Assessment of Social Distancing for Controlling COVID-19 in Korea: An Age-Structured Modeling Approach


Abstract
:1. Introduction
2. Materials and Methods
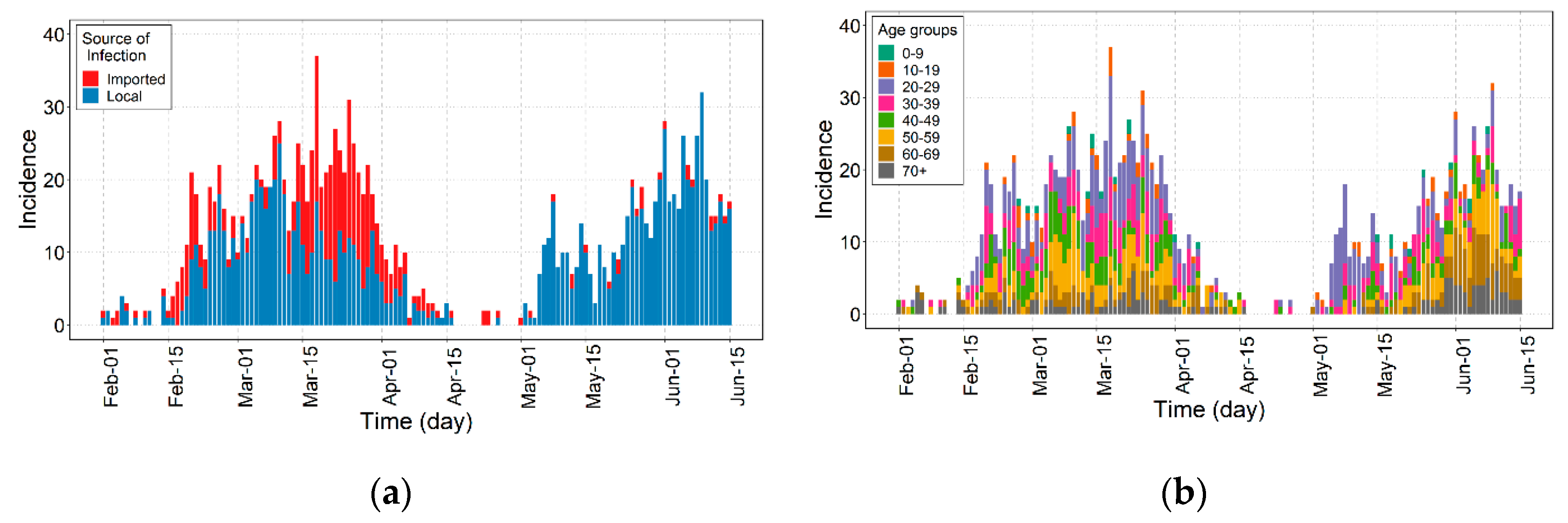
2.1. Epidemiological Data
2.2. Timeline of Control Interventions
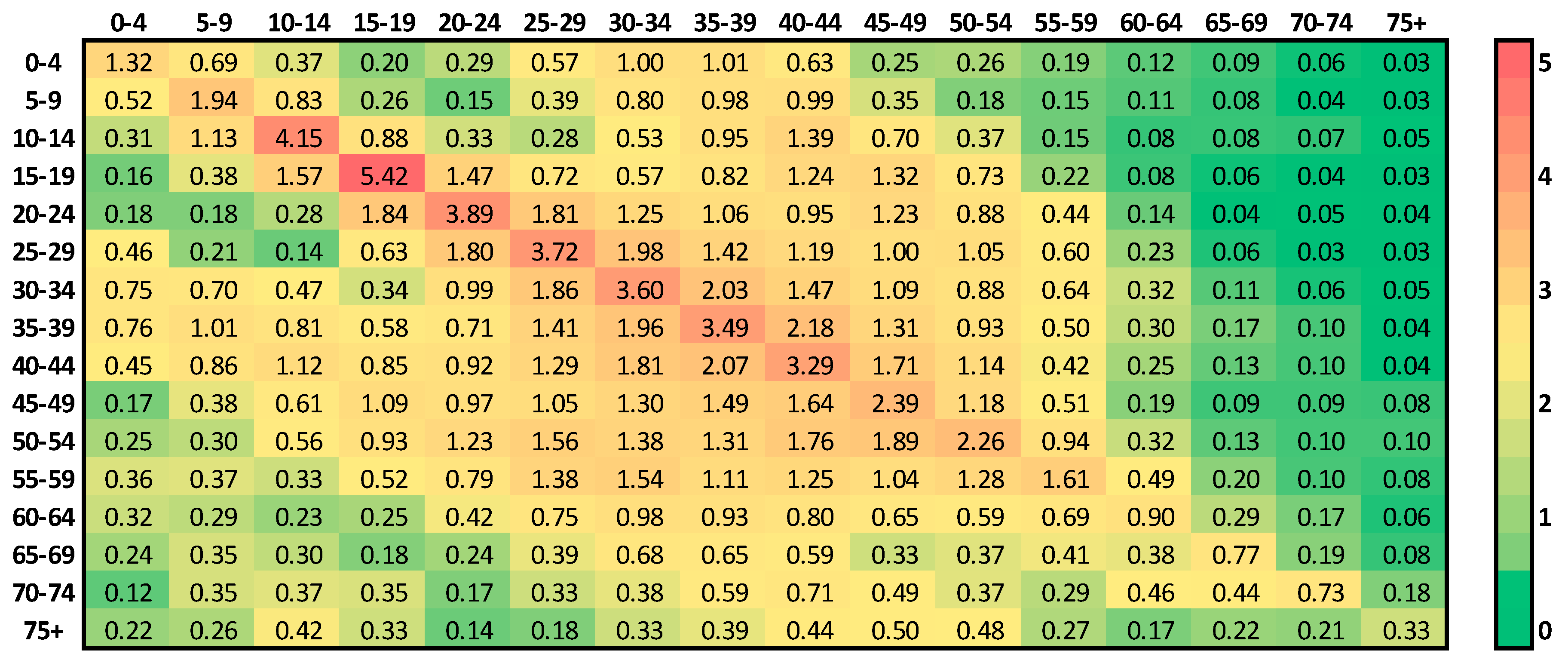
2.3. Contact Matrix
2.4. Mathematical Modeling
2.5. Ethical Considerations
2.6. Data Sharing Policy
3. Result
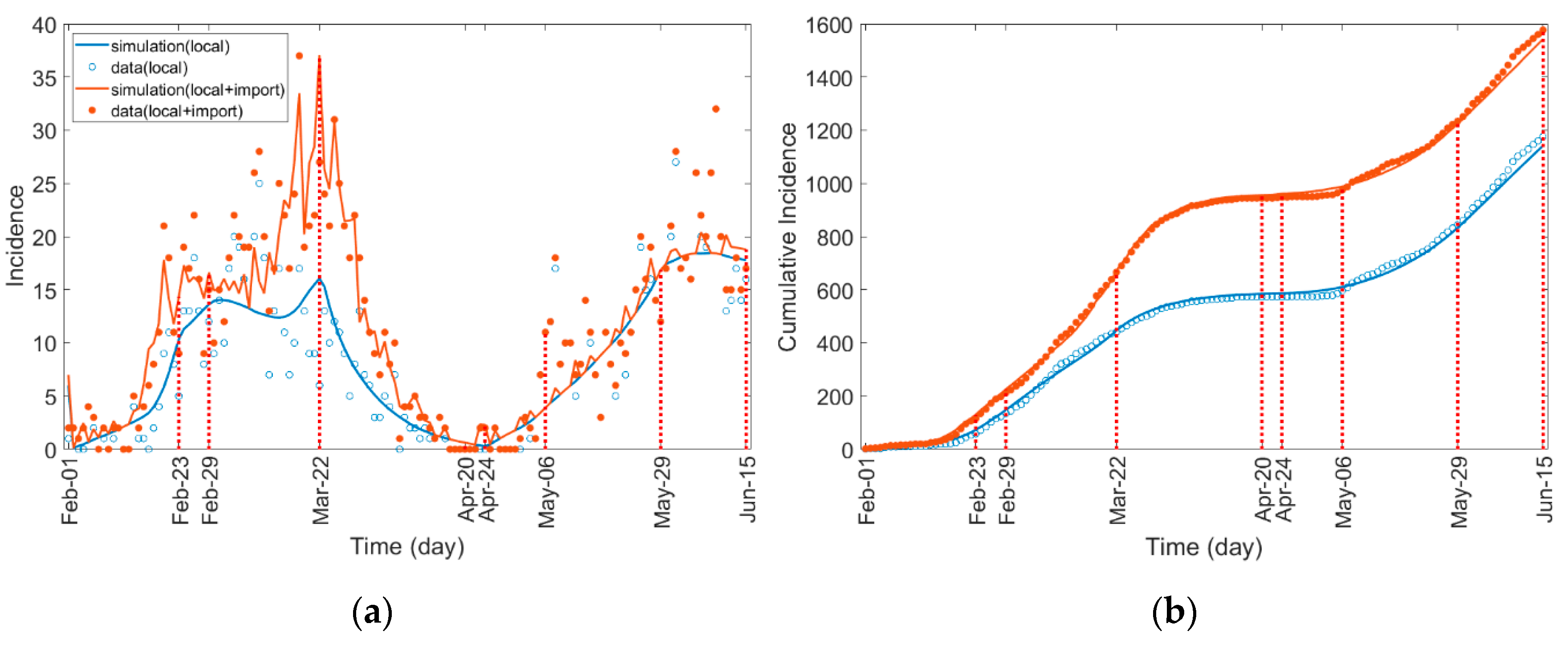
3.1. Estimation of Transmission Rate
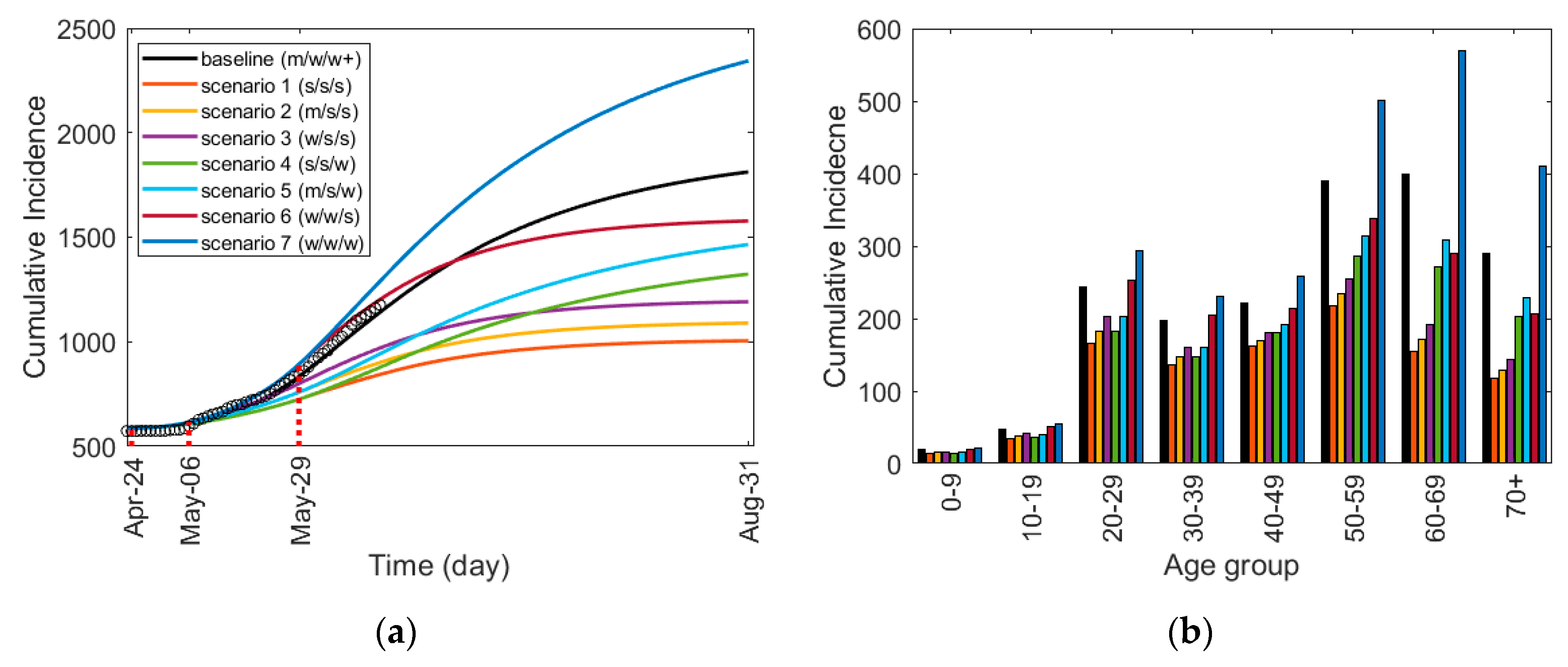
3.2. Effect of the Control Strategies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, X.; Song, Y.; Wong, G.; Cui, J. Bat origin of a new human coronavirus: There and back again. Sci. China Life Sci. 2020, 63, 461–462. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Gorbalenya, A.E.; Baker, S.; Baric, R.; Groot, R.J.D.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Director-General’s opening Remarks at the Media Briefing on COVID-19–11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 21 June 2020).
- World Health Organization (WHO). Coronavirus Disease 2019 (COVID-19) Situation Report—51. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 21 June 2020).
- World Health Organization (WHO). Coronavirus Disease 2019 (COVID-19) Situation Report—209. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200816-covid-19-sitrep-209.pdf?sfvrsn=5dde1ca2_2 (accessed on 19 August 2020).
- Amanat, F.; Krammer, F. SARS-CoV-2 Vaccines: Status Report. Immunity 2020, 52, 583–589. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Draft landscape of COVID-19 Candidate Vaccines. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 20 September 2020).
- World Health Organization (WHO). Coronavirus Disease 2019 (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 21 June 2020).
- Korea Centers for Disease Control & Prevention. Available online: http://www.cdc.go.kr/cdc_eng/ (accessed on 19 August 2020).
- Davies, N.G.; CMMID COVID-19 working group; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; Eggo, R.M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Bentout, S.; Tridane, A.; Djilali, S.; Touaoula, T.M. Age-structured Modeling of COVID-19 Epidemic in the USA, UAE and Algeria. Alex. Eng. J. 2020. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control & Prevention. Cases in Korea by City/Province. Available online: http://ncov.mohw.go.kr/en/bdBoardList.do?brdId=16&brdGubun=162&dataGubun=&ncvContSeq=&contSeq=&board_id=&gubun= (accessed on 5 August 2020).
- Korea Centers for Disease Control & Prevention. Available online: http://ncov.mohw.go.kr/bdBoardList_Real.do?brdId=1&brdGubun=11&ncvContSeq=&contSeq=&board_id=&gubun= (accessed on 5 August 2020).
- Gyeonggi Infectious Disease Control Center. Available online: http://www.gidcc.or.kr/%ec%bd%94%eb%a1%9c%eb%82%98covid19-%ed%98%84%ed%99%a9/ (accessed on 27 July 2020).
- Seoul Metropolitan Government. Available online: https://www.seoul.go.kr/coronaV/coronaStatus.do (accessed on 10 August 2020).
- Korea Centers for Disease Control & Prevention. The Updates of COVID-19 (23 Februrary) in Korea. Available online: https://www.cdc.go.kr/board/board.es?mid=a30402000000&bid=0030&act=view&list_no=366307&tag=&nPage=1 (accessed on 8 August 2020).
- Ministry of Health and Welfare. Available online: http://ncov.mohw.go.kr/tcmBoardView.do?contSeq=355170 (accessed on 8 August 2020).
- Ministry of Health and Welfare. Available online: http://ncov.mohw.go.kr/tcmBoardView.do?brdId=&brdGubun=&dataGubun=&ncvContSeq=354773&contSeq=354773&board_id=&gubun=ALL (accessed on 8 August 2020).
- Gyeonggi Provincial Government. Available online: https://english.gg.go.kr/blog/daily-news/those-who-visited-itaewon-and-nonhyun-dong-after-april-24-need-to-be-tested-for-covid-19/ (accessed on 10 August 2020).
- Mossong, J.; Hens, N.; Jit, M.; Beutels, P.; Auranen, K.; Mikolajczyk, R.; Massari, M.; Salmaso, S.; Tomba, G.S.; Wallinga, J.; et al. Social Contacts and Mixing Patterns Relevant to the Spread of Infectious Diseases. PLoS Med. 2008, 5, e74. [Google Scholar] [CrossRef]
- Prem, K.; Cook, A.R.; Jit, M. Projecting social contact matrices in 152 countries using contact surveys and demographic data. PLoS Comput. Biol. 2017, 13, e1005697. [Google Scholar] [CrossRef]
- Arregui, S.; Aleta, A.; Sanz, J.; Moreno, Y. Projecting social contact matrices to different demographic structures. PLoS Comput. Biol. 2018, 14, e1006638. [Google Scholar] [CrossRef] [Green Version]
- Eames, K.T.D.; Tilston, N.L.; Brooks-Pollock, E.; Edmunds, W.J. Measured Dynamic Social Contact Patterns Explain the Spread of H1N1v Influenza. PLoS Comput. Biol. 2012, 8, e1002425. [Google Scholar] [CrossRef] [Green Version]
- Fumanelli, L.; Ajelli, M.; Manfredi, P.; Vespignani, A.; Merler, S. Inferring the Structure of Social Contacts from Demographic Data in the Analysis of Infectious Diseases Spread. PLoS Comput. Biol. 2012, 8, e1002673. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, N.; Laydon, D.; Nedjati-Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunubá, Z.; Cuomo-Dannenburg, G.; et al. Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand. Imp. Coll. Lond. 2020, 10, 77482. [Google Scholar] [CrossRef]
- Imai, N.; Dorigatti, I.; Cori, A.; Donnelly, C.; Riley, S.; Ferguson, N. Report 2: Estimating the potential total number of novel Coronavirus cases in Wuhan City, China. Imp. Coll. Lond. 2020. [Google Scholar] [CrossRef]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.-Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Korea Centers for Disease Control & Prevention. Updates on COVID-19 in Korea (as of 9 July). Available online: http://ncov.mohw.go.kr/en/tcmBoardView.do?brdId=12&brdGubun=125&dataGubun=&ncvContSeq=3025&contSeq=3025&board_id=&gubun= (accessed on 10 August 2020).
- Zhao, S.; Musa, S.S.; Hebert, J.T.; Cao, P.; Ran, J.; Meng, J.; He, D.; Qin, J. Modelling the effective reproduction number of vector-borne diseases: The yellow fever outbreak in Luanda, Angola 2015-2016 as an example. PeerJ 2020, 8, e8601. [Google Scholar] [CrossRef]
- Lee, H.; Lee, S.; Lee, C.H. Stochastic methods for epidemic models: An application to the 2009 H1N1 influenza outbreak in Korea. Appl. Math. Comput. 2016, 286, 232–249. [Google Scholar] [CrossRef]
- Modchang, C.; Iamsirithaworn, S.; Auewarakul, P.; Triampo, W. A modeling study of school closure to reduce influenza transmission: A case study of an influenza A (H1N1) outbreak in a private Thai school. Math. Comput. Model. 2012, 55, 1021–1033. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Total | Source of Infection | Region | ||
|---|---|---|---|---|---|
| Local | Imported | Seoul | Gyeonggi | ||
| All age groups | 1577 (100.0%) | 1176 (74.6%) | 401 (25.4%) | 798 (50.6%) | 779 (49.4%) |
| 0–9 | 22 (1.4%) | 19 (1.6%) | 3 (0.7%) | 7 (0.9%) | 15 (1.9%) |
| 10–19 | 61 (3.9%) | 46 (3.9%) | 15 (3.7%) | 34 (4.3%) | 27 (3.5%) |
| 20–29 | 382 (24.2%) | 224 (19.0%) | 158 (39.4%) | 215 (26.9%) | 167 (21.4%) |
| 30–39 | 271 (17.2%) | 177 (15.1%) | 94 (23.4%) | 119 (14.9%) | 152 (19.5%) |
| 40–49 | 217 (13.8%) | 172 (14.6%) | 45 (11.2%) | 104 (13.0%) | 113 (14.5%) |
| 50–59 | 279 (17.7%) | 231 (19.6%) | 48 (12.0%) | 141 (17.7%) | 138 (17.7%) |
| 60–69 | 195 (12.4%) | 170 (14.5%) | 25 (6.2%) | 101 (12.7%) | 94 (12.1%) |
| 70 and older | 150 (9.5%) | 137 (11.6%) | 13 (3.2%) | 77 (9.6%) | 73 (9.4%) |
| Social Distancing | Description |
|---|---|
| Weak Social Distancing (WSD) | Allows daily social and economic activities under epidemic prevention regulations while managing incidence levels under the capacity of the healthcare system.
|
| Weak Social Distancing+ (WSD+) | While Weak Social Distancing is implemented, additional enhanced epidemic control measures are enforced [22].
|
| Medium Social Distancing (MSD) | Reduce incidence levels such that the healthcare system is able to function at its usual operating levels.
|
| Strong Social Distancing (SSD) | Stop the rapid spread of disease and recover quarantine controls.
|
| Policies | Notation | ** | |||
|---|---|---|---|---|---|
| School Opening No Social Distancing | 1 | 1 | 1 | ||
| School Closing No Social Distancing | 1 | 0 * | 1 | ||
| School Closing Weak Social Distancing | 1 * | 0 * | 0.7 * | ||
| School Closing Weak Social Distancing+ | 1 * | 0 * | 0.6 * | ||
| School Closing Medium Social Distancing | 1 * | 0 * | 0.5 * | ||
| School Closing Strong Social Distancing | 1 * | 0 * | 0.3 * |
| Parameter | Description | Value | Reference |
|---|---|---|---|
| Incubation period (day) | 5 | [30] | |
| Symptom onset to confirmed period (day) | Table 5 | Estimated | |
| Transmission rate from age group to | Table 5 | Estimated | |
| Number of contacts made by an individual in age group with individuals in age group | Figure 3 | [25] | |
| Infection probability of a person in age group per contact | Table 5 | Estimated | |
| Recovered/removed rate | * | [13,17] |
| Period | Time Interval | Contact Matrix | * | ||
|---|---|---|---|---|---|
| P1 | 1 February–23 February | 2.1971 | 8 | ||
| P2 | 23 February–29 February | 1.2173 | 5 | ||
| P3 | 29 February–22 March | 0.6776 | 4 | ||
| P4 | 22 March–20 April | 0.1145 | 3 | ||
| P5-1 | 20 April–24 April | 0.0001 | 3 | ||
| P5-2 | 24 April–6 May | 2.4846 | 4 | ||
| P6 | 6 May–29 May | 1.3804 | 3 | ||
| P7 | 29 May–15 June | 0.8047 | 3 |
| Scenario | Time Interval | ||
|---|---|---|---|
| 24 April–6 May | 6 May–29 May | 29 May–31 August | |
| baseline | Medium | Weak | Weak+ |
| 1 | Strong | Strong | Strong |
| 2 | Medium | Strong | Strong |
| 3 | Weak | Strong | Strong |
| 4 | Strong | Strong | Weak |
| 5 | Medium | Strong | Weak |
| 6 | Weak | Weak | Strong |
| 7 | Weak | Weak | Weak |
| Scenario | Age Groups | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | 0–9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70+ | |
| baseline | 1809 | 19 | 48 | 244 | 197 | 222 | 390 | 400 | 289 |
| 1 | 1002 | 14 | 35 | 165 | 136 | 162 | 218 | 154 | 118 |
| −44.6% * | −25.4% | −26.7% | −32.5% | −30.7% | −27.1% | −44.2% | −61.4% | −59.0% | |
| 2 | 1086 | 15 | 38 | 182 | 147 | 170 | 234 | 171 | 129 |
| −40.0% | −20.7% | −21.2% | −25.5% | −25.0% | −23.4% | −40.0% | −57.1% | −55.2% | |
| 3 | 1189 | 16 | 41 | 202 | 161 | 180 | 254 | 192 | 143 |
| −34.3% | −15.0% | −14.5% | −17.1% | −18.2% | −19.0% | −34.9% | −52.0% | −50.6% | |
| 4 | 1320 | 14 | 37 | 182 | 147 | 180 | 286 | 271 | 203 |
| −27.0% | −22.4% | −23.3% | −25.4% | −25.3% | −18.8% | −26.8% | −32.2% | −29.6% | |
| 5 | 1460 | 15 | 40 | 202 | 160 | 191 | 314 | 309 | 229 |
| −19.3% | −17.1% | −17.1% | −17.1% | −18.7% | −13.7% | −19.5% | −22.7% | −20.6% | |
| 6 | 1575 | 20 | 51 | 252 | 205 | 214 | 338 | 289 | 206 |
| −12.9% | 5.7% | 6.1% | 3.0% | 4.1% | −3.3% | −13.4% | −27.7% | −28.7% | |
| 7 | 2338 | 21 | 55 | 294 | 230 | 258 | 501 | 569 | 410 |
| 29.2% | 12.9% | 14.4% | 20.0% | 17.0% | 16.5% | 28.4% | 42.4% | 42.0% | |
| Scenario | May to August | May | June | July | August | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 20–49 | 50+ | Total | 20–49 | 50+ | Total | 20–49 | 50+ | Total | 20–49 | 50+ | Total | 20–49 | 50+ | |
| baseline | 1185 | 357 | 81 | 254 | 170 | 84 | 500 | 120 | 380 | 294 | 45 | 249 | 135 | 20 | 115 |
| 1 | 396 | 157 | 239 | 136 | 96 | 40 | 175 | 47 | 128 | 66 | 11 | 55 | 16 | 2 | 14 |
| −66.6% * | −55.8% | −71.1% | −46.5% | −43.7% | −51.8% | −65.0% | −60.7% | −66.1% | −77.6% | −75.0% | −77.9% | −88.1% | −85.6% | −87.0% | |
| 2 | 476 | 193 | 283 | 169 | 120 | 49 | 208 | 56 | 152 | 77 | 13 | 64 | 20 | 3 | 17 |
| −59.8% | −45.8% | −65.7% | −33.5% | −29.5% | −40.7% | −58.4% | −53.1% | −59.9% | −73.8% | −70.9% | −74.2% | −85.2% | −83.2% | −84.9% | |
| 3 | 573 | 236 | 337 | 210 | 149 | 61 | 248 | 67 | 181 | 90 | 15 | 75 | 23 | 3 | 20 |
| −51.6% | −33.8% | −59.2% | −17.3% | −12.4% | −27.4% | −50.4% | −43.9% | −52.4% | −69.4% | −65.9% | −69.8% | −83.0% | −80.3% | −82.3% | |
| 4 | 713 | 204 | 509 | 137 | 96 | 41 | 271 | 62 | 209 | 195 | 29 | 166 | 107 | 15 | 92 |
| −39.8% | −42.9% | −38.5% | −46.1% | −43.6% | −51.1% | −45.8% | −48.3% | −44.9% | −33.7% | −34.9% | −33.1% | −20.7% | −22.3% | −20.2% | |
| 5 | 850 | 248 | 602 | 170 | 120 | 50 | 322 | 74 | 248 | 229 | 34 | 195 | 125 | 18 | 107 |
| −28.3% | −30.6% | −27.3% | −33.1% | −29.4% | −39.9% | −35.6% | −38.4% | −34.7% | −22.1% | −23.8% | −21.5% | −7.4% | −9.0% | −6.5% | |
| 6 | 946 | 364 | 582 | 313 | 211 | 102 | 437 | 120 | 317 | 153 | 26 | 127 | 40 | 6 | 34 |
| −20.2% | 2.0% | −29.7% | 23.2% | 24.0% | 21.7% | −12.6% | −0.6% | −16.4% | −48.0% | −42.4% | −48.7% | −70.4% | −66.8% | −70.1% | |
| 7 | 1705 | 475 | 1230 | 314 | 211 | 103 | 673 | 156 | 517 | 463 | 70 | 393 | 253 | 37 | 216 |
| 43.9% | 33.1% | 48.5% | 23.6% | 24.2% | 23.3% | 34.6% | 29.7% | 36.0% | 57.5% | 53.0% | 57.9% | 87.4% | 82.8% | 87.9% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Kim, J.S.; Choi, H.; Lee, H.; Lee, C.H. Assessment of Social Distancing for Controlling COVID-19 in Korea: An Age-Structured Modeling Approach. Int. J. Environ. Res. Public Health 2020, 17, 7474. https://doi.org/10.3390/ijerph17207474
Choi Y, Kim JS, Choi H, Lee H, Lee CH. Assessment of Social Distancing for Controlling COVID-19 in Korea: An Age-Structured Modeling Approach. International Journal of Environmental Research and Public Health. 2020; 17(20):7474. https://doi.org/10.3390/ijerph17207474
Chicago/Turabian StyleChoi, Yongin, James Slghee Kim, Heejin Choi, Hyojung Lee, and Chang Hyeong Lee. 2020. "Assessment of Social Distancing for Controlling COVID-19 in Korea: An Age-Structured Modeling Approach" International Journal of Environmental Research and Public Health 17, no. 20: 7474. https://doi.org/10.3390/ijerph17207474