
A Rapid Review on the Influence of COVID-19 Lockdown and Quarantine Measures on Modifiable Cardiovascular Risk Factors in the General Population


Abstract
:1. Introduction
2. Materials and Methods
- Population: general population (all age groups)
- Exposure: COVID-19 lockdown and quarantine measures
- Comparison: no quarantine and lockdown measures or different forms of quarantine and lockdown measures
- Study design: epidemiological observational studies (i.e., cohort studies, case-control studies, cross-sectional, studies) using representative sampling methods and secondary data studies
2.1. Inclusion and Exclusion Criteria
2.1.1. Population
2.1.2. Exposure
2.1.3. Comparison
2.1.4. Outcome
2.1.5. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Critical Appraisal
2.6. Data Synthesis
3. Results
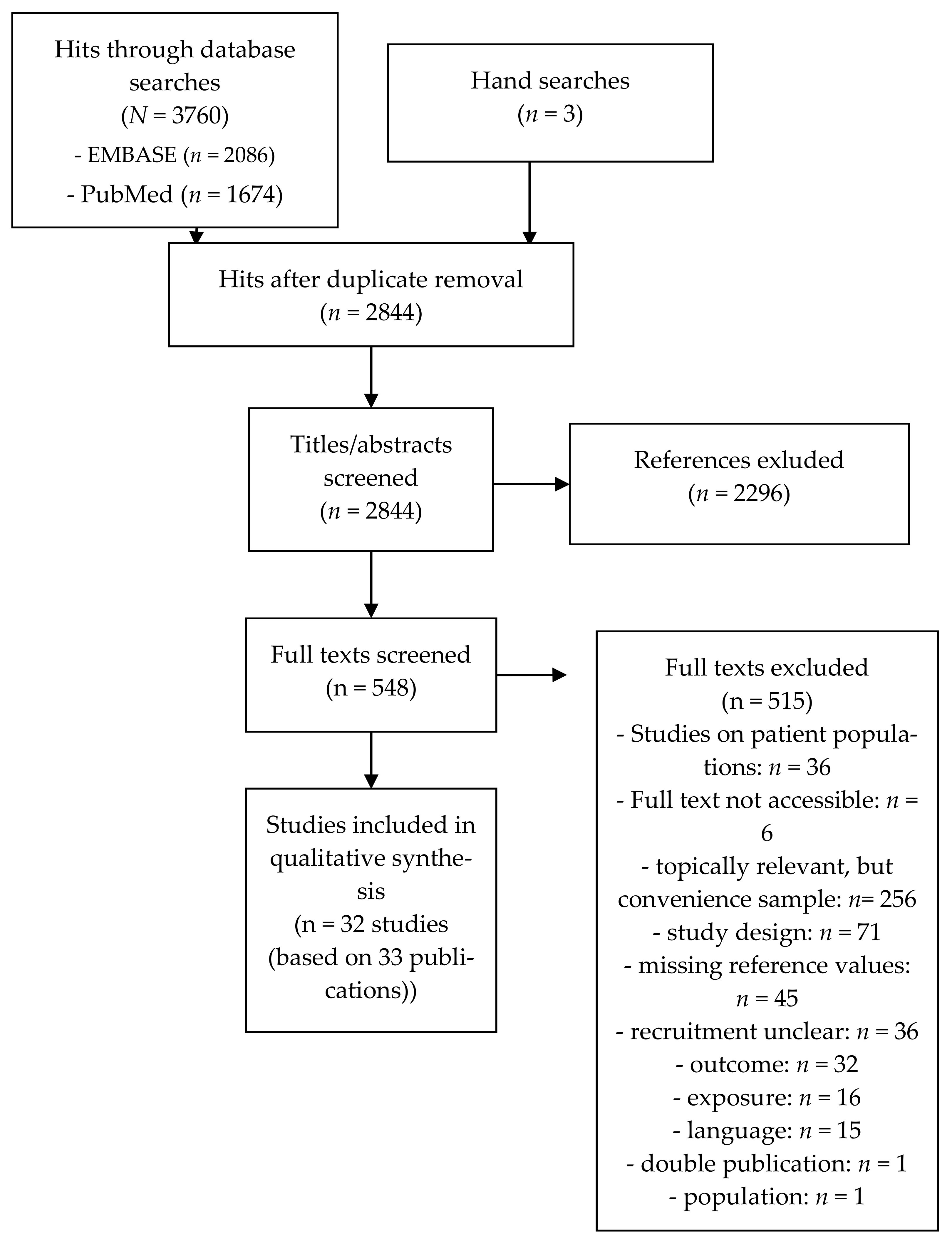
3.1. Results of the Literature Search
3.2. Study Characteristics
3.3. Results of the Risk of Bias-Assessment
3.4. Results from the Included Studies
3.4.1. Physical Activity

{kind=link}
| Reference (Study Design) | Country | Population (Sample Size) | Results | |||
|---|---|---|---|---|---|---|
| Children and Adolescents | ||||||
| Medrano et al., 2020 [87] (Cohort study) | Spain | School children aged 8–16 years (baseline: n = 281, follow-up: n = 113) | Change since lockdown | |||
| T1 (before lockdown) | T2 (during lockdown) | p | ||||
| (M SD)) | (M SD)) | |||||
| Physical activity (minutes/day) | 154 (40) | 63 (39) | <0.001 | |||
| Change since lockdown | ||||||
| Prevalence (%) | ||||||
| Worsening of physical activity | 95.2 | |||||
| Schmidt et al., 2020 [93] (Cohort study) | Germany | Children and adolescents (baseline: n = 2722, follow-up: n = 1711) | Change since lockdown | |||
| Baseline (%) | Follow-up (%) | p | ||||
| Days active (days/week) for more than 60 min with moderate to vigorous intensity | 4.3 (1.8) | 4.7 (2.0) | <0.01 | |||
| Physical activity guideline adherence | 19.1 | 30.1 | <0.01 | |||
| Total amount of (organized and non-organized) sports (minutes per day) | 34.9 (26.0) | 24.3 (36.2) | < 0.01 | |||
| Total amount of (organized and non-organized) sports (minutes per day) | 34.9 (26.0) | 24.3 (36.2) | < 0.01 | |||
| Tornaghi et al., 2020 [95] (Cohort study) | Italy | Adolescents (15–18 years) (baseline: n = 1568, follow-up: n = 1568) | Change since lockdown | |||
| Pre-lockdown | During lockdown | Post-lockdown | ||||
| (n (%)) | (n (%)) | (n (%)) | ||||
| Physically inactive | 154 (17.8) | 102 (25.8) | 53 (18.5) | |||
| Moderate activity | 573 (66.3) | 214 (53.6) | 177 (61.7) | |||
| Intense activity | 137 (15.8) | 79 (19.8) | 57 (19.9) | |||
| Change since lockdown | ||||||
| Pre-lockdown | During lockdown | Post-lockdown | ||||
| (M (SD)) | (M (SD)) | (M (SD)) | ||||
| Physical activity (minutes/week) | 1676 (21) | n.r. | 1775 (34) | |||
| - statistically significant difference in physical activity measured as MET-min/week, absolute, or categorical physical activity levels (3 × 3 ANOVA): higher physical activity during and after lockdown than before | ||||||
| McCormack et al., 2020 [86] (Cross-sectional study) | Canada | Children aged 5–17 years (n = 328) | Change since lockdown | |||
| Prevalence (n%) | ||||||
| Physical activity at home | ||||||
| Increased | 48.8 | |||||
| No change | 32.9 | |||||
| Decreased | 18.3 | |||||
| Physical activity outdoors | ||||||
| Increased | 38.7 | |||||
| No change | 22.3 | |||||
| Decreased | 39 | |||||
| Playing at a park | ||||||
| Increased | 15.5 | |||||
| No change | 31.7 | |||||
| Decreased | 52.7 | |||||
| Playing at other public places | ||||||
| Increased | 9.5 | |||||
| No change | 36.9 | |||||
| Decreased | 53.7 | |||||
| ADULTS | ||||||
| Savage et al., 2020 [92] (Cohort study) | United Kingdom | Students (baseline: n = 1477, follow-up: n = 214) | Change since lockdown | |||
| p | Cohens’ d | |||||
| Moderate to vigorous physical activity levels | <0.01 ** | 0.12 | ||||
| Wickersham et al., 2021 [98] (Prospective secondary data analysis) | United Kingdom | Students who had enrolled in the remote measurement techno-locy (RMT) King’s Move Physical Activity (PA) tracker app (n = 736) | Change since lockdown | |||
| Steps/week | IRR (95% CI) | p | ||||
| Linear effect | 1.00 (0.97–1.03) | 0.984 | ||||
| Quadratic effect | 1.00 (1.00–1.01) | 0.047 | ||||
| Barkley et al., 2020 [74] (Cross-sectional study) | United States | Students (baseline: n = 184) | Change since campus closure | |||
| Pre-campus closure (M (SD)) | Post-campus closure (M (SD)) | |||||
| Mild physical activity | ||||||
| Undergraduate students | 16.3 (22.6) | 10.8 (12.9) | ||||
| Graduate students | 12.0 (22.4) | 11.2 (11.7) | ||||
| Moderate physical activity | ||||||
| Undergraduate students | 15.0 (15.7) | 12.9 (12.4) | ||||
| Graduate students | 17.1 (36.9) | 16.6 (19.7) | ||||
| Strenuous physical activity | ||||||
| Undergraduate students | 16.0 (22.1) | 14.0 (17.9) | ||||
| Graduate students | 19.1 (32.9) | 21.0 (33.7) | ||||
| Total physical activity | ||||||
| Undergraduate students | 47.2 (40.2) | 37.7 (30.7) | ||||
| Graduate students | 48.2 (75.2) | 48.7 (58.8) | ||||
| Özden and Kilic, 2021 [88] (Cross-sectional study) | Turkey | Nursing students (n = 1011) | Change since lockdown | |||
| Before COVID-19 outbreak (%) | During lockdown (%) | |||||
| Regular exercise every day | 32.6 | 43.3 | ||||
| Karuc et al., 2020 [83] (Cross-sectional study) | Kroatia | Young adults (n = 91) | Change since lockdown | |||
| Physical activity | Prevalence (%) | |||||
| Women | ||||||
| No change | 25 | |||||
| Increase | 19 | |||||
| Decrease | 56 | |||||
| Men | ||||||
| No change | 31 | |||||
| Increase | 19 | |||||
| Decrease | 50 | |||||
| Change since lockdown | ||||||
| Moderate-to-vigorous physical activity (minutes/day) | Pre-restrictions | Post-restrictions | p | |||
| (Median (IQR)) | (Median (IQR)) | |||||
| Women | 120.0 (227.1) | 64.3 (75.0) | >0.0001 | |||
| Men | 135.0 (127.5) | 85.7 (56.8) | 0.006 | |||
| Di Sebastiano et al., 2020 [81] (Prospective secondary data analysis) | Canada | Adults (≥18 years) using a physical activity tracking app (baseline: n = 2338, follow-up: 2388 (only complete data sets were used)) | Change since lockdown | |||
| 4 weeks prior physical distancing (M (SE)) | 1 weeks after beginning of physical distancing (M (SE)) | p | ||||
| Moderate-to-vigorous physical activity (minutes) | 194.2 (5.2) | 176.7 (5.0) | <0.001 | |||
| Light physical activity (minutes) | 1000.5 (17.0) | 874.1 (15.6) | <0.001 | |||
| Steps | 48,625 (745) | 43,395 (705) | <0.001 | |||
| Change since lockdown | ||||||
| 4 weeks prior physical distancing (M (SE)) | 6 weeks after beginning of physical distancing (M (SE)) | p | ||||
| Moderate-to-vigorous physical activity (minutes) | 194.2 (5.2) | 204.4 (5.4) | 0.498 | |||
| Light physical activity (minutes) | 1000.5 (17.0) | 732.0 (14.3) | <0.001 | |||
| Steps | 48,625 (745) | 41,946 (763) | <0.001 | |||
| To et al., 2021 [94] (Prospective secondary data analysis) | Australia | Adults using a physical activity tracking app (baseline: n = 60,560, follow-up: 2388 (only complete data sets were used)) | Change since lockdown | |||
| Before lockdown | After lockdown | p | ||||
| 7-day average of steps per day | 9500 | 9175 | <0.001 | |||
| 30-day average of steps per day | 9684 | 9199 | <0.001 | |||
| Wang et al., 2020 [96] (Cohort study) | China | Middle-aged and older adults (≥40 years) using a physical activity tracking app (baseline: n = 4145, follow-up: 3544) | Change since lockdown | |||
| Comparison 2019 with lockdown (mean difference (95% CI)) | Comparison early 2020 with lockdown (mean difference (95% CI)) | |||||
| Number of daily steps | −413 (−501–(−325)) | −2672 (−2763–(−2582)) | ||||
| Crochemore-Silva et al., 2020 [79] (Cross-sectional study) | Brazil | Adults (n = 377) | Change in leisure time physical activity according to level of social distancing | |||
| Level of social distancing | Engaging in physical activity (%) | p | ||||
| Very little | ~20 | 0.023 | ||||
| Little | Not reported (~21 *) | |||||
| Average | 37.7 | |||||
| A lot | Not reported (~25 *) | |||||
| Virtually isolated | ~20 | |||||
| Duncan et al., 2020 [73] (Cross-sectional study) | United States | Adult twins (n = 3971) | Change since lockdown | |||
| Physical activity | Prevalence (%) | |||||
| Decreased a lot | 15.1 | |||||
| Decreased somewhat | 28.7 | |||||
| No change | 26.4 | |||||
| Increased a lot | 5.2 | |||||
| Increased somewhat | 21.2 | |||||
| Okely et al., 2020 [33] (Cohort study) | Scotland | Older adults (born in 1936) (baseline: n not reported, follow-up: n = 137) | Change since lockdown | |||
| Baseline (2017–2019) (n (%)) | Follow-up (2020) (n (%)) | p | ||||
| Only household chores | 14 (10.2) | 26 (19.0) | 0.012 | |||
| Outdoor activities 1–2×/week | 28 (20.4) | 23 (16.8) | ||||
| Outdoor activities >2×/week | 67 (48.9) | 74 (54.0) | ||||
| Moderate exercise 1–2×/week | 19 (13.9) | 4 (2.9 | ||||
| Moderate exercise >2×/week | 6 (4.4) | 10 (7.3) | ||||
| Keep-fit/heavy exercise several times/week | 3 (2.2) | 0 (0.0) | ||||
| Yamada et al., 2020 [99] (Cohort study) | Japan | Physically independent residents, living in a continuing care retirement community (baseline: n = 114, follow-up: n = 114) |
| |||
| Berard et al., 2021 [75] (Cross-sectional study) | France | Older adults (aged ≥50 years) (n = 536) | Change since lockdown | |||
| Prevalence (n (%)) | ||||||
| Decreased physical activity | 194 (36.2) | |||||
| Sasaki et al., 2021 [91] (Cross-sectional study) | Japan | Older adults (60–95 years) (baseline: n = 2008) | Change since lockdown | |||
| Before restrictions | After restrictions | p | ||||
| (M (SD)) | (M (SD)) | |||||
| Vigorous physical activity (MET) | ||||||
| Men | 1690.6 (2668.8) | 1604.8 (2598.2) | 0.035 | |||
| Women | 742.5 (1701.3) | 717.5 (1738.0) | 0.4 | |||
| Moderate physical activity (MET) | ||||||
| Men | 1064.7 (1332.8) | 1002.6 (1306.4) | 0.0024 | |||
| Women | 712.5 (1062.7) | 644.4 (1005.1) | 0.0022 | |||
| Walking (MET) | ||||||
| Men | 922.9 (1035.5) | 877.4 (1028.9) | 0.0054 | |||
| Women | 717.2 (899.6) | 647.2 (870.5) | <0.001 | |||
| Total physical activity (MET) | ||||||
| Men | 3678.2 (4163.1) | 3484.8 (4112.3) | 0.0024 | |||
| Women | 2172.1 (2873.2) | 2009.2 (2876.6) | <0.001 | |||
3.4.2. Sedentary Behaviour
| Reference (Study Design) | Country | Population (Sample Size) | Results | |||
|---|---|---|---|---|---|---|
| Children and Adolescents | ||||||
| Medrano et al., 2020 [87] (Cohort study) | Spain | School children aged 8–16 years (baseline: n = 281, follow-up: n = 113) | Change since lockdown | |||
| T1 (before lockdown) | T2 (during lockdown) | p | ||||
| (M SD)) | (M SD)) | |||||
| Screen time (hours/day) | 4.3 (2.4) | 6.1 (2.4) | <0.001 | |||
| TV time ≥2 h/day (N, %) | 3 (2.8) | 14 (13.2) | 0.005 | |||
| Videogame time ≥2 h/day (N, %) | 6 (5.7) | 7 (6.6) | 0.775 | |||
| Computer (no homework) ≥2 h/day (N, %) | 1 (0.9) | 0 (0.0) | 0.316 | |||
| Total mobile-phone ≥2 h/day (N, %) | 4 (3.8) | 20 (18.9) | 0.001 | |||
| Total screen time ≥2 ≥2 h/day (N, %) | 70 (66.0) | 93 (87.7) | <0.001 | |||
| Change since lockdown | ||||||
| Prevalence (%) | ||||||
| Worsening of screen time | 68.9 | |||||
| Schmidt et al., 2020 [93] (Cohort study) | Germany | Children and adolescents (baseline: n = 2722, follow-up: n = 1711) | Change since lockdown | |||
| Baseline (%) | Follow-up (%) | p | ||||
| Screen time guideline adherence | 60.9 | 37.6 | <0.01 | |||
| Recreational screen time (TV, gaming, recreational internet) (minutes per day | 133.3 (123.1) | 194.5 (141.3) | <0.01 | |||
| McCormack et al., 2020 [86] (Cross-sectional study) | Canada | Children aged 5–17 years (n = 328) | Change since lockdown | |||
| Prevalence (n%) | ||||||
| Watching TV | ||||||
| Increased | 58.8 | |||||
| No change | 38.4 | |||||
| Decreased | 2.7 | |||||
| Playing video games | ||||||
| Increased | 56.4 | |||||
| No change | 40.9 | |||||
| Decreased | 2.7 | |||||
| Using screen-based devices | ||||||
| Increased | 75.9 | |||||
| No change | 22 | |||||
| Decreased | 2.1 | |||||
| Ozturk Eyimaya and Yalçin Irmak, 2020 [89] (Cross-sectional study) | Turkey | Children aged 6–13 years (n = 1155) | Change since lockdown | |||
| Screen time | Prevalence (n%) | |||||
| Increase | 71.7 | |||||
| Decrease | 6.1 | |||||
| No change | 23.2 | |||||
| ADULTS | ||||||
| Savage et al., 2020 [92] (Cohort study) | United Kingdom | Students (baseline: n = 1477, follow-up: n = 214) | Change since lockdown | |||
| p | Cohens’ d | |||||
| Time spent in sedentary behaviour on a typical day in the last month | <0.0001 * | 0.78 | ||||
| Barkley et al., 2020 [74] (Cross-sectional study) | United States | Students (baseline: n = 184) | Change since campus closure | |||
| Sedentary behaviour (minutes/week) | Pre-campus closure (M (SD)) | Post-campus closure (M (SD)) | ||||
| Undergraduate students | 3089.2 (1455.4) | 3681.0 (1600.3) | ||||
| Graduate students | 3129.1 (1329.7) | 3696.4 (1566.5) | ||||
| - statistically significant (p = 0.003) main effect of time for sedentary behaviour | ||||||
| Colley et al., 2020 [78] (Cross-sectional study) | Canada | Adults (baseline: n = 4524) | Increase since lockdown | |||
| Watching TV | Prevalence (% (95% CI)) | |||||
| Men | 59.8 (56.3–63.2) | |||||
| Women | 66.0 (63.2–68.6) | |||||
| Sasaki et al., 2021 [91] (Cross-sectional study) | Japan | Older adults (60–95 years) (baseline: n = 2008) | Change since lockdown | |||
| Sitting time (minutes/day) | Before restrictions | After restrictions | p | |||
| (M (SD)) | (M (SD)) | |||||
| Men | 273.4 (203.4) | 287.7 (204.1) | <0.001 | |||
| Women | 243.7 (181.5) | 267.8 (191.6) | <0.001 | |||
3.4.3. Alcohol Consumption
| Reference (Study Design) | Country | Population (Sample Size) | Results | ||||
|---|---|---|---|---|---|---|---|
| Adults | |||||||
| Niedzwiedz et al., 2020 [32] (Cohort study) | United Kingdom | Adults (baseline: n = 27,141, analysed at follow-up: n = 9748) | Association between lockdown and … | ||||
| Model 1 * | Model 2 ** | ||||||
| RR (95% CI) | RR (95% CI) | ||||||
| Binge drinking | |||||||
| During COVID-19 | 1.18 (0.97–1.45) | 1.27 (1.08–1.48) | |||||
| Alcohol frequency (drinking 4+ days per week) | |||||||
| During COVID-19 | 1.06 (0.96–1.17) | 1.23 (1.11–1.35) | |||||
| Heavy drinking (5+ drinks on a typical day when drinking) | |||||||
| During COVID-19 | 0.60 (0.42–0.86) | 0.46 (0.38–0.55) | |||||
| * adjusted for year, age group, gender, ethnicity, period and period × age group interaction | |||||||
| ** adjusted for year, age group, gender, ethnicity, period and period × gender interaction | |||||||
| Daly and Robinson, 2021 [80] (Cohort study) | United Kingdom | Adults (follow-up: n = 3358) | Change since lockdown | ||||
| 2016–2018 (M (SD)) | May 2020 (M (SD)) | p | |||||
| Overall AUDITPC score | 3.17 (2.46) | 3.34 (2.77) | 0.003 | ||||
| Change since lockdown | |||||||
| 2016–2018 (%) | May 2020 (%) | p | |||||
| High-risk drinking | 19.3 | 24.6 | 0.001 | ||||
| Alpers et al., 2021 [69] (Cross-sectional study) | Norway | Adults (n = 25,708) | Change since lockdown | ||||
| Alcohol consumption | Prevalence (n%) | ||||||
| Increase | 13 | ||||||
| Decrease | 23 | ||||||
| Association between several risk factors and an increase in alcohol consumption | |||||||
| OR (95% CI) * | |||||||
| Temporarily lay-off | 1.3 (1.1–1.4) | ||||||
| Quarantine | 1.2 (1.1–1.4) | ||||||
| Home office/study | 1.4 (1.3–1.5) | ||||||
| * adjusted for age, gender, economic worries, health worries, temporarily lay-off and/or quarantine and/or home office/study | |||||||
| Avery et al., 2020 [72] (Cross-sectional study) | United States | Adult twins (n = 3971) | Change since lockdown | ||||
| Alcohol consumption | Prevalence (%) | ||||||
| Do not use | 35.5 | ||||||
| Use more | 14.3 | ||||||
| Use the same | 39.4 | ||||||
| Use less | 10.9 | ||||||
| Cicero et al., 2021 [77] (Cross-sectional study) | Italy | Adults (n = 359) | Change since lockdown | ||||
| Pre-quarantine (% (SD)) | During quarantine (% (SD)) | p | |||||
| Total energy derived from the alcohol | 2.9 (0.6) | 4.9 (1.0) | 0.002 | ||||
| Bourion-Bedes et al., 2021 [76] (Cross-sectional study) | France | Students (n = 3936) | Change since lockdown | ||||
| Alcohol consumption | Prevalence (%) | ||||||
| None | 34.2 | ||||||
| No change | 17.1 | ||||||
| Increased | 13.7 | ||||||
| Reduced | 35 | ||||||
| Lechner et al., 2020 [84] (Cross-sectional study) | United States | Students (n = 1958) | Change since lockdown | ||||
| Week prior to university closing (M (SD)) | Week succeeding university closing (M (SD)) | ||||||
| Number of weekly standard drinks | 3.48 (5.45) | 5.01 (6.86) | |||||
| Number of drinking days | 1.36 (1.55) | 1.94 (1.84) | |||||
| White et al., 2021 [97] (Cross-sectional study) | United States | Students (n = 297) | Change since lockdown | ||||
| Pre-closure (M) | Post-closure (M) | p | d | ||||
| Drinking frequency (in days) | 3 | 3.2 | <0.05 | 0.12 | |||
| Weekly quantity (drinks/week) | 11.5 | 9.9 | <0.01 | 0.15 | |||
| Maximum number of drinks in one day | 4.9 | 3.3 | <0.001 | 0.47 | |||
3.4.4. Weight and Body-Mass-Index
| Reference (Study Design) | Country | Population (Sample Size) | Results | |||
|---|---|---|---|---|---|---|
| Adults | ||||||
| Mason et al., 2020 [85] (Cohort study) | United States | Young adults (baseline: 2013: n = 4100, 2020: n = 2548, follow-up: 1820) | Change since lockdown | |||
| M (SD) | M% (SD) | |||||
| Weight change (pounds) | 3.47 (14.57) | 2.5 % (8.6 %) | ||||
| Cicero et al., 2021 [77] (Cross-sectional study) | Italy | Adults (n = 359) | Change since lockdown | |||
| Pre-quarantine (M (SD)) | During quarantine (M (SD)) | p | ||||
| Body mass index | 26.6 (4.7) | 26.9 (4.5) | 0.361 | |||
| Radwan et al., 2021 [90] (Cross-sectional study) | United Arab Emirates | Adults (n = 2060) | Change since lockdown | |||
| Weight | Prevalence (n (%)) | |||||
| Increase | 606 (29.4) | |||||
| Decrease | 476 (23.1) | |||||
| Same | 978 (47.5) | |||||
| Barkley et al., 2020 [74] (Cross-sectional study) | United States | Students (n = 184) | Change since campus closure | |||
| Bodyweight (pounds) | Pre-campus closure (M (SD)) | Post-campus closure (M (SD)) | ||||
| Undergraduate students | 175.4 (48.4) | 176.8 (48.4) | ||||
| Graduate students | 163.7 (45.6) | 164.5 (45.6) | ||||
| - no statistically significant (p ≥ 0.16) main or interaction effects of time for bodyweight | ||||||
| Özden and Kilic, 2021 [88] (Cross-sectional study) | Turkey | Nursing students (n = 1011) | Change since lockdown | |||
| Weight | Prevalence (%) | |||||
| Increase | 46.9 | |||||
| Decrease | 33.4 | |||||
| Same | 19.7 | |||||
| Berard et al., 2021 [75] (Cross-sectional study) | France | Older adults (aged ≥ 50 years) (n = 536) | Change since lockdown | |||
| Prevalence (n (%)) | ||||||
| Weight gain | 137 (25.6) | |||||
3.4.5. Eating Behaviour
| Reference (Study Design) | Country | Population (Sample Size) | Results | |||
|---|---|---|---|---|---|---|
| Children and Adolescents | ||||||
| Medrano et al., 2020 [87] (Cohort study) | Spain | School children aged 8–16 years (baseline: n = 281, follow-up: n = 113) | Change since lockdown | |||
| T1 (before lockdown) | T2 (during lockdown) | p | ||||
| (M SD)) | (M SD)) | |||||
| Adherence to the Mediterranean diet | 5.9 (1.8) | 6.4 (1.5) | 0.018 | |||
| Low adherence to the Mediterranean diet | 86 (81.1) | 81 (76.4) | 0.476 | |||
| Change since lockdown | ||||||
| Prevalence (%) | ||||||
| Worsening of the adherence to the Mediterranean diet | 31.4 | |||||
| Adults | ||||||
| Cicero et al., 2021 [77] (Cross-sectional study) | Italy | Adults (n = 359) | Change since lockdown | |||
| Pre-quarantine (M (SD)) | During quarantine (M (SD)) | p | ||||
| Energy intake | 2568 (322) | 2739 (442) | <0.001 | |||
| Dietary quality index | 42.4 (4.1) | 37.8 (4.7) | 0.011 | |||
| Change since lockdown for total energy derived from the main diet components | ||||||
| Pre-quarantine (% (SD)) | During quarantine (% (SD)) | p | ||||
| Total carbohydrates | 49.3 (4.6) | 52.6 (6.5) | 0.048 | |||
| Simple sugars | 3.1 (0.9) | 4.6 (1.1) | 0.002 | |||
| Total fats | 28.1 (3.2) | 31.4 (2.9) | 0.047 | |||
| Added fats | 3.9 (1.1) | 4.3 (1.2) | 0.021 | |||
| Garre-Olmo et al., 2020 [82] (Cross-sectional study) | Spain | Adults (n = 692) | Change since lockdown | |||
| Prevalence (n (%)) | ||||||
| Worsening dietary pattern | 134 (19.4) | |||||
| Radwan et al., 2021 [90] (Cross-sectional study) | United Arab Emirates | Adults (n = 2060) | Change since lockdown | |||
| Food intake | Prevalence (n (%)) | |||||
| Increase | 655 (31.8) | |||||
| Decrease | 344 (16.7) | |||||
| Same | 1061 (51.5) | |||||
| Berard et al., 2021 [75] (Cross-sectional study) | France | Older adults (aged ≥ 50 years) (n = 536) | Change since lockdown | |||
| Prevalence (n (%)) | ||||||
| Decreased diet quality | 142 (26.5) | |||||
3.4.6. Smoking
| Reference (Study Design) | Country | Population (Sample Size) | Results | ||
|---|---|---|---|---|---|
| Adults | |||||
| Niedzwiedz et al., 2020 [32] (Cohort study) | United Kingdom | Adults (baseline: n = 27,141, analysed at follow-up: n = 9748) | Association between lockdown and … | ||
| Model 1 * | Model 2 ** | ||||
| RR (95 % CI) | RR (95 % CI) | ||||
| Current smoking | |||||
| During COVID-19 | 0.80 (0.69–0.93) | 0.88 (0.78–0.98) | |||
| Regular e-cigarette use | |||||
| During COVID-19 | 0.68 (0.46–1.01) | 0.61 (0.43–0.86) | |||
| * adjusted for year, age group, gender, ethnicity, period and period × age group interaction ** adjusted for year, age group, gender, ethnicity, period and period × gender interaction | |||||
| Cicero et al., 2021 [77] (Cross-sectional study) | Italy | Adults (n = 359) | Change since lockdown | ||
| Prevalence (%) | |||||
| Reduction | 2.2 | ||||
| Increase | 1.7 | ||||
| Radwan et al., 2021 [90] (Cross-sectional study) | United Arab Emirates | Adults (n = 2060) | Change since lockdown | ||
| Prevalence (n (%)) | |||||
| Increase | 50 (21.0) | ||||
| Decrease | 93 (39.1) | ||||
| Same | 95 (39.9) | ||||
| Bourion-Bedes et al., 2021 [76] (Cross-sectional study) | France | Students (n = 3936) | Change since lockdown | ||
| Prevalence (%) | |||||
| None | 83.5 | ||||
| No change | 3 | ||||
| Increased | 7.2 | ||||
| Reduced | 6.3 | ||||
| Berard et al., 2021 [75] (Cross-sectional study) | France | Older adults (aged ≥ 50 years) (n = 536) | Change since lockdown | ||
| Prevalence (n (%)) | |||||
| Increased smoking | 21 (4.0) | ||||
3.4.7. Antihypertensive/Lipid-Lowering/Hypoglycaemic Medication
| Reference (Study Design) | Country | Population (Sample Size) | Results | |
|---|---|---|---|---|
| Adults | ||||
| Berard et al., 2021 [75] (Cross-sectional study) | France | Older adults (aged ≥ 50 years) (n = 536) | Change since lockdown | |
| Prevalence (n (%)) | ||||
| Increased antihypertensive, lipid-lowering, or hypoglycaemic drug treatment | 2 (0.37) | |||
4. Discussion
4.1. Summary of Findings
4.2. Discussion of Findings
4.3. Practical Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gori, T.; Lelieveld, J.; Münzel, T. Perspective: Cardiovascular disease and the COVID-19 pandemic. Basic Res. Cardiol. 2020, 115, 32. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Bovo, C.; Sanchis-Gomar, F. Health risks and potential remedies during prolonged lockdowns for coronavirus disease 2019 (COVID-19). Diagnosis 2020, 7, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19 Related School Closings and Risk of Weight Gain among Children. Obesity 2020, 28, 1008–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscogiuri, G.; Barrea, L.; Savastano, S.; Colao, A. Nutritional recommendations for CoVID-19 quarantine. Eur. J. Clin. Nutr. 2020, 74, 850–851. [Google Scholar] [CrossRef] [PubMed]
- García-Álvarez, L.; Fuente-Tomás, L.; Sáiz, P.A.; García-Portilla, M.P.; Bobes, J. Will changes in alcohol and tobacco use be seen during the COVID-19 lockdown? Adicciones 2020, 32, 85–89. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Ballerini Puviani, M. Lifestyle at Time of COVID-19: How Could Quarantine Affect Cardiovascular Risk. Am. J. Lifestyle. Med. 2020, 14, 240–242. [Google Scholar] [CrossRef] [PubMed]
- Gierveld, J.; van Tilburg, T.; Dykstra, P. Loneliness and Social Isolation. In The Cambridge Handbook of Personal Relationships; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Röhr, S.; Müller, F.; Jung, F.; Riedel-Heller, S. Psychosoziale Folgen von Quarantänemaßnahmen bei schwerwiegenden Coronavirus-Ausbrüchen: Ein Rapid Review. Psychiatr. Prax. 2020, 47, 179–189. [Google Scholar] [PubMed]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care. Community 2017, 25, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Hawkley, L.C.; Capitanio, J.P. Perceived social isolation, evolutionary fitness and health outcomes: A lifespan approach. Philos. Trans. R Soc. Lond. B Biol. Sci. 2015, 370, 20140114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef]
- Koeneman, M.A.; Verheijden, M.W.; Chinapaw, M.J.; Hopman-Rock, M. Determinants of physical activity and exercise in healthy older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, S.A.; Reed, J.L.; Martinello, N.; Adamo, K.B.; Fodor, J.G.; Hiremath, S.; Kristjansson, E.A.; Mullen, K.A.; Nerenberg, K.A.; Tulloch, H.E.; et al. Why are adult women physically active? A systematic review of prospective cohort studies to identify intrapersonal, social environmental and physical environmental determinants. Obes. Rev. 2016, 17, 919–944. [Google Scholar] [CrossRef]
- Wendel-Vos, W.; Droomers, M.; Kremers, S.; Brug, J.; van Lenthe, F. Potential environmental determinants of physical activity in adults: A systematic review. Obes. Rev. 2007, 8, 425–440. [Google Scholar] [CrossRef] [PubMed]
- Kauppi, M.; Elovainio, M.; Stenholm, S.; Virtanen, M.; Aalto, V.; Koskenvuo, M.; Kivimäki, M.; Vahtera, J. Social networks and patterns of health risk behaviours over two decades: A multi-cohort study. J. Psychosom. Res. 2017, 99, 45–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, L.C.; Steptoe, A. Social Isolation, Loneliness, and Health Behaviors at Older Ages: Longitudinal Cohort Study. Ann. Behav. Med. 2018, 52, 582–593. [Google Scholar] [CrossRef] [Green Version]
- Josey, M.J.; Moore, S. The influence of social networks and the built environment on physical inactivity: A longitudinal study of urban-dwelling adults. Health Place 2018, 54, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Dyal, S.R.; Valente, T.W. A Systematic Review of Loneliness and Smoking: Small Effects, Big Implications. Subst. Use Misuse 2015, 50, 1697–1716. [Google Scholar] [CrossRef] [Green Version]
- Oyewole, B.K.; Animasahun, V.J.; Chapman, H.J. Tobacco use in Nigerian youth: A systematic review. PLoS ONE 2018, 13, e0196362. [Google Scholar] [CrossRef] [Green Version]
- Barbosa Filho, V.C.; Campos, W.; Lopes Ada, S. Prevalence of alcohol and tobacco use among Brazilian adolescents: A systematic review. Rev. Saude Publica 2012, 46, 901–917. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.J.; Smith, R.A. Members, isolates, and liaisons: Meta-analysis of adolescents’ network positions and their smoking behavior. Subst. Use Misuse 2013, 48, 612–622. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, S.C.; Donnelly, M.; Bhatnagar, P.; Carlin, A.; Kee, F.; Hunter, R.F. Peer social network processes and adolescent health behaviors: A systematic review. Prev. Med. 2020, 130, 105900. [Google Scholar] [CrossRef] [PubMed]
- Seo, D.C.; Huang, Y. Systematic review of social network analysis in adolescent cigarette smoking behavior. J. Sch. Health. 2012, 82, 21–27. [Google Scholar] [CrossRef]
- Moore, S.; Teixeira, A.; Stewart, S. Effect of network social capital on the chances of smoking relapse: A two-year follow-up study of urban-dwelling adults. Am. J. Public. Health 2014, 104, e72–e76. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Olanrewaju, O.; Cowan, A.; Brayne, C.; Lafortune, L. Alcohol and older people: A systematic review of barriers, facilitators and context of drinking in older people and implications for intervention design. PLoS ONE 2018, 13, e0191189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanesby, O.; Labhart, F.; Dietze, P.; Wright, C.J.C.; Kuntsche, E. The contexts of heavy drinking: A systematic review of the combinations of context-related factors associated with heavy drinking occasions. PLoS ONE 2019, 14, e0218465. [Google Scholar] [CrossRef] [PubMed]
- Cuffee, Y.; Ogedegbe, C.; Williams, N.J.; Ogedegbe, G.; Schoenthaler, A. Psychosocial risk factors for hypertension: An update of the literature. Curr. Hypertens. Rep. 2014, 16, 483. [Google Scholar] [CrossRef] [PubMed]
- Petitte, T.; Mallow, J.; Barnes, E.; Petrone, A.; Barr, T.; Theeke, L. A Systematic Review of Loneliness and Common Chronic Physical Conditions in Adults. Open Psychol. J. 2015, 8 (Suppl. S2), 113–132. [Google Scholar] [CrossRef] [PubMed]
- Valtorta, N.K.; Kanaan, M.; Gilbody, S.; Ronzi, S.; Hanratty, B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart 2016, 102, 1009–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, C.A.; Thurston, R.C.; Matthews, K.A. Psychosocial factors in the development of heart disease in women: Current research and future directions. Psychosom. Med. 2010, 72, 842–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prati, G.; Mancini, A.D. The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 2021, 51, 201–211. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2021, 75, 224–231. [Google Scholar] [PubMed]
- Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in Physical Activity, Sleep Quality, and Psychosocial Variables during COVID-19 Lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2020, 18, 210. [Google Scholar] [CrossRef] [PubMed]
- Ramalho, R. Alcohol consumption and alcohol-related problems during the COVID-19 pandemic: A narrative review. Australas. Psychiatry 2020, 28, 524–526. [Google Scholar] [CrossRef]
- Zupo, R.; Castellana, F.; Sardone, R.; Sila, A.; Giagulli, V.A.; Triggiani, V.; Cincione, R.I.; Giannelli, G.; De Pergola, G. Preliminary Trajectories in Dietary Behaviors during the COVID-19 Pandemic: A Public Health Call to Action to Face Obesity. Int. J. Environ. Res. Public Health 2020, 17, 7073. [Google Scholar] [CrossRef] [PubMed]
- Pinho, C.S.; Caria, A.C.I.; Aras Júnior, R.; Pitanga, F.J.G. The effects of the COVID-19 pandemic on levels of physical fitness. Rev. Assoc. Med. Bras. 2020, 66 (Suppl. S2), 34–37. [Google Scholar] [CrossRef]
- Cachón-Zagalaz, J.; Sánchez-Zafra, M.; Sanabrias-Moreno, D.; González-Valero, G.; Lara-Sánchez, A.J.; Zagalaz-Sánchez, M.L. Systematic Review of the Literature About the Effects of the COVID-19 Pandemic on the Lives of School Children. Front. Psychol. 2020, 11, 569348. [Google Scholar] [CrossRef] [PubMed]
- Stavridou, A.; Kapsali, E.; Panagouli, E.; Thirios, A.; Polychronis, K.; Bacopoulou, F.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Obesity in Children and Adolescents during COVID-19 Pandemic. Children 2021, 8, 135. [Google Scholar] [CrossRef]
- López-Bueno, R.; López-Sánchez, G.F.; Casajús, J.A.; Calatayud, J.; Tully, M.A.; Smith, L. Potential health-related behaviors for pre-school and school-aged children during COVID-19 lockdown: A narrative review. Prev. Med. 2021, 143, 106349. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Suárez-Iglesias, D.; Sanchez-Lastra, M.A.; Ayán, C. Impact of COVID-19 Pandemic on University Students’ Physical Activity Levels: An Early Systematic Review. Front. Psychol. 2020, 11, 624567. [Google Scholar] [CrossRef]
- Chandrasekaran, B.; Ganesan, T.B. Sedentarism and chronic disease risk in COVID 19 lockdown—A scoping review. Scott. Med. J. 2021, 66, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, R.; Martin, L.; Shearer, E.; Greci, S. Rapid International Evidence Review: Impact of the COVID-19 Disease Control Measures on Physical Activity and Dietary Behaviours and Weight. Public Health Scotland. 2020. Available online: https://publichealthscotland.scot/media/2844/impact-of-the-covid-19-disease-control-measures-on-physical-activity-and-dietary-behaviours-and-weight-oct2020-english.pdf (accessed on 4 June 2021).
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.I.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef] [PubMed]
- Chtourou, H.; Trabelsi, K.; H’Mida, C.; Boukhris, O.; Glenn, J.M.; Brach, M.; Bentlage, E.; Bott, N.; Shephard, R.J.; Ammar, A.; et al. Staying Physically Active During the Quarantine and Self-Isolation Period for Controlling and Mitigating the COVID-19 Pandemic: A Systematic Overview of the Literature. Front. Psychol. 2020, 11, 1708. [Google Scholar] [CrossRef] [PubMed]
- Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; Sansano-Nadal, O.; Guerra-Balic, M. Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9419. [Google Scholar] [CrossRef]
- Abdo, C.; Miranda, E.P.; Santos, C.S.; de Bessa Júnior, J.; Bernardo, W.M. Domestic violence and substance abuse during COVID-19: A systematic review. Indian J. Psychiatry 2020, 62 (Suppl. S3), S337–S342. [Google Scholar] [CrossRef]
- Banerjee, D.; Vaishnav, M.; Rao, T.S.; Raju, M.; Dalal, P.K.; Javed, A.; Saha, G.; Mishra, K.K.; Kumar, V.; Jagiwala, M.P. Impact of the COVID-19 pandemic on psychosocial health and well-being in South-Asian (World Psychiatric Association zone 16) countries: A systematic and advocacy review from the Indian Psychiatric Society. Indian J. Psychiatry 2020, 62 (Suppl. S3), S343–S353. [Google Scholar] [CrossRef]
- Imran, N.; Aamer, I.; Sharif, M.I.; Bodla, Z.H.; Naveed, S. Psychological burden of quarantine in children and adolescents: A rapid systematic review and proposed solutions. Pak. J. Med. Sci. 2020, 36, 1106–1116. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.; Young, E.; Butler, I.; Coe, S. The Impact of Lockdown during the COVID-19 Outbreak on Dietary Habits in Various Population Groups: A Scoping Review. Front. Nutr. 2021, 8, 626432. [Google Scholar] [CrossRef] [PubMed]
- Tyrer, S.; Heyman, B. Sampling in epidemiological research: Issues, hazards and pitfalls. BJ Psych. Bull. 2016, 40, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Kunz, R.; Khan, K.; Kleijnen, J.; Antes, G. Systematische Übersichtsarbeiten und Meta-Analysen. In Einführung in Instrumente der Evidenzbasierten Medizin für Ärzte, Klinische Forscher und Experten im Gesundheitswesen; Huber: Bern, Switzerland, 2009. [Google Scholar]
- WHO. Cardiovascular Diseases (CVDs). World Health Organization. 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 4 June 2021).
- WHF. Cardiovascular Risk Factors. World Heart Federation. 2017. Available online: https://www.world-heart-federation.org/resources/risk-factors/ (accessed on 4 June 2021).
- Seidler, A.; Nußbaumer-Streit, B.; Apfelbacher, C.; Zeeb, H. Rapid Reviews in the Time of COVID-19—Experiences of the Competence Network Public Health COVID-19 and Proposal for a Standardized Procedure. Gesundheitswesen 2021, 83, 173–179. [Google Scholar]
- Freiberg, A.; Schubert, M.; Romero Starke, K.; Hegewald, J.; Seidler, A. Influence of COVID-19 Lockdown and Quarantine Measures on Modifiable Cardiovascular Risk Factors: A Rapid Review. PROSPERO. 2020. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020222405 (accessed on 4 June 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Participants, S.T.C.P. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, C.; Gerds, T.; Fosbøl, E.; Phelps, M.; Andersen, J.; Lamberts, M.; Holt, A.; Butt, J.H.; Madelaire, C.; Gislason, G.; et al. Incidence of New-Onset and Worsening Heart Failure Before and After the COVID-19 Epidemic Lockdown in Denmark: A Nationwide Cohort Study. Circ. Heart Fail. 2020, 13, e007274. [Google Scholar] [CrossRef] [PubMed]
- Bromage, D.I.; Cannatà, A.; Rind, I.A.; Gregorio, C.; Piper, S.; Shah, A.M.; McDonagh, T.A. The impact of COVID-19 on heart failure hospitalization and management: Report from a Heart Failure Unit in London during the peak of the pandemic. Eur. J. Heart. Fail. 2020, 22, 978–984. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersen, E.S.; Jahr, S.H.; Thommessen, B.; Rønning, O.M. Effect of COVID-19 pandemic on stroke admission rates in a Norwegian population. Acta. Neurol. Scand. 2020, 142, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Hauguel-Moreau, M.; Pillière, R.; Prati, G.; Beaune, S.; Loeb, T.; Lannou, S.; Mallet, S.; Mustafic, H.; Bégué, C.; Dubourg, O.; et al. Impact of Coronavirus Disease 2019 outbreak on acute coronary syndrome admissions: Four weeks to reverse the trend. J. Thromb. Thrombolysis 2021, 51, 31–32. [Google Scholar] [CrossRef]
- Hoyer, C.; Ebert, A.; Huttner, H.B.; Puetz, V.; Kallmünzer, B.; Barlinn, K.; Haverkamp, C.; Harloff, A.; Brich, J.; Platten, M.; et al. Acute Stroke in Times of the COVID-19 Pandemic: A Multicenter Study. Stroke 2020, 51, 2224–2227. [Google Scholar] [CrossRef]
- Rudilosso, S.; Laredo, C.; Vera, V.; Vargas, M.; Renú, A.; Llull, L.; Obach, V.; Amaro, S.; Urra, X.; Torres, F.; et al. Acute Stroke Care Is at Risk in the Era of COVID-19: Experience at a Comprehensive Stroke Center in Barcelona. Stroke 2020, 51, 1991–1995. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Ijaz, S.; Verbeek, J.; Seidler, A.; Lindbohm, M.L.; Ojajärvi, A.; Orsini, N.; Costa, G.; Neuvonen, K. Night-shift work and breast cancer--a systematic review and meta-analysis. Scand. J. Work. Environ. Health 2013, 39, 431–447. [Google Scholar] [CrossRef]
- Kuijer, P.; Verbeek, J.H.; Seidler, A.; Ellegast, R.; Hulshof, C.T.J.; Frings-Dresen, M.H.W.; Van der Molen, H.F. Work-relatedness of lumbosacral radiculopathy syndrome: Review and dose-response meta-analysis. Neurology 2018, 91, 558–564. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Alpers, S.E.; Skogen, J.C.; Mæland, S.; Pallesen, S.; Rabben, Å.K.; Lunde, L.H.; Fadnes, L.T. Alcohol Consumption during a Pandemic Lockdown Period and Change in Alcohol Consumption Related to Worries and Pandemic Measures. Int. J. Environ. Res. Public Health 2021, 18, 1220. [Google Scholar] [CrossRef]
- Anyan, F.; Hjemdal, O.; Ernstsen, L.; Havnen, A. Change in Physical Activity during the Coronavirus Disease 2019 Lockdown in Norway: The Buffering Effect of Resilience on Mental Health. Front. Psychol. 2020, 11, 598481. [Google Scholar] [CrossRef]
- Ernstsen, L.; Havnen, A. Mental health and sleep disturbances in physically active adults during the COVID-19 lockdown in Norway: Does change in physical activity level matter? Sleep Med. 2021, 77, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Avery, A.R.; Tsang, S.; Seto, E.Y.W.; Duncan, G.E. Stress, Anxiety, and Change in Alcohol Use During the COVID-19 Pandemic: Findings among Adult Twin Pairs. Front. Psychiatry 2020, 11, 571084. [Google Scholar] [CrossRef] [PubMed]
- Duncan, G.E.; Avery, A.R.; Seto, E.; Tsang, S. Perceived change in physical activity levels and mental health during COVID-19: Findings among adult twin pairs. PLoS ONE 2020, 15, e0237695. [Google Scholar] [CrossRef]
- Barkley, J.E.; Lepp, A.; Glickman, E.; Farnell, G.; Beiting, J.; Wiet, R.; Dowdell, B. The Acute Effects of the COVID-19 Pandemic on Physical Activity and Sedentary Behavior in University Students and Employees. Int. J. Exerc. Sci. 2020, 13, 1326–1339. [Google Scholar] [PubMed]
- Bérard, E.; Huo Yung Kai, S.; Coley, N.; Bongard, V.; Ferrières, J. Lockdown-related factors associated with the worsening of cardiovascular risk and anxiety or depression during the COVID-19 pandemic. Prev. Med. Rep. 2021, 21, 101300. [Google Scholar] [CrossRef]
- Bourion-Bédès, S.; Tarquinio, C.; Batt, M.; Tarquinio, P.; Lebreuilly, R.; Sorsana, C.; Legrand, K.; Rousseau, H.; Baumann, C. Psychological impact of the COVID-19 outbreak on students in a French region severely affected by the disease: Results of the PIMS-CoV 19 study. Psychiatry Res. 2021, 295, 113559. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Giovannini, M.; Mezzadri, M.; Grandi, E.; Borghi, C.; The Brisighella Heart Study Group. COVID-19-Related Quarantine Effect on Dietary Habits in a Northern Italian Rural Population: Data from the Brisighella Heart Study. Nutrients 2021, 13, 309. [Google Scholar] [CrossRef]
- Colley, R.C.; Bushnik, T.; Langlois, K. Exercise and screen time during the COVID-19 pandemic. Health Rep. 2020, 31, 3–11. [Google Scholar] [PubMed]
- Crochemore-Silva, I.; Knuth, A.G.; Wendt, A.; Nunes, B.P.; Hallal, P.C.; Santos, L.P.; Harter, J.; Pellegrini, D. Physical activity during the COVID-19 pandemic: A population-based cross-sectional study in a city of South Brazil. Cien. Saude. Colet. 2020, 25, 4249–4258. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. High-Risk Drinking in Midlife Before Versus During the COVID-19 Crisis: Longitudinal Evidence From the United Kingdom. Am. J. Prev. Med. 2021, 60, 294–297. [Google Scholar] [CrossRef]
- Di Sebastiano, K.M.; Chulak-Bozzer, T.; Vanderloo, L.M.; Faulkner, G. Don’t Walk So Close to Me: Physical Distancing and Adult Physical Activity in Canada. Front. Psychol. 2020, 11, 1895. [Google Scholar] [CrossRef] [PubMed]
- Garre-Olmo, J.; Turró-Garriga, O.; Martí-Lluch, R.; Zacarías-Pons, L.; Alves-Cabratosa, L.; Serrano-Sarbosa, D.; Vilalta-Franch, J.; Ramos, R. Changes in lifestyle resulting from confinement due to COVID-19 and depressive symptomatology: A cross-sectional a population-based study. Compr. Psychiatry 2021, 104, 152214. [Google Scholar] [CrossRef] [PubMed]
- Karuc, J.; Sorić, M.; Radman, I.; Mišigoj-Duraković, M. Moderators of Change in Physical Activity Levels during Restrictions Due to COVID-19 Pandemic in Young Urban Adults. Sustainability 2020, 12, 6392. [Google Scholar] [CrossRef]
- Lechner, W.V.; Laurene, K.R.; Patel, S.; Anderson, M.; Grega, C.; Kenne, D.R. Changes in alcohol use as a function of psychological distress and social support following COVID-19 related University closings. Addict. Behav. 2020, 110, 106527. [Google Scholar] [CrossRef]
- Mason, T.B.; Barrington-Trimis, J.; Leventhal, A.M. Eating to Cope With the COVID-19 Pandemic and Body Weight Change in Young Adults. J. Adolesc. Health 2021, 68, 277–283. [Google Scholar] [CrossRef] [PubMed]
- McCormack, G.R.; Doyle-Baker, P.K.; Petersen, J.A.; Ghoneim, D. Parent anxiety and perceptions of their child’s physical activity and sedentary behaviour during the COVID-19 pandemic in Canada. Prev. Med. Rep. 2020, 20, 101275. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2021, 16, e12731. [Google Scholar] [CrossRef]
- Özden, G.; Parlar Kiliç, S. The Effect of Social Isolation during COVID-19 Pandemic on Nutrition and Exercise Behaviors of Nursing Students. Ecol. Food. Nutr. 2021, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Ozturk Eyimaya, A.; Yalçin Irmak, A. Relationship between Parenting Practices and Children’s Screen Time During the COVID-19 Pandemic in Turkey. J. Pediatr. Nurs. 2021, 56, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Radwan, H.; Al Kitbi, M.; Hasan, H.; Al Hilali, M.; Abbas, N.; Hamadeh, R.; Saif, E.R.; Naja, F. Indirect Health Effects of COVID-19: Unhealthy Lifestyle Behaviors during the Lockdown in the United Arab Emirates. Int. J. Environ. Res. Public Health 2021, 18, 1964. [Google Scholar] [CrossRef]
- Sasaki, S.; Sato, A.; Tanabe, Y.; Matsuoka, S.; Adachi, A.; Kayano, T.; Yamazaki, H.; Matsuno, Y.; Miyake, A.; Watanabe, T. Associations between Socioeconomic Status, Social Participation, and Physical Activity in Older People during the COVID-19 Pandemic: A Cross-Sectional Study in a Northern Japanese City. Int. J. Environ. Res. Public Health 2021, 18, 1477. [Google Scholar] [CrossRef]
- Savage, M.J.; Hennis, P.J.; Magistro, D.; Donaldson, J.; Healy, L.C.; James, R.M. Nine Months into the COVID-19 Pandemic: A Longitudinal Study Showing Mental Health and Movement Behaviours Are Impaired in UK Students. Int. J. Environ. Res. Public Health 2021, 18, 2930. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.C.E.; Anedda, B.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Nigg, C.; Niessner, C.; Oriwol, D.; Worth, A.; Woll, A. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: A natural experiment. Sci. Rep. 2020, 10, 21780. [Google Scholar] [CrossRef] [PubMed]
- To, Q.G.; Duncan, M.J.; Van Itallie, A.; Vandelanotte, C. Impact of COVID-19 on Physical Activity Among 10,000 Steps Members and Engagement with the Program in Australia: Prospective Study. J. Med. Internet Res. 2021, 23, e23946. [Google Scholar] [CrossRef]
- Tornaghi, M.; Lovecchio, N.; Vandoni, M.; Chirico, A.; Codella, R. Physical activity levels across COVID-19 outbreak in youngsters of Northwestern Lombardy. J. Sports Med. Phys. Fitness 2020. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Bennell, K.; White, D.K.; Wei, J.; Wu, Z.; He, H.; Liu, S.; Luo, X.; Hu, S.; et al. Physical Distancing Measures and Walking Activity in Middle-aged and Older Residents in Changsha, China, During the COVID-19 Epidemic Period: Longitudinal Observational Study. J. Med. Internet Res. 2020, 22, e21632. [Google Scholar] [CrossRef]
- White, H.R.; Stevens, A.K.; Hayes, K.; Jackson, K.M. Changes in Alcohol Consumption among College Students Due to COVID-19: Effects of Campus Closure and Residential Change. J. Stud. Alcohol Drugs 2020, 81, 725–730. [Google Scholar] [CrossRef]
- Wickersham, A.; Carr, E.; Hunt, R.; Davis, J.P.; Hotopf, M.; Fear, N.T.; Downs, J.; Leightley, D. Changes in Physical Activity among United Kingdom University Students Following the Implementation of Coronavirus Lockdown Measures. Int. J. Environ. Res. Public Health 2021, 18, 2792. [Google Scholar] [CrossRef]
- Yamada, Y.; Uchida, T.; Ogino, M.; Ikenoue, T.; Shiose, T.; Fukuma, S. Changes in Older People’s Activities during the Coronavirus Disease 2019 Pandemic in Japan. J. Am. Med. Dir. Assoc. 2020, 21, 1387–1388. [Google Scholar] [CrossRef]
- Richter, D.; Riedel-Heller, S.; Zürcher, S.J. Mental health problems in the general population during and after the first lockdown phase due to the SARS-Cov-2 pandemic: Rapid review of multi-wave studies. Epidemiol. Psychiatr. Sci. 2021, 30, e27. [Google Scholar] [CrossRef]
- Dixit, S.; Nandakumar, G. Promoting healthy lifestyles using information technology during the COVID-19 pandemic. Rev. Cardiovasc. Med. 2021, 22, 115–125. [Google Scholar] [CrossRef]
- Alexander, S.A.; Shareck, M. Widening the gap? Unintended consequences of health promotion measures for young people during COVID-19 lockdown. Health. Promot. Int. 2021. [Google Scholar] [CrossRef]
- Srivastav, A.K.; Khadayat, S.; Samuel, A.J. Mobile-Based Health Apps to Promote Physical Activity during COVID-19 Lockdowns. J. Rehabil. Med. Clin. Commun. 2021, 4, 1000051. [Google Scholar] [PubMed]
- Fallon, K. Exercise in the time of COVID-19. Aust. J. Gen. Pract. 2020, 49. [Google Scholar] [CrossRef]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Polero, P.; Rebollo-Seco, C.; Adsuar, J.C.; Pérez-Gómez, J.; Rojo-Ramos, J.; Manzano-Redondo, F.; Garcia-Gordillo, M.Á.; Carlos-Vivas, J. Physical Activity Recommendations during COVID-19: Narrative Review. Int. J. Environ. Res. Public Health 2020, 18, 65. [Google Scholar] [CrossRef]
- Ghram, A.; Briki, W.; Mansoor, H.; Al-Mohannadi, A.S.; Lavie, C.J.; Chamari, K. Home-based exercise can be beneficial for counteracting sedentary behavior and physical inactivity during the COVID-19 pandemic in older adults. Postgrad. Med. 2020, 133, 469–480. [Google Scholar] [CrossRef]
- Füzéki, E.; Groneberg, D.A.; Banzer, W. Physical activity during COVID-19 induced lockdown: Recommendations. J. Occup. Med. Toxicol. 2020, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.H.; Synnot, A.; Turner, T.; Simmonds, M.; Akl, E.A.; McDonald, S.; Salanti, G.; Meerpohl, J.; MacLehose, H.; Hilton, J.; et al. Living systematic review: 1. Introduction-the why, what, when, and how. J. Clin. Epidemiol. 2017, 91, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, J.H.; Turner, T.; Clavisi, O.; Thomas, J.; Higgins, J.P.T.; Mavergames, C.; Gruen, R.L. Living systematic reviews: An emerging opportunity to narrow the evidence-practice gap. PLoS Med. 2014, 11, e1001603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fassin, Y. Research on COVID-19: A disruptive phenomenon for bibliometrics. Scientometrics 2021, 126, 5305–5319. [Google Scholar] [CrossRef] [PubMed]

| Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | healthy humans of the general population (also including subgroups like pupils, students, or workers) of all ages (i.e., children, adolescents, adults, and older adults) | patient populations only (e.g., obese patients, diabetes patients, patients with cardiovascular diseases) animals |
| Exposure | quarantine/isolation and lockdown measures during the COVID-19 pandemic | quarantine/isolation and lockdown measures during other pandemics (e.g., SARS, MERS, Ebola) |
| Comparison | no or other forms of quarantine/isolation and lockdown measures | no comparison |
| Outcome | modifiable cardiovascular risk factors: physical inactivity sedentary behaviour harmful use of alcohol tobacco use unhealthy diet (excessive consumption of (saturated) fat, salt, and sugar, and low intake of fruits and vegetables) obesity bad blood lipids (hyperlipidaemia, hypercholesterolemia, hypertriglyceridemia) hypertension | non-modifiable cardiovascular risk factors (e.g., family history, diabetes, socioeconomic status) cardiovascular diseases (myocardial infarction, stroke, thrombosis, embolism, arteriosclerosis) other acute or chronic diseases (e.g., mental disorders, cognitive impairments, musculoskeletal disorders) environmental (air pollution, traffic noise) and work-related risk factors (shift work, long working hours) |
| Study design | epidemiological observational studies (cohort studies, case-control studies, cross-sectional studies) | qualitative studies (interview studies, focus group studies) clinical epidemiological studies (case series, case reports) subjective study types (editorial, commentary, expert opinion) animal studies reviews only abstract available |
| Reference, Overall Risk of Bias | Region, Study Design | Time of Survey | Population (Sample Size (% Female), Age (Mean or Median), Response, Lost to Follow-Up (in Cohort Studies)) | Exposure * | Outcome |
|---|---|---|---|---|---|
| Alpers et al., 2021 [69], High risk | Norway, Cross-sectional study | 15–30 April 2020 | Adults Sample size: n = 25,708 (56.2% female) Age (median (IQR)): 50 years (36–63) Response: 31.7% | COVID-19 pandemic measures (implemented on 12 March 2020)
| Alcohol consumption: Alcohol Use Disorders Identification Test Consumption, self-reported question about change |
| Anyan et al., 2020 [70], Ernsten and Havnen 2020 [71], High risk | Norway, Cross-sectional study | 3–15 June 2020 | Physically active adults (members of one Norwegian fitness association) Sample size: n = 1314 (30.8% female) Age (mean (SD)): 49 years (11.5) Response: 19.4% | COVID-19 pandemic lockdown (12 March–15 June 2020) - measures: n.r. | Physical activity: self-reported question about change |
| Avery et al., 2020 [72], High risk | United States, Cross-sectional study | 26 March 2020–5 April 2020 | (Identical, same-sex fraternal) adult twins Sample size: n = 3971 (69.2% female) Age (mean (SD)): 50.4 years (16.0) Response: individual: 32.8%, pairwise: 21.1% | COVID-19 mitigation strategies (Washington implemented the state-wide “stay home, stay healthy” order on 24 March 2020) - measures: n.r. | Alcohol use: self-reported question about change |
| Barkley et al., 2020 [74], High risk | United States, Cross-sectional study | 18 May–18 June 2020 | University students Sample size: n = 184 (73.2% female (of all participants incl. university staff)) Age (mean (SD)): undergraduate students: 26.9 years (8.9), graduate students: 29.9 years (8.7) Response: 3.7% | Campus closure due to the COVID-19 pandemic (since 11 March 2020) - measures: cancellation of face-to-face classes, closure of the campus, including all fitness facilities, students were sent home, governor’s “stay at home” order (22 March 2020) | Physical activity: Godin physical activity questionnaire Sedentary behaviour: International Physical Activity Questionnaire Weight: self-reported question |
| Berard et al., 2021 [75], High risk | France, Cross-sectional study | 17 April–10 May 2020 | Older adults (aged ≥50 years) Sample size: n = 536 (52% female) Age (mean (range)): 67 years (50–89) Response: 69% | COVID-19 lockdown (17 March–10 May 2020)
| Dietary quality: Short, qualitative food frequency questionnaire Physical activity, weight, smoking, antihypertensive, lipid-lowering or hypoglycaemic drug treatment: self-reported question about change |
| Bourion-Bedes et al., 2021 [76], High risk | France, Cross-sectional study | 7–17 May 2020 | Students Sample size: n = 3936 (70.6% female) Age (mean (SD)): 21.7 years (4.0) Response: around 7.9% | Lockdown due to the COVID-19 outbreak - measures: n.r. | Alcohol consumption, smoking: self-reported question about change |
| Cicero et al., 2021 [77], High risk | Italy, Cross-sectional study | n.r. | Adults Sample size: n = 359 (56.5% female) Age (mean (SD)): 64.6 years (13.3) Response: 23.3% | COVID-19-related quarantine (February–April 2020) - measures: n.r. | Dietary quality: Dietary Quality Index Alcohol consumption: 1 item from the Dietary Quality Index Smoking, body mass index: 1 self-reported question |
| Colley et al., 2020 [78], High risk | Canada, Cross-sectional study | 29 March–3 April 2020 | Adults Sample size: n = 4524 (53.4% female) Age: n.r. Response: 62.5% | Physical distancing measures (implemented in March 2020): - measures: border, school, and business closures, avoiding unnecessary trips | Screen time behaviours: 3 self-reported questions |
| Crochemore-Silva et al., 2020 [79], High risk | Brazil, Cross-sectional study | 7–9 May 2020 | Adults Sample size: n = 377 (62.9% female) Age: n.r. Response: 94.3% | Social distancing
| Leisure-time physical activity: 1 item from an adapted version of the International Physical Activity Questionnaire |
| Daly and Robinson, 2021 [80], High risk | United Kingdom, Cohort study | T1: 2016–2018 T2: May 2020 | Adults born in Britain in 1970 Sample size at follow-up: n = 3358 (50% female) Age (range): 46–48 years Response at follow-up: 32.1% Lost to follow-up: n.r. | COVID-19 lockdown restrictions (between late March and early July 2020) - measures: closure of pubs, bars, and restaurants and other nonessential businesses | High-risk alcohol consumption: Alcohol Use Disorders Identification Test |
| Di Sebastiano et al., 2020 [81], High risk | Canada, (Prospective) secondary data analyses | 10 February–19 April 2020 T0: 4 weeks prior physical distancing protocols T1: 1 weeks after the beginning of the physical distancing protocols T2: 6 weeks after physical distancing protocols | Adults (≥18 years) using a physical activity tracking ParticipACTION app Sample size: n = 2338 (90.2% female) Age: n.r. Response: n.a. Lost-to follow-up: n.a. (only complete data sets used) | Physical distancing protocols - measures: n.r. | Physical activity: data from a national physical activity tracking app based on steps |
| Duncan et al., 2020 [73], High risk | United States, Cross-sectional study | 26 March–5 April 2020 | (Identical, same-sex fraternal) adult twins Sample size: n = 3971 (69.2% female) Age (mean (SD)): 50.4 years (16.0) Response: individual: 32.8%, pair-wise: 21.1% | COVID-19 mitigation strategies (Washington implemented the state-wide “stay home, stay healthy” order on 24 March 2020) - measures: n.r. | Physical activity: 1 self-reported question about change |
| Garre-Olmo et al., 2020 [82], High risk | Spain, Cross-sectional study | 8 April–4 May 2020 | Adults Sample size: n = 692 (54.8% female) Age (mean (SD)): 50.2 years (16.3) Response: 90.5% | Movement restrictions and confinement due to the COVID-19 pandemic (implemented on 15 March 2020) - measures: suspension of all academic activities, obligation to stay at home except to purchase food and medicines, to go to work, or to attend emergencies, more restrictive lockdown period including the temporary closure of all the non-essential activities and businesses (29 March–9 April 2020) | Physical activity, dietary pattern: 1 self-reported question about change |
| Karuc et al., 2020 [83], High risk | Croatia, Cross-sectional study | 24 April–8 May 2020 | Young adults Sample size: n = 91 (64.8% female) Age (mean (SD)): 21.6 years (0.4) Response: 25.1% | Restrictions due to COVID-19 Pandemic (19 March–11 May 2020) - measures: restriction of gatherings in public places and parks, suspension of public transportation, closing of institutions, prohibition of all social gatherings, work in retail and services including sports activities | Physical activity: 7-day recall of moderate intensity physical activity (MPA) and vigorous intensity physical activity (VPA): School Health Action, Planning, Evaluation System (SHAPES) questionnaire, 1 self-reported question about change |
| Lechner et al., 2020 [84], High risk | United States, Cross-sectional study | 26–31 March 2020 | Students (using alcohol in the past 30 days) Sample size: n = 1958 (80% female) Age (mean (SD)): 24.94 (7.65) Response: 12.8% (all students) | University closings (on 11 March 2020) - measures: n.r. | Alcohol consumption: Timeline Follow-Back Interview |
| Mason et al., 2020 [85], High risk | United States, Cohort study | T1: October 2018–October 2019 T2: May–July 2020 | Young adults Sample size at follow-up: n = 1820 (61.5% female) Age (mean (SD)): 19.72 years (0.47) Response at follow-up: 71.4% Lost to follow-up: n.r. | COVID-19 restrictions - measures: n.r. | Weight: 1 self-reported question about change |
| McCormack et al., 2020 [86], High risk | Canada, Cross-sectional study | 14 April–27 May 2020 | Children (5–17 years) Sample size: n = 328 (45.1% female) Age: n.r. Response: 4.5% (adults) | COVID-19 public health emergency response - measures: forced closures of educational and day-care facilities, non-essential businesses, and private and public recreation facilities, physical distancing for individuals, forgoing international travel, self-quarantine in case of symptoms | Physical activity, sedentary behaviour: Parents-reported questions about change |
| Medrano et al., 2020 [87], Low risk | Spain, Cohort study | T1: September–December 2019 T2: March–April 2020 | Children (8–16 years) Sample size at follow-up: n = 113 Age (mean (SD)): 12.1 years (2.4) Response: 83.6% Lost to follow-up: 61.2 | Home confinement during the COVID-19 pandemic - measures: closure of schools, mandatory home confinement for children, total lockdown (children were not allowed to leave their house at all) from 14 March–26 April 2020 | Physical activity, screen time: “The Youth Activity Profile” questionnaire Adherence to Mediterranean diet: Mediterranean Diet Quality Index for children and teenagers (KIDMED) questionnaire |
| Niedzwiedz et al., 2020 [32], Low risk (outcome: “alcohol consumption”), High risk (outcome: “smoking”) | United Kingdom, Cohort study | 2015–2020 T1: 2015–2017 T2: 2016–2018 T3: 2017–2019 T4: 24–30 April 2020 | Adults (≥18 years) Sample size at follow-up: n = 9748 (52.2% female) Age: n.r. Response T4: 48.6% Lost to follow-up T1–T4: 59.6% | COVID-19 lockdown - measures: 12 March 2020: isolation of all with all with symptoms of possible COVID-19 for 7days, 16 March 2020: isolation of all living with someone with symptoms of possible COVID19 for 14 days, advise against unnecessary social contact and travel, banning of mass gatherings, 17 March 2020: advise against all nonessential world-wide travel, 20 March 2020: closure of entertainment, hospitality and indoor leisure premises, schools, colleges and nurseries close for all except children of key workers or children identified as vulnerable, 22 March 2020: advise for extremely clinically vulnerable persons to begin ‘shielding’, 23 March 2020: no permission for the whole population to leave home except for very limited purposes (to buy food; to exercise once per day; for any medical need; to care for a vulnerable person; to travel to/from essential work), banning of all gatherings of more than two people in public, 27 March 2020: public advise to only use open spaces near own house for exercise, and to stay at least 2 m apart from other households while outdoors | Alcohol consumption: Alcohol Use Disorder Identification Test for Consumption: Cigarette smoking: 2 self-reported single questions E-Cigarette use: 1 self-reported question |
| Okely et al., 2020 [33], High risk | Scotland, Cohort study | T1: 2017–2019 T2: 27 May–8 June 2020 | Older adults (born in 1936) Sample size at follow-up: n = 137 (48.2% female) Age (mean): 84 years Response: 30.2% Lost to follow-up: n.r. | COVID-19 lockdown (that lasted 34 days at the beginning of data collection): - measures: n.r. | Physical activity: 1 self-reported question |
| Özden and Kilic, 2021 [88], High risk | Turkey, Cross-sectional study | 15–29 May 2020 | Nursing students Sample size: n = 1011 (60% female) Age (mean (SD)): 19.97 years (3.11) Response: 72.2% | Closure of schools and universities - measures: closure of all schools and universities (16 March 2020), continuation of university education with distance learning possibilities | Weight, exercise: 1 self-reported question about change |
| Ozturk Eyimaya and Yalçin Irmak, 2020 [89], High risk | Turkey, Cross-sectional study | 15–31 May 2020 | Children (6–13 years) Sample size: n = 1115 (53.4% female) Age (mean (SD)): 9.03 years (1.95) Response: 72.2% (parents) | Lockdown - measures: closure of schools (16 March 2020), temporary lockdown on children and young people (<20 years) (3 April 2020) | Screen time: 1 self-reported question about change |
| Radwan et al., 2021 [90], High risk | United Arab Emirates, Cross-sectional study | 5–18 May 2020 | Adults Sample size: n = 2060 (75.1% female) Age: n.r. Response: 15.8% | COVID-19 lockdown (from 22 March 2020 onwards) - measures: n.r. | Dietary intake, weight, physical activity, smoking: 1 self-reported question about change |
| Sasaki et al., 2021 [91], High risk | Japan, Cross-sectional study | August 2020 | Older adults (60–95 years) Sample size: n = 999 (53.8% female) Age (mean (SD)): 74.5 years (6.3) Response: 74.3% | COVID-19-related distancing restrictions - measures: n.r. | Physical activity: International Physical Activity Questionnaire Short Form Sitting: International Physical Activity Questionnaire Short Form |
| Savage et al., 2020 [92], High risk | United Kingdom, Cohort study | T1: 14 October 2019 T2: 28 January 2020 T3: 20 March 2020 T4: 27 April 2020 | University students Sample size at follow-up: n = 214 (72.0% female) Age (mean: 28.0 years Response: 15.6 % Lost to follow-up: 85.5 % | Lockdown: - measures: requirement to stay at home as much as possible, allowance only to leave home once per day for exercise | Physical activity: Exercise Vital Sign (EVS) questionnaire Sedentary behaviour: 1 self-reported question |
| Schmidt et al., 2020 [93], High risk | Germany, Cohort study | T1: August 2018 T2: 20 April–1 May 2020 | Children and adolescents Sample size at follow-up: n = 1711 (49.8% female) Age (mean (SD)): 10.36 years (4.04) Response: 25.2% Lost to follow-up: 36.4% | COVID-19 lockdown - measures: closure of kindergartens, schools, sports clubs, gyms, and other leisure institutions relevant to children’s and adolescents organized physical activity (11 March 2020), physical distancing measures and contact restrictions (no more than 2 people from different households to meet in public space), nonorganized sports activities, such as workouts at home, or jogging, and other forms of habitual physical activity besides sports, like going for a walk or playing outside remained allowed if done alone or with people from the same household | Physical activity: MoMo PA Questionnaire Screen time: Self-reported questions |
| To et al., 2021 [94], High risk | Australia, (Prospective) secondary data analyses | 1 January 2018–30 June 2020 (continuous data collection) | Adults (who are registered as members of the 10,000 Steps program) Sample size: n = 60,560 (67.0% female) Age: n.r. % active users (of those registered with the app) providing data: 13.1% | Lockdown (2 March 2020) - measures: social distancing guidelines, closure of nonessential businesses, such as gyms, indoor sports facilities, and clubs, allowance to be outside only for exercise or other essential needs, offering of takeaway and delivery services for restaurants and cafes (Relaxation of restrictions: 8 May 2020) | Physical activity: number of steps logged per day (via app) |
| Tornaghi et al., 2020 [95], High risk | Italy, Cohort study | T1: 27–30 January 2020 T2: 4–10 April 2020 T3: 4–10 May 2020 | Adolescents (15–18 years) Sample size at follow-up: n = 1568 (% female: n.r.) Age: n.r. Response: 93% Lost to follow-up: 0% | COVID-19 lockdown (11 and 22 March 2020) - measures: abrogation of nonessential movement, including outdoor sports and motor activity, with the exception of activities practiced in a 200 m home-block area and provision of at least 1 m of interhuman distance | Physical activity: International Physical Activity Questionnaire |
| Wang et al., 2020 [96], High risk | China, Cohort study | T0: 2019 T1: 30 days prior to 21 January 2020 T2: 30 days after 21 January 2020 | Middle-aged and older adults Sample size at follow-up: n = 3544 (34.6% female) Age (mean (SD)): 51.6 years (8.9) Response: 57.1% Lost to follow-up: 15.0% | Physical distancing measures - measures: n.r. | Walking activity: daily steps collected via a smartphone linked to WeChat |
| White et al., 2021 [97], High risk | United States, Cross-sectional study | n.r. | College students (who reported drinking alcohol pre- and post-campus closure) Sample size at follow-up: n = 297 (62% female) Age (mean (SD)): 21.1 years (0.82) Response: 66% | Campus closure because of COVID-19 - measures: n.r. | Drinking: Daily Drinking Questionnaire |
| Wickersham et al., 2021 [98], High risk | United Kingdom, (Prospective) secondary data analyses | T1: 23 March 2020 T2: 23 March–10 May 2020 T3: 11 May–14 June 2020 (continuous data collection) | Students (who had enrolled in the remote measurement technology King’s Move Physical Activity tracker app) Sample size: n = 763 Age (median (IQR): 22 years (20–25) % active users (of those registered with the app) providing data: 73.5% (but only 2.2% off all students) | COVID-19 lockdown (23 March 2020) - measures: closure of services, including fitness centres, hospitality, leisure, and educational institutions, allowance only go outside for one form of exercise per day or to make essential shopping trips, closure of all university campuses (easing of restrictions: 11 May 2020) | Physical activity: app data (measuring steps walked and miles run per week) |
| Yamada et al., 2020 [99], High risk | Japan, Cohort study | 1 January–25 May 2020(continuous data collection) | Physically independent residents, living in a continuing care retirement community Sample size at follow-up: n = 114 Age (range): 67–92 years Response: 38.5% Lost to follow-up: 0% | Social/physical distancing and self-isolation - measures: announcement of the continuing care retirement community of a cancellation of all upcoming in-facility events/exhibitions and the closure of some common facilities as a precaution measure (24 February 2020), state of emergency asking people to stay at home (7 April 2020) | Walking: walking distance within the continuing care retirement community based on behaviour logs from a beacon transmitter |
| Reference | Major Domains | Minor Domains | Overall Risk | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Recruitment Procedure and Follow-Up (in Cohort Studies) | 2. Exposure Definition and Measurement | 3. Outcome Source and Validation | 4. Confounding and Effect Modification | 5. Analysis Method | 6. Chronology | 7. Blinding of Assessors | 8. Funding | 9. Conflict of Interest | ||
| Alpers et al., 2021 [69] (for investigation of association between self-reported quarantine status and alcohol consumption) |  |  | | | | | | | | |
| Alpers et al., 2021 [69] (outcome: change in alcohol consumption) | | | | | | | | | | |
| Anyan et al., 2020 [70], Ernsten and Havnen 2020 [71] | | | | | | | | | | |
| Avery et al., 2020 [72] | | | | | | | | | | |
| Barkley et al., 2020 [74] (outcomes: physical activity, sedentary behaviour) | | | | | | | | | | |
| Barkley et al., 2020 [74] (outcome: weight) | | | | | | | | | | |
| Berard et al., 2021 [75] (outcome: dietary quality) | | | | | | | | | | |
| Berard et al., 2021 [75] (outcomes: physical activity, weight, and smoking) | | | | | | | | | | |
| Bourion-Bedes et al., 2021 [76] | | | | | | | | | | |
| Cicero et al., 2021 [77] (outcome: dietary quality) | | | | | | | | | | |
| Cicero et al., 2021 [77] (outcomes: BMI, smoking) | | | | | | | | | | |
| Colley et al., 2020 [78] | | | | | | | |  | | |
| Crochemore-Silva et al., 2020 [79] | | | | | | | | | | |
| Daly and Robinson, 2021 [80] a | | | | | | | | | | |
| Di Sebastiano et al., 2020 [81] | | | | | | | | | | |
| Duncan et al., 2020 [73] | | | | | | | | | | |
| Garre-Olmo et al., 2020 [82] | | | | | | | | | | |
| Karuc et al., 2020 [83] (for investigation of association between quarantine status and physical activity) | | | | | | | | | | |
| Karuc et al., 2020 [83] (outcome: change in physical activity) | | | | | | | | | | |
| Lechner et al., 2020 [84] | | | | | | | | | | |
| Mason et al., 2020 [85] | | | | | | | | | | |
| McCormack et al., 2020 [86] | | | | | | | | | | |
| Medrano et al., 2020 [87] | | | | | | | | | | |
| Niedzwiedz et al., 2020 [32] (Outcome: alcohol consumption) | | | | | | | | | | |
| Niedzwiedz et al., 2020 [32] (Outcome: smoking) | | | | | | | | | | |
| Okely et al., 2020 [33] | | | | | | | | | | |
| Özden and Kilic, 2021 [88] | | | | | | | | | | |
| Ozturk Eyimaya and Yalçin Irmak, 2020 [89] | | | | | | | | | | |
| Radwan et al., 2021 [90] | | | | | | | | | | |
| Sasaki et al., 2021 [91] | | | | | | | | | | |
| Savage et al., 2020 [92] (outcome: physical activity) | | | | | | | | | | |
| Savage et al., 2020 [92] (outcome: sedentary behaviour) | | | | | | | | | | |
| Schmidt et al., 2020 [93] | | | | | | | | | | |
| To et al., 2021 [94] | | | | | | | | | | |
| Tornaghi et al., 2020 [95] | | | | | | | | | | |
| Wang et al., 2020 [96] | | | | | | | | | | |
| White et al., 2021 [97] | | | | | | | | | | |
| Wickersham et al., 2021 [98] | | | | | | | | | | |
| Yamada et al., 2020 [99] | | | | | | | | | | |
Low risk, High risk, Unclear risk.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freiberg, A.; Schubert, M.; Romero Starke, K.; Hegewald, J.; Seidler, A. A Rapid Review on the Influence of COVID-19 Lockdown and Quarantine Measures on Modifiable Cardiovascular Risk Factors in the General Population. Int. J. Environ. Res. Public Health 2021, 18, 8567. https://doi.org/10.3390/ijerph18168567
Freiberg A, Schubert M, Romero Starke K, Hegewald J, Seidler A. A Rapid Review on the Influence of COVID-19 Lockdown and Quarantine Measures on Modifiable Cardiovascular Risk Factors in the General Population. International Journal of Environmental Research and Public Health. 2021; 18(16):8567. https://doi.org/10.3390/ijerph18168567
Chicago/Turabian StyleFreiberg, Alice, Melanie Schubert, Karla Romero Starke, Janice Hegewald, and Andreas Seidler. 2021. "A Rapid Review on the Influence of COVID-19 Lockdown and Quarantine Measures on Modifiable Cardiovascular Risk Factors in the General Population" International Journal of Environmental Research and Public Health 18, no. 16: 8567. https://doi.org/10.3390/ijerph18168567