
Clinical Evaluation of an Immunochromatographic-Based IgM/IgG Antibody Assay (GenBody™ COVI040) for Detection of Antibody Seroconversion in Patients with SARS-CoV-2 Infection

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Reagents Used in the Kit
2.2.1. Preparation of SARS-CoV-2 Nucleocapsid Protein (NP) Antigen
2.2.2. Preparation of SARS-CoV-2 S Antigen
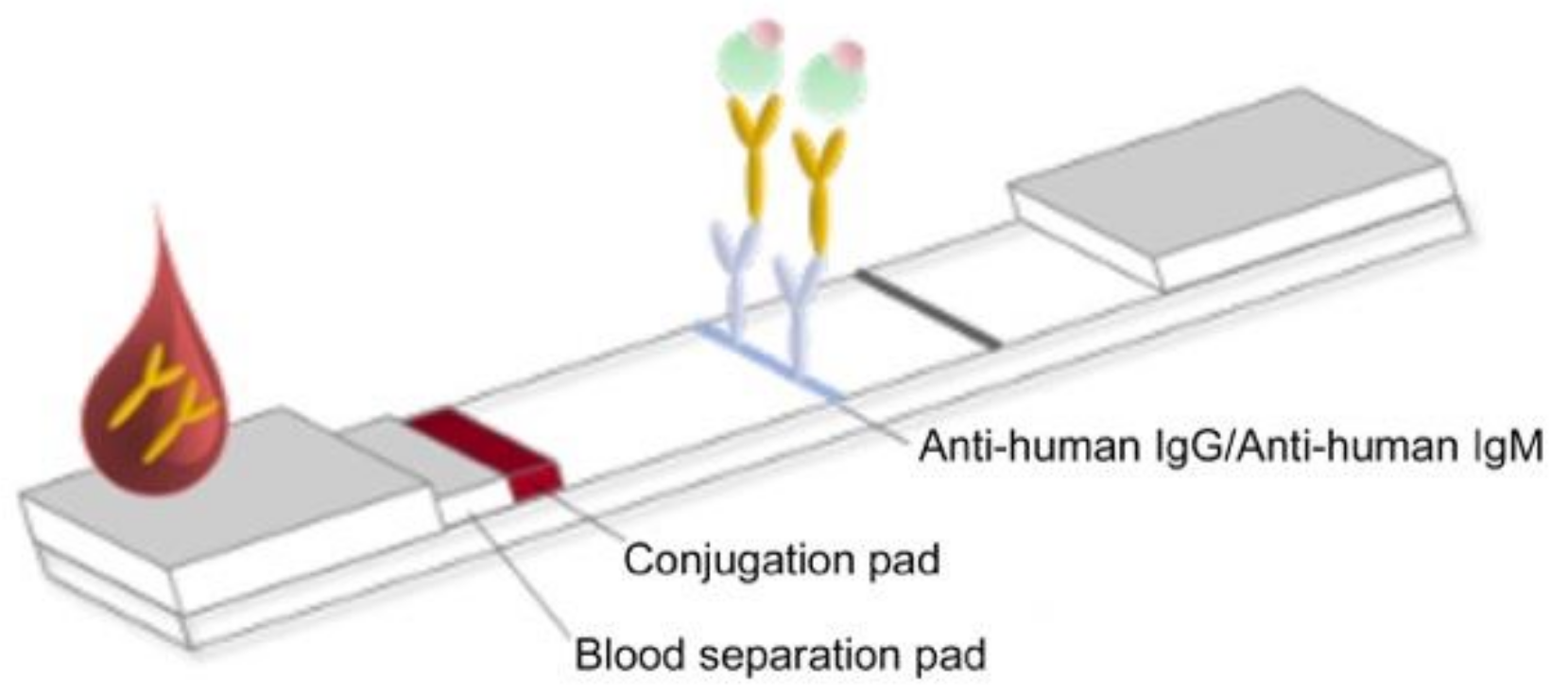
2.3. Preparation of RDT Strips
2.4. Specimen Collection
2.5. Calculation of the Sample Size
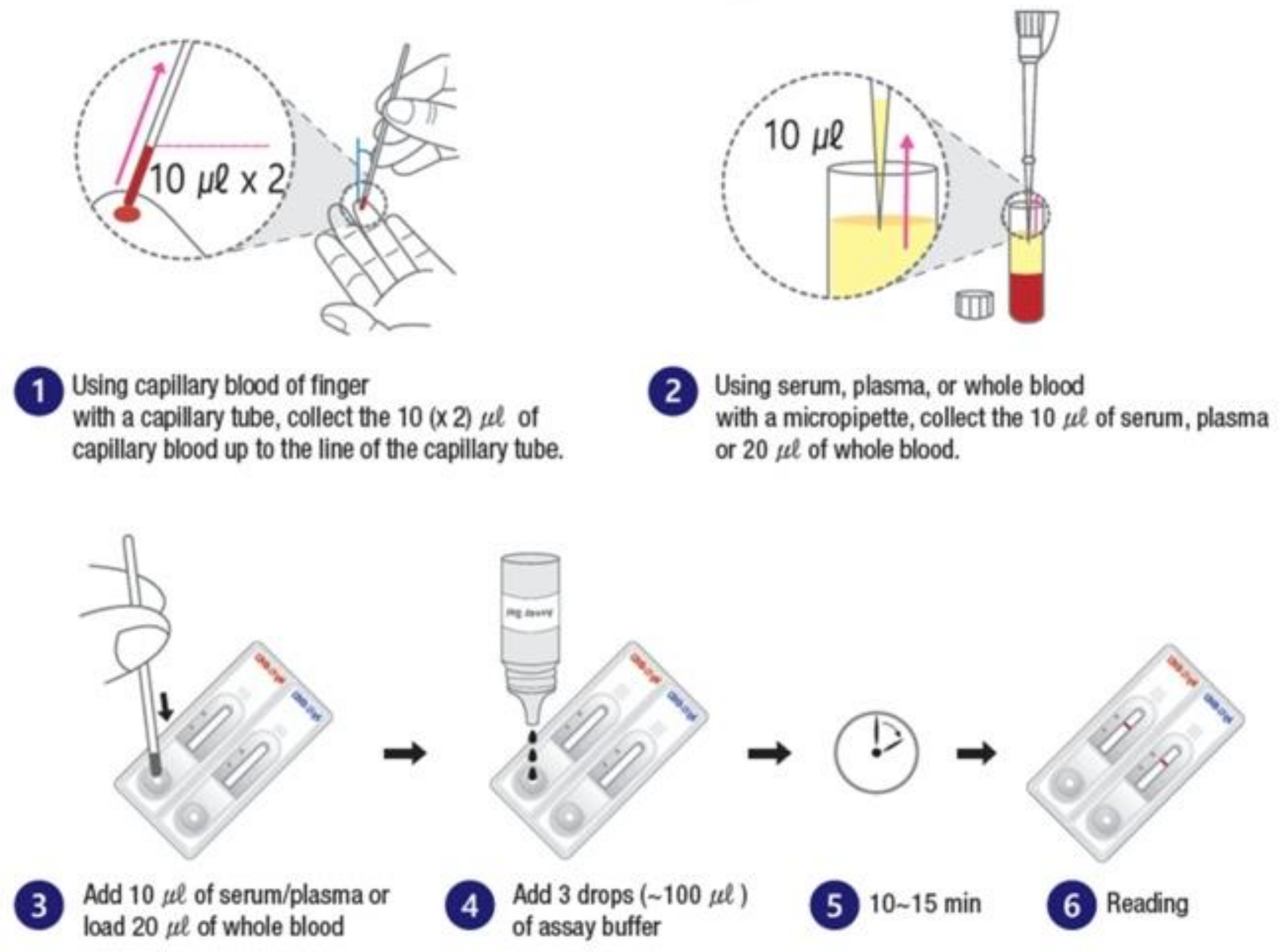
2.6. Methods for Using the Diagnostic Test
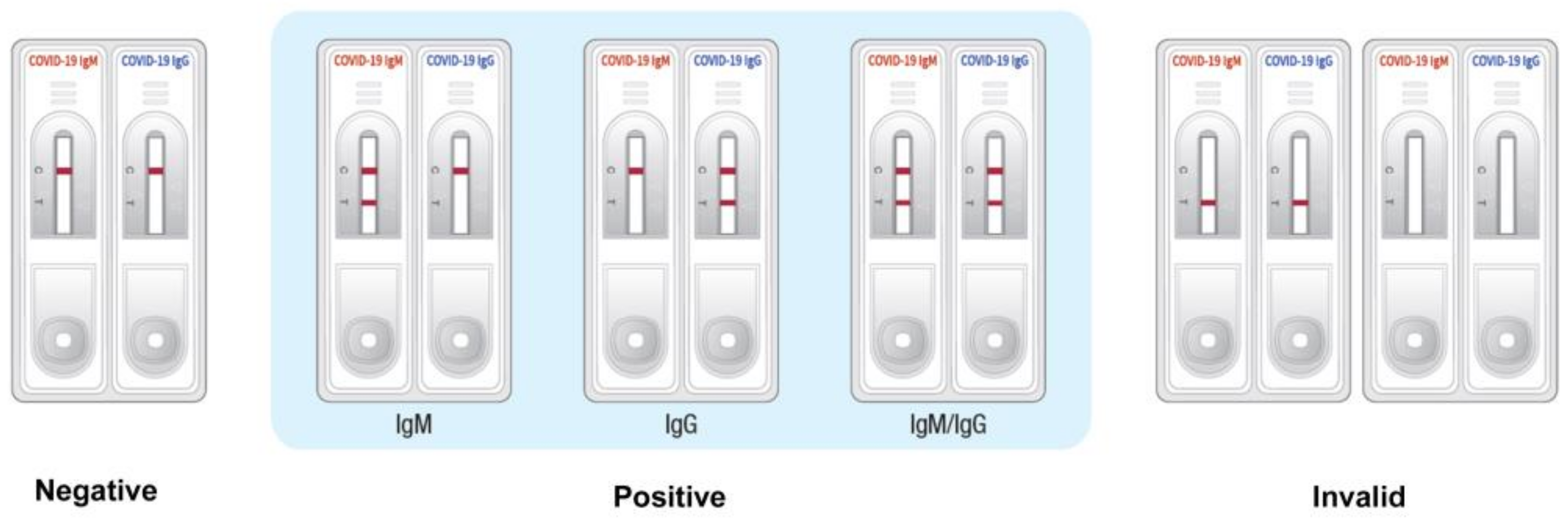
2.7. Interpretation of the Results
2.8. Evaluation Criteria
3. Results
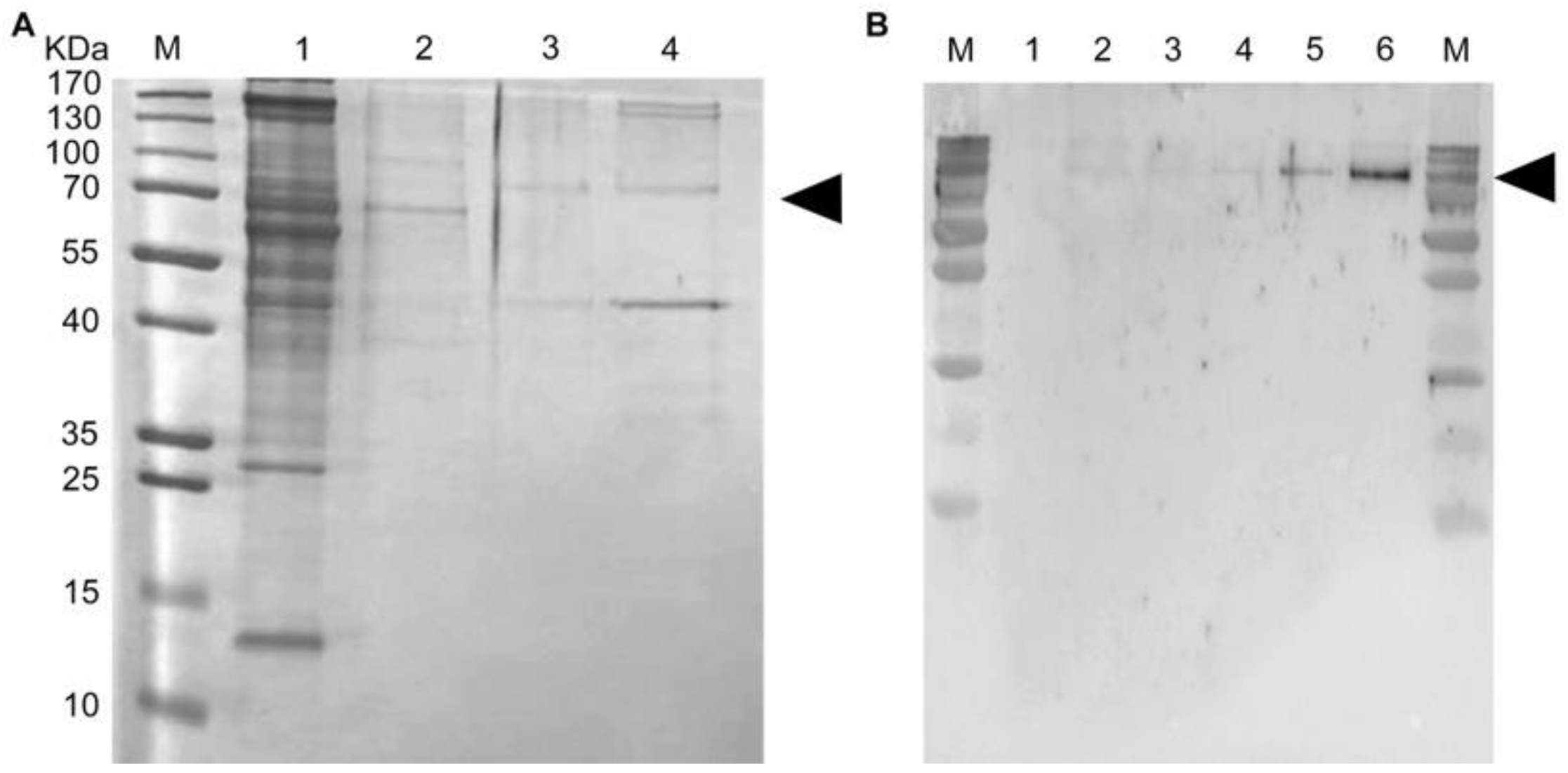
3.1. Expression and Purification of Recombinant SARS-CoV-2 NP and SARS-CoV-2 S
3.2. Clinical Specimen Validation
3.3. Clinical Sensitivity and Specificity of the GenBody™ COVI040 Assay
3.3.1. Clinical Sensitivity and Specificity of IgM/IgG Detection
3.3.2. Clinical Sensitivity and Specificity Based on Days PSO
3.4. Limit of Detection by the GenBody COVID-19 Kit
3.5. Evaluation of Seroconversion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, R.; Zhu, L.; Xue, L.; Liu, L.; Yan, X.; Wang, J.; Zhang, B.; Xu, T.; Ji, F.; Zhao, Y.; et al. Clinical findings of patients with coronavirus disease 2019 in Jiangsu province, China: A retrospective, multi-center study. PLoS Negl. Trop. Dis. 2020, 14, e0008280. [Google Scholar] [CrossRef]
- Kim, D.; Lee, J.Y.; Yang, J.S.; Kim, J.W.; Kim, V.N.; Chang, H. The architecture of SARS-CoV-2 transcriptome. Cell 2020, 181, 914–921. [Google Scholar] [CrossRef]
- Khailany, R.A.; Safdar, M.; Ozaslan, M. Genomic characterization of a novel SARS-CoV-2. Gene Rep. 2020, 19, 100682. [Google Scholar] [CrossRef]
- Grzelak, L.; Temmam, S.; Planchais, C.; Demeret, C.; Tondeur, L.; Huon, C.; Guivel-Benhassine, F.; Staropoli, I.; Chazal, M.; Dufloo, J.; et al. A comparison of four serological assays for detecting anti-SARS-CoV-2 antibodies in human serum samples from different populations. Sci. Transl. Med. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Vashist, S.K. In vitro diagnostic assays for COVID-19: Recent advances and emerging trends. Diagnostics 2020, 10, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- To, K.K.; Tsang, O.T.; Yip, C.C.; Chan, K.H.; Wu, T.C.; Chan, J.M.; Leung, W.S.; Chik, T.S.; Choi, C.Y.; Kandamby, D.H.; et al. Consistent detection of 2019 novel coronavirus in saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Li, R.; Pei, S.; Chen, B.; Song, Y.; Zhang, T.; Yang, W.; Shaman, J. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Wolfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Muller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Hou, H.; Wang, T.; Zhang, B.; Luo, Y.; Mao, L.; Wang, F.; Wu, S.; Sun, Z. Detection of IgM and IgG antibodies in patients with coronavirus disease 2019. Clin. Transl. Immunol. 2020, 9, e01136. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J.; et al. Antibody responses to SARS-CoV-2 in patients with novel coronavirus disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, X.; Liu, J.; Ban, Y.; Li, N.; Wu, Y.; Liu, Y.; Ye, R.; Liu, J.; Li, X.; et al. Serological detection of 2019-nCoV respond to the epidemic: A useful complement to nucleic acid testing. Int. Immunopharmacol. 2020, 88, 106861. [Google Scholar] [CrossRef] [PubMed]
- Lou, B.; Li, T.-D.; Zheng, S.-F.; Su, Y.-Y.; Li, Z.-Y.; Liu, W.; Yu, F.; Ge, S.-X.; Zou, Q.-D.; Yuan, Q.; et al. Serology characteristics of SARS-CoV-2 infection since exposure and post symptom onset. Eur. Respir. J. 2020, 2000763. [Google Scholar] [CrossRef] [PubMed]
- Andrey, D.O.; Cohen, P.; Meyer, B.; Torriani, G.; Yerly, S.; Mazza, L.; Calame, A.; Arm-Vernez, I.; Guessous, I.; Stringhini, S.; et al. Head-to-Head Accuracy Comparison of Three Commercial COVID-19 IgM/IgG Serology Rapid Tests. J. Clin. Med. 2020, 9, 2369. [Google Scholar] [CrossRef] [PubMed]
- Theel, E.S.; Couturier, M.R.; Filkins, L.; Palavecino, E.; Mitchell, S.; Campbell, S.; Pentella, M.; Butler-Wu, S.; Jerke, K.; Dharmarha, V.; et al. Application, verification, and implementation of SARS-CoV-2 serologic assays with emergency use authorization. J. Clin. Microbiol. 2020, 59. [Google Scholar] [CrossRef] [PubMed]
- Robosa, R.S.; Sandaradura, I.; Dwyer, D.E.; O’Sullivan, M.V.N. Clinical evaluation of SARS-CoV-2 point-of-care antibody tests. Pathology 2020, 52, 783–789. [Google Scholar] [CrossRef]
- Zhen, W.; Smith, E.; Manji, R.; Schron, D.; Berry, G.J. Clinical Evaluation of Three Sample-to-Answer Platforms for Detection of SARS-CoV-2. J. Clin. Microbiol. 2020, 58, e00783-20. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Hillyer, C.; Du, L. Neutralizing Antibodies against SARS-CoV-2 and Other Human Coronaviruses. Trends Immunol. 2020, 41, 355–359. [Google Scholar] [CrossRef]
- Rongqing, Z.; Li, M.; Song, H.; Chen, J.; Ren, W.; Feng, Y.; Gao, G.F.; Song, J.; Peng, Y.; Su, B.; et al. Early Detection of Severe Acute Respiratory Syndrome Coronavirus 2 Antibodies as a Serologic Marker of Infection in Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2066–2072. [Google Scholar] [CrossRef]
- Velay, A.; Gallais, F.; Benotmane, I.; Wendling, M.J.; Danion, F.; Collange, O.; De Seze, J.; Schmidt-Mutter, C.; Schneider, F.; Bilbault, P.; et al. Evaluation of the performance of SARS-CoV-2 serological tools and their positioning in COVID-19 diagnostic strategies. Diagn. Microbiol. Infect. Dis. 2020, 98, 115181. [Google Scholar] [CrossRef]
- Van Elslande, J.; Houben, E.; Depypere, M.; Brackenier, A.; Desmet, S.; Andre, E.; Van Ranst, M.; Lagrou, K.; Vermeersch, P. Diagnostic performance of seven rapid IgG/IgM antibody tests and the Euroimmun IgA/IgG ELISA in COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Lin, J.; Duan, X.; Huang, W.; Lu, X.; Zhou, J.; Zong, Z. Asymptomatic COVID-19 patients can contaminate their surroundings: An environment sampling study. mSphere 2020, 5. [Google Scholar] [CrossRef]
- Peng, L.; Liu, J.; Xu, W.X.; Luo, Q.M.; Chen, D.B.; Lei, Z.Y.; Huang, Z.L.; Li, X.J.; Deng, K.J.; Lin, B.L.; et al. SARS-CoV-2 can be detected in urine, blood, anal swabs, and oropharyngeal swabs specimens. J. Med Virol. 2020, 92, 1676–1680. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Sun, J.; Nie, S.; Li, H.; Kong, Y.; Liang, M.; Hou, J.; Huang, X.; Li, D.; Ma, T.; et al. Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China. Nat. Med. 2020, 26, 1193–1195. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.X.; Liu, B.Z.; Deng, H.J.; Wu, G.C.; Deng, K.; Chen, Y.K.; Liao, P.; Qiu, J.F.; Lin, Y.; Cai, X.F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Bruggen, M.C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Positive | Negative | Total | ||||
|---|---|---|---|---|---|---|
| Days post symptom onset (PSO) | ≤7 | 7–13 | ≥14 | Total | ||
| Number of Samples | 14 | 27 | 89 | 130 | 100 | 230 |
| Evaluation Results of Test Equipment (GenBody COVID-19 Kit) IgM/IgG | Confirmed Results through RT-PCR | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Positive | 127 | 0 | 127 |
| Negative | 3 | 100 | 103 |
| Total | 130 | 100 | 230 |
| Evaluation Results of Test Equipment (GenBody COVID-19 kit) IgM | Confirmed Results through RT-PCR | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Positive | 107 | 0 | 107 |
| Negative | 23 | 100 | 123 |
| Total | 130 | 100 | 230 |
| Evaluation Results of Test Equipment (GenBody COVID-19 Kit) IgG | Confirmed RESULTS through RT-PCR | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Positive | 127 | 0 | 127 |
| Negative | 3 | 100 | 103 |
| Total | 130 | 100 | 230 |
| Evaluation Results of Test Equipment (GenBody COVID-19 Kit) | Confirmed Results through RT-PCR Positive | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0–6 Days PSO | 7–13 Days PSO | ≥14 Days PSO | |||||||
| IgM/IgG | IgM | IgG | IgM/IgG | IgM | IgG | IgM/IgG | IgM | IgG | |
| Positive | 11 | 10 | 11 | 27 | 23 | 27 | 89 | 74 | 89 |
| Negative | 03 | 04 | 03 | 00 | 04 | 00 | 00 | 15 | 00 |
| Total | 14 | 14 | 14 | 27 | 27 | 27 | 89 | 89 | 89 |
| Sensitivity | 78.57% | 71.43% | 78.57% | 100.00% | 85.19% | 100.00% | 100.00% | 83.15% | 100.00% |
| 95% CI | 49.20~95.34% | 41.90%~91.61% | 49.20~95.34% | 87.23~100.00% | 66.27~100.00% | 87.23~100.00% | 95.94~100.00% | 73.73~90.25% | 95.94~100.00% |
| Sample No. | Symptom Onset/PCR Confirmation Date | Date of Sample Collection for GenBody Kit Analysis | Days PSO | GenBody COVID-19 IgM/IgG | ||
|---|---|---|---|---|---|---|
| IgM | IgG | Remarks | ||||
| 1 | 2020-03-02 | 2020-03-08 | 06 | + | + | + |
| 2020-03-02 | 2020-03-16 | 14 | + | + | + | |
| 2020-03-02 | 2020-03-23 | 21 | + | + | + | |
| 2 | 2020-03-09 | 2020-03-10 | 01 | - | - | - |
| 2020-03-09 | 2020-03-17 | 08 | + | + | + | |
| 2020-03-09 | 2020-03-24 | 05 | + | + | + | |
| 2020-03-09 | 2020-03-31 | 22 | + | + | + | |
| 3 | 2020-03-10 | 2020-03-10 | 00 | - | - | - |
| 2020-03-10 | 2020-03-25 | 15 | - | + | + | |
| 2020-03-10 | 2020-03-30 | 20 | - | + | + | |
| 4 | 2020-03-03 | 2020-03-07 | 04 | + | + | + |
| 2020-03-03 | 2020-03-13 | 10 | + | + | + | |
| 2020-03-03 | 2020-03-19 | 16 | + | + | + | |
| 2020-03-03 | 2020-03-24 | 21 | + | + | + | |
| 5 | 2020-03-02 | 2020-03-09 | 07 | + | + | + |
| 2020-03-02 | 2020-03-16 | 14 | + | + | + | |
| 2020-03-02 | 2020-03-25 | 24 | + | + | + | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Lee, J.; Bal, J.; Chong, C.-K.; Lee, J.H.; Park, H. Clinical Evaluation of an Immunochromatographic-Based IgM/IgG Antibody Assay (GenBody™ COVI040) for Detection of Antibody Seroconversion in Patients with SARS-CoV-2 Infection. Diagnostics 2021, 11, 537. https://doi.org/10.3390/diagnostics11030537
Kim D, Lee J, Bal J, Chong C-K, Lee JH, Park H. Clinical Evaluation of an Immunochromatographic-Based IgM/IgG Antibody Assay (GenBody™ COVI040) for Detection of Antibody Seroconversion in Patients with SARS-CoV-2 Infection. Diagnostics. 2021; 11(3):537. https://doi.org/10.3390/diagnostics11030537
Chicago/Turabian StyleKim, Doyeong, Jihoo Lee, Jyotiranjan Bal, Chom-Kyu Chong, Jong Ho Lee, and Hyun Park. 2021. "Clinical Evaluation of an Immunochromatographic-Based IgM/IgG Antibody Assay (GenBody™ COVI040) for Detection of Antibody Seroconversion in Patients with SARS-CoV-2 Infection" Diagnostics 11, no. 3: 537. https://doi.org/10.3390/diagnostics11030537