
Delirium in Critically Ill Patients with and without COVID-19—A Retrospective Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
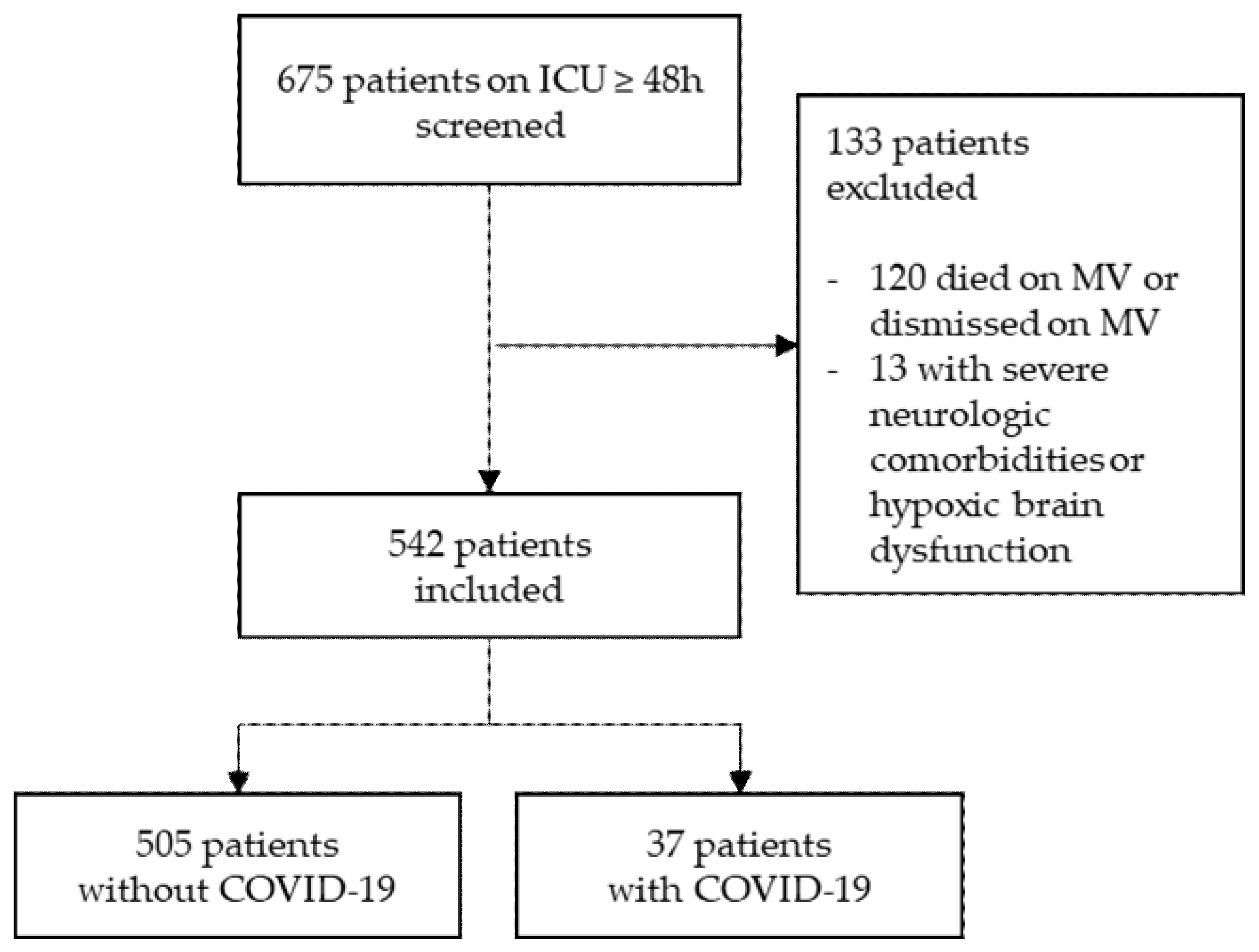
2.1. Patient Selection and Data Collection
2.2. Definition of Delirium
2.3. Bias
2.4. Statistical Methods
3. Results
3.1. Study Population
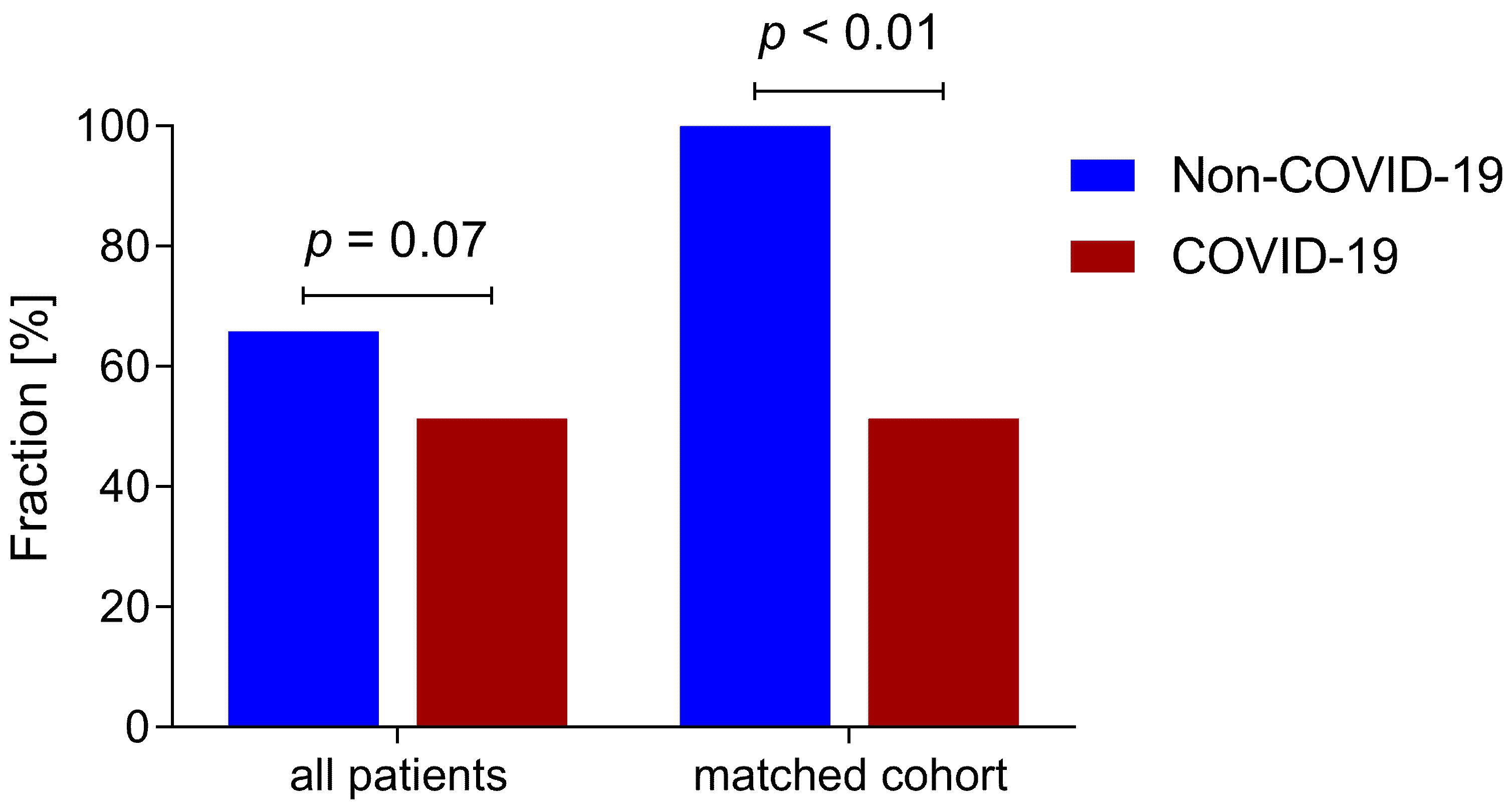
3.2. Delirium
3.3. Subgroup Analysis
3.4. Association of COVID-19 and Delirium
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, Y.-C.; Lu, M.-C.; Yang, S.-F.; Bien, M.-Y.; Chen, Y.-F.; Li, Y.-T. Respiratory care for the critical patients with 2019 novel coronavirus. Respir. Med. 2021, 186, 106516. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R.; Nahid, M.; Ringel, J.B.; et al. Clinical Characteristics of COVID-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Schenck, M.; Severac, F.; Clere-Jehl, R.; Studer, A.; Radosavljevic, M.; Kummerlen, C.; Monnier, A.; et al. Delirium and encephalopathy in severe COVID-19: A cohort analysis of ICU patients. Crit. Care 2020, 24, 491. [Google Scholar] [CrossRef]
- Song, E.; Zhang, C.; Israelow, B.; Lu-Culligan, A.; Prado, A.V.; Skriabine, S.; Lu, P.; Weizman, O.-E.; Liu, F.; Dai, Y.; et al. Neuroinvasion of SARS-CoV-2 in human and mouse brain. J. Exp. Med. 2021, 218, e20202135. [Google Scholar] [CrossRef]
- Verkhratsky, A.; Li, Q.; Melino, S.; Melino, G.; Shi, Y. Can COVID-19 pandemic boost the epidemic of neurodegenerative diseases? Biol. Direct 2020, 15, 28. [Google Scholar] [CrossRef]
- Maldonado, J.R. Delirium pathophysiology: An updated hypothesis of the etiology of acute brain failure. Int. J. Geriatr. Psychiatry 2018, 33, 1428–1457. [Google Scholar] [CrossRef] [PubMed]
- Cerejeira, J.; Nogueira, V.; Luís, P.; Vaz-Serra, A.; Mukaetova-Ladinska, E.B. The cholinergic system and inflammation: Common pathways in delirium pathophysiology. J. Am. Geriatr. Soc. 2012, 60, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Jäckel, M.; Bemtgen, X.; Wengenmayer, T.; Bode, C.; Biever, P.M.; Staudacher, D.L. Is delirium a specific complication of viral acute respiratory distress syndrome? Crit. Care 2020, 24, 401. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Hemkens, L.G.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. Das RECORD-Statement zum Berichten von Beobachtungsstudien, die routinemäßig gesammelte Gesundheitsdaten verwenden. Z. Evid. Fortbild. Qual. Gesundhwes. 2016, 115–116, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Gaudreau, J.-D.; Gagnon, P.; Harel, F.; Tremblay, A.; Roy, M.-A. Fast, systematic, and continuous delirium assessment in hospitalized patients: The nursing delirium screening scale. J. Pain Symptom Manag. 2005, 29, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Bergjan, M.; Zilezinski, M.; Schwalbach, T.; Franke, C.; Erdur, H.; Audebert, H.J.; Hauß, A. Validation of two nurse-based screening tools for delirium in elderly patients in general medical wards. BMC Nurs. 2020, 19, 72. [Google Scholar] [CrossRef] [PubMed]
- Luetz, A.; Heymann, A.; Radtke, F.M.; Chenitir, C.; Neuhaus, U.; Nachtigall, I.; von Dossow, V.; Marz, S.; Eggers, V.; Heinz, A.; et al. Different assessment tools for intensive care unit delirium: Which score to use? Crit. Care Med. 2010, 38, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond Agitation-Sedation Scale: Validity and reliability in adult intensive care unit patients. Am. J. Respir. Crit. Care Med. 2002, 166, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.F.; Pun, B.T.; Dittus, R.S.; Thomason, J.W.W.; Jackson, J.C.; Shintani, A.K.; Ely, E.W. Delirium and its motoric subtypes: A study of 614 critically ill patients. J. Am. Geriatr. Soc. 2006, 54, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Shintani, A.; Truman, B.; Speroff, T.; Gordon, S.M.; Harrell, F.E.; Inouye, S.K.; Bernard, G.R.; Dittus, R.S. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 2004, 291, 1753–1762. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.-M.; Liu, C.-Y.; Wang, C.-H.; Lin, H.-C.; Huang, C.-D.; Huang, P.-Y.; Fang, Y.-F.; Shieh, M.-H.; Kuo, H.-P. The impact of delirium on the survival of mechanically ventilated patients. Crit. Care Med. 2004, 32, 2254–2259. [Google Scholar] [CrossRef]
- Thomason, J.W.W.; Shintani, A.; Peterson, J.F.; Pun, B.T.; Jackson, J.C.; Ely, E.W. Intensive care unit delirium is an independent predictor of longer hospital stay: A prospective analysis of 261 non-ventilated patients. Crit. Care 2005, 9, R375–R381. [Google Scholar] [CrossRef] [Green Version]
- Balas, M.C.; Deutschman, C.S.; Sullivan-Marx, E.M.; Strumpf, N.E.; Alston, R.P.; Richmond, T.S. Delirium in older patients in surgical intensive care units. J. Nurs. Scholarsh. 2007, 39, 147–154. [Google Scholar] [CrossRef]
- Robinson, T.N.; Wu, D.S.; Pointer, L.F.; Dunn, C.L.; Moss, M. Preoperative cognitive dysfunction is related to adverse postoperative outcomes in the elderly. J. Am. Coll. Surg. 2012, 215, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Van den Boogaard, M.; Schoonhoven, L.; van der Hoeven, J.G.; van Achterberg, T.; Pickkers, P. Incidence and short-term consequences of delirium in critically ill patients: A prospective observational cohort study. Int. J. Nurs. Stud. 2012, 49, 775–783. [Google Scholar] [CrossRef] [Green Version]
- Veiga, D.; Luis, C.; Parente, D.; Fernandes, V.; Botelho, M.; Santos, P.; Abelha, F. Postoperative Delirium in Intensive Care Patients: Risk Factors and Outcome. Braz. J. Anesthesiol. 2012, 62, 469–483. [Google Scholar] [CrossRef] [Green Version]
- Pisani, M.A.; Murphy, T.E.; van Ness, P.H.; Araujo, K.L.B.; Inouye, S.K. Characteristics associated with delirium in older patients in a medical intensive care unit. Arch. Intern. Med. 2007, 167, 1629–1634. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, S.J.; Soto, G.J.; Hope, A.A.; Ponea, A.; Gong, M.N. The association between acute respiratory distress syndrome, delirium, and in-hospital mortality in intensive care unit patients. Am. J. Respir. Crit. Care Med. 2015, 191, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pun, B.T.; Badenes, R.; La Heras Calle, G.; Orun, O.M.; Chen, W.; Raman, R.; Simpson, B.-G.K.; Wilson-Linville, S.; Hinojal Olmedillo, B.; La Vallejo de Cueva, A.; et al. Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): A multicentre cohort study. Lancet Respir. Med. 2021, 9, 239–250. [Google Scholar] [CrossRef]
- Wilcox, M.E.; Shankar-Hari, M.; McAuley, D.F. Delirium in COVID-19: Can we make the unknowns knowns? Intensive Care Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jäckel, M.; Zotzmann, V.; Wengenmayer, T.; Duerschmied, D.; Biever, P.M.; Spieler, D.; von zur Mühlen, C.; Stachon, P.; Bode, C.; Staudacher, D.L. Incidence and predictors of delirium on the intensive care unit after acute myocardial infarction, insight from a retrospective registry. Catheter. Cardiovasc. Interv. 2020. [Google Scholar] [CrossRef]
- Siew, E.D.; Fissell, W.H.; Tripp, C.M.; Blume, J.D.; Wilson, M.D.; Clark, A.J.; Vincz, A.J.; Ely, E.W.; Pandharipande, P.P.; Girard, T.D. Acute Kidney Injury as a Risk Factor for Delirium and Coma during Critical Illness. Am. J. Respir. Crit. Care Med. 2017, 195, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Kotfis, K.; Roberson, S.W.; Wilson, J.E.; Dabrowski, W.; Pun, B.T.; Ely, E.W. COVID-19: ICU delirium management during SARS-CoV-2 pandemic. Crit. Care 2020, 24, 176. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | COVID-19 (n = 37) | Non-COVID-19 (n = 505) | p-Value |
|---|---|---|---|
| Age | 61.0 (47.5–72.0) | 69.5 (58.5–79.0) | 0.002 |
| Female | 11 (29.7%) | 186 (36.8%) | 0.386 |
| Comorbidities | |||
| Heart rhythm disturbances | 8 (21.6%) | 141 (27.9%) | 0.407 |
| Coronary heart disease | 9 (24.3%) | 130 (25.7%) | 0.849 |
| Obesity | 7 (18.9%) | 60 (11.9%) | 0.200 |
| Pulmonary disease | 6 (16.2%) | 101 (20.0%) | 0.577 |
| Liver disease | 1 (2.7%) | 46 (9.1%) | 0.237 |
| Chronic kidney disease | 7 (18.9%) | 104 (20.6%) | 0.807 |
| Peripheral/cerebral arterial occlusive disease | 2 (5.4%) | 59 (11.7%) | 0.415 |
| Neurologic disease | 4 (10.8%) | 122 (24.2%) | 0.064 |
| Malignancy | 5 (13.5%) | 83 (16.4%) | 0.642 |
| Psychiatric disease | 2 (5.4%) | 56 (11.1%) | 0.410 |
| Dementia | 0 (0.0%) | 28 (5.5%) | 0.246 |
| Alcohol abuse | 0 (0.0%) | 45 (8.9%) | 0.062 |
| Drug abuse | 0 (0.0%) | 18 (3.6%) | 0.626 |
| Clinical Characteristics | COVID-19 (n = 37) | Non-COVID-19 (n = 505) | p |
|---|---|---|---|
| Delirium (NuDESC ≥ 2) | 19 (51.4%) | 333 (65.9%) | 0.073 |
| Delirium positive days (%) | 4.4 (0–65.2) | 39.1 (0–83.9) | 0.068 |
| ICU stay (days) | 10.6 (4.9–18.7) | 4.7 (2.9–8.1) | <0.001 |
| Mortality | 7 (18.9%) | 70 (13.9%) | 0.395 |
| TISS 10 * | 10 (10–15) | 10 (5–15); n = 503 | 0.270 |
| SAPS2 * | 43 (30–47) | 43 (34–52); n = 503 | 0.214 |
| Non-invasive ventilation | 28 (75.7%) | 202 (40.0%) | <0.001 |
| Invasive ventilation | 18 (48.6%) | 187 (37.0%) | 0.159 |
| Non-invasive or invasive ventilation | 33 (89.2%) | 298 (59.0%) | <0.001 |
| Days on ventilation ** | 14.3 (6.0–17.6) | 5.6 (2.3–9.3) | 0.006 |
| V-V ECMO | 5 (13.5%) | 10 (2.0%) | 0.002 |
| Catecholamine therapy | 25 (67.6%) | 294 (58.2%) | 0.265 |
| Norepinephrine | 25 (67.6%) | 277 (54.9%) | 0.133 |
| Dobutamine | 3 (8.1%) | 38 (7.5%) | 0.753 |
| Vasopressin | 2 (5.4%) | 22 (4.4%) | 0.675 |
| Renal replacement therapy | 5 (13.5%) | 63 (12.5%) | 0.798 |
| Necessity of blood transfusions | 16 (43.2%) | 177 (35.0%) | 0.315 |
| Cause of illness | |||
| Respiratory | 29 (78.4%) | 122 (24.2%) | <0.001 |
| Cardiac | 7 (18.9%) | 254 (50.3%) | <0.001 |
| Septic | 1 (2.7%) | 96 (19.0%) | 0.012 |
| Other | 0 (0.0%) | 79 (15.6%) | 0.009 |
| COVID-19 (n = 19) | Non-COVID-19 (n = 333) | p | |
|---|---|---|---|
| Delirium onset (days) * | 1 (0–2) | 0 (0–1) | 0.260 |
| Highest NuDESC | 4 (3–5) | 4 (3–6) | 0.726 |
| Duration of delirium (days) | 3 (1–7) | 3 (1–5) | 0.643 |
| Hypoactive delirium | 6 (31.6% **) | 104 (31.2% **) | 0.975 |
| Mixed delirium | 8 (42.1% **) | 169 (50.8% **) | 0.464 |
| Hyperactive delirium | 5 (26.3% **) | 60(18.0% **) | 0.365 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jäckel, M.; Aicher, N.; Biever, P.M.; Heine, L.; Bemtgen, X.; Rilinger, J.; Zotzmann, V.; Supady, A.; Stachon, P.; Wengenmayer, T.; et al. Delirium in Critically Ill Patients with and without COVID-19—A Retrospective Analysis. J. Clin. Med. 2021, 10, 4412. https://doi.org/10.3390/jcm10194412
Jäckel M, Aicher N, Biever PM, Heine L, Bemtgen X, Rilinger J, Zotzmann V, Supady A, Stachon P, Wengenmayer T, et al. Delirium in Critically Ill Patients with and without COVID-19—A Retrospective Analysis. Journal of Clinical Medicine. 2021; 10(19):4412. https://doi.org/10.3390/jcm10194412
Chicago/Turabian StyleJäckel, Markus, Nico Aicher, Paul Marc Biever, Laura Heine, Xavier Bemtgen, Jonathan Rilinger, Viviane Zotzmann, Alexander Supady, Peter Stachon, Tobias Wengenmayer, and et al. 2021. "Delirium in Critically Ill Patients with and without COVID-19—A Retrospective Analysis" Journal of Clinical Medicine 10, no. 19: 4412. https://doi.org/10.3390/jcm10194412