Risk of Adverse Drug Events Following the Virtual Addition of COVID-19 Repurposed Drugs to Drug Regimens of Frail Older Adults with Polypharmacy

 ,
,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Subjects and Study Design
2.2. Medication Risk Score and Simulation Strategy
2.3. Data Processing and Statistical Analysis
3. Results
3.1. Participant Characteristics
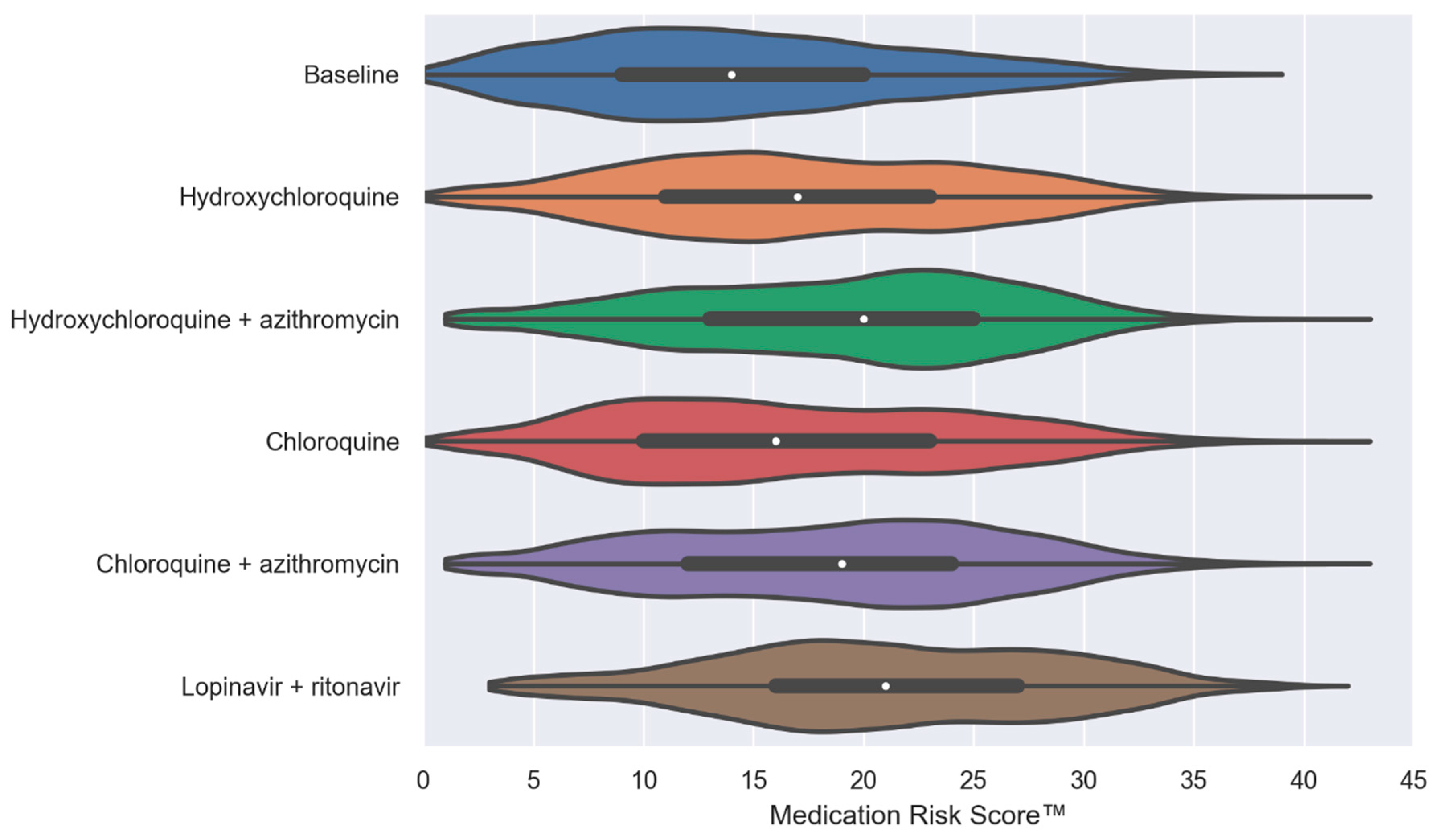
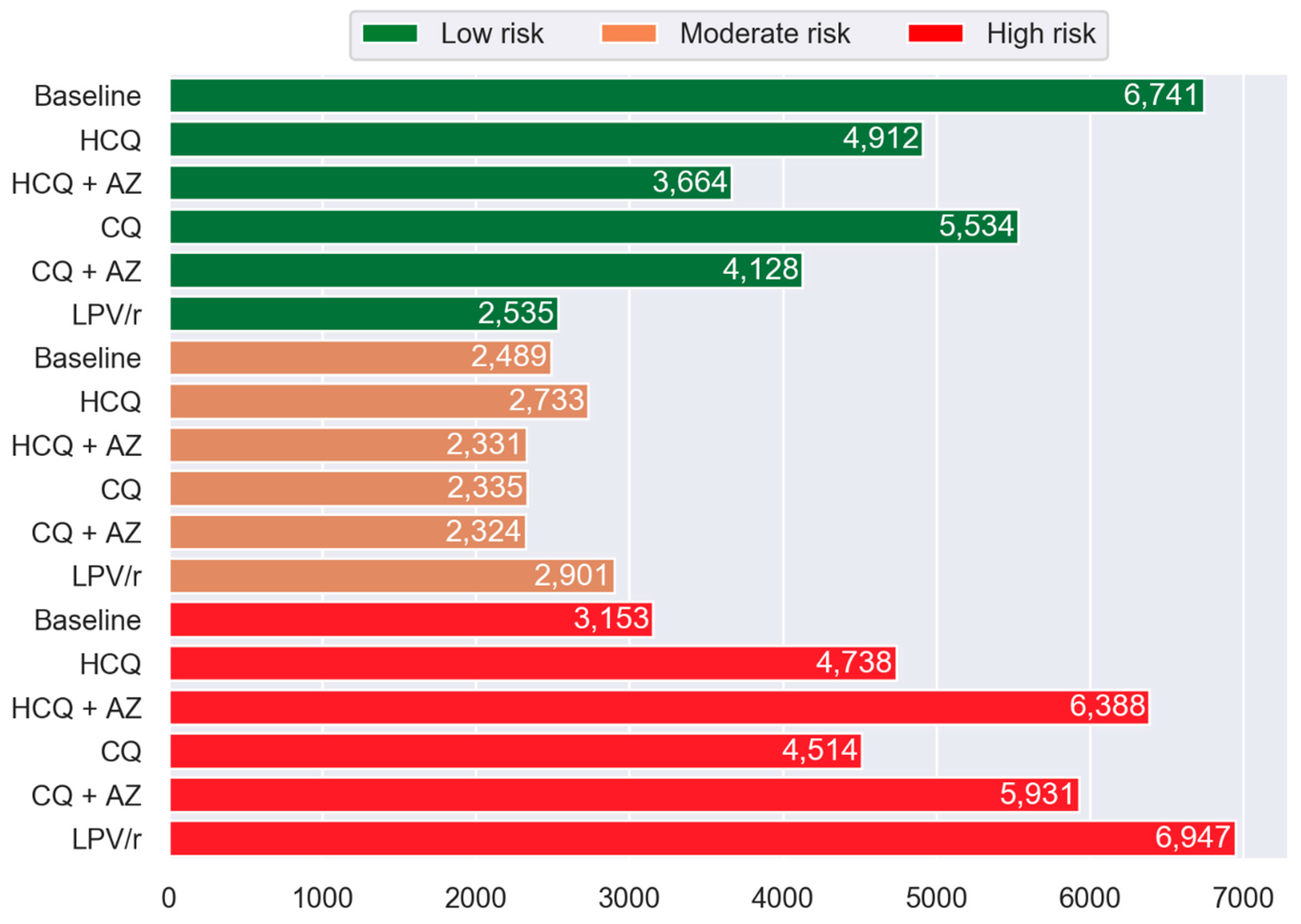
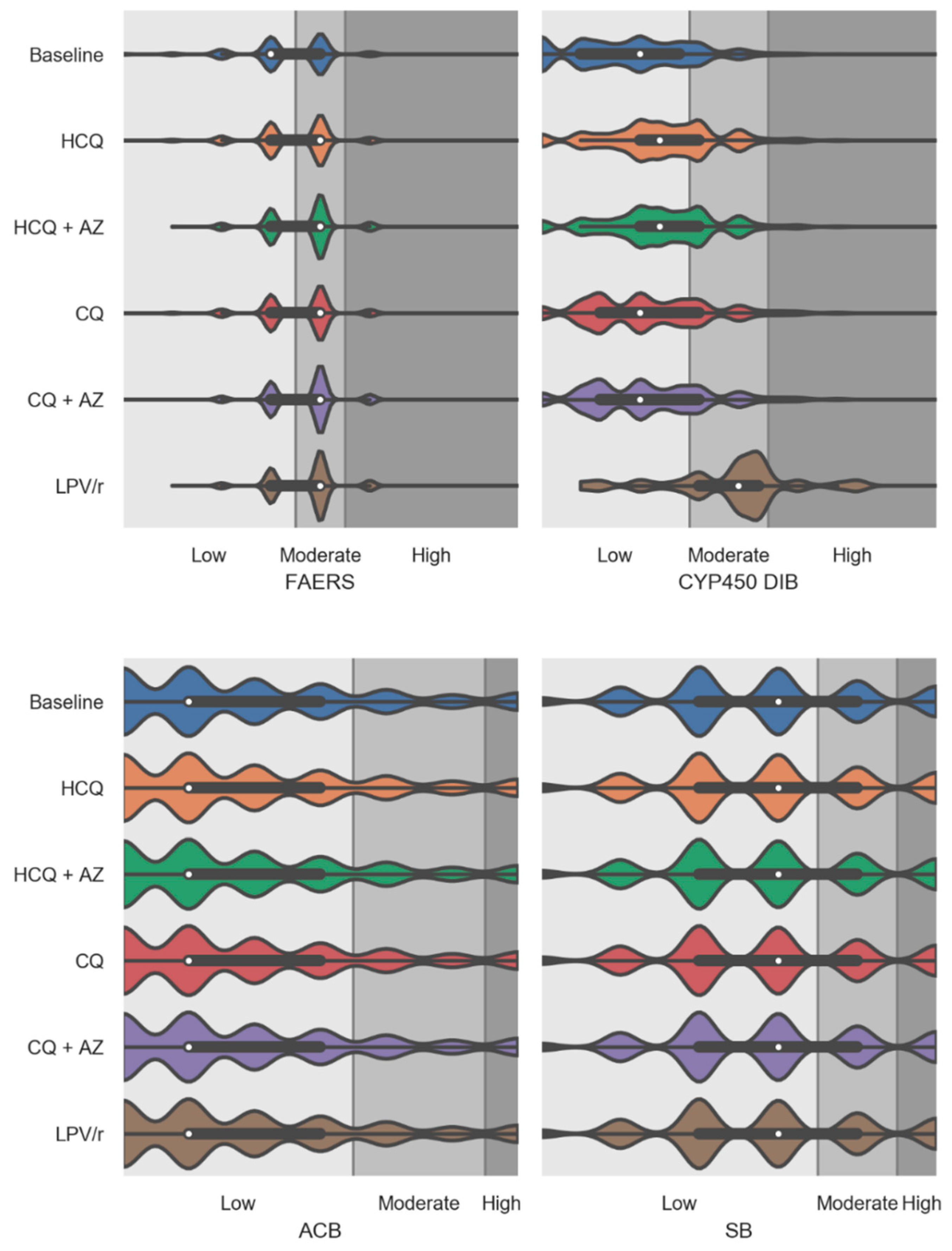
3.2. Simulated Effects of Repurposed Drugs for COVID-19 on MRS™
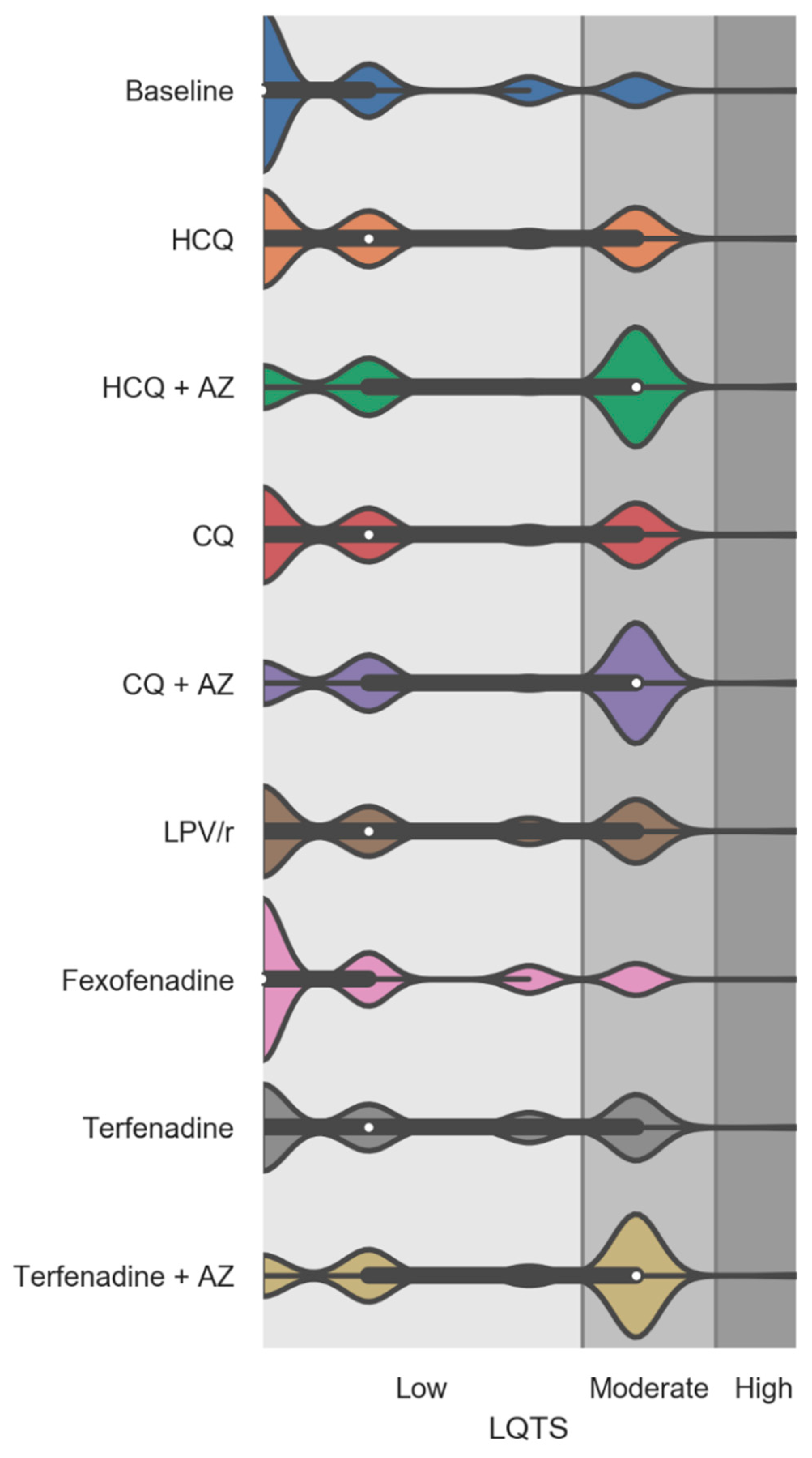
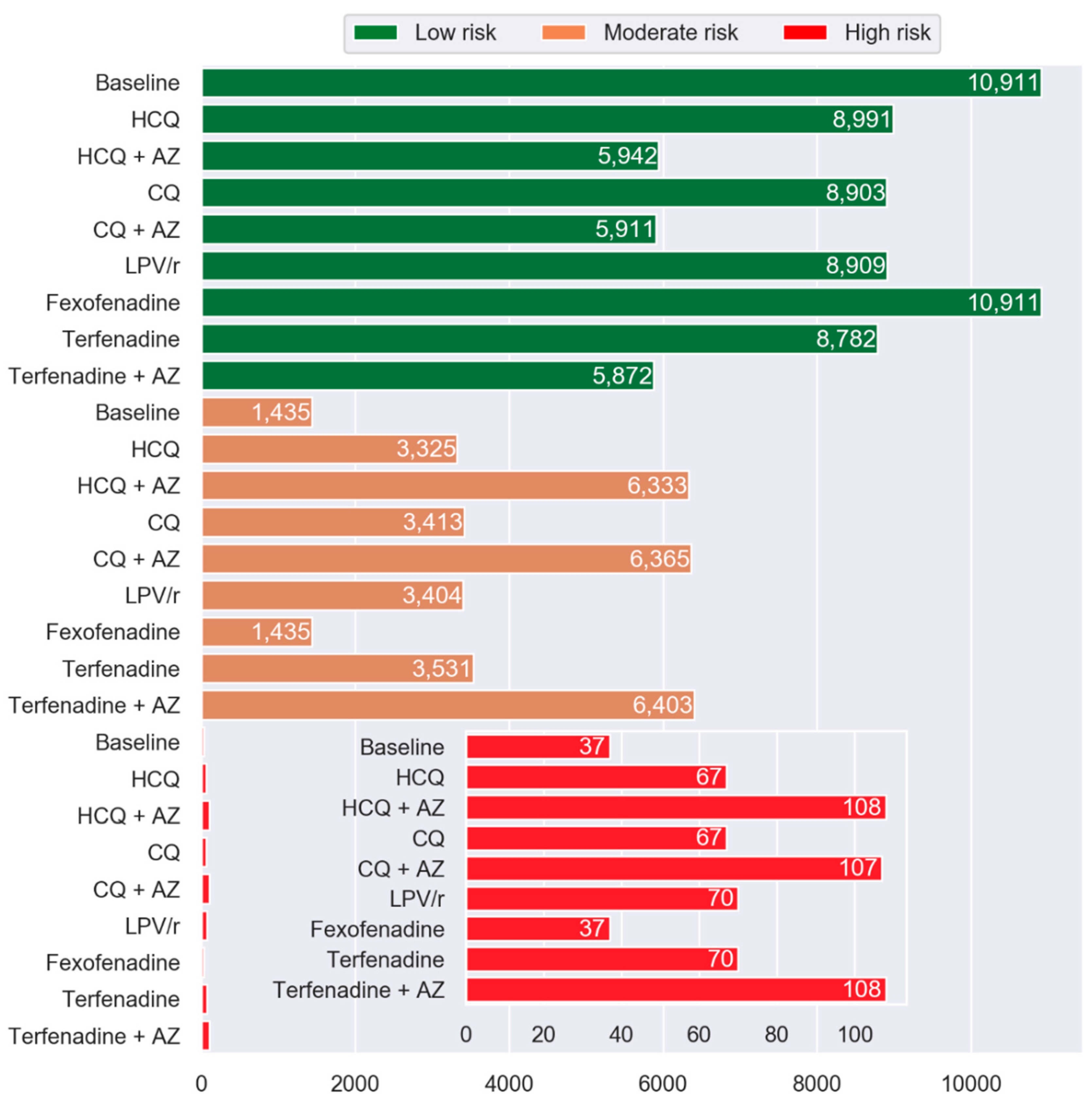
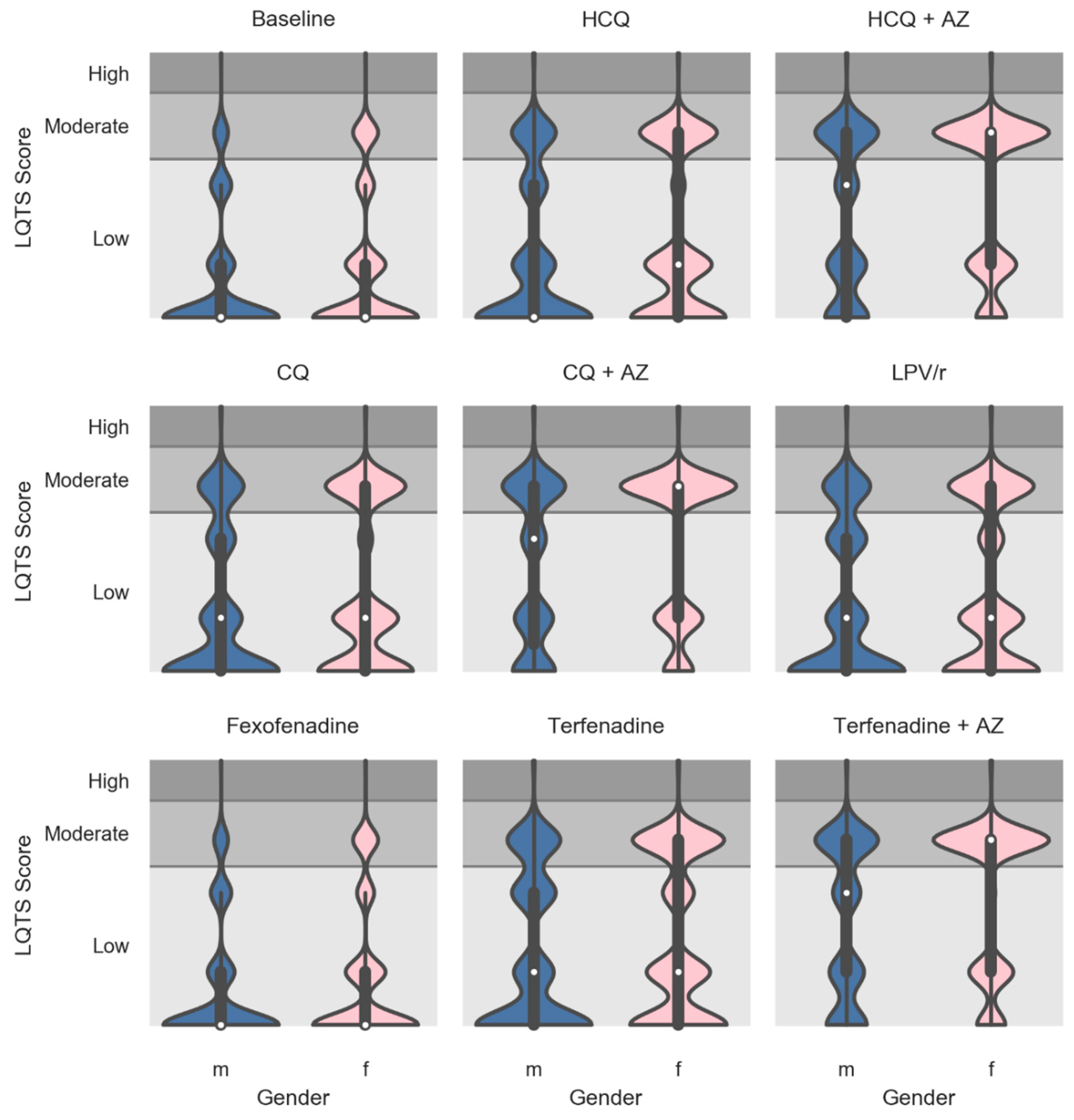
3.3. Simulated Effects of Repurposed Drugs for COVID-19 on the LQTS Risk Score
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Center for Disease Prevention and Control. Cluster of Pneumonia Cases Caused by a Novel Coronavirus, Wuhan, China. Rapid Risk Assessment. Available online: http://wjw.wuhan.gov.cn/front/web/showDetail/2019123108989 (accessed on 22 July 2020).
- World Health Organization. Pnemonia of an Unknown Cause. Emergencies Preparedness, Response. Available online: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/ (accessed on 5 June 2020).
- Johns Hopkins University and Medicine. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University and Medicine. Available online: https://coronavirus.jhu.edu/map.html (accessed on 5 August 2020).
- U.S. Food and Drug Administration. Emergency Use Authorization (EUA) for Emergency Use of Remdesivir for the Treatment of Hospitalized 2019 Coronavirus Disease (COVID-19) Patients. Available online: https://www.fda.gov/media/137564/download (accessed on 22 July 2020).
- U.S. Food and Drug Administration. Request for Emergency Use Authorization For Use of Chloroquine Phosphate or Hydroxychloroquine Sulfate Supplied from the Strategic National Stockpile for Treatment of 2019 Coronavirus Disease. Revoked. Available online: https://www.fda.gov/media/136534/download (accessed on 23 July 2020).
- Al Rihani, S.B.; Deodhar, M.; Michaud, V.; Turgeon, J.; Lucio, E.; Condon, G.; Dow, P. Potential COVID-19 Treatment Options (Off-Label). Available online: https://trhc.spprdi.com/covid19/home (accessed on 7 July 2020).
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.-X.; et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 27 July 2020).
- U.S. Food and Drug Administration. FDA cautions against use of hydroxychloroquine or chloroquine for COVID-19 outside of the hospital setting or a clinical trial due to risk of heart rhythm problems. In Does not Affect FDA-Approved Uses for Malaria, Lupus, and Rheumatoid Arthritis; U.S. Food and Drug Administration: Washington, DC, USA, 2020. [Google Scholar]
- Milberg, P.; Eckardt, L.; Bruns, H.J.; Biertz, J.; Ramtin, S.; Reinsch, N.; Fleischer, D.; Kirchhof, P.; Fabritz, L.; Breithardt, G.; et al. Divergent proarrhythmic potential of macrolide antibiotics despite similar QT prolongation: Fast phase 3 repolarization prevents early afterdepolarizations and torsade de pointes. J. Pharmacol. Exp. Ther. 2002, 303, 218–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, B.H.; Chi-hua, W.; Hsia, C.-P.; Yin Chen, C. Azithromycin-induced torsade de pointes. Pacing Clin. Electrophysiol. 2007, 30, 1579–1582. [Google Scholar] [CrossRef] [PubMed]
- Kezerashvili, A.; Khattak, H.; Barsky, A.; Nazari, R.; Fisher, J.D. Azithromycin as a cause of QT-interval prolongation and torsade de pointes in the absence of other known precipitating factors. J. Interv. Card. Electrophysiol. 2007, 18, 243–246. [Google Scholar] [CrossRef]
- Demazière, J.; Fourcade, J.M.; Busseuil, C.T.; Adeleine, P.; Meyer, S.M.; Saïssy, J.M. The hazards of chloroquine self prescription in west Africa. J. Toxicol. Clin. Toxicol. 1995, 33, 369–370. [Google Scholar] [CrossRef]
- Chen, C.Y.; Wang, F.L.; Lin, C.C. Chronic hydroxychloroquine use associated with QT prolongation and refractory ventricular arrhythmia. Clin. Toxicol. 2006, 44, 173–175. [Google Scholar] [CrossRef]
- Morgan, N.D.; Patel, S.V.; Dvorkina, O. Suspected hydroxychloroquine-associated QT-interval prolongation in a patient with systemic lupus erythematosus. J. Clin. Rheumatol. 2013, 19, 286–288. [Google Scholar] [CrossRef]
- O’Laughlin, J.P.; Mehta, P.H.; Wong, B.C. Life threatening severe QTc prolongation in patient with systemic lupus erythematosus due to hydroxychloroquine. Case Rep. Cardiol. 2016, 4626279. [Google Scholar] [CrossRef] [Green Version]
- Geleris, J.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.K.; Kubin, C.; Barr, R.G.; et al. Observational study of hydroxychloroquine in hospitalized patients with Covid-19. N. Engl. J. Med. 2020, 382, 2411–2418. [Google Scholar] [CrossRef]
- Simpson, T.F.; Kovacs, R.; Stecker, E.C. Ventricular arrhythmia risk due to hydroxychloroquine-azithromycin treatment for COVID-19. Available online: https://www.acc.org/latest-in-cardiology/articles/2020/03/27/14/00/ventricular-arrhythmia-risk-due-to-hydroxychloroquine-azithromycin-treatment-for-covid-19 (accessed on 5 June 2020).
- Chorin, E.; Dai, M.; Shulman, E.; Wadhwani, L.; Bar-Cohen, R.; Barbhaiya, C.; Aizer, A.; Holmes, D.; Bernstein, S.; Spinelli, M.; et al. The QT interval in patients with COVID-19 treated with hydroxychloroquine and azithromycin. Nat. Med. 2020, 26, 808–809. [Google Scholar] [CrossRef]
- Chorin, E.; Wadhwani, L.; Magnani, S.; Dai, M.; Shulman, E.; Nadeau-Routhier, C.; Knotts, R.; Bar-Cohen, R.; Kogan, E.; Barbhaiya, C.; et al. QT Interval Prolongation and Torsade de Pointes in Patients with COVID-19 Treated with Hydroxychloroquine/Azithromycin. Heart Rhythm 2020. [Google Scholar] [CrossRef] [PubMed]
- Bankes, D.L.; Jin, H.; Finnel, S.; Michaud, V.; Knowlton, C.H.; Turgeon, J.; Stein, A. Association of a novel medication risk score with adverse drug events and other pertinent outcomes among participants of the programs of all-inclusive care for the elderly. Pharmacy 2020, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Turgeon, J.; Michaud, V.; Cicali, B. Population-Based Medication Risk Stratification and Personalized Medication Risk Score. U.S. Patent WO2019089725, 5 September 2019. [Google Scholar]
- Cicali, B.; Michaud, V.; Knowlton, C.H.; Turgeon, J. Application of a novel medication-related risk stratification strategy to a self-funded employer population. Benefits Q. 2018, 34, 49–55. [Google Scholar]
- Harpaz, R.; Haerian, K.; Chase, H.S.; Friedman, C. Statistical mining of potential drug interaction adverse effects in FDA’s spontaneous reporting system. Amia Annu. Symp. Proc. 2010, 2010, 281–285. [Google Scholar] [PubMed]
- Boustani, M.; Campbell, N.; Munger, S.; Maidment, I.; Fox, C. Impact of anticholinergics on the aging brain: A review and practical application. Aging Health 2008, 4, 311–320. [Google Scholar] [CrossRef]
- Taipale, H.T.; Bell, J.S.; Uusi-Kokko, M.; Lönnroos, E.; Sulkava, R.; Hartikainen, S. Sedative load among community-dwelling people aged 75 years and older: A population-based study. Drugs Aging 2011, 28, 913–925. [Google Scholar] [CrossRef]
- Linjakumpu, T.; Hartikainen, S.; Klaukka, T.; Koponen, H.; Kivelä, S.L.; Isoaho, R. A model to classify the sedative load of drugs. Int. J. Geriatr. Psychiatry. 2003, 18, 542–544. [Google Scholar] [CrossRef]
- Taipale, H.T.; Hartikainen, S.; Bell, J.S. A comparison of four methods to quantify the cumulative effect of taking multiple drugs with sedative properties. Am. J. Geriatr. Pharm. 2010, 8, 460–471. [Google Scholar] [CrossRef]
- Michaud, V.; Dow, P.; Al Rihani, S.B.; Deodhar, M.; Arwood, M.; Cicali, B.; Turgeon, J. Risk of drug-induced Long QT Syndrome associated with the use of repurposed COVID-19 drugs: A systematic review. medRxiv 2020. [published online ahead of print, 24 April 2020]. [Google Scholar] [CrossRef] [Green Version]
- Turgeon, J.; Michaud, V.; Steffen, L.E.; Badea, G. Treatment Methods Having Reduced Drug-Related Toxicity and Methods of Identifying the Likelihood of Patient Harm from Prescribed Medications. U.S. Patent WO2017213825, 14 December 2017. [Google Scholar]
- Doan, J.; Zakrzewski-Jakubiak, H.; Roy, J.; Turgeon, J.; Tannenbaum, C. Prevalence and risk of potential cytochrome P450-mediated drug-drug interactions in older hospitalized patients with polypharmacy. Ann. Pharm. 2013, 47, 324–332. [Google Scholar] [CrossRef]
- MedicareBlueRx PDP. Enhanced Medication Therapy Management (EMTM) Pilot. Available online: https://www.yourmedicaresolutions.com/members/emtm-providers#:~:text=Enhanced%20Medication%20Therapy%20Management%20 (accessed on 7 July 2020).
- Centers for Medicare and Medicaid Services. Program of All-Inclusive Care for the Elderly. Long Term Services & Supports. Available online: https://www.medicaid.gov/medicaid/long-term-services-supports/program-all-inclusive-care-elderly/index.html (accessed on 22 July 2020).
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.a.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankelson, L.; Karam, G.; Becker, M.L.; Chinitz, L.A.; Tsai, M.-C. QT prolongation, torsades de pointes and sudden death with short courses of chloroquine or hydroxychloroquine as used in COVID-19: A systematic review. Heart Rhythm 2020, 1–8. [Google Scholar] [CrossRef]
- Szekely, Y.; Lichter, Y.; Shrkihe, B.A.; Bruck, H.; Oster, H.S.; Viskin, S. Chloroquine-induced torsades de pointes in a patient with coronavirus disease 2019. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7198423/pdf/main.pdf (accessed on 6 August 2020).
- Woosley, R.L.; Chen, Y.; Freiman, J.P.; Gillis, R.A. Mechanism of the cardiotoxic actions of terfenadine. JAMA 1993, 269, 1532–1536. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.A.; Park, J.Y.; Lee, J.S.; Lim, S. Cytochrome P450 2C8 and CYP3A4/5 are involved in chloroquine metabolism in human liver microsomes. Arch. Pharm. Res. 2003, 26, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Vinayagamoorthy, N.; Han, K.; Kwok, S.K.; Ju, J.H.; Park, K.S.; Jung, S.H.; Park, S.W.; Chung, Y.J.; Park, S.H. Association of polymorphisms of cytochrome P450 2D6 with blood hydroxychloroquine levels in patients with systemic lupus erythematosus. Arthritis Rheumatol. 2016, 68, 184–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Projean, D.; Baune, B.; Farinotti, R.; Flinois, J.-P.; Beaune, P.; Taburet, A.-M.; Ducharme, J. In Vitro Metabolism of Chloroquine: Identification of CYP2C8, CYP3A4, and CYP2D6 as the Main Isoforms Catalyzing N-Desethylcholoroquine Formation. Drug Metab. Dispos. 2003, 31, 748–754. [Google Scholar] [CrossRef] [Green Version]
- Yeh, R.F.; Gaver, V.E.; Patterson, K.B.; Rezk, N.L.; Baxter-Meheux, F.; Blake, M.J.; Eron, J.J., Jr.; Klein, C.E.; Rublein, J.C.; Kashuba, A.D. Lopinavir/ritonavir induces the hepatic activity of cytochrome P450 enzymes CYP2C9, CYP2C19, and CYP1A2 but inhibits the hepatic and intestinal activity of CYP3A as measured by a phenotyping drug cocktail in healthy volunteers. J. Acquir. Immune Defic. Syndr. 2006, 42, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Kumar, G.N.; Dykstra, J.; Roberts, E.M.; Jayanti, V.K.; Hickman, D.; Uchic, J.; Yao, Y.; Surber, B.; Thomas, S.; Granneman, G.R. Potent inhibition of the cytochrome P-450 3A-mediated human liver microsomal metabolism of a novel HIV protease inhibitor by ritonavir: A positive drug-drug interaction. Drug Metab. Dispos. 1999, 27, 902–908. [Google Scholar]
- U.S. Food and Drug Administration. NOVIR (Ritonavir) [Drug Label]. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/020659s034,020945s017lbl.pdf (accessed on 5 June 2020).
- Food and Drug Administration, HSS. International Conference on Harmonisation; guidance on S7B Nonclinical Evaluation of the Potential for Delayed Ventricular Repolarization (QT Interval Prolongation) by Human Pharmaceuticals; availability. Notice. Fed. Regist. 2005, 70, 61133–61134. [Google Scholar]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19). Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar]
- Oakes, B.; Thompson, K.; Inouye, S. Ageism Leaves Older Patients Out Of Important Clinical Trials For COVID-19, Says Harvard Researcher. WBUR Morning Edition. Available online: https://www.wbur.org/commonhealth/2020/06/25/covid-19-coronavirus-ageism (accessed on 17 July 2020).
- Skipper, C.P.; Pastick, K.A.; Engen, N.W.; Bangdiwala, A.S.; Abassi, M.; Lofgren, S.M.; Williams, D.A.; Okafor, E.C.; Pullen, M.F.; Nicol, M.R.; et al. Hydroxychloroquine in Nonhospitalized Adults With Early COVID-19. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7384270/pdf/aim-olf-M204207.pdf (accessed on 6 August 2020).
- Ross, S.B.; Wilson, M.G.; Papillon-Ferland, L.; Elsayed, S.; Wu, P.E.; Battu, K.; Porter, S.; Rashidi, B.; Tamblyn, R.; Pilote, L.; et al. COVID-SAFER: Deprescribing guidance for hydroxychloroquine drug interactions in older adults. J. Am. Geriatr. Soc. 2020. [published online ahead of print, 22 May, 2020]. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.A.; Murray, K.T.; Hall, K.; Arbogast, P.G.; Stein, C.M. Azithromycin and the Risk of Cardiovascular Death. N. Engl. J. Med. 2012, 366, 1881–1890. [Google Scholar] [CrossRef]
- World Health Organization. The cardiotoxicity of antimalarials. In Proceedings of the Malaria Policy Advisory Committee Meeting, Geneva, Switzerlan, 22–24 March 2017. [Google Scholar]
- Simkó, J.; Csilek, A.; Karászi, J.; Lorincz, I. Proarrhythmic potential of antimicrobial agents. Infection 2008, 36, 194–206. [Google Scholar] [CrossRef]
- Stas, P.; Faes, D.; Noyens, P. Conduction disorder and QT prolongation secondary to long-term treatment with chloroquine. Int. J. Cardiol. 2008, 127, e80–e82. [Google Scholar] [CrossRef]
- De Olano, J.; Howland, M.A.; Su, M.K.; Hoffman, R.S.; Biary, R. Toxicokinetics of hydroxychloroquine following a massive overdose. Am. J. Emerg. Med. 2019, 37, e2264–e2265. [Google Scholar] [CrossRef]
- Bessière, F.; Roccia, H.; Delinière, A.; Charrière, R.; Chevalier, P.; Argaud, L.; Cour, M. Assessment of QT intervals in a case series of patients with coronavirus disease 2019 (COVID-19) infection treated with hydroxychloroquine alone or in combination with azithromycin in an intensive care unit. JAMA Cardiol. 2020, e201787, [published online ahead of print, 1 May, 2020]. [Google Scholar] [CrossRef]
- Mercuro, N.J.; Yen, C.F.; Shim, D.J.; Maher, T.R.; McCoy, C.M.; Zimetbaum, P.J.; Gold, H.S. Risk of QT Interval prolongation associated with use of hydroxychloroquine with or without concomitant azithromycin among hospitalized patients testing positive for coronavirus disease 2019 (COVID-19). JAMA Cardiol 2020, e201834, [published online ahead of print,1 May 2020]. [Google Scholar] [CrossRef]
- Gautret, P.; Lagiera, J.C.; Parolaa, P.; Thuan Hoanga, V.; Meddeba, L.; Mailhea, M.; Doudiera, B.; Courjone, J.; Giordanengoh, V.; Esteves Vieiraa, V.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an openlabel non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Bauman, J.L.; Tisdale, J.E. Chloroquine and hydroxychloroquine in the era of SARS—CoV2: Caution on their cardiac toxicity. Pharmacotherapy 2020, 40, 387–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. “Solidarity” Clinical Trial for COVID-19 Treatments. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-clinical-trial-for-covid-19-treatments (accessed on 22 July 2020).
- Department of Health and Human Services; Hoechst Marion Roussel, Inc.; Baker Norton Pharmaceuticals, Inc.; Terfenadine. Proposal to Withdraw Approval of Two New Drug Applications and One Abbreviated New Drug Application; Opportunity for a Hearing. Fed. Regist. 1997, 62, 1889–1892. [Google Scholar]
- Makkar, R.R.; Fromm, B.S.; Steinman, R.T.; Meissner, M.D.; Lehmann, M.H. Female gender as a risk factor for torsades de pointes associated with cardiovascular drugs. JAMA 1993, 270, 2590–2597. [Google Scholar] [CrossRef] [PubMed]
- Drici, M.D.; Knollmann, B.C.; Wang, W.X.; Woosley, R.L. Cardiac actions of erythromycin: Influence of female sex. JAMA 1998, 280, 1774–1776. [Google Scholar] [CrossRef] [Green Version]
- Gowda, R.M.; Khan, I.A.; Punukollu, G.; Vasavada, B.C.; Sacchi, T.J.; Wilbur, S.L. Female preponderance in ibutilide-induced torsade de pointes. Int. J. Cardiol. 2004, 95, 219–222. [Google Scholar] [CrossRef]
- Sarganas, G.; Garbe, E.; Klimpel, A.; Hering, R.C.; Bronder, E.; Haverkamp, W. Epidemiology of symptomatic drug-induced long QT syndrome and torsade de pointes in Germany. Europace 2014, 16, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Arunachalam, K.; Lakshmanan, S.; Maan, A.; Kumar, N.; Dominic, P. Impact of drug induced long QT syndrome: A systematic review. J. Clin. Med. Res. 2018, 10, 384–390. [Google Scholar] [CrossRef] [Green Version]
- U.S. National Library of Medicine. Clinical Trial Search COVID-19, SARS-CoV-2. 2020. Available online: https://clinicaltrials.gov/ct2/results?cond=COVID-19. (accessed on 20 July 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics at Baseline | |
|---|---|
| Total number of patients, n | 12,383 |
| Age (years); mean ± SD (range) | 76 ± 10 (55 to 89) |
| Sex; male, N (%) female, N (%) | 4039 (32.6%) 8344 (67.4%) |
| Number of drugs/day per patient; N ± SD (range) | 11.8 ± 5.7 (0–47) |
| Total MRSTM; mean ± SD (range) | 14.4 ± 7.7 (0–39) |
| 6741 (54.4%) 8.6 ± 3.7 |
| 2489 (20.1%) 16.9 ± 1.4 |
| 3153 (25.5%) 24.8 ± 3.7 |
Patients currently receiving prescribed drugs proposed for repurposing:
| 106 (0.9%) 0 125 (1.0%) 5 (0.04%) |
Potential CYP450 drug-drug interactions, patients currently receiving:
| 693 (5.6%) 137 (1.1%) 8952 (72%) 7439 (60%) 5861 (47%) 415 (3.4%) |
| Drug Names | Number of Patients, N (%) | Long QT-JT Index Category * | CredibleMeds Category ŧ |
|---|---|---|---|
| Furosemide | 2629 (21%) | Moderate | Conditional |
| Pantoprazole | 2402 (19%) | Moderate | Conditional |
| Sertraline | 1583 (12%) | Low | Conditional |
| Trazodone | 1479 (11%) | High | Conditional |
| Famotidine | 1422 (11%) | Moderate | Conditional |
| Omeprazole | 1395 (11%) | Moderate | Conditional |
| Hydrochlorothiazide | 1359 (10%) | Moderate | Conditional |
| Donepezil | 1073 (8%) | Moderate | Known |
| Mirtazapine | 1004 (8%) | Moderate | Possible |
| Quetiapine | 853 (6%) | High | Conditional |
| Escitalopram | 752 (6%) | High | Known |
| Citalopram | 681 (5%) | High | Known |
| Risperidone | 500 (4%) | High | Conditional |
| Mirabegron | 429 (3%) | Low | Possible |
| Aripiprazole | 400 (3%) | Moderate | Possible |
| Venlafaxine | 380 (3%) | High | Possible |
| Fluoxetine | 357 (2%) | Moderate | Conditional |
| Olanzapine | 270 (2%) | Low | Conditional |
| Esomeprazole | 216 (1%) | Moderate | Conditional |
| Amiodarone | 212 (1%) | High | Known |
| Ondansetron | 177 (1%) | High | Known |
| Paroxetine | 182 (1%) | Moderate | Conditional |
| Loperamide | 154 (1%) | High | Conditional |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Rihani, S.B.; Smith, M.K.; Bikmetov, R.; Deodhar, M.; Dow, P.; Turgeon, J.; Michaud, V. Risk of Adverse Drug Events Following the Virtual Addition of COVID-19 Repurposed Drugs to Drug Regimens of Frail Older Adults with Polypharmacy. J. Clin. Med. 2020, 9, 2591. https://doi.org/10.3390/jcm9082591
Al Rihani SB, Smith MK, Bikmetov R, Deodhar M, Dow P, Turgeon J, Michaud V. Risk of Adverse Drug Events Following the Virtual Addition of COVID-19 Repurposed Drugs to Drug Regimens of Frail Older Adults with Polypharmacy. Journal of Clinical Medicine. 2020; 9(8):2591. https://doi.org/10.3390/jcm9082591
Chicago/Turabian StyleAl Rihani, Sweilem B., Matt K. Smith, Ravil Bikmetov, Malavika Deodhar, Pamela Dow, Jacques Turgeon, and Veronique Michaud. 2020. "Risk of Adverse Drug Events Following the Virtual Addition of COVID-19 Repurposed Drugs to Drug Regimens of Frail Older Adults with Polypharmacy" Journal of Clinical Medicine 9, no. 8: 2591. https://doi.org/10.3390/jcm9082591