
Impaired Endothelial Function in Convalescent Phase of COVID-19: A 3 Month Follow Up Observational Prospective Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Patients
- The “Home care” group, obtained by merging the following two original categories: (a) patients not admitted to hospital with resumption of normal activities, and (b) patients not admitted to hospital, but unable to resume normal activities;
- The “Hospital, no oxygen” group, including patients admitted to hospital but not requiring supplemental oxygen;
- The “Hospital, oxygen” group, including patients admitted to hospital, requiring supplemental oxygen, but not requiring high-flow nasal canula (HFNC), non-invasive ventilation (NIV), invasive mechanical ventilation (IMV), or extracorporeal membrane oxygenation (ECMO);
- The “Hospital, NIV or ICU” group, obtained by merging these two original categories: (a) patients admitted to hospital requiring HFNC or NIV, and (b) patients admitted to hospital requiring IMV, ECMO, or both.
2.3. Vascular Assessment
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Sample
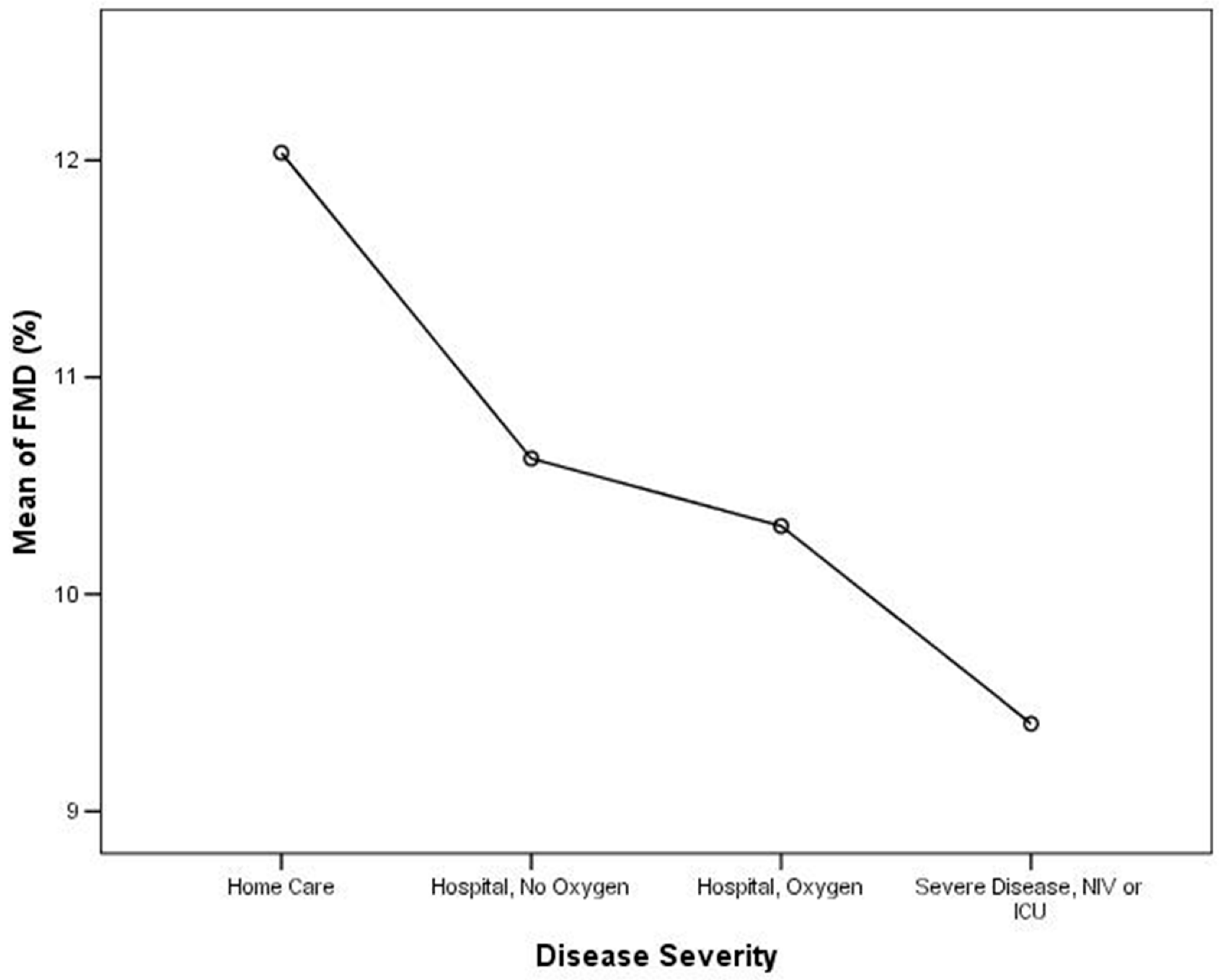
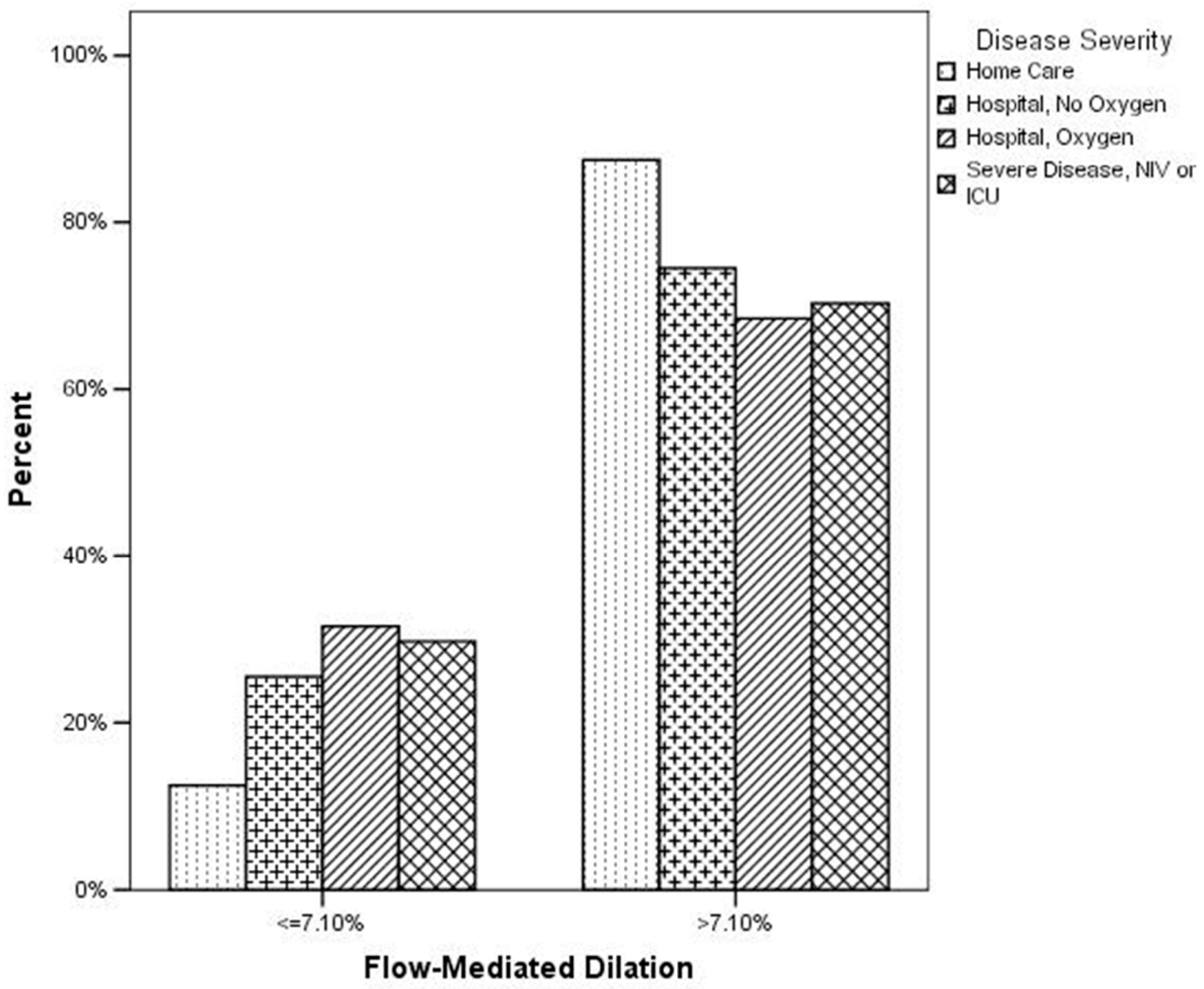
3.2. Relationship between FMD and COVID-19 Severity
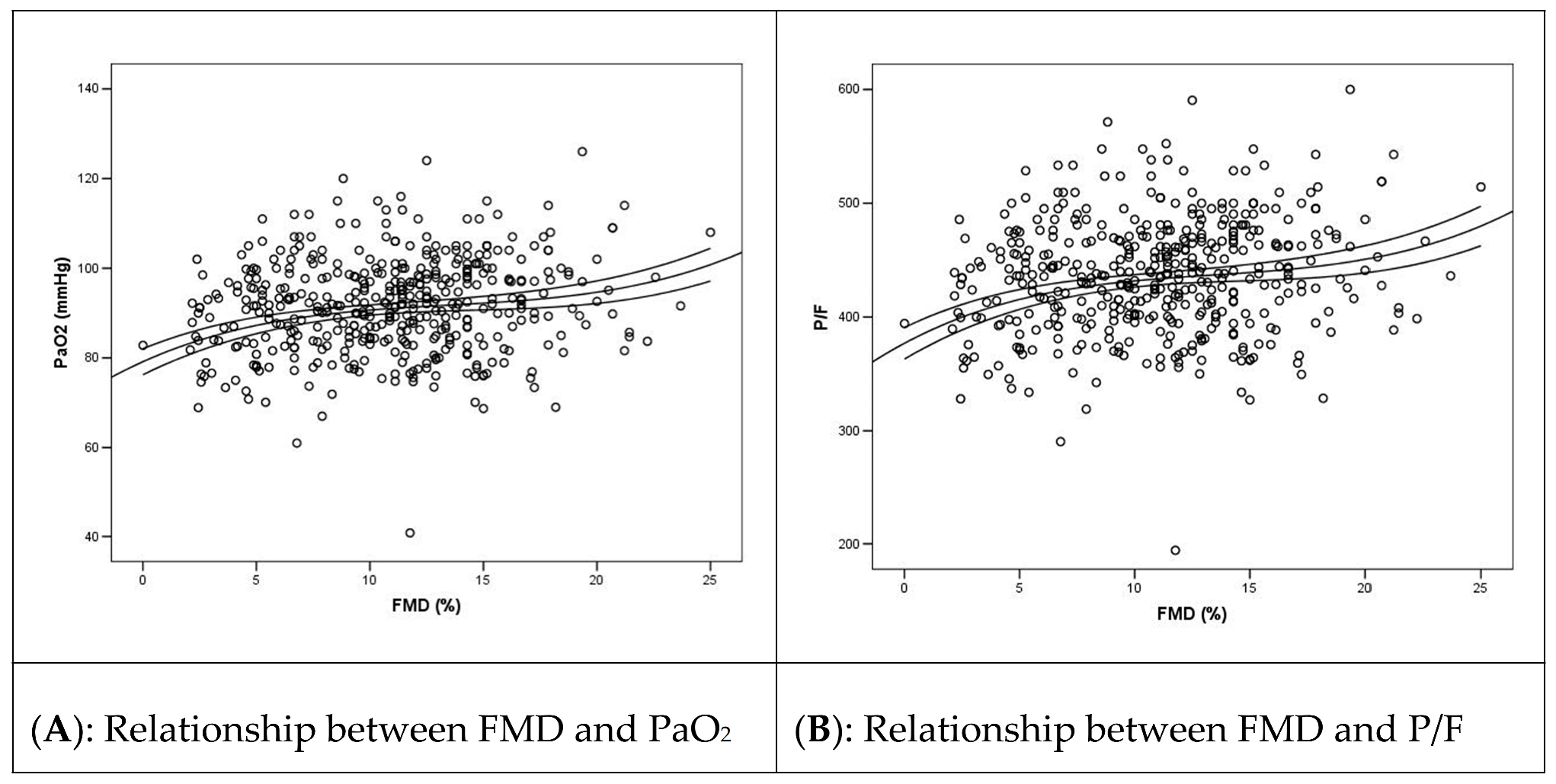
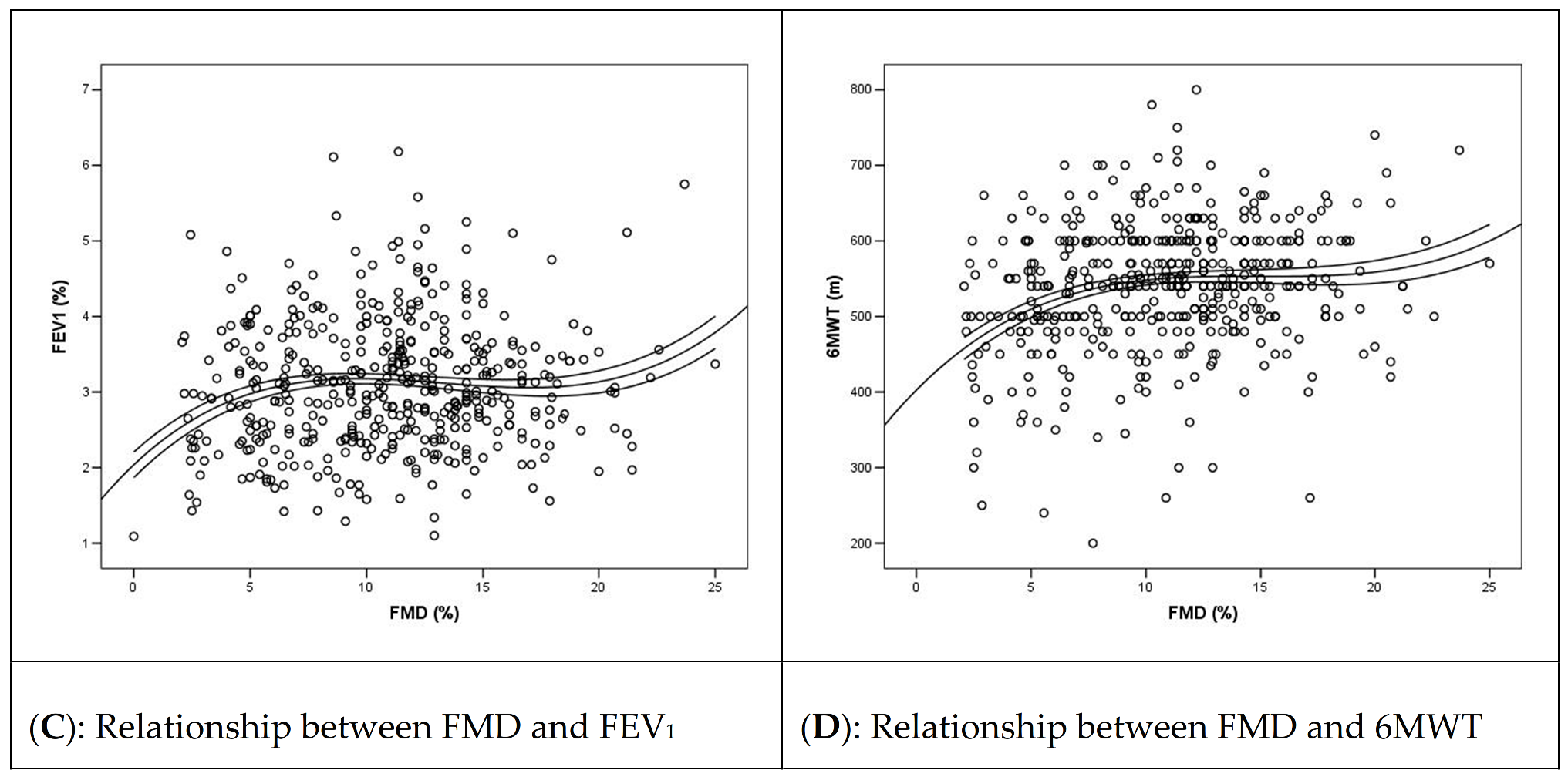
3.3. Relationship between FMD and Pulmonary Function Outcomes
4. Discussion
4.1. Study Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Nägele, M.P.; Haubner, B.; Tanner, F.C.; Ruschitzka, F.; Flammer, A.J. Endothelial dysfunction in COVID-19: Current findings and therapeutic implications. Atherosclerosis 2020, 314, 58–62. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Pons, S.; Fodil, S.; Azoulay, E.; Zafrani, L. The vascular endothelium: The cornerstone of organ dysfunction in severe SARS-CoV-2 infection. Crit. Care 2020, 24, 353. [Google Scholar] [CrossRef]
- Zimmer, S.; Steinmetz, M.; Asdonk, T.; Motz, I.; Coch, C.; Hartmann, E.; Barchet, W.; Wassmann, S.; Hartmann, G.; Nickenig, G. Activation of Endothelial Toll-Like Receptor 3 Impairs Endothelial Function. Circ. Res. 2011, 108, 1358–1366. [Google Scholar] [CrossRef] [Green Version]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.-H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; Van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0049384820301201 (accessed on 10 January 2022). [CrossRef] [PubMed]
- Llitjos, J.-F.; Leclerc, M.; Chochois, C.; Monsallier, J.-M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Santoliquido, A.; Porfidia, A.; Nesci, A.; De Matteis, G.; Marrone, G.; Porceddu, E.; Cammà, G.; Giarretta, I.; Fantoni, M.; Landi, F.; et al. Incidence of Deep Vein Thrombosis among non-ICU Patients Hospitalized for COVID-19 Despite Pharmacological Thromboprophylaxis. J. Thromb. Haemost. 2020, 18, 2358–2363. [Google Scholar] [CrossRef] [PubMed]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef]
- Mahmud, E.; Dauerman, H.L.; Welt, F.G.; Messenger, J.C.; Rao, S.V.; Grines, C.; Mattu, A.; Kirtane, A.J.; Jauhar, R.; Meraj, P.; et al. Management of acute myocardial infarction during the COVID-19 pandemic. Catheter. Cardiovasc. Interv. 2020, 96, 336–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colling, M.E.; Kanthi, Y. COVID-19-associated coagulopathy: An exploration of mechanisms. Vasc. Med. 2020, 25, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients after Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Evans, P.C.; Rainger, G.E.; Mason, J.C.; Guzik, T.J.; Osto, E.; Stamataki, Z.; Neil, D.; Hoefer, I.E.; Fragiadaki, M.; Waltenberger, J.; et al. Endothelial dysfunction in COVID-19: A position paper of the ESC Working Group for Atherosclerosis and Vascular Biology, and the ESC Council of Basic Cardiovascular Science. Cardiovasc. Res. 2020, 116, 2177–2184. [Google Scholar] [CrossRef]
- Ratchford, S.M.; Stickford, J.L.; Province, V.M.; Stute, N.; Augenreich, M.A.; Koontz, L.K.; Bobo, L.K.; Stickford, A.S. Vascular alterations among young adults with SARS-CoV-2. Am. J. Physiol. Circ. Physiol. 2021, 320, H404–H410. [Google Scholar] [CrossRef]
- Fogarty, H.; Townsend, L.; Morrin, H.; Ahmad, A.; Comerford, C.; Karampini, E.; Englert, H.; Byrne, M.; Bergin, C.; O’Sullivan, J.M.; et al. Persistent endotheliopathy in the pathogenesis of long COVID syndrome. J. Thromb. Haemost. 2021, 19, 2546–2553. [Google Scholar] [CrossRef]
- Mejia-Renteria, H.; Travieso, A.; Sagir, A.; Martínez-Gómez, E.; Carrascosa-Granada, A.; Toya, T.; Núñez-Gil, I.J.; Estrada, V.; Lerman, A.; Escaned, J. In-vivo evidence of systemic endothelial vascular dysfunction in COVID-19. Int. J. Cardiol. 2021, 345, 153–155. [Google Scholar] [CrossRef]
- Ambrosino, P.; Calcaterra, I.; Molino, A.; Moretta, P.; Lupoli, R.; Spedicato, G.; Papa, A.; Motta, A.; Maniscalco, M.; Di Minno, M. Persistent Endothelial Dysfunction in Post-Acute COVID-19 Syndrome: A Case-Control Study. Biomedicines 2021, 9, 957. [Google Scholar] [CrossRef]
- Seitz, A.; Ong, P. Endothelial dysfunction in COVID-19: A potential predictor of long-COVID? Int. J. Cardiol. 2022, 349, 155–156. [Google Scholar] [CrossRef]
- Landi, F.; Gremese, E.; Bernabei, R.; Fantoni, M.; Gasbarrini, A.; Settanni, C.R.; Benvenuto, F.; Bramato, G.; Carfì, A.; Ciciarello, F.; et al. Gemelli against COVID-19 Post-Acute Care Study Group. Post-COVID-19 global health strategies: The need for an interdisciplinary approach. Aging Clin. Exp. Res. 2020, 32, 1613–1620. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Deanfield, J.; Donald, A.; Ferri, C.; Giannattasio, C.; Halcox, J.; Halligan, S.; Lerman, A.; Mancia, G.; Oliver, J.J.; Pessina, A.C.; et al. Endothelial function and dysfunction. Part I. J. Hypertens. 2005, 23, 7–17. [Google Scholar] [CrossRef]
- Walters, J.F.; Hampton, S.M.; Deanfield, J.E.; Donald, A.E.; Skene, D.J.; Ferns, G.A. Circadian variation in endothelial function is attenuated in postmenopausal women. Maturitas 2006, 54, 294–303. [Google Scholar] [CrossRef]
- Ser, T.R. Physical Status: The Use and Interpretation of Anthropometry; Report of a WHO Expert Committee; World Health Organ Tech Rep Ser; WHO: Geneve, Switzerland, 1995; Volume 854, pp. 1–452. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8594834 (accessed on 10 January 2022).
- Maruhashi, T.; Kajikawa, M.; Kishimoto, S.; Hashimoto, H.; Takaeko, Y.; Yamaji, T.; Harada, T.; Han, Y.; Aibara, Y.; Yusoff, F.M.; et al. Diagnostic Criteria of Flow-Mediated Vasodilation for Normal Endothelial Function and Nitroglycerin-Induced Vasodilation for Normal Vascular Smooth Muscle Function of the Brachial Artery. J. Am. Heart Assoc. 2020, 9, e013915. [Google Scholar] [CrossRef]
- de Lucas-Ramos, P.; Izquierdo-Alonso, J.L.; Moro, J.M.R.G.; Frances, J.F.; Lozano, P.V.; Bellón-Cano, J.M.; CONSISTE Study Group. Chronic obstructive pulmonary disease as a cardiovascular risk factor. Results of a case—Control study (CONSISTE study). Int. J. COPD 2012, 7, 679–686. [Google Scholar]
- Magro, C.; Mulvey, J.J.; Berlin, D.; Nuovo, G.; Salvatore, S.; Harp, J.; Baxter-Stoltzfus, A.; Laurence, J. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl. Res. 2020, 220, 1–13. [Google Scholar] [CrossRef]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef]
- Bermejo-Martin, J.F.; Almansa, R.; Torres, A.; González-Rivera, M.; Kelvin, D.J. COVID-19 as a cardiovascular disease: The potential role of chronic endothelial dysfunction. Cardiovasc. Res. 2020, 116, e132–e133. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Anesi, G.L.; Jablonski, D.J.; Harhay, M.O.; Atkins, J.H.; Bajaj, J.; Baston, C.; Brennan, P.J.; Candeloro, C.L.; Catalano, L.M.; Cereda, M.F.; et al. Characteristics, Outcomes, and Trends of Patients with COVID-19–Related Critical Illness at a Learning Health System in the United States. Ann. Intern. Med. 2021, 174, 613–621. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Cohort | Home Care | Hospital, No Oxygen | Hospital, Oxygen | Hospital, NIV/ICU | p |
|---|---|---|---|---|---|---|
| Age (mean ± SD), years | 53.4 (14.9) | 46.6 (14.0) | 51.9 (15.0) | 59.8 (13.7) | 62.6 (11.4) | 0.0001 |
| Female sex (n, %) | 335 (48.9%) | 187 (27.5%) | 62 (9.1%) | 56 (8.2%) | 30 (4.4%) | 0.0001 |
| BMI (mean ± SD), kg/m2 | 25.8 (4.28) | 24.5 (4.29) | 26.0 (4.79) | 27.0 (4.17) | 26.8 (4.06) | 0.0001 |
| COVID-19 Severity: | ||||||
| Home care (n, %) | 285 (41.6%) | |||||
| Hospital, no oxygen (n, %) | 115 (16.8%) | |||||
| Hospital, oxygen (n, %) | 177 (25.8%) | |||||
| Hospital, NIV/ICU (n, %) | 108 (15.8%) | |||||
| FMD (mean ± SD), % | 10.8 (4.53) | 12.0 (4.34) | 10.6 (4.66) | 10.3 (4.55) | 9.40 (4.29) | 0.0001 |
| FMD ≤ 7.10 % (n, %) | 120 (22.7%) | 26 (12.5%) | 25 (25.5%) | 47 (31.5%) | 22 (29.7%) | 0.0001 |
| Smoking status | ||||||
| Never smoker (n, %) | 319 (46.6%) | 148 (25.8%) | 51 (8.9%) | 65 (11.3%) | 55 (9.6%) | |
| Active smoker (n, %) | 50 (8.7%) | 32 (5.6%) | 8 (1.4%) | 6 (1.0%) | 4 (0.7%) | |
| Previous smoker (n, %) | 204 (35.6%) | 56 (9.8%) | 34 (5.9%) | 83 (14.5%) | 31 (5.4%) | 0.0001 |
| Hypertension (n, %) | 203 (29.6%) | 49 (7.2%) | 28 (4.1%) | 75 (10.9%) | 51 (7.4%) | 0.0001 |
| Diabetes (n, %) | 51 (7.4%) | 10 (1.5%) | 4 (0.6%) | 24 (3.5%) | 13 (1.9%) | 0.0001 |
| FMD Mean | SD | 95% CI | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Home care | 12.03 | 4.33 | 11.44 | 12.63 |
| Hospital, No oxygen | 10.62 | 4.66 | 9.69 | 11.56 |
| Hospital, oxygen | 10.31 | 4.55 | 9.57 | 11.05 |
| Hospital, NIV, or ICU | 9.40 | 4.29 | 8.40 | 10.39 |
| Severity (I) | Severity (J) | (I − J) | p | 95% CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Home care | Hospital, no oxygen | 1.41 | 0.01 | 0.34 | 2.48 |
| Hospital, oxygen | 1.72 | 0.0003 | 0.78 | 2.66 | |
| Hospital, NIV or ICU | 2.63 | 0.0001 | 1.44 | 3.81 | |
| Hospital, no oxygen | Home care | −1.41 | 0.01 | −2.48 | −0.33 |
| Hospital, oxygen | 0.311 | 0.59 | −0.83 | 1.44 | |
| Hospital, NIV or ICU | 1.22 | 0.07 | −0.12 | 2.57 | |
| Hospital, oxygen | Home care | 1.72 | 0.0003 | −2.66 | −0.78 |
| Hospital, no oxygen | −0.31 | 0.59 | −1.44 | 0.82 | |
| Hospital, NIV or ICU | 0.91 | 0.15 | −0.33 | 2.15 | |
| Hospital, NIV, or ICU | Home care | −2.63 | 0.0001 | 3.81 | −1.44 |
| Hospital, no oxygen | −1.22 | 0.07 | −2.57 | 0.12 | |
| Hospital, oxygen | −0.91 | 0.15 | −2.15 | 0.33 | |
| FMD | Disease Severity | Total | ||||
|---|---|---|---|---|---|---|
| Home Care | Hospital Care | |||||
| No Oxygen | Oxygen | NIV or ICU | Total | |||
| >7.10% | 44.5% | 17.8% | 24.9% | 12.7% | 55.4% | 100% |
| ≤7.10% | 21.7% | 20.8% | 39.2% | 18.3% | 78.3% | 100% |
| Severity | p | OR | 95% CI | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Hospital, no oxygen | FMD ≤ 7.10% | 0.005 | 2.39 | 1.29 | 4.42 |
| Hospital, oxygen | FMD ≤ 7.10% | 0.0001 | 3.22 | 1.88 | 5.51 |
| Hospital, NIV, or ICU | FMD ≤ 7.10% | 0.0009 | 2.96 | 1.55 | 5.65 |
| OR | 95% CI | |||
|---|---|---|---|---|
| p | Lower | Upper | ||
| Disease severity | 0.011 | 1.354 | 1.06 | 1.71 |
| Age | 0.0001 | 1.933 | 1.370 | 2.726 |
| Sex | 0.71 | 1.09 | 0.67 | 1.78 |
| BMI | 0.70 | 0.94 | 0.68 | 1.29 |
| CRP | 0.62 | 0.98 | 0.93 | 1.04 |
| Arterial hypertension | 0.48 | 0.82 | 0.47 | 1.42 |
| T2DM | 0.11 | 1.89 | 0.85 | 4.22 |
| Smoking status | 0.51 | 1.08 | 0.85 | 1.39 |
| Constant | 0.0001 | 0.06 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santoro, L.; Falsetti, L.; Zaccone, V.; Nesci, A.; Tosato, M.; Giupponi, B.; Savastano, M.C.; Moroncini, G.; Gasbarrini, A.; Landi, F.; et al. Impaired Endothelial Function in Convalescent Phase of COVID-19: A 3 Month Follow Up Observational Prospective Study. J. Clin. Med. 2022, 11, 1774. https://doi.org/10.3390/jcm11071774
Santoro L, Falsetti L, Zaccone V, Nesci A, Tosato M, Giupponi B, Savastano MC, Moroncini G, Gasbarrini A, Landi F, et al. Impaired Endothelial Function in Convalescent Phase of COVID-19: A 3 Month Follow Up Observational Prospective Study. Journal of Clinical Medicine. 2022; 11(7):1774. https://doi.org/10.3390/jcm11071774
Chicago/Turabian StyleSantoro, Luca, Lorenzo Falsetti, Vincenzo Zaccone, Antonio Nesci, Matteo Tosato, Bianca Giupponi, Maria Cristina Savastano, Gianluca Moroncini, Antonio Gasbarrini, Francesco Landi, and et al. 2022. "Impaired Endothelial Function in Convalescent Phase of COVID-19: A 3 Month Follow Up Observational Prospective Study" Journal of Clinical Medicine 11, no. 7: 1774. https://doi.org/10.3390/jcm11071774