
Thermal Perception and Physiological Responses under Different Protection States in Indoor Crowded Spaces during the COVID-19 Pandemic in Summer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
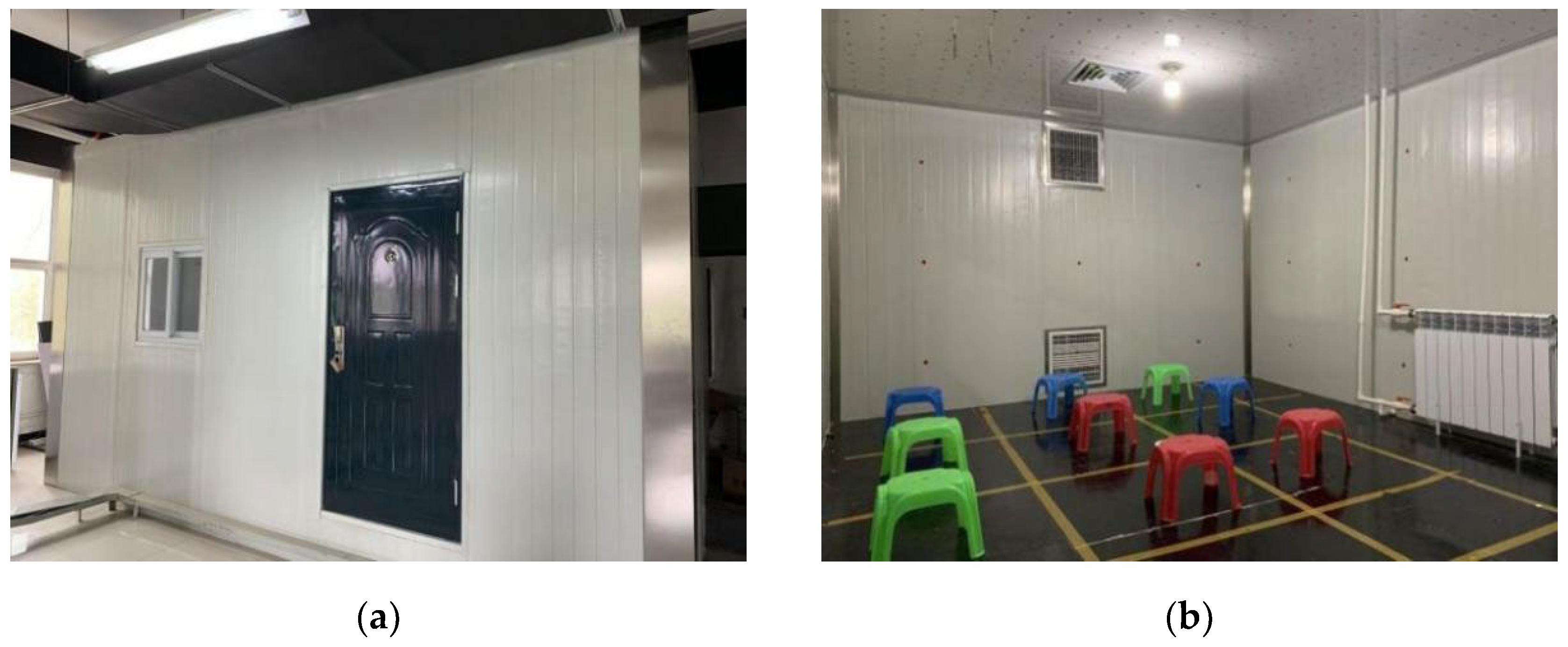
2.1. Human Subjects
2.2. Measurements
2.2.1. Environmental Measurements
2.2.2. Physiological Measurements
2.2.3. Subjective Measurements
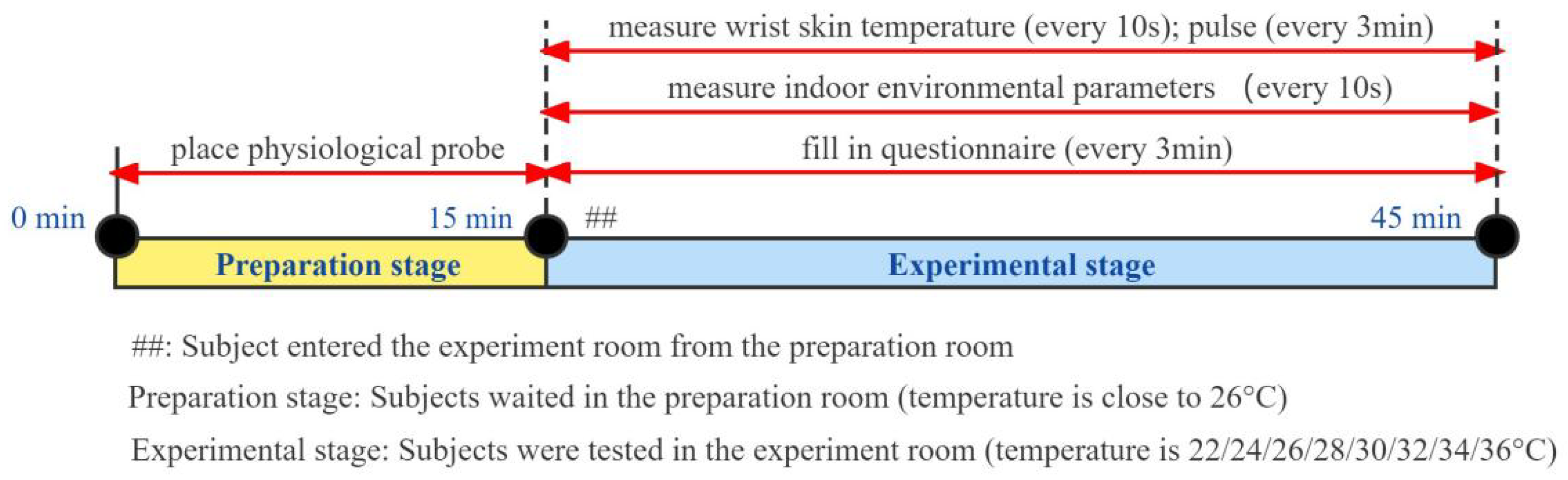
2.3. Experiment Procedure
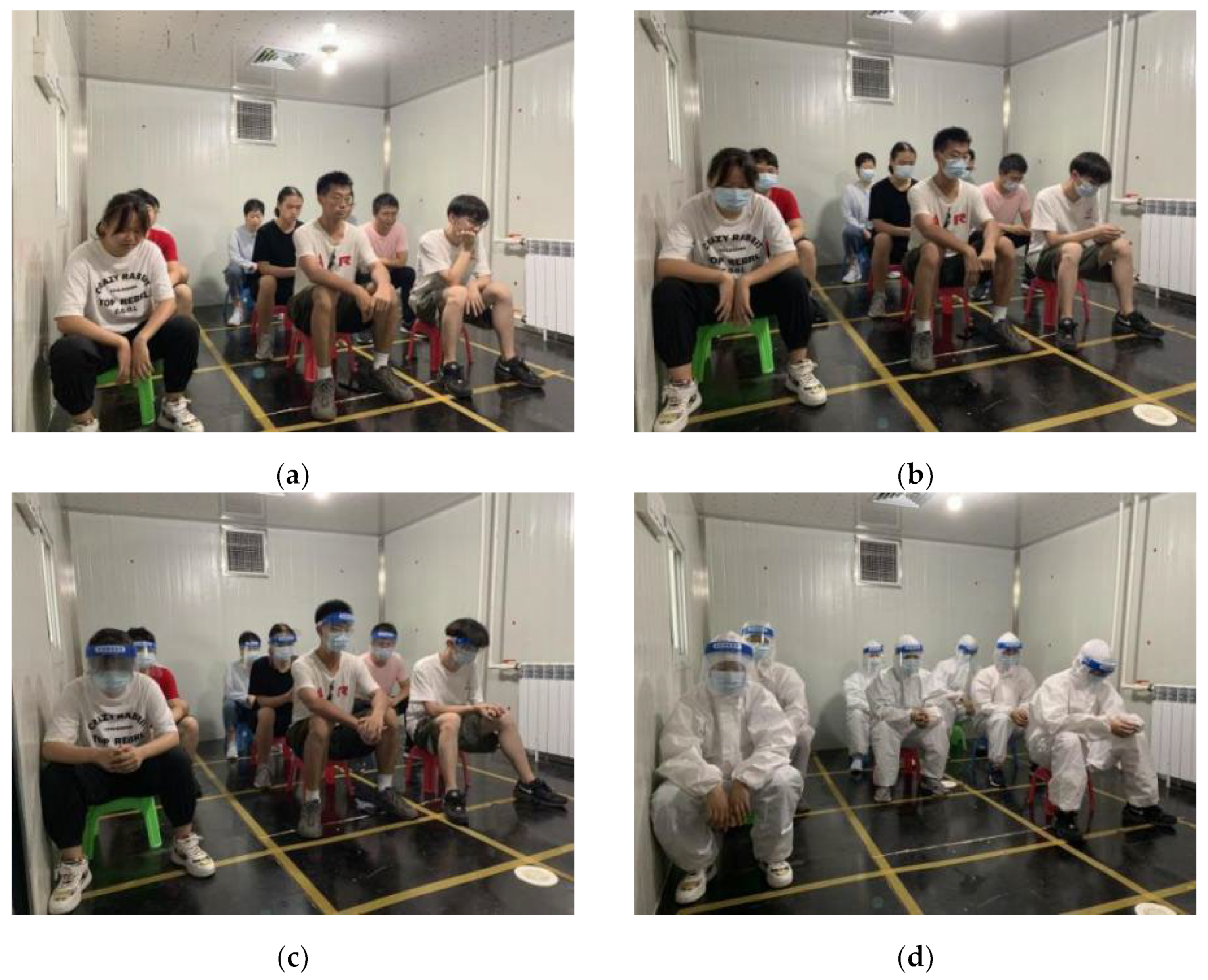
2.4. Protective States
2.5. Statistical Analysis
3. Results
3.1. Subjective Perception
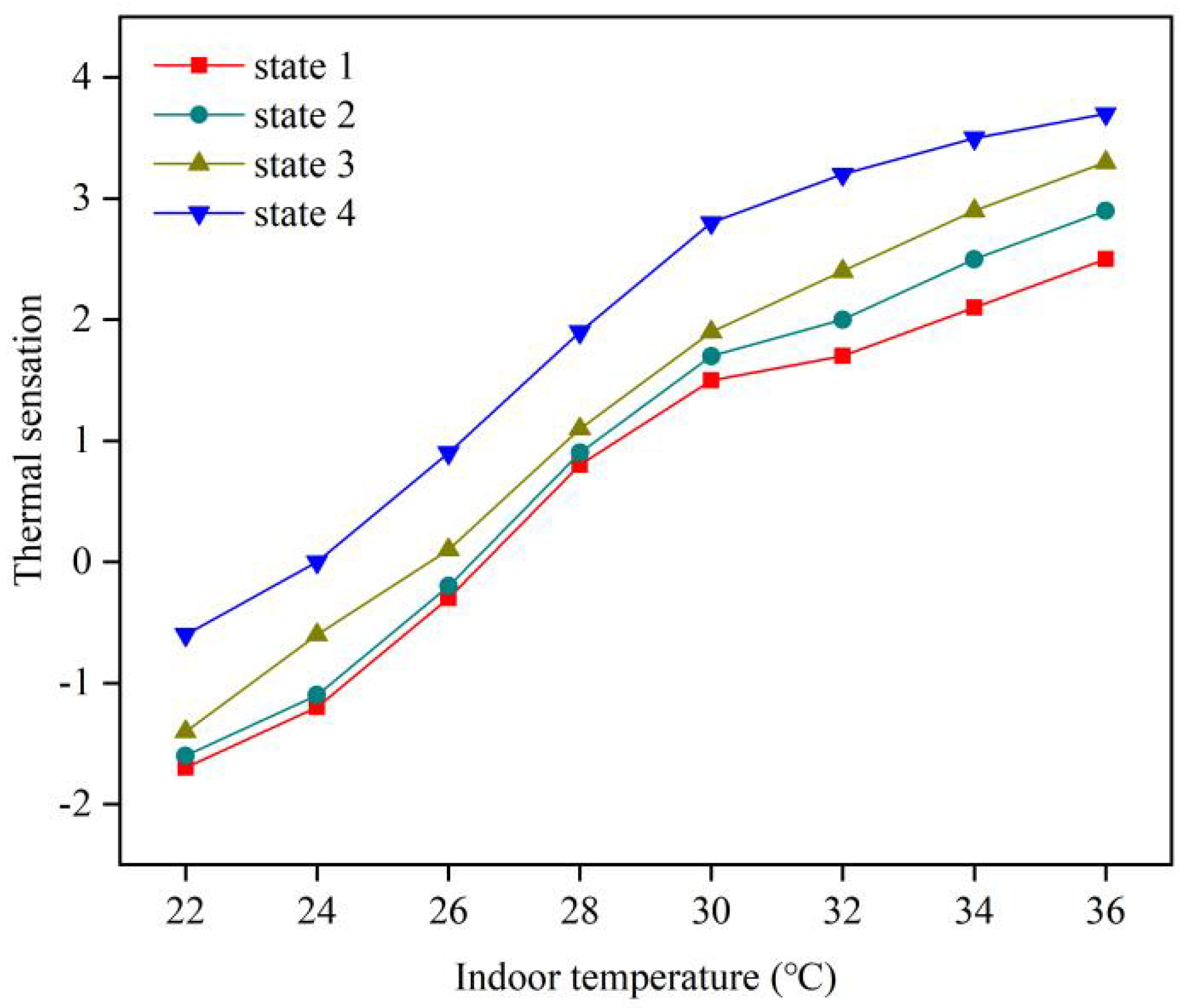
3.1.1. Thermal Sensation
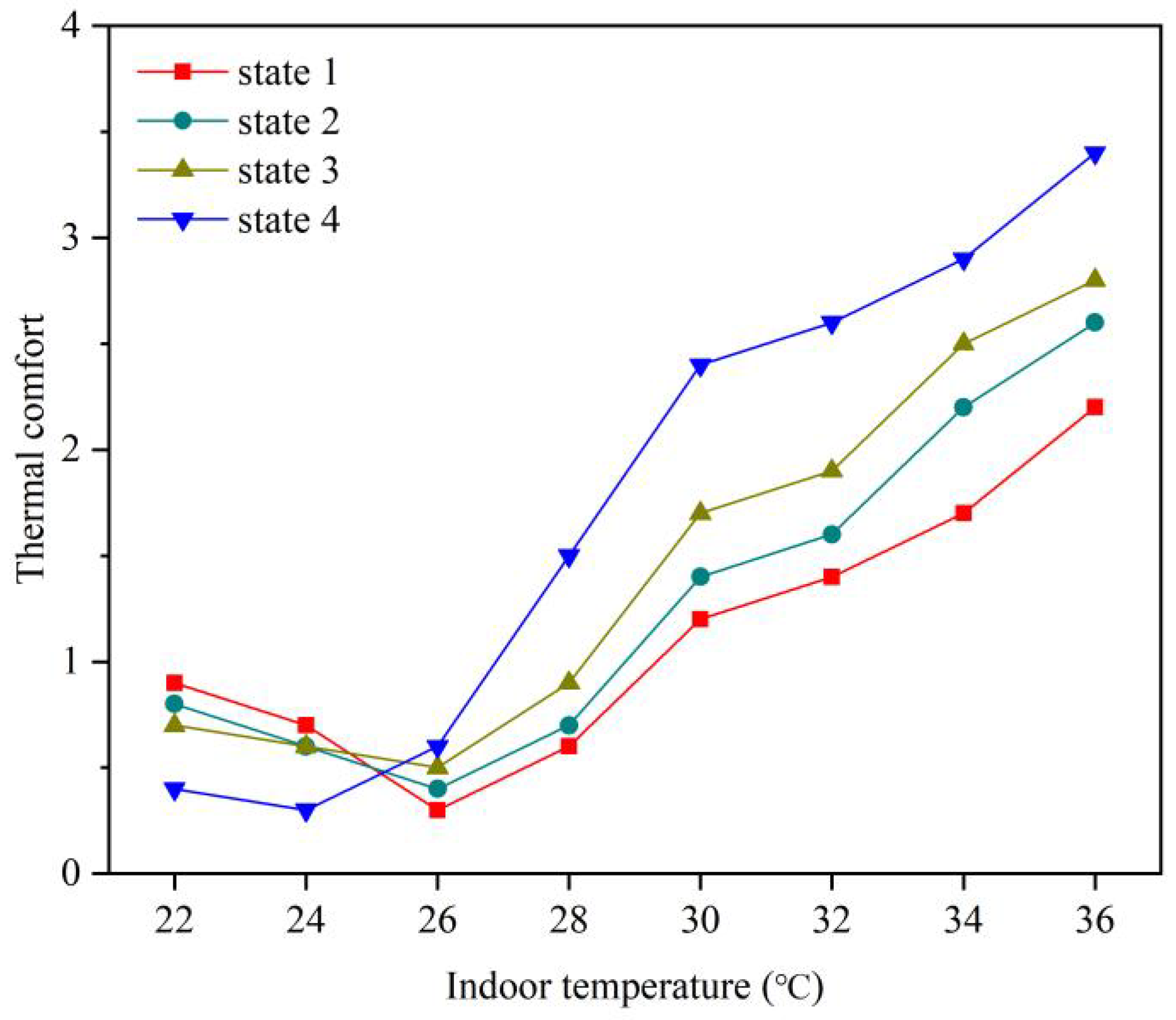
3.1.2. Thermal Comfort
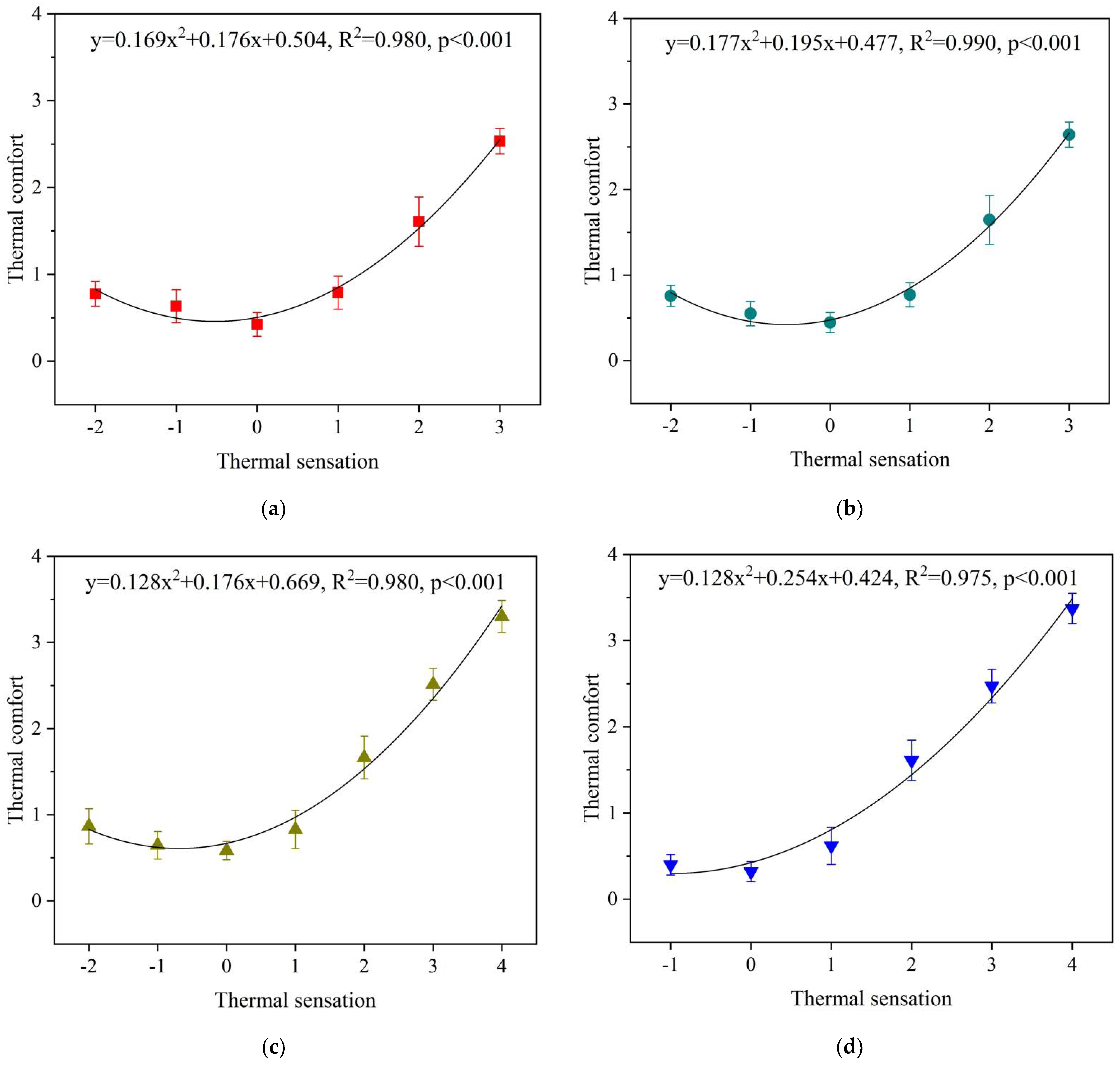
3.1.3. The Relation between Thermal Sensation and Thermal Comfort
3.2. Physiological Responses
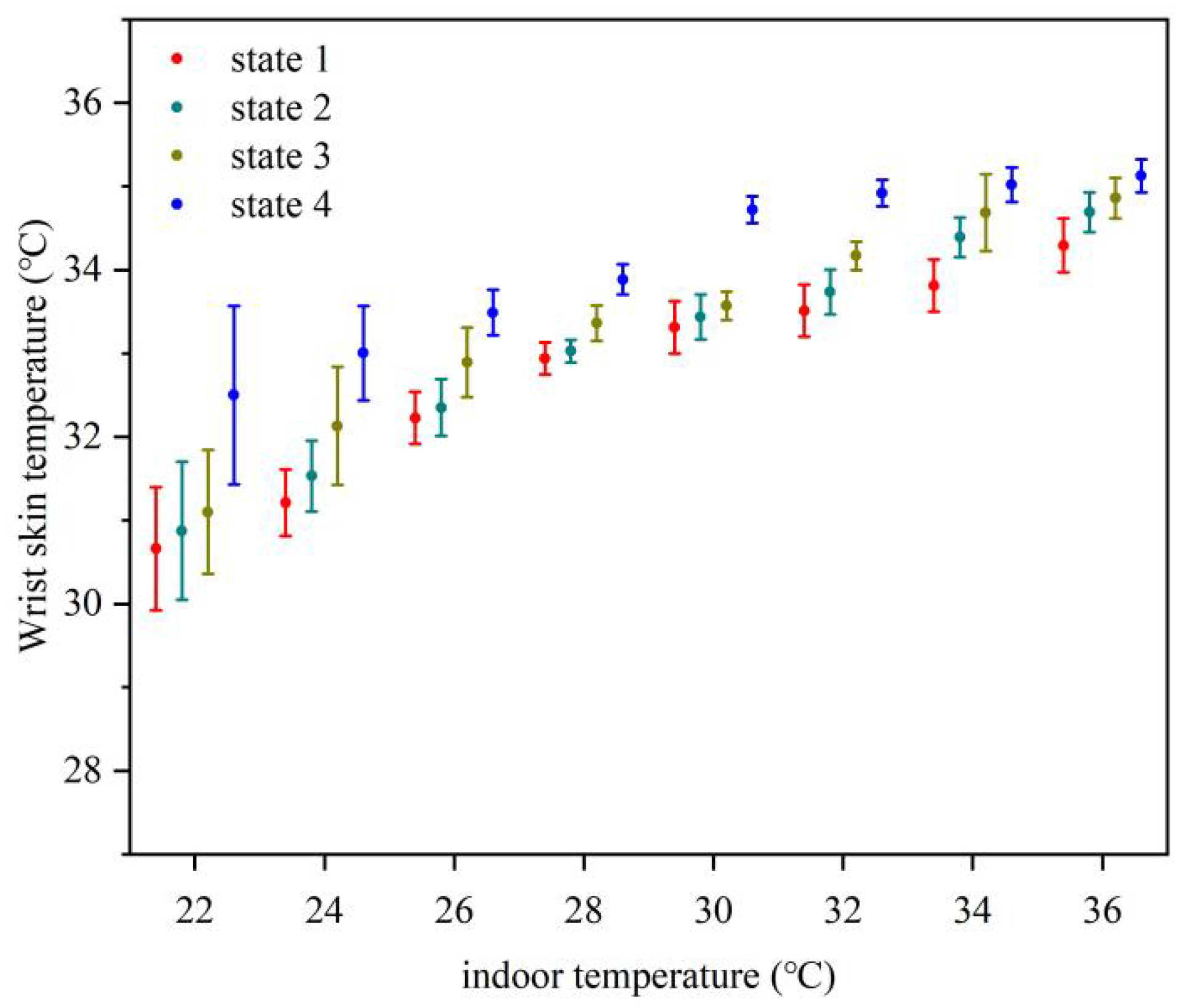
3.2.1. Wrist Skin Temperature
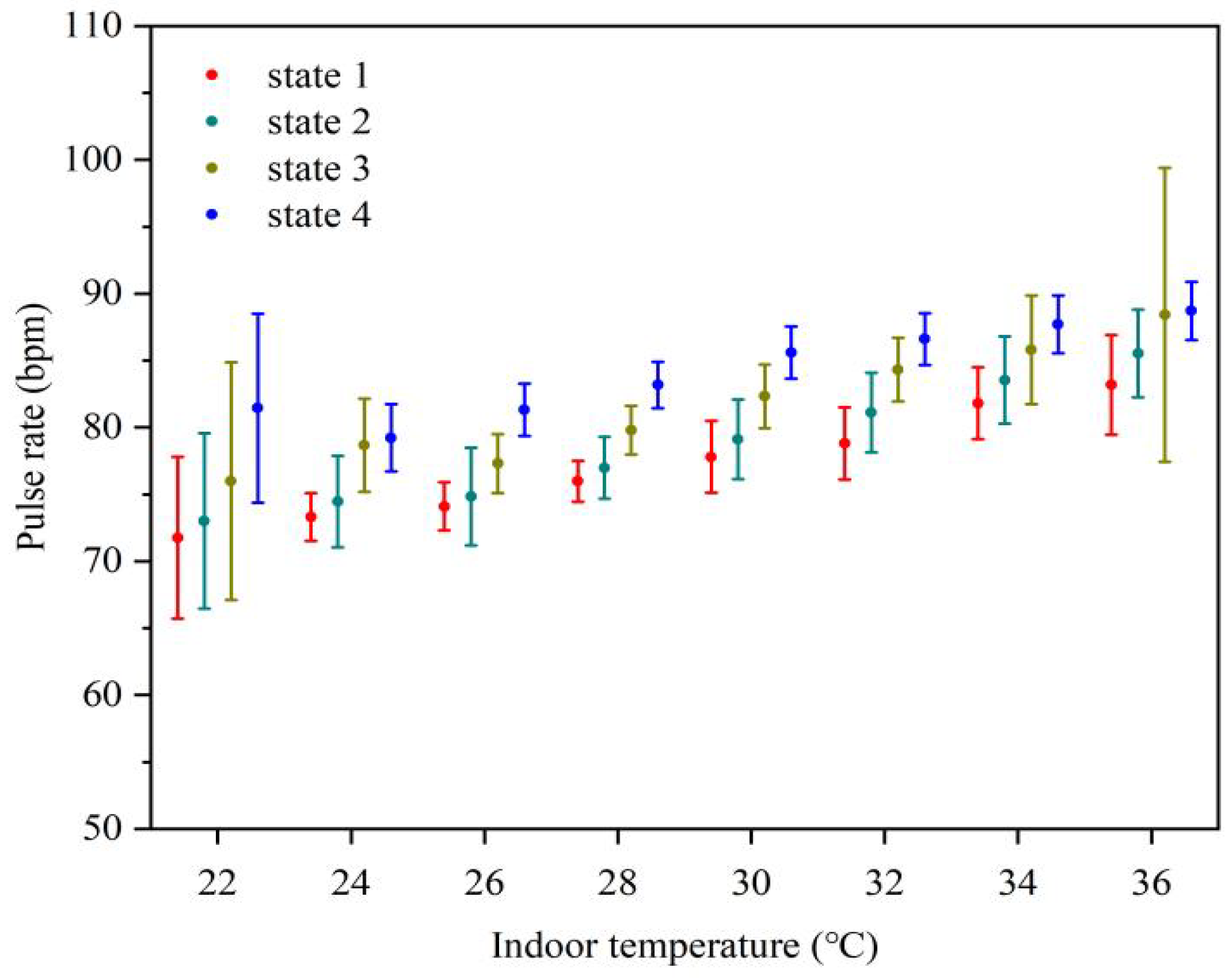
3.2.2. Pulse Rate
3.3. Relationship between Physiological Parameters and Thermal Sensation
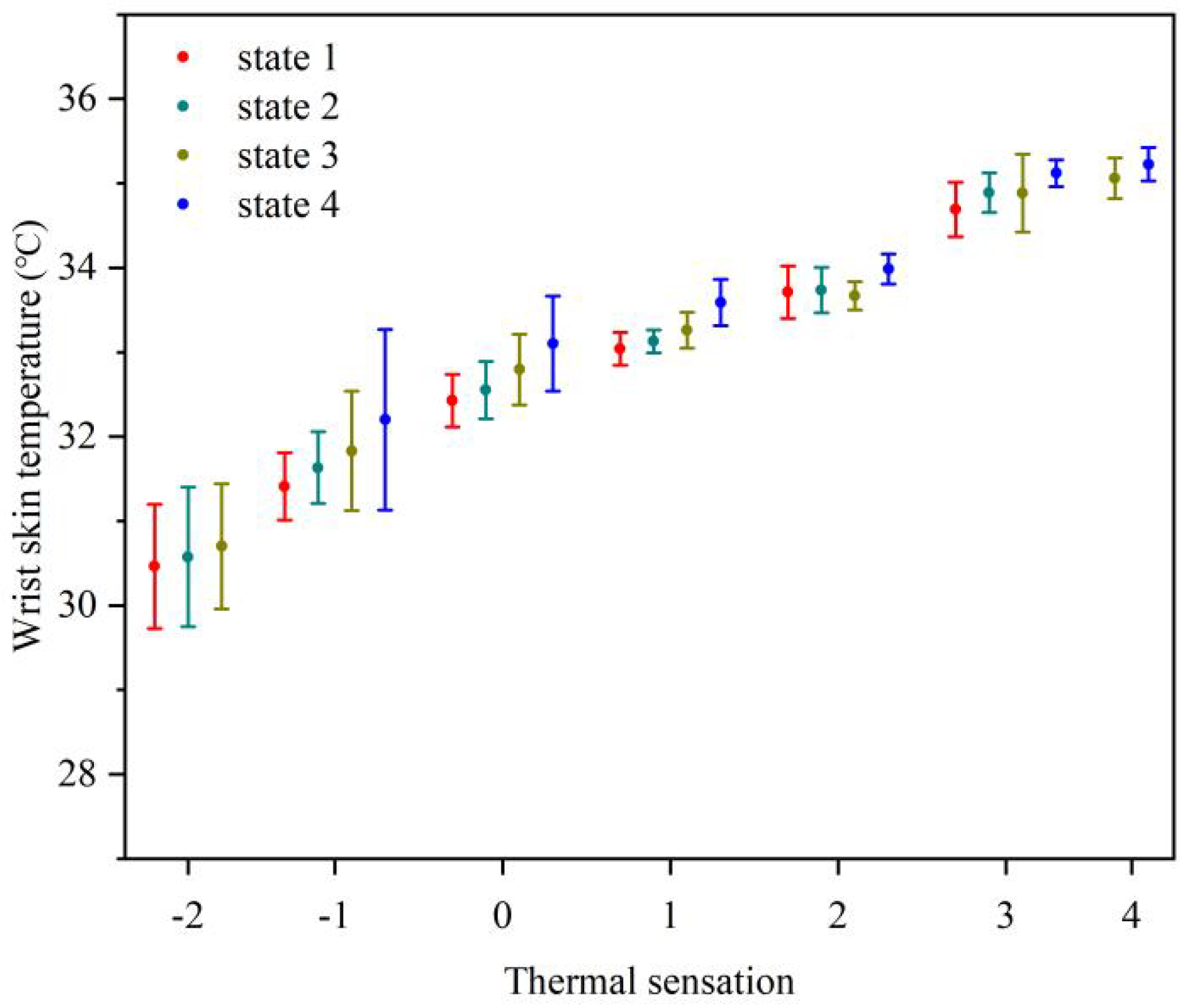
3.3.1. Relationship between Wrist Skin Temperature and Thermal Sensation
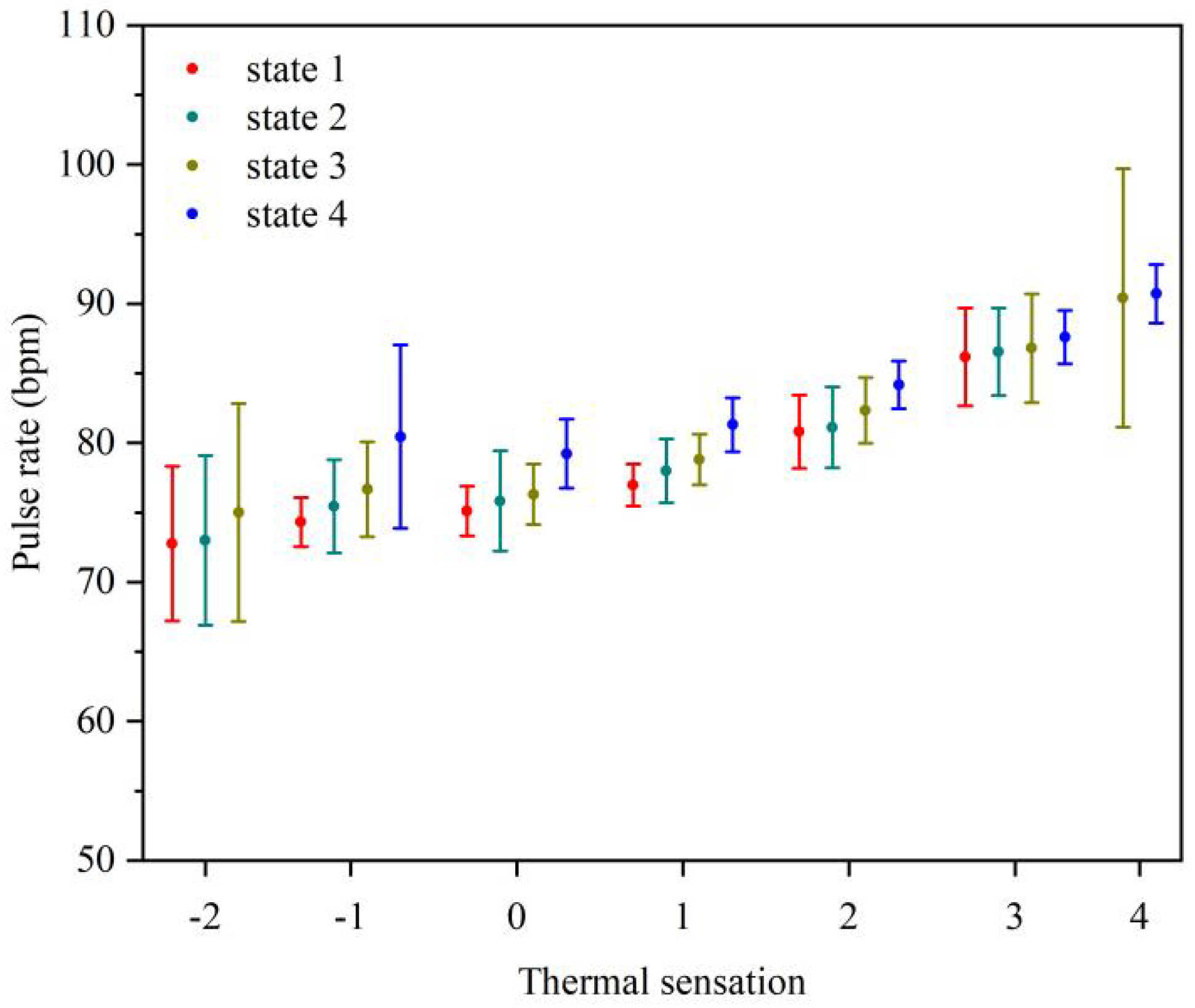
3.3.2. Relationship between Pulse Rate and Thermal Sensation
3.3.3. Thermal Sensation Estimation Model
- : The thermal sensation vote, which is used to evaluate the degree of human thermal sensation;
- : The average temperature of wrist skin (°C);
- : the pulse rate (bpm).
- : The standardized regression coefficients;
- : The standard deviation of
- : The standard deviation of
- : Independent variable;
- : Dependent variable;
- : The unit influence of on ;
- : The total number of observations sets.
3.4. Discussion
4. Conclusions
- (1)
- Medical protective clothing has the most obvious effect in blocking heat exchange between human body and environment. The thermal sensation in state 4 was significantly higher (p < 0.05) than that in the other three states. When the indoor temperature was 22–24 °C, the thermal comfort in state 4 was lower than that in other states. However, when the indoor temperature was 26–36 °C, the thermal comfort in state 4 was significantly higher than that in other states. At low temperature (22–28 °C), masks had little effect on human thermal perception. The thermal perception in state 1 was basically the same as those in state 2.
- (2)
- The thermal sensation under the four protective states increased with the increase of indoor temperature, and the thermal comfort first decreased and then increased.
- (3)
- As the indoor temperature increased from 22 °C to 36 °C, wrist skin temperature and pulse rate gradually increased under different protection states. In addition, at the same room temperature, the average wrist skin temperature and average pulse rate under different protection states increased with the strengthening of protection state.
- (4)
- The thermal sensation estimation model was established by using multiple linear regression models with wrist skin temperature and pulse rate as variables. Among all of the models, the thermal sensation estimation model in state 1 showed the highest accuracy, and the adjusted R2 was above 82% in the remaining three protection states. Moreover, the RMSE of all models were less than 1, indicating that the thermal sensation estimation model had a good prediction effect.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.who.int/zh/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19-how-is-it-transmitted (accessed on 30 April 2021).
- Felter, C.; Bussemaker, N. Which Countries Are Requiring Face Masks? Council on Foreign Relations: New York, NY, USA, 2020. [Google Scholar]
- Ahmad, A.; Garhwal, S.; Ray, S.K. The Number of Confirmed Cases of Covid-19 by using Machine Learning: Methods and Challenges. Arch. Comput. Methods Eng. 2020, 28, 1–9. [Google Scholar] [CrossRef]
- Zender-Wiercz, E.; Telejko, M.; Galiszewska, B. Influence of Masks Protecting against SARS-CoV-2 on Thermal Comfort. Energies 2021, 14, 3315. [Google Scholar] [CrossRef]
- Zhang, R.; Liu, J.; Zhang, L. The distorted power of medical surgical masks for changing the human thermal psychology of indoor personnel in summer. Indoor Air 2021, 31, 1645–1656. [Google Scholar] [CrossRef]
- Tang, T.; Zhu, Y.; Zhou, X. Investigation of the effects of face masks on thermal comfort in Guangzhou, China. Build. Environ. 2022, 214, 108932. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Jun, L.I.; Wang, G.H. Thermal Comfort Properties of Nonwovens Used in Medical Protective Clothing. J. Donghua Univ. (Nat. Sci.) 2006, 6, 116–119+133. [Google Scholar]
- Bongers, C.C.; Korte, J.Q.D.; Catoire, M. Infographic. Cooling strategies to attenuate PPE-induced heat strain during the COVID-19 pandemic. Br. J. Sports Med. 2020, 55, 69–70. [Google Scholar] [CrossRef]
- Kuklane, K.; Lundgren, K.; Gao, C. Ebola: Improving the Design of Protective Clothing for Emergency Workers Allows Them to Better Cope with Heat Stress and Help to Contain the Epidemic. Ann. Occup. Hyg. 2015, 59, 258–261. [Google Scholar]
- Troynikov, O.; Nawaz, N.; Watson, C. Medical protective clothing. Prot. Cloth. 2014, 20, 192–224. [Google Scholar]
- Zhao, M.; Gao, C.; Li, J. Effects of two cooling garments on post-exercise thermal comfort of female subjects in the heat. Fibers Polym. 2015, 16, 1403–1409. [Google Scholar] [CrossRef]
- Loibner, M.; Hagauer, S.; Schwantzer, G. Limiting factors for wearing personal protective equipment (PPE) in a health care environment evaluated in a randomised study. PLoS ONE 2019, 14, e0210775. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Facial Skin Temperature and Discomfort When Wearing Protective Face Masks: Thermal Infrared Imaging Evaluation and Hands Moving the Mask. Int. J. Environ. Res. Public Health 2020, 17, 4624. [Google Scholar] [CrossRef]
- Shi, D.; Song, J.; Du, R. Dual challenges of heat wave and protective facemask-induced thermal stress in Hong Kong. Build. Environ. 2021, 206, 108317. [Google Scholar] [CrossRef]
- Arens, E.A.; Zhang, H. The skin’s role in human thermoregulation and comfort. Therm. Moisture Transp. Fibrous Mater. 2006, 560–602. [Google Scholar] [CrossRef] [Green Version]
- Charkoudian, N. Skin blood flow in adult human thermoregulation: How it works, when it does not, and why. Mayo Clin. Proc. 2003, 78, 603–612. [Google Scholar] [CrossRef] [Green Version]
- Fanger, P.O. Thermal Comfort, Analysis and Application in Environmental Engineering; Danish Technical Press: Copenhagen, Denmark, 1970. [Google Scholar]
- Leblanc, J.; Blais, B.; Barabé, B. Effects of temperature and wind on facial temperature, heart rate, and sensation. J. Appl. Physiol. 1976, 40, 127–131. [Google Scholar] [CrossRef]
- Xiong, J.; Lian, Z.; Zhou, X.; You, J.; Lin, Y. Potential indicators for the effect of temperature steps on human health and thermal comfort. Energy Build. 2016, 113, 87–98. [Google Scholar] [CrossRef]
- Guy, G.P., Jr.; Lee, F.C.; Sunshine, G. Association of State-Issued Mask Mandates and Allowing On-Premises Restaurant Dining with County-Level COVID-19 Case and Death Growth Rates—United States, March 1–December 31, 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 350–354. [Google Scholar] [CrossRef]
- Bo, Y.; Guo, C.; Lin, C. Effectiveness of non-pharmaceutical interventions on COVID-19 transmission in 190 countries from 23 January to 13 April 2020. Int. J. Infect. Dis. 2021, 102, 247–253. [Google Scholar] [CrossRef]
- Eikenberry, S.E.; Mancuso, M.; Iboi, E. To mask or not to mask: Modeling the potential for face mask use by the general public to curtail the COVID-19 pandemic. Infect. Dis. Model 2020, 5, 293–308. [Google Scholar] [CrossRef]
- Standard 55-2017; Thermal Environmental Conditions for Human Occupancy. ASHRAE: Peachtree Corners, GA, USA, 2017.
- Choi, J.H.; Yeom, D. Study of data-driven thermal sensation prediction model as a function of local body skin temperatures in a built environment. Build. Environ. 2017, 121, 130–147. [Google Scholar] [CrossRef]
- Chaudhuri, T.; Zhai, D.; Soh, Y.C. Thermal comfort prediction using normalized skin temperature in a uniform built environment. Energy Build. 2018, 159, 426–440. [Google Scholar] [CrossRef]
- Chaudhuri, T.; Chai, Y.S.; Li, H.; Xie, L. Machine learning driven personal comfort prediction by wearable sensing of pulse rate and skin temperature. Build. Environ. 2020, 170, 106615. [Google Scholar] [CrossRef]
- Chaudhuri, T.; Zhai, D.; Chai, Y.S.; Li, H.; Xie, L. Random forest based thermal comfort prediction from gender-specific physiological parameters using wearable sensing technology. Energy Build. 2018, 166, 391–406. [Google Scholar] [CrossRef]
- ISO 10551; Ergonomics of the Thermal Environment. Assessment of the Influence of the Thermal Environment Using Subjective Judgment Scales. International Organization for Standardization: Geneva, Switzerland, 1995.
- ASHRAE. Data and Measurements in Thermal Comfort, American Society of Heating, Refrigerating and Air-Conditioning Engineers; ASHRAE: Atlanta, GA, USA, 2013; Chapter 9. [Google Scholar]
- Choi, J.H.; Yeom, D. Investigation of the relationships between thermal sensations of local body areas and the whole body in an indoor built environment. Energy Build. 2017, 149, 204–215. [Google Scholar] [CrossRef]
- Choi, J.H.; Loftness, V. Investigation of human body skin temperatures as a bio-signal to indicate overall thermal sensations. Build. Environ. 2012, 58, 258–269. [Google Scholar] [CrossRef]
- Revel, G.; Arnesano, M.; Pietroni, F. Integration of Real-Time metabolic rate measurement in a Low-Cost tool for the thermal comfort monitoring in all environments. In Ambient Assisted Living; Springer: Cham, Switzerland, 2015; pp. 101–110. [Google Scholar]
- Green, J.A. The heart rate method for estimating metabolic rate: Review and recommendations. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2011, 158, 287–304. [Google Scholar] [CrossRef]
- Butler, P.J.; Green, J.A.; Boyd, I.L. Measuring metabolic rate in the field: The pros and cons of the doubly labelled water and heart rate methods. Funct. Ecol. 2004, 18, 168–183. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Count | Age (Years) | Height (cm) | Weight (kg) | BMI 0 (kg/m2) | Icl 1 (clo) |
|---|---|---|---|---|---|---|
| Male | 7 | 22.6 ± 1.9 | 177.4 ± 5.7 | 67.6 ± 8.2 | 21.5 ± 2.6 | 0.44 ± 0.2 |
| Female | 3 | 22.7 ± 1.7 | 161.7 ± 1.7 | 54.5 ± 8.4 | 20.8 ± 2.9 | 0.46 ± 0.1 |
| Parameter | Model | Specifications |
|---|---|---|
| Environmental measurements | ||
| Air temperature | UX100-003 | Accuracy: ±0.21 °C/(0–50) °C, Range: (−20–70) °C |
| Relative humidity | UX100-003 | Accuracy: ±3.5%, Range: (15–95)% |
| Air velocity | AZ9671 | Accuracy: ±2%, Range: (0.6–32) m/s |
| Physiological measurements | ||
| Skin temperature | DS1922L | Accuracy: ±0.5 °C, Range: (−40–85) °C |
| Pulse rate | CMS50D | Accuracy: ±2%, Range: (30–250) bpm |
| −4 | −3 | −2 | −1 | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|---|---|
| Very cold | Cold | Cool | Slightly cool | Neutral | Slightly warm | Warm | Hot | Very hot |
| Number | Protection State | Indoor Temperature Range |
|---|---|---|
| State 1 | without protection | 22/24/26/28/30/32/34/36 °C |
| State 2 | wearing masks | |
| State 3 | wearing face shield | |
| State 4 | wearing medical protective clothing |
| Protection State | Regression Coefficient | Sig. | Correlation Coefficient | Adjusted R2 | RMSE | ||
|---|---|---|---|---|---|---|---|
| a | b | c | |||||
| state 1 | −19.415 | 0.685 | 0.075 | 0.000 | 0.911 | 0.886 | 0.621 |
| state 2 | −20.256 | 0.787 | 0.065 | 0.000 | 0.895 | 0.872 | 0.654 |
| state 3 | −21.300 | 0.853 | 0.042 | 0.000 | 0.872 | 0.851 | 0.695 |
| state 4 | −23.745 | 0.962 | 0.032 | 0.000 | 0.841 | 0.825 | 0.769 |
| oversall | −22.540 | 0.884 | 0.038 | 0.000 | 0.858 | 0.843 | 0.723 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, T.; Shan, X.; Deng, Q.; Zhou, Z.; Yang, G.; Wang, J.; Ren, Z. Thermal Perception and Physiological Responses under Different Protection States in Indoor Crowded Spaces during the COVID-19 Pandemic in Summer. Sustainability 2022, 14, 5477. https://doi.org/10.3390/su14095477
Liu T, Shan X, Deng Q, Zhou Z, Yang G, Wang J, Ren Z. Thermal Perception and Physiological Responses under Different Protection States in Indoor Crowded Spaces during the COVID-19 Pandemic in Summer. Sustainability. 2022; 14(9):5477. https://doi.org/10.3390/su14095477
Chicago/Turabian StyleLiu, Tao, Xiaofang Shan, Qinli Deng, Zeng Zhou, Guang Yang, Jue Wang, and Zhigang Ren. 2022. "Thermal Perception and Physiological Responses under Different Protection States in Indoor Crowded Spaces during the COVID-19 Pandemic in Summer" Sustainability 14, no. 9: 5477. https://doi.org/10.3390/su14095477