
Altered Vascular Endothelium-Dependent Responsiveness in Frail Elderly Patients Recovering from COVID-19 Pneumonia: Preliminary Evidence

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Overview
2.1.1. Data Collection
2.1.2. Systemic Vascular Function via sPLM
2.1.3. Level of Physical Function
2.2. Data Analysis
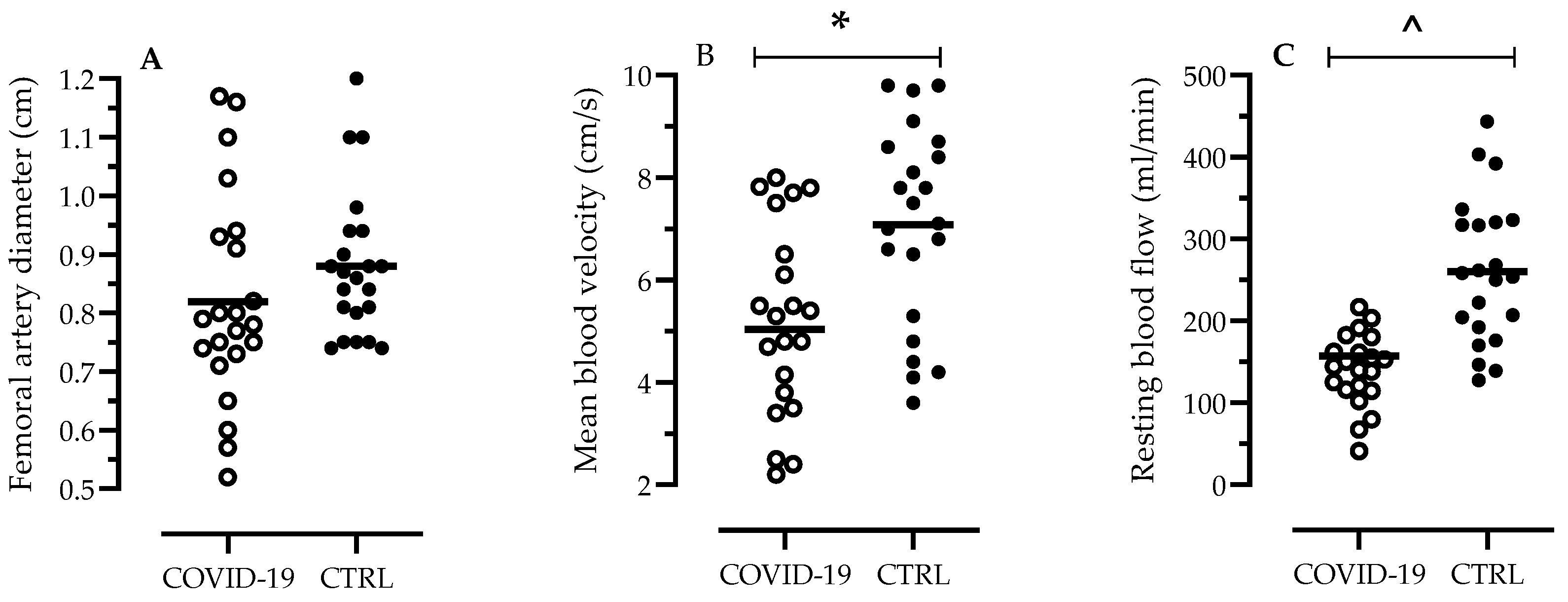
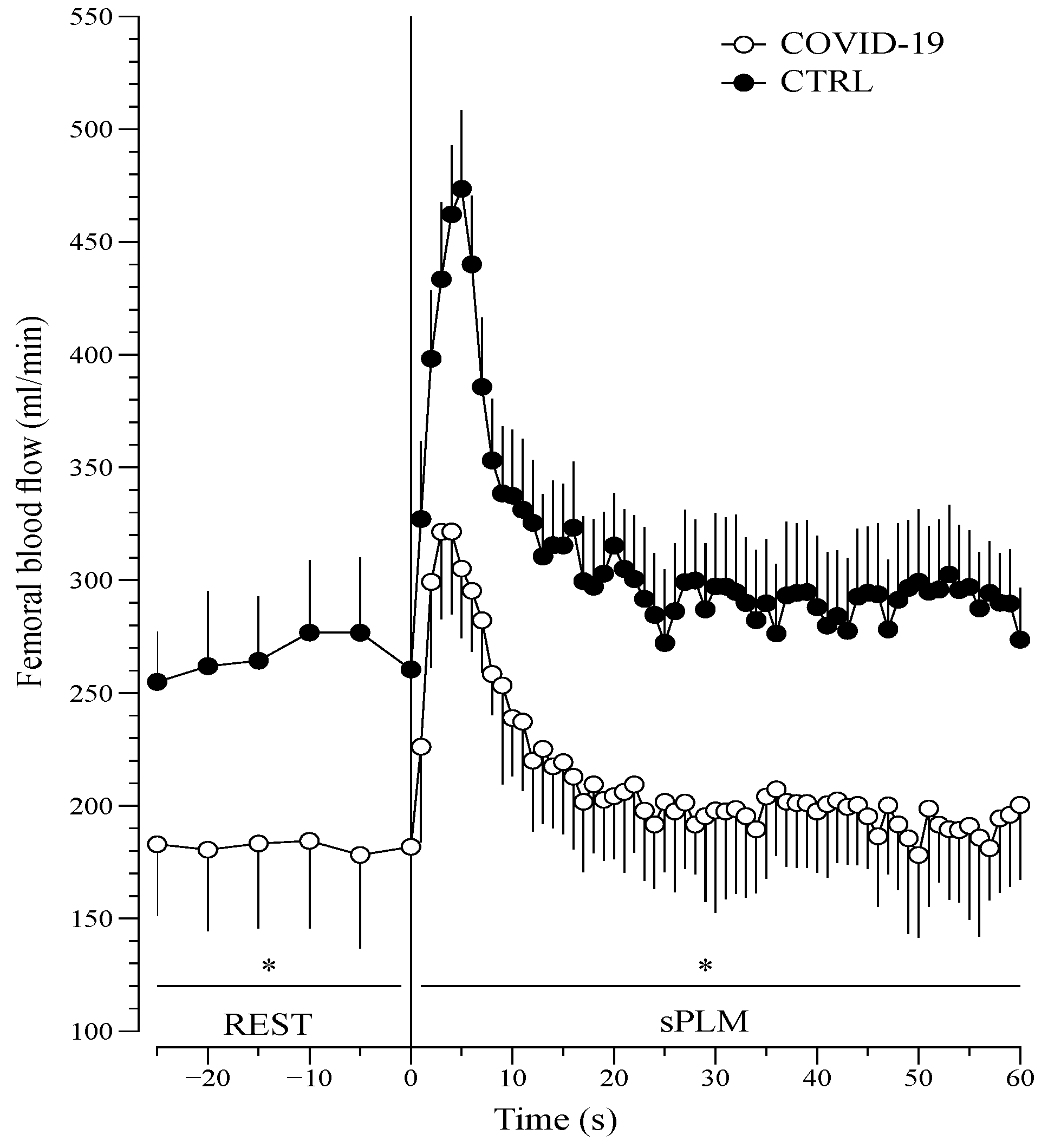
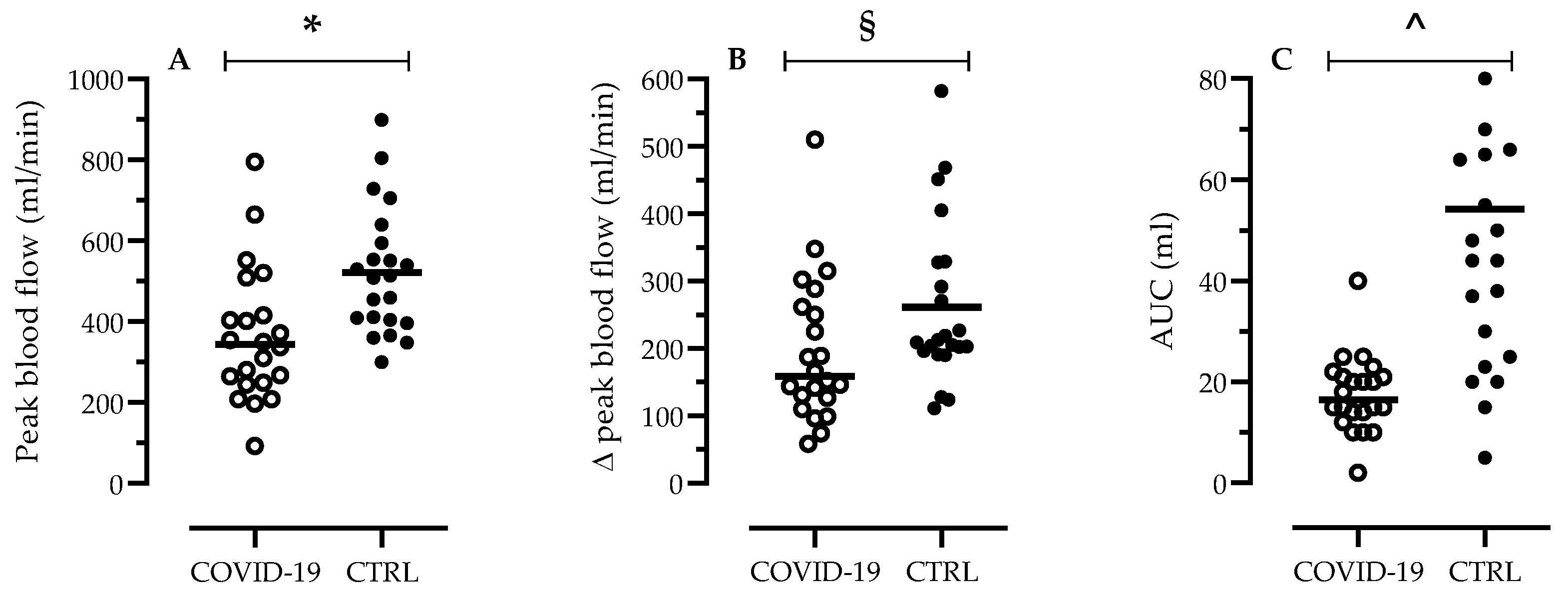
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The origins of viral infection sleuth. Cell 2021, 184, 1960–1961. [CrossRef] [PubMed]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamming, I.; Timens, W.; Bulthuis, M.; Lely, A.; Navis, G.; Van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–6379. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endothelitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Cui, S.; Chen, S.; Li, X. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef]
- Llitjos, J.F.; Leclerc, M.; Chochois, C. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Al-Ani, F.; Chehade, S.; Lazo-Langner, A. Thrombosis risk associated with COVID-19 infection. A scoping review. Thromb. Res. 2020, 192, 152–160. [Google Scholar] [CrossRef]
- Evans, P.C.; Rainger, G.E.; Mason, J.C.; Guzik, T.J.; Osto, E.; Stamataki, Z.; Neil, D.; Hoefer, I.E.; Fragiadaki, M.; Waltenberger, J.; et al. Endothelial dysfunction in COVID-19: A position paper of the ESC Working Group for Atherosclerosis and Vascular Biology, and the ESC Council of Basic Cardiovascular Science. Cardiovasc. Res. 2020, 116, 2177–2184. [Google Scholar] [CrossRef]
- Broxterman, R.M.; Trinity, J.D.; Gifford, J.R.; Kwon, O.S.; Kithas, A.C.; Hydren, J.R.; Nelson, A.D.; Morgan, D.E.; Jessop, J.E.; Bledsoe, A.D.; et al. Single passive leg movement assessment of vascular function: Contribution of nitric oxide. J. Appl. Physiol. 2017, 123, 1468–1476. [Google Scholar] [CrossRef]
- Ratchford, S.M.; Stickford, J.L.; Province, V.M.; Stute, N.; Augenreich, M.A.; Koontz, L.K.; Bobo, L.K.; Stickford, A.S.L. Vascular alterations among young adults with SARS-CoV-2. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H404–H410. [Google Scholar] [CrossRef]
- Salvi, F.; Miller, M.D.; Grilli, A.; Giorgi, R.; Towers, A.L.; Morichi, V.; Spazzafumo, L.; Mancinelli, L.; Espinosa, E.; Rappelli, A.; et al. A manual of guidelines to score the modified cumulative illness rating scale and its validation in acute hospitalized elderly patients. J. Am. Geriatr. Soc. 2008, 56, 1926–1931. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. ATS/ERS Task Force. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. ERS Global Lung Function Initiative. Multi-ethnic reference values for spirometry for the 3-95-yr age range: The global lung function 2012 equations.Multi-ethnic reference values for spirometry for the 3–95 years age range: The global lung function 2012 equations. Report of the Global Lung Function Initiative (GLI), ERS Task Force to establish improved Lung Function Reference Values. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar]
- Venturelli, M.; Layec, G.; Trinity, J.; Hart, C.R.; Broxterman, R.M.; Richardson, R.S. Single passive leg movement-induced hyperemia: A simple vascular function assessment without a chronotropic response. J. Appl. Physiol. 2017, 122, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Bergland, A.; Strand, B.H. Norwegian reference values for the Short Physical Performance Battery (SPPB): The Tromsø Study. BMC Geriatr. 2019, 19, 216. [Google Scholar] [CrossRef] [Green Version]
- Casanova, C.; Celli, B.R.; Barria, P.; Casas, A.; Cote, C.; de Torres, J.P.; Jardim, J.; Lopez, M.V.; Marin, J.M.; Montes de Oca, M.; et al. Six Minute Walk Distance Project (ALAT). The 6-min walk distance in healthy subjects: Reference standards from seven countries. Eur. Respir. J. 2011, 37, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Amraei, R.; Rahimi, N. COVID-19, Renin-Angiotensin System and Endothelial Dysfunction. Cells 2020, 9, 1652. [Google Scholar] [CrossRef] [PubMed]
- Godo, S.; Shimokawa, H. Endothelial Functions. Arter. Thromb. Vasc. Biol. 2017, 37, e108–e114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pober, J.S.; Sessa, W.C. Evolving functions of endothelial cells in inflammation. Nat. Rev. Immunol. 2007, 7, 803–815. [Google Scholar] [CrossRef]
- Opitz, B.; Eitel, J.; Meixenberger, K.; Suttorp, N. Role of Toll-like receptors, NOD-like receptors and RIG-I-like receptors in endothelial cells and systemic infections. Thromb. Haemost. 2009, 102, 1103–1109. [Google Scholar]
- Blasius, A.L.; Beutler, B. Intracellular toll-like receptors. Immunity 2010, 32, 305–315. [Google Scholar] [CrossRef] [Green Version]
- Shenoy, S. Coronavirus (Covid-19) sepsis: Revisiting mitochondrial dysfunction in pathogenesis, aging, inflammation, and mortality. Inflamm. Res. 2020, 69, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Wenham, C.; Smith, J.; Morgan, R. Gender and COVID-19 Working Group. COVID-19: The gendered impacts of the outbreak. Lancet 2020, 395, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Tang, N.; Li, D.; Wang, X. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedrinolla, A.; Colosio, A.L.; Magliozzi, R.; Danese, E.; Kirmizi, E.; Rossi, S.; Pogliaghi, S.; Calabrese, M.; Gelati, M.; Muti, E.; et al. The Vascular Side of Chronic Bed Rest: When a Therapeutic Approach Becomes Deleterious. J. Clin. Med. 2020, 9, 918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossman, M.J.; Kaplon, R.E.; Hill, S.D.; McNamara, M.N.; Santos-Parker, J.R.; Pierce, G.L.; Seals, D.R.; Donato, A.J. Endothelial cell senescence with aging in healthy humans: Prevention by habitual exercise and relation to vascular endothelial function. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, H890–H895. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: A prospective study. Lancet Respir. Med. 2021. [Google Scholar] [CrossRef]
- Cardozo, G.G.; Lopes, K.G.; Bottino, D.A.; Souza, M.D.G.C.; Bouskela, E.; Farinatti, P.; Brandão de Oliveira, R. Acute effects of physical exercise with different levels of blood flow restriction on vascular reactivity and biomarkers of muscle hypertrophy, endothelial function and oxidative stress in young and elderly subjects—A randomized controlled protocol. Contemp. Clin. Trials Commun. 2021, 22, 100740. [Google Scholar] [CrossRef] [PubMed]
- Pedrinolla, A.; Magliozzi, R.; Colosio, A.L.; Danese, E.; Gelati, M.; Rossi, S.; Pogliaghi, S.; Calabrese, M.; Muti, E.; Cè, E.; et al. Repeated passive mobilization to stimulate vascular function in individuals of advanced age who are chronically bedridden. A randomized controlled trial. J. Gerontol. Ser. A 2021, glab148. [Google Scholar] [CrossRef] [PubMed]
- Corrao, S.; Mallaci Bocchio, R.; Lo Monaco, M.; Natoli, G.; Cavezzi, A.; Troiani, E.; Argano, C. Does Evidence Exist to Blunt Inflammatory Response by Nutraceutical Supplementation during COVID-19 Pandemic? An Overview of Systematic Reviews of Vitamin D, Vitamin C, Melatonin, and Zinc. Nutrients 2021, 13, 1261. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.K.; Freemantle, N.; Breuer, J.; Dehbi, H.M.; Chowdhury, K.; Jones, G.; Ikeji, F.; Ndoutoumou, A.; Santhirakumar, K.; Longley, N.; et al. Early antiviral treatment in outpatients with COVID-19 (FLARE): A structured summary of a study protocol for a randomised controlled trial. Trials 2021, 22, 193. [Google Scholar] [CrossRef] [PubMed]
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Vahedian-Azimi, A.; Mohammadi, S.M.; Heidari Beni, F.; Banach, M.; Guest, P.C.; Jamialahmadi, T.; Sahebkar, A. Improved COVID-19 ICU admission and mortality outcomes following treatment with statins: A systematic review and meta-analysis. Arch. Med. Sci. 2021, 17, 579–595. [Google Scholar] [CrossRef]
- Trinity, J.D.; Kwon, O.S.; Broxterman, R.M.; Gifford, J.R.; Kithas, A.C.; Hydren, J.R.; Jarrett, C.L.; Shields, K.L.; Bisconti, A.V.; Park, S.H.; et al. The role of the endothelium in the hyperemic response to passive leg movement: Looking beyond nitric oxide. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H668–H678. [Google Scholar] [CrossRef] [PubMed]
- Trinity, J.D.; Craig, J.C.; Fermoyle, C.C.; McKenzie, A.I.; Lewis, M.T.; Park, S.H.; Rondina, M.T.; Richardson, R.S. Impact of Presymptomatic COVID-19 on Vascular and Skeletal Muscle Function: A Case Study. J. Appl. Physiol. 2021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| COVID-19 Patients (n = 22) | CTRL (n = 22) | p | |
|---|---|---|---|
| Age, years | 72.6 ± 8.7 | 72.5 ± 8.5 | 0.9694 |
| Sex, male% | 72.7 | 68.2 | 0.7436 |
| BMI, Kg/m2 | 24.7 ± 3.3 | 24.6 ± 1.8 | 0.9013 |
| Barthel index, score | 76.6 ± 25.7 | 98.1 ± 3.7 | 0.0004 |
| 6-MWT, meters | 195.4 ± 117.1 | 545 ± 135.5 | <0.001 |
| SPPB, score | 5.8 ± 3.7 | 10.7 ± 0.6 | <0.001 |
| Comorbidities, % | |||
| Hypertension | 57 | 56 | 0.9467 |
| Diabetes | 19 | 30 | 0.3963 |
| Heart failure | 26 | 19 | 0.5782 |
| Ischemic Heart Disease | 17 | 10 | 0.4969 |
| Pulmonary Chronic Disease | 39 | 28 | 0.4395 |
| CIRS1, score | 2.2 ± 0.6 | ||
| CIRS2, score | 5.8 ± 3.1 | ||
| PaO2, mmHg | 61.2 ± 8.5 | Normal value: >85 mmHg | |
| PaCO2, mmHg | 42.3 ± 3.6 | Normal value: 37–43 mmHg | |
| pH | 7.43 ±0.01 | Normal value: 7.37–7.44 | |
| FEV1, % | 71 ± 23 | Normal value: >80% | |
| FVC, % | 63 ± 23 | Normal value: 80–120% | |
| FEV1/FVC | 89 ± 10 | Normal value: 80 | |
| CRP, mg/dl | 27.13 ± 37.52 | Normal Value: ≤5 mg/L | |
| ESR, mm/h | 64.24 ± 32.37 | Normal value: W ≤ 30 mm/h M ≤ 20 mm/h | |
| 47.33 ± 25.06 | |||
| 73.45 ± 30.65 | |||
| D-dimer, ng/ml | 1043 ± 729 | Normal value: ≤300 ng/mL | |
| Clinical History, % | |||
| Mechanical ventilation use | 41 | ||
| Oxygen | 100 | ||
| Embolism | 23 | ||
| Pneumothorax | 23 | ||
| Drugs, % | |||
| Anti-rheumatic | 5 | ||
| Cortisone | 30 | ||
| Anti-malarial | 35 | ||
| Anti-viral | 25 | ||
| Anti-platelet | 53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paneroni, M.; Pasini, E.; Vitacca, M.; Scalvini, S.; Comini, L.; Pedrinolla, A.; Venturelli, M. Altered Vascular Endothelium-Dependent Responsiveness in Frail Elderly Patients Recovering from COVID-19 Pneumonia: Preliminary Evidence. J. Clin. Med. 2021, 10, 2558. https://doi.org/10.3390/jcm10122558
Paneroni M, Pasini E, Vitacca M, Scalvini S, Comini L, Pedrinolla A, Venturelli M. Altered Vascular Endothelium-Dependent Responsiveness in Frail Elderly Patients Recovering from COVID-19 Pneumonia: Preliminary Evidence. Journal of Clinical Medicine. 2021; 10(12):2558. https://doi.org/10.3390/jcm10122558
Chicago/Turabian StylePaneroni, Mara, Evasio Pasini, Michele Vitacca, Simonetta Scalvini, Laura Comini, Anna Pedrinolla, and Massimo Venturelli. 2021. "Altered Vascular Endothelium-Dependent Responsiveness in Frail Elderly Patients Recovering from COVID-19 Pneumonia: Preliminary Evidence" Journal of Clinical Medicine 10, no. 12: 2558. https://doi.org/10.3390/jcm10122558