
Risk Management of COVID-19 in the Residential Educational Setting: Lessons Learned and Implications for Moving Forward

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Setting and Population
3. Methods
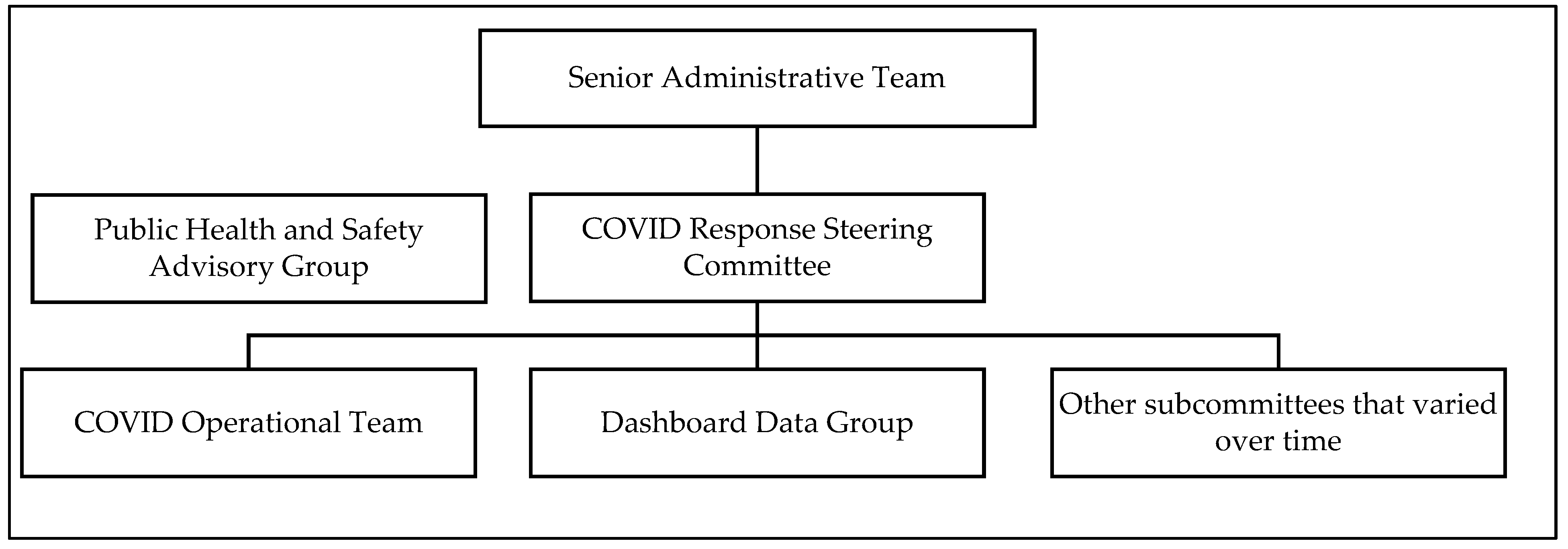
3.1. Public Health Planning and Response Structure and Collaborations
3.1.1. Internal University Structure
3.1.2. External Collaborations
3.2. Implementation of Prevention and Mitigation Strategies
3.2.1. Changes to Academic Calendar
3.2.2. Primary Prevention
3.2.3. Secondary Prevention
3.2.4. Tertiary Prevention
3.3. Fall Semester Events and Public Health Responses
3.4. Inter-Semester Disease Activity and Public Health Planning
3.5. Development and Implementation of Operational Phases
3.6. Spring Semester Events and Public Health Responses
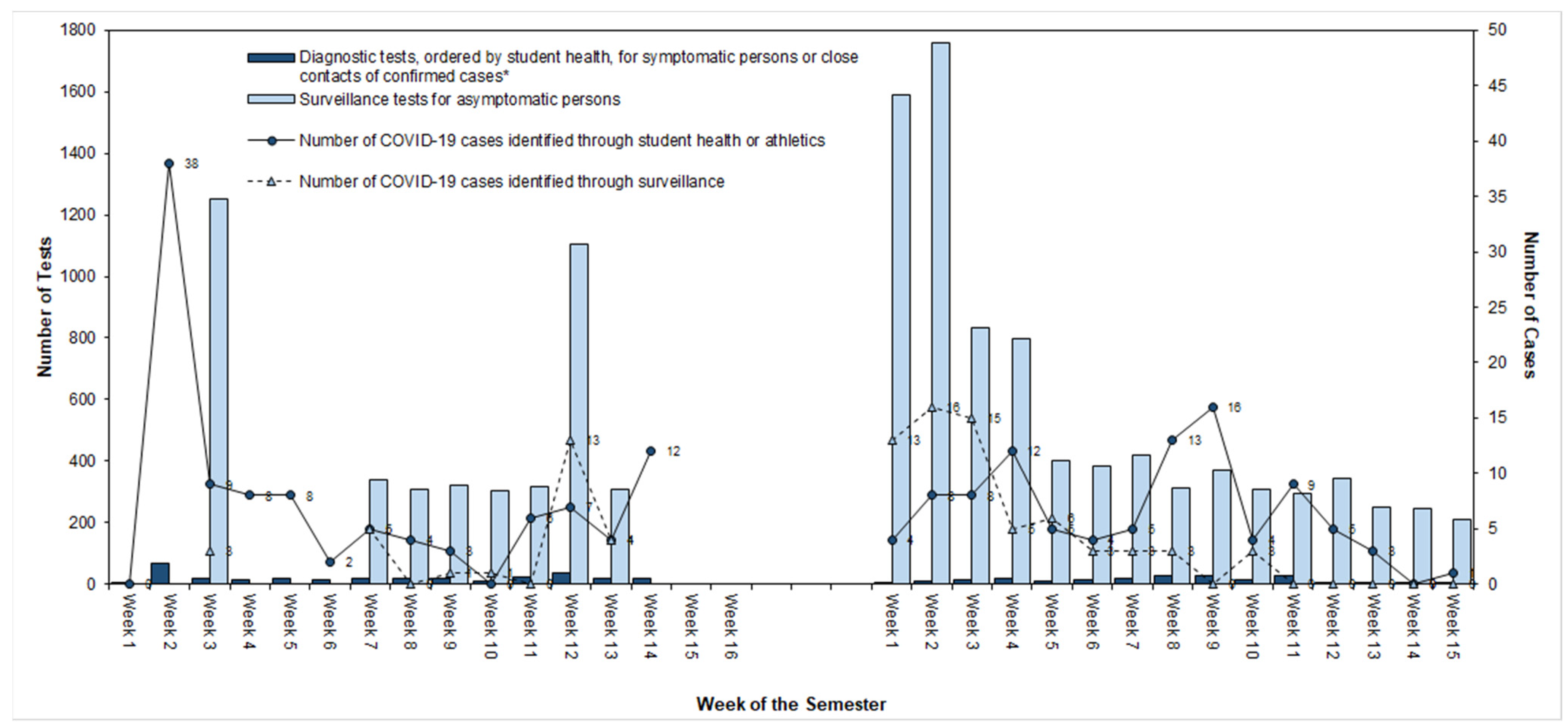
3.7. Data and Analysis for COVID-19 Outcomes
4. Results
COVID-19 Disease Outcomes
5. Discussion
5.1. Successes
5.2. Lessons Learned
5.3. Challenges
5.4. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Declining Enrollment Revenue Risk More Acute for Private Colleges. Available online: https://www.fitchratings.com/research/us-public-finance/declining-enrollment-revenue-risk-more-acute-for-private-colleges-08-06-2020 (accessed on 26 May 2021).
- Looking Ahead to Fall 2020: How COVID-19 Continues to Influence the Choice of College-Going Students. Available online: https://www.artsci.com/studentpoll-covid-19-edition-2 (accessed on 26 May 2021).
- Gardner, L. How college leaders are planning for the fall. Chron High Educ. 2020, 66. Available online: https://www.chronicle.com/article/how-college-leaders-are-planning-for-the-fall/ (accessed on 26 May 2021).
- Fox, M.D.; Bailey, D.C.; Seamon, M.D.; Miranda, M.L. Response to a COVID-19 outbreak on a university campus—Indiana, August 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.; Donovan, C.V.; Campbell, M.; Chai, T.; Pittman, K.; Seña, A.C.; Pettifor, A.; Weber, D.J.; Mallick, A.; Cope, A.; et al. Multiple COVID-19 clusters on a university campus—North Carolina, August 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1416–1418. [Google Scholar] [CrossRef] [PubMed]
- Vang, K.E.; Krow-Lucal, E.R.; James, A.E.; Cima, M.J.; Kothari, A.; Zohoori, N.; Porter, A.; Campbell, E.M. Participation in fraternity and sorority activities and the spread of COVID-19 among residential university communities—Arkansas, 21 August–5 September 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 20–23. [Google Scholar] [CrossRef] [PubMed]
- South Carolina Department of Health and Environmental Control. Recent Disease Activity, by County, for SC Department of Education. 13 January 2021. Available online: https://scdhec.gov/sites/default/files/media/document/RecentDiseaseActivity1_13_2021.pdf (accessed on 20 May 2021).
- Furman University. How We’re Leading. Available online: https://www.furman.edu/furman-focused/preparation (accessed on 4 June 2021).
- COVID-19 Testing: What We Know as of 3 June 2020. American College Health Association. Available online: https://images.magnetmail.net/images/clients/ACHA1//attach/COVID-19_Testing_June-3-2020.pdf (accessed on 21 May 2020).
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19): Interim Considerations for Institutions of Higher Education Administrators for SARS-CoV-2 Testing; US Department of Health and Human Services: Atlanta, GA, USA, 2020.
- Paltiel, A.D.; Zheng, A.; Walensky, R.P. Assessment of SARS-CoV-2 screening strategies to permit the safe reopening of college campuses in the United States. JAMA Netw. Open 2020, 3, e2016818. [Google Scholar] [CrossRef] [PubMed]
- Bahl, R.; Eikmeier, N.; Fraser, A.; Junge, M.; Keesing, F.; Nakahata, K.; Wang, L.Z. Modeling COVID-19 spread in small colleges. arXiv 2020, arXiv:2008.09597. [Google Scholar]
- Furman University. COVID-19 Dashboard and Campus Operational Phases. Available online: https://www.furman.edu/furman-focused/health-resources/covid-19-dashboard/ (accessed on 7 June 2021).
- Kutscher, E.; Greene, R.E. A Harm-Reduction Approach to Coronavirus Disease 2019 (COVID-19)—Safer Socializing. JAMA Health Forum 2020, 1, e200656. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| COVID Response Steering Committee (CRSC) | |
| Members | Responsibilities |
| Vice President for Academic Affairs and Provost (co-chair) Vice President for Student Life (co-chair) Dean of Students (lead/facilitator) Vice President for University Communications Assistant Vice President for University Communications Associate Provost for Engaged Learning Associate Provost for Integrative Science Associate Vice President for Enrollment Services Chief of Police Associate Athletics Director/Senior Women’s Administrator | Oversee COVID-19 planning and implementation of approved recommendations |
| Public Health and Safety Advisory Group (PHSAG) | |
| Members | Responsibilities |
| Associate Provost for Integrative Science (chair) Chief of Police University Student Health Medical Director Associate Athletics Director/Director of Sports Medicine Biomedical Ethicist Epidemiologists (3) University Risk Manager | Make recommendations to CRSC and provide guidance based on emergent research and guidelines Review protocols and proposals developed by subcommittees and university entities Develop surveillance program Review community and on-campus data to recommend university operational phases |
| COVID Operational Team | |
| Members | Responsibilities |
| Student Life Dean of Students (chair) Assistant Dean of Students Director of the Center for Inclusive Communities Assistant Vice President for Student Development Director of Campus Recreation Director of Office of Student Involvement and Inclusion Director of Housing & Residence Life Associate Director, Office of Student Involvement and Inclusion Associate Director of Administration and Finance University Student Health Medical Director Academic Affairs Associate Provost for Integrative Science Associate Provost for Engaged Learning Associate Academic Dean Assistant Academic Dean Athletics Associate Athletics Director/Senior Women’s Administrator Associate Athletics Director/Director of Sports Medicine Associate Athletics Director/Facilities & Game Operations Assistant Athletics Director/Associate Director of Sports Medicine Finance and Administration Associate Vice President for Human Resources Director of Facilities Operations Director of Risk Management Director of Auxiliary Services Chief of Police Other Divisions Associate Vice President for Enrollment Services Assistant Vice President for Strategic Communications Executive Director Alumni and Parent Engagement Bon Appetit Resident District Manager | Operationalize COVID-19 protocols on academic instruction, facilities, student and residence life, technology, and human resources Oversee engagement with campus community and public |
| Dashboard Data Group | |
| Members | Responsibilities |
| Dean of Students Chief of Police University Student Health Medical Director Healthcare Administrator for Athletics University Risk Manager Director of Housing & Residence Life | Collect and review daily data from testing and surveillance Update quarantine and isolation usage Communicate with contact tracing |
| Subcommittees and Workgroups | |
| Strategic Academic Redesign Team Student Advisory Group Academic and Curricular Subcommittee Accessibility and Accommodations Subcommittee Athletic and Sporting Events Subcommittee Buildings and Building Management Subcommittee Communications Subcommittee Dining Subcommittee Education and Training Subcommittee Engaged Learning Subcommittee External Groups, Alumni, Parents, and Visitors Subcommittee | Fall Retention Subcommittee Housing and Residence Life Subcommittee Orientation and Advising Subcommittee Phased Return to Campus Subcommittee Physical Distancing and Safety Measures Enforcement Subcommittee Prevention, Screening, Testing, and Contact Tracing Subcommittee Student Involvement, Programs, and Activities Subcommittee Winter Break Housing Subcommittee Vendors and Contractors Subcommittee |
| Measures Informing Campus Operations Phases | |
|---|---|
| Campus Measures | Total number of students with a positive test in the last 7 days |
| Percent positivity from surveillance tests | |
| Percent of campus in quarantine and/or isolation | |
| Percent of on-campus quarantine and isolation spaces utilized | |
| Community Measures * | Upstate SC acute hospital bed occupancy when elective procedures are cancelled |
| Greenville County two-week cumulative incidence | |
| Greenville County two-week percent positivity | |
| Greenville County two-week incidence trend | |
| Campus Operations Phases | |
| Green: Normal Operations | COVID-19 indicators in the campus and local community are favorable. Vaccines are available and have been successfully distributed both on campus and in the community. Good public health practices remain in place. |
| Purple: Basic Precautions | COVID-19 indicators in the local and/or campus community are at low levels and are trending favorably. Classes are conducted in Flex mode, and campus buildings may be approved to operate under normal hours. Indoor dining is available with a to-go option for students. Face masks and physical distancing are in place, and symptomatic testing is provided for students on-campus. With approval, university-sponsored off-campus activities are permitted, and on-campus activities and community events with more than 30 individuals may be held. Visitors to campus are permitted with limitations. On-campus work for most employees is permitted. |
| Yellow: Enhanced Precautions | COVID-19 indicators in the local and/or campus community are at a moderate or elevated level. Classes are conducted in Flex mode. Academic buildings including the fitness center are open with restricted hours and at a reduced capacity. Indoor dining available with a to-go option for students. On-campus activities of up to 30 individuals may be permitted. Face masks, physical distancing, and enhanced testing are in place. University-sponsored off-campus activities may be permitted on a case-by-case basis. Employees participate in approved remote work options. |
| Orange: High Precautions | COVID-19 indicators in the local and/or campus community are elevated or trending unfavorably, with potential impact on local healthcare systems. Classes may shift to remote learning. Dining options are to-go only, the fitness center is closed, and employees approved to work remotely are encouraged to remain off-campus. Students are asked to reduce contacts as much as possible. Except for normal class meetings, organized campus activities are limited to 10 individuals, and off-campus activities are suspended or remote. Face masks, physical distancing, and enhanced testing are in place, and students are strongly encouraged to remain on-campus. The campus is closed to visitors, and university-sponsored off-campus activities are suspended unless approved, on a case-by-case basis. |
| Red: Full Precautions | COVID-19 indicators in the local and/or campus community suggest widespread transmission with an impact on local healthcare systems. Only essential activities are permitted, which should occur in a virtual setting whenever possible. Campus and building access is limited to essential functions and personnel. Students are required to limit their contacts to roommates, suitemates, or apartment-mates. Dining service is limited to pre-packaged to-go items only. The fitness center is closed, and all employees who are approved to work remotely are required to remain off-campus. Face masks, physical distancing, and enhanced testing measures are in place. The campus is closed to visitors, and both on and off-campus activities are suspended. |
| Student Activity or Characteristic | % Students Infected (No. of Cases/No. of Students) | p-Value † |
|---|---|---|
| Gender | 0.04 | |
| Female | 12.2 (167/1364) | |
| Male | 15.3 (135/885) | |
| Race * | 0.01 | |
| Black, non-Hispanic | 6.0 (9/150) | |
| Hispanic | 9.1 (10/110) | |
| White, non-Hispanic | 14.5 (256/1769) | |
| Other | 12.3 (27/220) | |
| Housing | 0.08 | |
| Dorm (community bath) | 14.6 (107/731) | |
| Dorm (suite bath) | 12.6 (38/302) | |
| On-campus apt | 14.4 (131/909) | |
| Off-campus apt/house | 8.0 (12/150) | |
| Commuter | 8.9 (14/157) | |
| Sorority or Fraternity Membership | <0.01 | |
| Members | 17.2 (180/1044) | |
| Not Members | 10.1 (122/1205) | |
| Education Level | 0.08 | |
| Graduate | 2.9 ‡ | |
| Undergraduate | 13.6 ‡ | |
| Division I Athletes | 0.20 | |
| Athlete | 15.5 (56/361) | |
| Non-athlete | 13.0 (246/1888) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cass, A.L.; Slining, M.M.; Carson, C.; Cassidy, J.; Epright, M.C.; Gilchrist, A.E.; Peterson, K.; Wheeler, J.F.; The, N.S. Risk Management of COVID-19 in the Residential Educational Setting: Lessons Learned and Implications for Moving Forward. Int. J. Environ. Res. Public Health 2021, 18, 9743. https://doi.org/10.3390/ijerph18189743
Cass AL, Slining MM, Carson C, Cassidy J, Epright MC, Gilchrist AE, Peterson K, Wheeler JF, The NS. Risk Management of COVID-19 in the Residential Educational Setting: Lessons Learned and Implications for Moving Forward. International Journal of Environmental Research and Public Health. 2021; 18(18):9743. https://doi.org/10.3390/ijerph18189743
Chicago/Turabian StyleCass, Anna L., Meghan M. Slining, Connie Carson, Jason Cassidy, M. Carmela Epright, Ann E. Gilchrist, Kenneth Peterson, John F. Wheeler, and Natalie S. The. 2021. "Risk Management of COVID-19 in the Residential Educational Setting: Lessons Learned and Implications for Moving Forward" International Journal of Environmental Research and Public Health 18, no. 18: 9743. https://doi.org/10.3390/ijerph18189743