | 64 (87.7) |
| No/not sure | 9 (12.3) |
| Variables | Frequency n (%) |
|---|---|
| Any chronic disease ǃ | |
| Yes | 46 (63.0) |
| No | 27 (37.0) |
| Asthma ǂ | |
| Yes | 6 (8.2) |
| No | 59 (80.8) |
| Hypertension ǂ | |
| Yes | 34 (46.6) |
| No | 36 (49.3) |
| Sickle cell anemia ǂ | |
| Yes | 1 (1.4) |
| No | 67 (91.7) |
| Obesity ǂ | |
| Yes | 15 (20.5) |
| No | 55 (75.3) |
| Any heart condition ǂ | |
| Yes | 8 (11.0) |
| No | 62 (85.0) |
| Kidney disease ǂ | |
| Yes | 2 (2.7) |
| No | 66 (91.8) |
| Variables | Frequency (%) |
|---|---|
| Awareness of COVID-19 vaccination | |
| Symptom of COVID-19 | |
| Yes | 47 (64.4) |
| No/not sure | 26 (35.6) |
| Tested for COVID-19 | |
| Yes | 34 (46.6) |
| No | 38 (52.1) |
| Tested positive for COVID-19 ǂ | |
| Yes | 14 (41.2) |
| No | 20 (58.8) |
| Aware that COVID-19 vaccines have been developed | |
| Yes | 71 (97.3) |
| No | 1 (1.4) |
| Have you been vaccinated against COVID-19 | |
| Yes | 5 (6.8) |
| No | 67 (91.8) |
| Will you be willing to take COVID-19 vaccine when it becomes available in your country? | |
| Yes (willing) | 48 (65.8) |
| No/not sure (refusal/hesitancy) | 19 (26.0) |
| Risk perception of COVID-19 vaccination | |
| Do you think COVID-19 virus is real | |
| Yes | 68 (93.2) |
| No/not sure | 5 (6.8) |
| COVID-19 vaccine can prevent COVID-19 infection and its complications | |
| Strongly agree | 17 (23.3) |
| Agree | 25 (34.2) |
| Don’t know | 15 (20.5) |
| Disagree | 8 (11.0) |
| Strongly disagree | 1 (1.4) |
| Perception of risk of dying from COVID-19 infection | |
| Very high | 13 (17.8) |
| High | 25 (34.2) |
| Unlikely | 7 (9.6) |
| Low | 18 (24.7) |
| Very low | 8 (11.0) |
| Perception of risk of becoming infected | |
| Very high | 12 (16.4) |
| High | 35 (47.9) |
| Unlikely | 8 (11.0) |
| Low | 16 (21.9) |
| Very low | 2 (2.7) |
| Variables | No/Not Sure | Yes | p-Value |
|---|---|---|---|
| Gender | |||
| Male | 7 (14.6) | 36 (75.0) | 0.008 |
| Female | 12 (48.0) | 12 (48.0) | |
| SSA region of origin | |||
| Central Africa | 2 (28.6) | 5 (71.4) | 0.045 |
| East Africa | 2 (40.0) | 3 (60.0) | |
| Southern Africa | 5 (16.7) | 25 (83.3) | |
| West Africa | 10 (32.3) | 15 (48.4) | |
| Place of residence | |||
| Diaspora | 3 (33.3) | 3 (33.3) | 0.009 |
| Local | 15 (24.2) | 44 (71.0) | |
| Have you been tested for COVID-19? | 7 (20.6) | 26 (76.5) | 0.006 |
| Are you concerned about the vaccine safety? | 11 (64.7) | 5 (29.4) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osuagwu, U.L.; Langsi, R.; Ovenseri-Ogbomo, G.; Mashige, K.P.; Abu, E.K.; Envuladu, E.A.; Goson, P.C.; Ekpenyong, B.N.; Oloruntoba, R.; Miner, C.A.; et al. Analysis of Perception, Reasons, and Motivations for COVID-19 Vaccination in People with Diabetes across Sub-Saharan Africa: A Mixed-Method Approach. Int. J. Environ. Res. Public Health 2022, 19, 7875. https://doi.org/10.3390/ijerph19137875
Osuagwu UL, Langsi R, Ovenseri-Ogbomo G, Mashige KP, Abu EK, Envuladu EA, Goson PC, Ekpenyong BN, Oloruntoba R, Miner CA, et al. Analysis of Perception, Reasons, and Motivations for COVID-19 Vaccination in People with Diabetes across Sub-Saharan Africa: A Mixed-Method Approach. International Journal of Environmental Research and Public Health. 2022; 19(13):7875. https://doi.org/10.3390/ijerph19137875
Chicago/Turabian StyleOsuagwu, Uchechukwu Levi, Raymond Langsi, Godwin Ovenseri-Ogbomo, Khathutshelo Percy Mashige, Emmanuel Kwasi Abu, Esther Awazzi Envuladu, Piwuna Christopher Goson, Bernadine Nsa Ekpenyong, Richard Oloruntoba, Chundung Asabe Miner, and et al. 2022. "Analysis of Perception, Reasons, and Motivations for COVID-19 Vaccination in People with Diabetes across Sub-Saharan Africa: A Mixed-Method Approach" International Journal of Environmental Research and Public Health 19, no. 13: 7875. https://doi.org/10.3390/ijerph19137875