
Balancing Benefits and Harms of COVID-19 Vaccines: Lessons from the Ongoing Mass Vaccination Campaign in Lombardy, Italy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Target Population and Data Sources
2.2. The Italian Vaccination Campaign
2.3. Cohort Selection and Typing
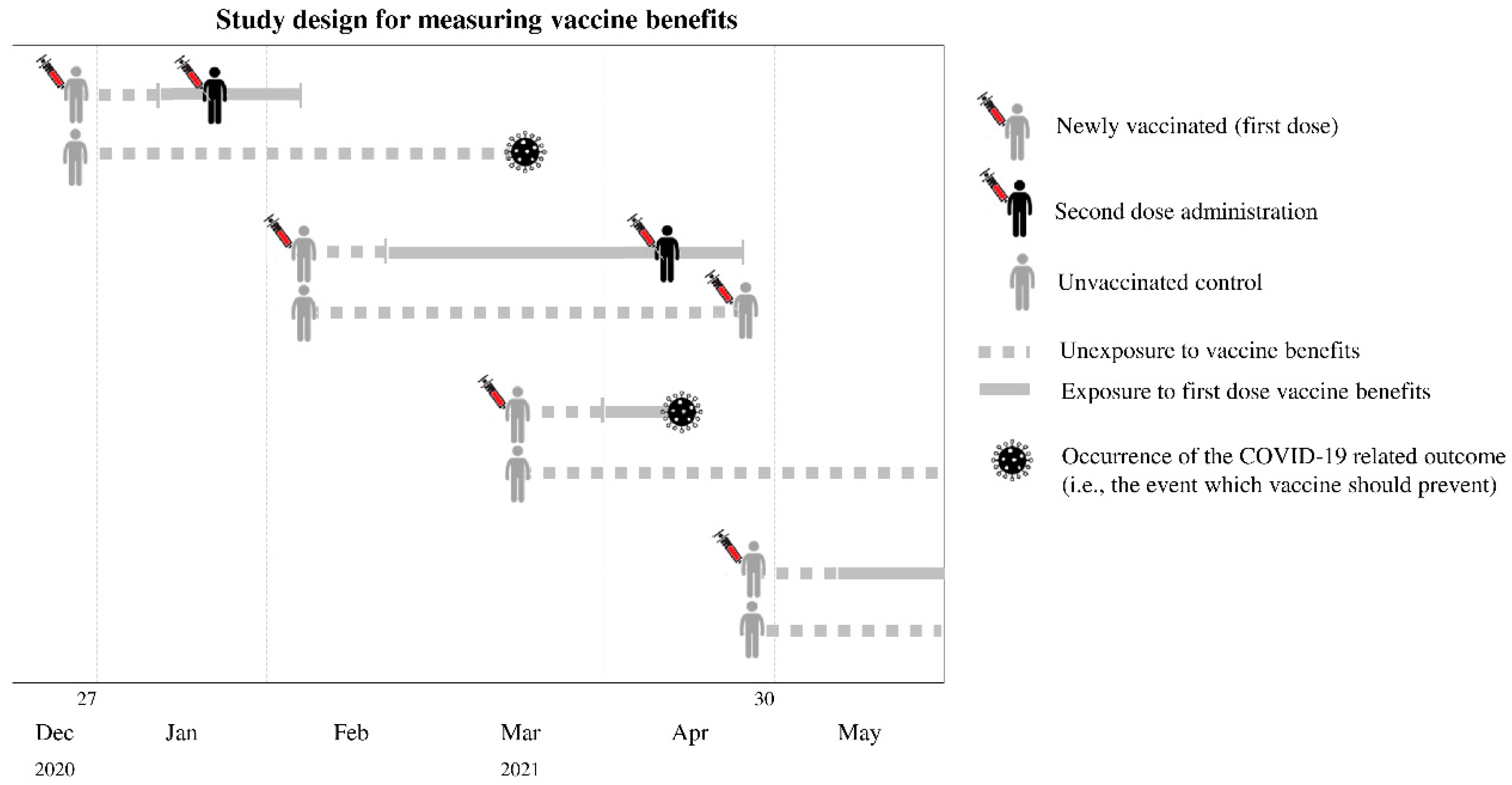
2.4. Measuring Vaccine Benefits
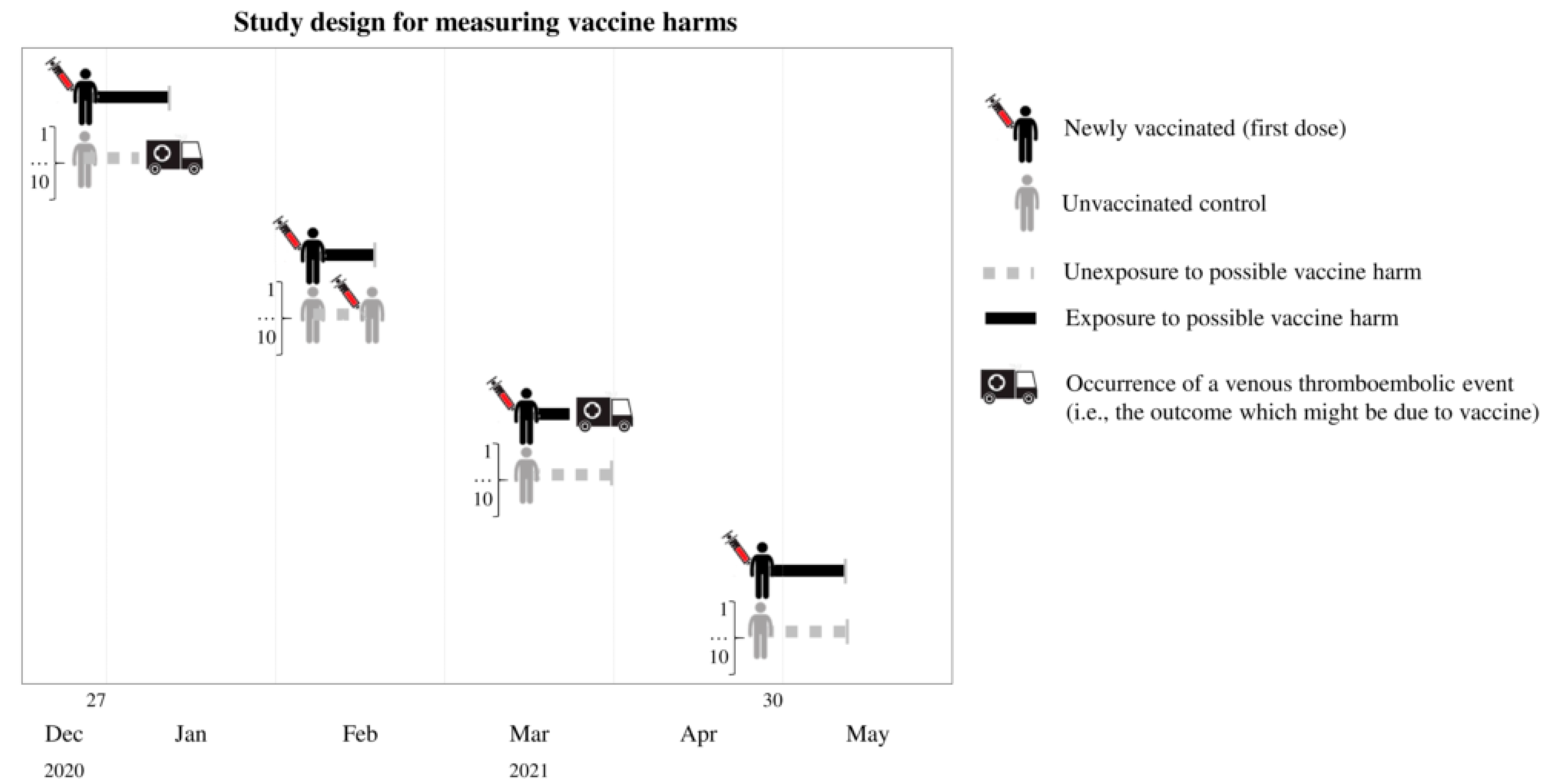
2.5. Measuring Vaccine Harm
2.6. Main Analyses
2.7. Supplementary Analyses
3. Results
3.1. Study Population
3.2. Benefit-Related Outcomes
3.3. Harm-Related Outcomes
3.4. Benefits and Harms Associated with Oxford-AstraZeneca Vaccination
3.5. Benefits and Harms Associated with Pfizer or Moderna Vaccination
3.6. Supplementary Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Code Availability
References
- Conte, C.; Sogni, F.; Affanni, P.; Veronesi, L.; Argentiero, A.; Esposito, S. Vaccines against Coronaviruses: The State of the Art. Vaccines 2020, 8, 309. [Google Scholar] [CrossRef] [PubMed]
- Forman, R.; Shah, S.; Jeurissen, P.; Jit, M.; Mossialos, E. COVID-19 vaccine challenges: What have we learned so far and what remains to be done? Health Policy 2021, 125, 553–567. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2021, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.; Folegatti, P.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: A pooled analysis of four randomised trials. Lancet 2021, 397, 881–891. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Wise, J. COVID-19: European countries suspend use of Oxford-AstraZeneca vaccine after reports of blood clots. Br. Med. J. 2021, 372, n699. [Google Scholar] [CrossRef]
- European Medicines Agency. COVID-19 Vaccine AstraZeneca: PRAC Investigating Cases of Thromboembolic Events—Vaccine’s Benefits Currently still Outweigh Risks—Update. 11 March 2021. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccineastrazeneca-prac-investigating-casesthromboembolic-events-vaccines-benefits (accessed on 14 June 2021).
- European Medicines Agency. Annex to Vaxzevria Art.5.3—Visual Risk Contextualization. 23 April 2021. Available online: https://www.ema.europa.eu/en/documents/chmp-annex/annex-vaxzevria-art53-visual-risk-contextualisation_en.pdf (accessed on 14 April 2022).
- Pottegård, A.; Lund, L.C.; Karlstad, Ø.; Dahl, J.; Andersen, M.; Hallas, J.; Lidegaard, Ø.; Tapia, G.; Gulseth, H.L.; Ruiz, P.L.-D.; et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: Population based cohort study. Br. Med. J. 2021, 373, n1114. [Google Scholar] [CrossRef] [PubMed]
- Trifirò, G.; Gini, R.; Barone-Adesi, F.; Beghi, E.; Cantarutti, A.; Capuano, A.; Carnovale, C.; Clavenna, A.; Dellagiovanna, M.; Ferrajolo, C.; et al. The Role of European Healthcare Databases for Post-Marketing Drug Effectiveness, Safety and Value Evaluation: Where Does Italy Stand? Drug Saf. 2019, 42, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Rea, F.; Ludergnani, M.; Apolone, G.; Corrao, G. Renin-Angiotensin-Aldosterone System Blockers and the Risk of COVID-19. N. Engl. J. Med. 2020, 382, 2431–2440. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. People with Certain Medical Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 3 February 2021).
- Ebrahimi, M.; Malehi, A.S.; Rahim, F. COVID-19 Patients: A Systematic Review and Meta-Analysis of Laboratory Findings, Comorbidities, and Clinical Outcomes Comparing Medical Staff versus the General Population. Osong. Public Health Res. Perspect. 2020, 11, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Wolberg, A.S.; Rosendaal, F.R.; Weitz, J.I.; Jaffer, I.H.; Agnelli, G.; Baglin, T.; Mackman, N. Venous thrombosis. Nat. Rev. Dis. Primers 2015, 1, 15006. [Google Scholar] [CrossRef]
- Østergaard, S.D.; Schmidt, M.; Horváth-Puhó, E.; Thomsen, R.W.; Sørensen, H.T. Thromboembolism and the Oxford-AstraZeneca COVID-19 vaccine: Side-effect or coincidence? Lancet 2021, 397, 1441–1443. [Google Scholar] [CrossRef]
- Austin, P.C. Using the Standardized Difference to Compare the Prevalence of a Binary Variable Between Two Groups in Observational Research. Commun. Stat. Simul. Comput. 2009, 38, 1228–1234. [Google Scholar] [CrossRef]
- Suter, K.; Briel, M.; Günther, J. The number needed to treat (NNT) and the number needed to harm (NNH). Med. Monatsschr. Pharm. 2015, 38, 103–106. [Google Scholar]
- Altman, D.G. Confidence intervals for the number needed to treat. BMJ 1998, 317, 1309–1312. [Google Scholar] [CrossRef] [Green Version]
- Stang, A.; Poole, C.; Bender, R. Common problems related to the use of number needed to treat. J. Clin. Epidemiol. 2010, 63, 820–825. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Zani, A.; Caccuri, F.; Messali, S.; Bonfanti, C.; Caruso, A. Serosurvey in BNT162b2 vaccine-elicited neutralizing antibodies against authentic B.1, B.1.1.7, B.1.351, B.1.525 and P.1 SARS-CoV-2 variants. Emerg. Microbes Infect. 2021, 10, 1241–1243. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Zuckerman, N.; Nemet, I.; Atari, N.; Kliker, L.; Regev-Yochay, G.; Sapir, E.; Mor, O.; Alroy-Preis, S.; Mendelson, E.; et al. Neutralising capacity against Delta (B.1.617.2) and other variants of concern following Comirnaty (BNT162b2, BioNTech/Pfizer) vaccination in health care workers, Israel. Euro Surveill. 2021, 26, 2100557. [Google Scholar] [CrossRef] [PubMed]
- Funk, T.; Pharris, A.; Spiteri, G.; Bundle, N.; Melidou, A.; Carr, M.; Gonzalez, G.; Garcia-Leon, A.; Crispie, F.; O’Connor, L.; et al. Characteristics of SARS-CoV-2 variants of concern B.1.1.7, B.1.351 or P.1: Data from seven EU/EEA countries, weeks 38/2020 to 10/2021. Euro Surveill. 2021, 26, 2100348. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, B.A.; Gerlovin, H.; Madenci, A.L.; Kurgansky, K.E.; Ferolito, B.R.; Muñiz, M.J.F.; Gagnon, D.R.; Gaziano, J.M.; Cho, K.; Casas, J.P.; et al. Comparative Effectiveness of BNT162b2 and mRNA-1273 Vaccines in U.S. Veterans. N. Engl. J. Med. 2022, 386, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Husby, A.; Hansen, J.V.; Fosbøl, E.; Thiesson, E.M.; Madsen, M.; Thomsen, R.W.; Sørensen, H.T.; Andersen, M.; Wohlfahrt, J.; Gislason, G.; et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: Population based cohort study. BMJ 2021, 375, e068665. [Google Scholar] [CrossRef] [PubMed]
- Lwanga, S.K.; Lemeshow, S. Sample Size Determination in Health Studies: A Practical Manual; World Health Organization: Geneva, Switzerland, 1991; Available online: https://apps.who.int/iris/handle/10665/40062 (accessed on 3 February 2021).



{kind=link}
{kind=link}
| AstraZeneca | Pfizer or Moderna | |||||
|---|---|---|---|---|---|---|
| Vaccinated (N = 755,557) | Unvaccinated (N = 755,557) | SMD | Vaccinated (N = 1,596,326) | Unvaccinated (N = 1,596,326) | SMD | |
| Women | ||||||
| <50 years | 110,500 (24.7%) | 110,500 (24.7%) | MV | 145,584 (15.7%) | 145,584 (15.7%) | MV |
| 50–59 years | 57,671 (12.9%) | 57,671 (12.9%) | 103,873 (11.2%) | 103,873 (11.2%) | ||
| 60–69 years | 80,917 (18.1%) | 80,917 (18.1%) | 127,078 (13.7%) | 127,078 (13.7%) | ||
| 70–79 years | 195,128 (43.6%) | 195,128 (43.6%) | 153,191 (16.6%) | 153,191 (16.6%) | ||
| ≥80 years | 2941 (0.7%) | 2941 (0.7%) | 394,754 (42.7%) | 394,754 (42.7%) | ||
| Men | ||||||
| <50 years | 55,659 (18.0%) | 55,659 (18.0%) | MV | 89,336 (13.3%) | 89,336 (13.3%) | MV |
| 50–59 years | 27,181 (8.8%) | 27,181 (8.8%) | 65,951 (9.8%) | 65,951 (9.8%) | ||
| 60–69 years | 65,065 (21.1%) | 65,065 (21.1%) | 120,553 (17.9%) | 120,553 (17.9%) | ||
| 70–79 years | 158,639 (51.4%) | 158,639 (51.4%) | 146,410 (21.8%) | 146,410 (21.8%) | ||
| ≥80 years | 1856 (0.6%) | 1856 (0.6%) | 249,596 (37.1%) | 249,596 (37.1%) | ||
| Risk factors for SARS-CoV-2 severe clinical manifestations | ||||||
| Solid malignancies and neoplasm of lymphatic and haematopoietic tissue | 15,972 (2.1%) | 24,084 (3.2%) | −0.067 | 91,288 (5.7%) | 63,503 (4.0%) | 0.081 |
| Hypothyroidism | 41,279 (5.5%) | 43,637 (5.8%) | −0.014 | 119,161 (7.5%) | 100,077 (6.3%) | 0.047 |
| Diabetes without insulin therapy | 35,120 (4.7%) | 53,418 (7.1%) | −0.103 | 169,941 (10.7%) | 134,946 (8.5%) | 0.075 |
| Insulin therapy | 2484 (0.3%) | 15,330 (2.0%) | −0.158 | 66,335 (4.2%) | 43,289 (2.7%) | 0.079 |
| Dyslipidaemia | 167,512 (22.2%) | 165,865 (22.0%) | 0.005 | 495,679 (31.1%) | 403,997 (25.3%) | 0.128 |
| Gout | 23,052 (3.1%) | 28,043 (3.7%) | −0.037 | 118,534 (7.4%) | 100,062 (6.3%) | 0.046 |
| Autoimmune haemolytic anaemias, other anaemias, anaemias only tracked from drug therapy | 48,496 (6.4%) | 61,673 (8.2%) | −0.067 | 227,932 (14.3%) | 199,795 (12.5%) | 0.052 |
| Psychosis | 10,039 (1.3%) | 15,095 (2.0%) | −0.052 | 65,713 (4.1%) | 61,796 (3.9%) | 0.013 |
| Depression | 73,365 (9.7%) | 72,610 (9.6%) | 0.003 | 236,767 (14.8%) | 204,808 (12.8%) | 0.058 |
| Parkinson’s disease and parkinsonism | 5373 (0.7%) | 7439 (1.0%) | −0.030 | 32,637 (2.0%) | 29,834 (1.9%) | 0.013 |
| Epilepsy and recurrent seizures | 8810 (1.2%) | 13,748 (1.8%) | −0.054 | 47,753 (3.0%) | 37,401 (2.3%) | 0.040 |
| Glaucoma | 23,734 (3.1%) | 21,864 (2.9%) | 0.014 | 78,886 (4.9%) | 69,309 (4.3%) | 0.029 |
| Ischaemic heart disease/angina | 10,882 (1.4%) | 15,155 (2.0%) | −0.043 | 68,664 (4.3%) | 59,692 (3.7%) | 0.029 |
| Arrhythmia | 20,037 (2.7%) | 21,561 (2.9%) | −0.012 | 96,275 (6.0%) | 80,751 (5.1%) | 0.043 |
| Hypertension | 140,756 (18.6%) | 137,931 (18.3%) | 0.010 | 430,070 (26.9%) | 373,414 (23.4%) | 0.082 |
| Coronary and peripheral vascular disease | 54,103 (7.2%) | 59,040 (7.8%) | −0.025 | 186,319 (11.7%) | 160,611 (10.1%) | 0.052 |
| Oral anticoagulant agents | 22,695 (3.0%) | 28,929 (3.8%) | −0.045 | 148,215 (9.3%) | 129,640 (8.1%) | 0.041 |
| Other diseases of the circulatory system | 10,506 (1.4%) | 14,921 (2.0%) | −0.045 | 56,681 (3.6%) | 45,482 (2.9%) | 0.040 |
| Chronic obstructive pulmonary disease, asthma, chronic respiratory disease only tracked from drug therapy | 67,906 (9.0%) | 66,118 (8.8%) | 0.008 | 170,732 (10.7%) | 152,844 (9.6%) | 0.037 |
| Other diseases of the respiratory system | 5695 (0.8%) | 9586 (1.3%) | −0.051 | 39,612 (2.5%) | 36,213 (2.3%) | 0.014 |
| Inflammatory bowel diseases (Ulcerative colitis and Chron’s disease) | 13,349 (1.8%) | 13,227 (1.8%) | 0.001 | 38,463 (2.4%) | 29,252 (1.8%) | 0.040 |
| Other diseases of the digestive system | 16,503 (2.2%) | 17,227 (2.3%) | −0.006 | 52,822 (3.3%) | 45,202 (2.8%) | 0.028 |
| Other diseases of the genitourinary system | 13,881 (1.8%) | 14,790 (2.0%) | −0.009 | 44,839 (2.8%) | 40,361 (2.5%) | 0.017 |
| Diseases of the skin and subcutaneous tissues, including no rheumatoid psoriasis | 9347 (1.2%) | 10,722 (1.4%) | −0.016 | 27,481 (1.7%) | 23,801 (1.5%) | 0.018 |
| Other diseases of the musculoskeletal system and connective tissue | 17,137 (2.3%) | 16,166 (2.1%) | 0.009 | 43,326 (2.7%) | 36,357 (2.3%) | 0.028 |
| Symptoms, signs, and ill-defined conditions | 4700 (0.6%) | 7611 (1.0%) | −0.043 | 30,252 (1.9%) | 25,403 (1.6%) | 0.023 |
| Chronic pain | 21,321 (2.8%) | 24,775 (3.3%) | −0.027 | 93,131 (5.8%) | 81,542 (5.1%) | 0.032 |
| Corticosteroids | 80,619 (10.7%) | 85,663 (11.3%) | −0.021 | 231,005 (14.5%) | 195,454 (12.2%) | 0.065 |
| Hormone therapy (oral contraceptives or replacement hormone therapy) among women | 10,841 (2.4%) | 9090 (2.0%) | 0.020 | 17,686 (1.9%) | 14,931 (1.6%) | 0.017 |
| Number of contacts with healthcare services of RHS | ||||||
| <5 | 273,563 (36.2%) | 253,203 (33.5%) | 0.057 | 333,773 (20.9%) | 473,336 (29.7%) | −0.202 |
| 5–100 | 400,607 (53.0%) | 445,051 (58.9%) | −0.119 | 901,350 (56.5%) | 836,878 (52.4%) | 0.081 |
| >100 | 81,387 (10.8%) | 57,303 (7.6%) | 0.111 | 361,203 (22.6%) | 286,112 (17.9%) | 0.117 |
| Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age Category (Years) | Exposure to Vaccine Benefits (First Dose) | Unexposure to Vaccine Benefits | Incidence Rate Ratio (95% CI) (a) | Number Needed to Treat (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 7 | 198,035 | 0.35 | 111 | 302,575 | 3.67 | 0.10 (0.05 to 0.22) | 0.11 (0.05 to 0.23) | 3063 (210 to 3957) |
| 50–59 | 8 | 95,952 | 0.83 | 78 | 149,102 | 5.23 | 0.16 (0.08 to 0.33) | 0.16 (0.08 to 0.34) | 2274 (180 to 3226) |
| 60–69 | 12 | 52,563 | 2.28 | 100 | 117,698 | 8.50 | 0.27 (0.15 to 0.49) | 0.31 (0.17 to 0.56) | 1609 (241 to 2472) |
| 70–79 | 10 | 58,529 | 1.71 | 190 | 190,324 | 9.98 | 0.17 (0.09 to 0.32) | 0.20 (0.10 to 0.38) | 1209 (177 to 1550) |
| ≥80 | 1 | 1997 | 5.01 | 8 | 4373 | 18.29 | 0.27 (0.03 to 2.19) | 0.30 (0.04 to 2.49) | - |
| Total | 38 | 407,077 | 0.93 | 487 | 764,072 | 6.37 | |||
| Age Category (Years) | Exposure to Vaccine Harms (First Dose) | Unexposure To Vaccine Harms | Incidence Rate Ratio (95% CI) (a) | Number Needed to Harm (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 7 | 99,556 | 0.70 | 30 | 995,563 | 0.30 | 2.33 (1.02 to 5.31) | 2.43 (1.05 to 5.63) | 23,207 (10,274 to 89,707) |
| 50–59 | 4 | 51,391 | 0.78 | 28 | 513,884 | 0.54 | 1.43 (0.50 to 4.07) | 1.53 (0.54 to 4.38) | - |
| 60–69 | 4 | 56,267 | 0.71 | 53 | 562,560 | 0.94 | 0.75 (0.27 to 2.08) | 0.78 (0.28 to 2.18) | - |
| 70–79 | 12 | 100,237 | 1.20 | 293 | 1,001,500 | 2.93 | 0.41 (0.23 to 0.73) | 0.39 (0.21 to 0.72) | - |
| ≥80 | 0 | 2191 | 0.00 | 12 | 21,792 | 5.51 | - | - | - |
| Total | 27 | 309,642 | 0.87 | 416 | 3,095,299 | 1.34 | |||
| Men | |||||||||
| Age Category (Years) | Exposure to Vaccine Benefits (First Dose) | Unexposure to Vaccine Benefits | Incidence Rate Ratio (95% CI) (a) | Number Needed to Treat (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 11 | 107,608 | 1.02 | 74 | 160,921 | 4.60 | 0.22 (0.15 to 0.48) | 0.27 (0.15 to 0.49) | 2796 (319 to 4283) |
| 50–59 | 8 | 49,469 | 1.62 | 90 | 75,166 | 11.97 | 0.14 (0.08 to 0.30) | 0.15 (0.08 to 0.30) | 966 (123 to 1313) |
| 60–69 | 9 | 38,341 | 2.35 | 112 | 89,850 | 12.47 | 0.19 (0.09 to 0.37) | 0.20 (0.10 to 0.39) | 988 (133 to 1366) |
| 70–79 | 22 | 45,579 | 4.83 | 296 | 151,433 | 19.55 | 0.25 (0.16 to 0.38) | 0.28 (0.18 to 0.43) | 679 (222 to 860) |
| ≥80 | 2 | 1277 | 15.66 | 10 | 2772 | 36.08 | 0.43 (0.10 to 1.98) | 0.46 (0.09 to 2.25) | - |
| Total | 52 | 242,274 | 2.15 | 582 | 480,142 | 12.12 | |||
| Age Category (Years) | Exposure to Vaccine Harms (First Dose) | Unexposure To Vaccine Harms | Incidence Rate Ratio (95% CI) (a) | Number Needed to Harm (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 1 | 50,669 | 0.20 | 33 | 506,677 | 0.65 | 0.30 (0.04–2.22) | 0.29 (0.04–2.12) | - |
| 50–59 | 3 | 24,608 | 1.22 | 28 | 246,071 | 1.14 | 1.07 (0.33–3.52) | 1.12 (0.34–3.69) | - |
| 60–69 | 8 | 43,846 | 1.82 | 98 | 438,323 | 2.24 | 0.82 (0.40–1.68) | 0.81 (0.39–1.68) | - |
| 70–79 | 14 | 79,934 | 1.75 | 332 | 797,823 | 4.16 | 0.42 (0.25–0.72) | 0.40 (0.24–0.69) | - |
| ≥80 | 1 | 1374 | 7.28 | 10 | 13,623 | 7.34 | 0.99 (0.13–7.75) | 1.18 (0.14–9.88) | - |
| Total | 27 | 200,431 | 1.35 | 501 | 2,002,517 | 2.50 | |||
| Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age Category (Years) | Exposure to Vaccine Benefits (First Dose) | Unexposure to Vaccine Benefits | Incidence Rate Ratio (95% CI) (a) | Number Needed to Treat (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 13 | 100,665 | 1.29 | 196 | 490,974 | 3.99 | 0.32 (0.19 to 0.57) | 0.28 (0.16 to 0.50) | 3479 (2678 to 4964) |
| 50–59 | 6 | 67,909 | 0.88 | 180 | 318,755 | 5.65 | 0.16 (0.07 to 0.35) | 0.14 (0.06 to 0.31) | 2059 (1690 to 2635) |
| 60–69 | 9 | 48,052 | 1.87 | 178 | 202,892 | 8.77 | 0.21 (0.11 to 0.43) | 0.20 (0.10 to 0.39) | 1425 (1140 to 1898) |
| 70–79 | 20 | 45,489 | 4.40 | 234 | 164,078 | 14.26 | 0.31 (0.21 to 0.52) | 0.29 (0.18 to 0.46) | 988 (785 to 1331) |
| ≥80 | 248 | 142,079 | 17.46 | 2248 | 572,002 | 39.30 | 0.44 (0.40 to 0.53) | 0.45 (0.40 to 0.52) | 463 (411 to 529) |
| Total | 296 | 404,194 | 7.32 | 3036 | 1,748,702 | 17,36 | |||
| Age Category (Years) | Exposure to Vaccine Harms (First Dose) | Unexposure To Vaccine Harms | Incidence Rate Ratio (95% CI) (a) | Number Needed to Harm (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 10 | 131,525 | 0.76 | 38 | 1,309,922 | 0.29 | 2.62 (1.31 to 5.26) | 1.65 (0.79 to 3.47) | - |
| 50–59 | 2 | 91,961 | 0.22 | 34 | 916,009 | 0.37 | 0.59 (0.14 to 2.44) | 0.40 (0.09 to 1.67) | - |
| 60–69 | 10 | 84,627 | 1.18 | 93 | 843,316 | 1.10 | 1.07 (0.56 to 2.06) | 0.78 (0.40 to 1.50) | - |
| 70–79 | 16 | 85,737 | 1.87 | 273 | 854,630 | 3.19 | 0.58 (0.35 to 0.97) | 0.45 (0.27 to 0.76) | - |
| ≥80 | 99 | 268,027 | 3.69 | 1385 | 2,603,444 | 5.32 | 0.69 (0.57 to 0.85) | 0.70 (0.57 to 0.85) | - |
| Total | 137 | 661,878 | 2.07 | 1823 | 6,527,321 | 2.79 | |||
| Men | |||||||||
| Age Category (Years) | Exposure to Vaccine Benefits (First Dose) | Unexposure to Vaccine Benefits | Incidence Rate Ratio (95% CI) (a) | Number Needed to Treat (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 8 | 61,389 | 1.30 | 98 | 272,808 | 3.59 | 0.36 (0.18 to 0.78) | 0.30 (0.14 to 0.63) | 3977 (2777 to 7002) |
| 50–59 | 9 | 42,272 | 2.13 | 166 | 171,452 | 9.68 | 0.22 (0.12 to 0.44) | 0.18 (0.09 to 0.36) | 1260 (1013 to 1666) |
| 60–69 | 21 | 44,774 | 4.69 | 315 | 187,785 | 16.77 | 0.28 (0.18 to 0.44) | 0.24 (0.16 to 0.38) | 784 (651 to 988) |
| 70–79 | 36 | 42,957 | 8.38 | 393 | 161,173 | 24.38 | 0.34 (0.26 to 0.51) | 0.33 (0.23 to 0.46) | 612 (501 to 786) |
| ≥80 | 179 | 76,801 | 23.31 | 1844 | 321,868 | 57.29 | 0.41 (0.36 to 0.49) | 0.41 (0.35 to 0.48) | 296 (262 to 339) |
| Total | 253 | 268,193 | 2816 | 1,115,086 | |||||
| Age Category (Years) | Exposure to Vaccine Harms (First Dose) | Unexposure to Vaccine Harms | Incidence Rate Ratio (95% CI) (a) | Number Needed to Harm (95% CI) (b) | |||||
| Events | PM | IR (per 10,000 PM) | Events | PM | IR (per 10,000 PM) | Unadjusted | Adjusted | ||
| <50 | 1 | 81,069 | 0.12 | 18 | 806,954 | 0.22 | 0.55 (0.07 to 4.14) | 0.46 (0.06 to 3.53) | - |
| 50–59 | 12 | 58,442 | 2.05 | 47 | 581,519 | 0.81 | 2.54 (1.35 to 4.79) | 1.69 (0.85 to 3.37) | - |
| 60–69 | 23 | 80,154 | 2.87 | 175 | 798,403 | 2.19 | 1.31 (0.85 to 2.02) | 0.93 (0.59 to 1.45) | - |
| 70–79 | 22 | 81,567 | 2.70 | 322 | 812,848 | 3.96 | 0.68 (0.44 to 1.05) | 0.60 (0.39 to 0.93) | - |
| ≥80 | 58 | 158,754 | 3.65 | 1025 | 1,530,971 | 6.70 | 0.55 (0.42 to 0.71) | 0.53 (0.41 to 0.70) | - |
| Total | 116 | 459,986 | 1587 | 4,530,695 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corrao, G.; Rea, F.; Franchi, M.; Cereda, D.; Barone, A.; Borriello, C.R.; Della Valle, G.P.; Ercolanoni, M.; Jara, J.; Preziosi, G.; et al. Balancing Benefits and Harms of COVID-19 Vaccines: Lessons from the Ongoing Mass Vaccination Campaign in Lombardy, Italy. Vaccines 2022, 10, 623. https://doi.org/10.3390/vaccines10040623
Corrao G, Rea F, Franchi M, Cereda D, Barone A, Borriello CR, Della Valle GP, Ercolanoni M, Jara J, Preziosi G, et al. Balancing Benefits and Harms of COVID-19 Vaccines: Lessons from the Ongoing Mass Vaccination Campaign in Lombardy, Italy. Vaccines. 2022; 10(4):623. https://doi.org/10.3390/vaccines10040623
Chicago/Turabian StyleCorrao, Giovanni, Federico Rea, Matteo Franchi, Danilo Cereda, Antonio Barone, Catia Rosanna Borriello, Giulia Petra Della Valle, Michele Ercolanoni, Jose Jara, Giuseppe Preziosi, and et al. 2022. "Balancing Benefits and Harms of COVID-19 Vaccines: Lessons from the Ongoing Mass Vaccination Campaign in Lombardy, Italy" Vaccines 10, no. 4: 623. https://doi.org/10.3390/vaccines10040623