Article Text

Abstract
Objective To assess the SARS-CoV-2 transmission in healthcare workers (HCWs) using seroprevalence as a surrogate marker of infection in our tertiary care centre according to exposure.
Design Seroprevalence cross-sectional study.
Setting Single centre at the end of the first COVID-19 wave in Lausanne, Switzerland.
Participants 1874 of 4074 responders randomly selected (46% response rate), stratified by work category among the 13 474 (13.9%) HCWs.
Main outcome measures Evaluation of SARS-CoV-2 serostatus paired with a questionnaire of SARS-CoV-2 acquisition risk factors internal and external to the workplace.
Results The overall SARS-CoV-2 seroprevalence rate among HCWs was 10.0% (95% CI 8.7% to 11.5%). HCWs with daily patient contact did not experience increased rates of seropositivity relative to those without (10.3% vs 9.6%, respectively, p=0.64). HCWs with direct contact with patients with COVID-19 or working in COVID-19 units did not experience increased seropositivity rates relative to their counterparts (10.4% vs 9.8%, p=0.69 and 10.6% vs 9.9%, p=0.69, respectively). However, specific locations of contact with patients irrespective of COVID-19 status—in patient rooms or reception areas—did correlate with increased rates of seropositivity (11.9% vs 7.5%, p=0.019 and 14.3% vs 9.2%, p=0.025, respectively). In contrast, HCWs with a suspected or proven SARS-CoV-2-infected household contact had significantly higher seropositivity rates than those without such contacts (19.0% vs 8.7%, p<0.001 and 42.1% vs 9.4%, p<0.001, respectively). Finally, consistent use of a mask on public transportation correlated with decreased seroprevalence (5.3% for mask users vs 11.2% for intermittent or no mask use, p=0.030).
Conclusions The overall seroprevalence was 10% without significant differences in seroprevalence between HCWs exposed to patients with COVID-19 and HCWs not exposed. This suggests that, once fully in place, protective measures limited SARS-CoV-2 occupational acquisition within the hospital environment. SARS-CoV-2 seroconversion among HCWs was associated primarily with community risk factors, particularly household transmission.
- occupational & industrial medicine
- virology
- epidemiology
- preventive medicine
- COVID-19
- infection control
Data availability statement
Data are available upon reasonable request. The data related to this study can be requested at CHUV to Dr Sylvain Meylan (Sylvain.Meylan@chuv.ch). Such transfer is submitted to the Human Research and the Data Protection Swiss Legislation and, accordingly, to the signature of a Data Sharing and User Agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Large population study randomly selected, stratified by work category covering all workers of our institution.
Ideal sampling period concentrated over 4 weeks at the very end of the first COVID-19 wave in our region, optimising the likelihood of capturing true seropositive individuals.
Use of a particularly sensitive and specific technology to quantify the trimeric form of the S-protein IgG.
This study is limited by the self-administered nature of the questionnaire as main outcomes, potentially fraught with reporting bias.
Introduction
Infection on the frontline of the COVID-19 pandemic is a major concern for healthcare workers (HCWs). Significant challenges to their safeguarding have included sudden and unpredictable surges in COVID-19 case volumes, potential shortages of personal protective equipment (PPE) and ongoing uncertainty about optimal protective approaches.1–5 In particular, the role of aerosols in SARS-CoV-2 transmission remains a matter of debate.6 7 Importantly, as hospital-associated protective measures are unlikely to impact infection risk to HCWs via community spread, it is important to discriminate likely sources of infection when making an assessment of measures designed to reduce intrahospital SARS-CoV-2 transmission.
Seroprevalence studies as a proxy of the risk of infection have identified seroprevalence rates ranging from 6.4% to 13.7% in HCWs.8–12 However, they were limited by several factors. First, as they were generally conducted during the first wave of the COVID-19 pandemic, the fraction of participants sampled who might later seroconvert was unknown. Second, the institutional measures taken to protect HCWs from infection within the hospital environment were not assessed. Third, they usually did not evaluate well the community exposition. A meta-analysis identified COVID-19-dedicated units and the lack of mask usages as main risk factors.12
In response to the SARS-CoV-2 pandemic, our tertiary care university medical centre, a 1531-bed hospital with a partner outpatient centre, took a series of preventive measures. Infections among HCWs were initially assessed via direct SARS-CoV-2 PCR from nasopharyngeal swabs in symptomatic individuals. Three hundred and twenty-two PCR-positive cases were identified between March and late May 2020. However, as the testing was initially restricted to symptomatic workers having direct contact with patients, or having personal vulnerability factors, or having recently travelled in a high-risk zone, the incidence of SARS-CoV-2 infection among HCWs at the institutional level remains unknown. The aims of our study were to (1) evaluate the SARS-CoV-2 seroprevalence among HCWs at the end of the first wave, (2) identify potential groups with increased infection rate by comparing serostatus of HCWs exposed to patients with COVID-19 with their unexposed counterparts, and (3) identify potential sources of infection within and outside the professional environment.
Methods
Study design, setting and participants
This was a single-centre seroprevalence study conducted at the tertiary care university centre in Lausanne, Switzerland, (thereafter the Centre) comprising the Centre Hospitalier Universitaire Vaudois (CHUV), a 1531-bed hospital, and the Centre for Primary Care and Public Health (Unisanté), serving the city of Lausanne and as a reference centre for the Canton of Vaud, an area of 799 145 inhabitants.
Participants were randomly selected, stratified by work category from the human resources database (see online supplemental methods). We aimed to assess approximately 15% of the 13 474 HCWs of the Centre, which would yield adequate representation of each work category. Selected participants were contacted by email or by postal mail if an email address was not available. Contacted HCWs had 48 hours to confirm participation. The overall response rate was 46%. Three rounds of recruitment were used to reach the target sample size of each work category, resulting in a total of 1874 participants (online supplemental table 1 and figure 1; see also online supplemental methods). Exclusion criteria were age under 18 years, symptoms within the 14 days prior to sampling (corresponding to the median time-window of seroconversion13 and participation in an alternative serological population study in the Canton of Vaud (SerocoViD). All participants provided informed consent via the e-form of the questionnaire and a formal written informed consent prior to serum sampling. Questionnaires and blood samples were collected between 18 May and 12 June 2020.
Supplemental material
Supplemental material
Patient and public involvement
Participants were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Questionnaire
In order to characterise SARS-CoV-2 exposure risk factors, an online questionnaire (see online supplemental questionnaire/survey) was designed according to PEW Research Center guidelines to assess demographic data, travel history outside Switzerland between 1 January and 17 March 2020 (date of closure of Switzerland borders), history of COVID-19, personal and professional risk factors and use of protective measures, prior symptoms consistent with COVID-19,14 prior nasopharyngeal SARS-CoV-2 tests with date and result, and COVID-19-related hospitalisations (including intensive care unit). The questionnaire was tested with pilot groups representing the main professions within the HCWs (administration, logistics, nurses, physicians) before being sent to participants.
Supplemental material
Serological assay
Serum samples were analysed for SARS-CoV-2 serology (IgG), using a previously described Luminex-based assay quantifying antibody binding to the trimeric form of the SARS-CoV-2 S-protein.15 This assay has shown a sensitivity and specificity of 97% and 98%, respectively, on hospitalised patients for the chosen cut-off of positivity defined at a ratio >5.90.15
PCR results
Aggregate PCR results of tests performed from 9 March to 9 May were extracted from occupational health records. Tests results reported in the questionnaire but performed outside the institution were also collected. In March, testing was limited to symptomatic HCWs who had personal vulnerability factors, direct contact with patients or contact with a laboratory-confirmed SARS-CoV-2 case, or recent travel in a high-risk area. As of 8 April, anosmia and/or ageusia were added to the list of the symptoms suggestive of COVID-19. On 19 April, PCR tests were extended to all symptomatic persons, irrespective of other criteria. PCR was performed according to standard protocols.16
COVID-19 preventive measures
Setting
The Centre opened several units dedicated to COVID-19 care. On 6 March, a dedicated outpatient COVID-19 screening unit with unidirectional patient flow was established. On 13 March, dedicated inpatient COVID-19 units for intensive, continuous and standard care were created. Remote work was established for non-essential staff.
Personnel protective equipment
Starting 20 January 2020, the Centre implemented preventive measures for patients with suspected or confirmed infection with SARS-CoV-2, based on historical recommendations for SARS-CoV-1: patients were placed in individual rooms with negative pressure, and contact and airborne transmission precautions were applied. PPE included an FFP2/N95 respirator mask, single-use gown, gloves and protective goggles. On 10 March, FFP2/N95 mask was substituted for surgical mask (contact and droplet transmission precautions), except for aerosol-generating procedures (nasopharyngeal swabbing, intubation, bronchoscopy, non-invasive ventilation, cardiopulmonary resuscitation, laryngoscopy, open system suction and high-flow ventilation). The quality of the FFP2/N95 masks was tested to ensure adequate filtration (laboratory test) and fit check. On 17 March, surgical masks became mandatory for all HCWs in close contact with patients and hand hygiene was reinforced. Pregnant employees, trainees, temporary workers or employees belonging to the group of vulnerable populations for COVID-19 according to the Federal Office of Public Health were not allowed to take part in the care of patients with suspected/confirmed COVID-19. Coaching of HCWs by the infection control team on hand hygiene and adequate use of PPE was implemented in COVID-19 units. On 8 April 2020, surgical masks became mandatory at work for all HCWs including those without patient contact.
Air management
In the outpatient screening facility, the air management included five cycles of air renewal per hour with 30% of fresh air and negative pressure (5–15 Pa). Air was recycled through H14 filters. In the main building, air processing was set to achieve three to five renewals per hour of fresh air only (F7–F9 filters) throughout the main building, and equipressure—or negative pressure where achievable—was implemented as of 13 March. On dedicated COVID-19 units, smoke tests were repeatedly performed to rule out overpressure of patients’ rooms.
Surface disinfection and waste management
Rooms with patients with suspected or confirmed COVID-19 were cleaned and disinfected on a daily basis with a product containing glucoprotamine at a final concentration of 0.5%. Surfaces (lavatories, beds, nightstands) were disinfected daily or more often if needed. Waste elimination followed regular protocols.
National and cantonal measures
The Swiss federal government declared a nationwide lockdown on 16 March 2020. All schools, restaurants and non-essential retail stores were closed. Gatherings of all sorts were massively reduced or forbidden. All non-urgent medical consultations or surgeries were postponed until 1 May 2020. The lockdown was loosened on 29 April. Wearing a mask on public transport was recommended as of 30 April 2020 and made mandatory on 6 July 2020 by the Swiss government.
Statistical analyses
The primary analysis of estimated COVID-19 seroprevalence was performed based on the random sample cohort, unweighted as well as weighted according to the work category. Point estimates of the seropositivity along with corresponding 95% exact binomial CI (95% CI) were provided overall, as well as by institution and work category. Prespecified subgroup analyses by demographic factors and work conditions were performed comparing the prevalence in subgroups of epidemiological factors of interest based on Fisher’s exact test as well as on Cochran-Mantel-Haenszel test stratified by the work category, while Breslow test was used for exploring homogeneity. Multivariable logistic regression model was applied to explore the effect of several epidemiological risk factors on seropositivity (demographics: age, gender and smoking; living region, household contacts, travel outside Switzerland, confirmed or suspected COVID-19 case at home, frequency and duration of using public transport, use of mask in public transportation; working conditions: work category, hospital domain, teleworking, full-time or part-time work rate, daily contact with patients and type of contact, direct contact with patient with COVID-19, work in COVID-19 unit and type of unit, use of hydroalcoholic solution at work; symptoms suggestive of COVID-19), taking into account the work category. In the multivariable model, the effect of the several risk factors (as specified above) was jointly examined. The factors with significant effect were chosen via the backward elimination method (removal criterion p>10%). Multicollinearity among factors was checked through tolerance and variance inflation factor. For each factor, OR, for seropositivity versus non-seropositivity, and corresponding 95% CI were derived from the corresponding logistic regression model. All statistical results were produced using SAS V.9.4 and all reported p values are two-sided and considered significant as significance level 5%. No adjustment for multiple comparisons was performed.
Results
Epidemiological context of the initial COVID-19 wave at the national, local and institutional levels
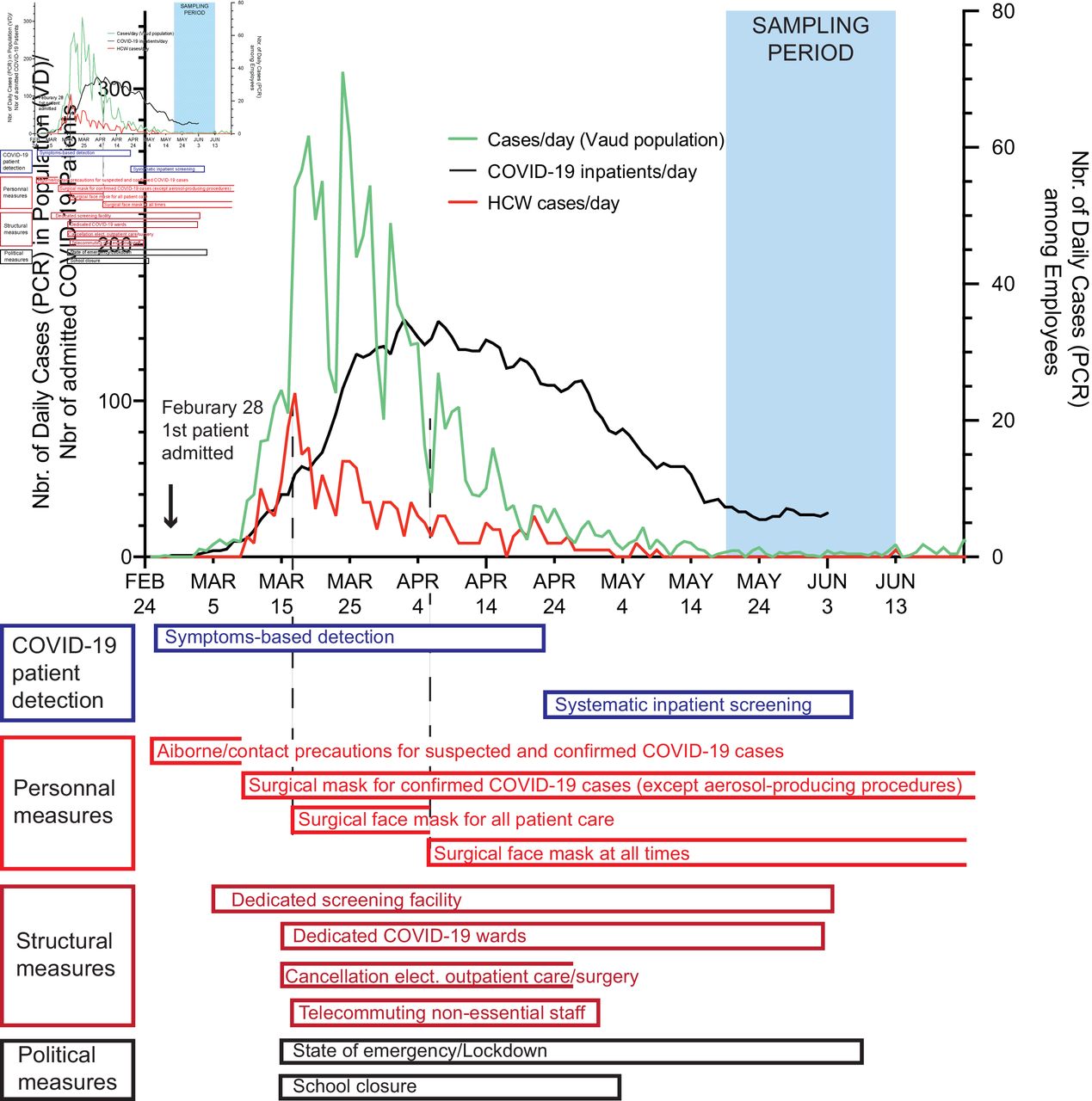
The initial COVID-19 wave started in late February 2020 in Switzerland and the first case in the Lausanne area was documented on 7 March. By 23 March, documented COVID-19 cases peaked in the area with an incidence of 38.6/100 000 daily cases, as assessed by SARS-CoV-2 PCR (figure 1).17 From 9 March until 9 May, 322 PCR-confirmed cases were documented among HCWs. However, HCW cases peaked earlier on 16 March with 24 cases and declined thereafter despite a continuous increase of COVID-19 hospitalised patients until 7 April, with a peak of 153 patients on that date.
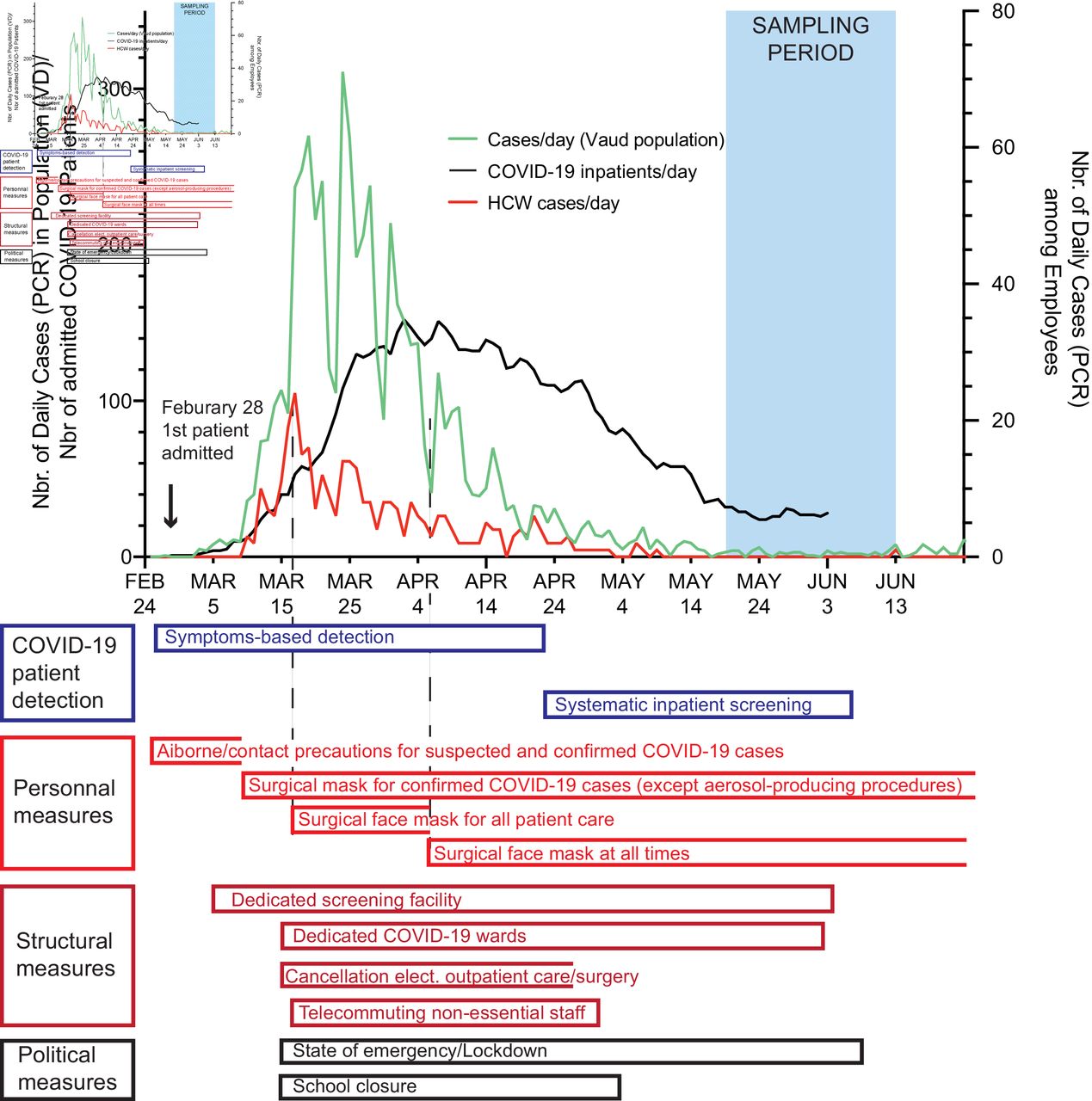
Epidemiological context of the serological evaluation at our tertiary care university centre. The timeline of the first wave is plotted against time (x axis) with cases as diagnosed by nasopharyngeal swab-based PCR in Vaud state (VD—green) admitted patients with COVID-19 (black line) on the left y axis and among healthcare workers of our tertiary care university centre (Inst—red) on the right y axis. The serological sampling is time zero is defined as 24 February, date of the first documented Swiss case. Institutional, state and national measures are plotted according to their timing (aligned on the graph’s x axis).
Study population
A total of 1888 of 4074 HCWs randomly selected (46% response rate), stratified by work categories among the total 13 474 (13.9%) HCWs (online supplemental table 1) were enrolled between 18 May and 12 June 2020. Fourteen participants were excluded: 12 due to symptoms consistent with COVID-19 in the 14 days prior to serum sampling, 1 due to a missing informed consent and 1 because of an invalid serum sample. Basic demographic characteristics by the stratification factor of work categories are summarised in online supplemental table 2. During this period, new daily COVID-19 cases remained below 1.0/100 000 in our area (figure 1). The average incidence among HCWs was below one case per day.
Prevalence of seropositivity for anti-SARS-CoV-2 IgG antibodies
Of the 1874 HCWs included, 188 (10.0%; 95% CI (8.7% to 11.5%)) tested seropositive for SARS-CoV-2. Stratified seroprevalence is described in table 1, with non-statistically significant variations by work category (p=0.074). There was no statistically significant difference according to sex (male seropositivity 9.6% vs female 10.3%, p=0.68) or age (11.0% for HCWs up to 40 years of age vs 9.1% for HCWs above 40 years, p=0.17), or other demographic characteristics (online supplemental table 3) .
COVID-19 seropositivity according to work category
Risk factors for seropositivity
Daily exposure to patients (irrespective of their SARS-CoV-2 status) did not correlate with increased seropositivity of HCWs (patient exposed 10.3% vs patient non-exposed 9.6%, p=0.64). Seroprevalence did not differ among hospital domains, including potentially highly exposed areas such as intensive care and emergency department (table 2). Furthermore, seroprevalence was not significantly higher among HCWs who had direct contact with patients with confirmed COVID-19 compared with those who did not (10.4% vs 9.8%, p=0.69). Similarly, seroprevalence of COVID-19-unit HCWs was not statistically different compared with their non-COVID-19-unit counterparts (10.6% vs 9.9%, p=0.69) irrespective of work category or COVID-19 unit type (table 3).
Seropositivity according to domains
COVID-19 seropositivity, work conditions and exposure to patients with COVID-19
However, among HCWs who had daily contact with patients, seroprevalence was significantly higher among those working in the rooms of patients on general wards as well as in reception areas compared with HCWs with patient contact in other areas (11.9% vs 7.5%, p=0.019 and 14.3% vs 9.2%, p=0.025) (online supplemental table 3). The impact of work in patients’ rooms was also confirmed in multivariable analysis (OR=1.39; 95% CI (1 to 1.94), p=0.05; online supplemental figure 2). A trend towards higher seroprevalence was also observed among HCWs exposed to patients in intervention rooms (intubation or endoscopic procedures) or waiting rooms (13.6% vs 9.6%, p=0.095 and 13.2% vs 9.4%, p=0.071, respectively; OR=1.64, p=0.053 and OR=1.78, p=0.013, respectively, in multivariable analyses; online supplemental figure 2). In contrast, exposure in outpatient examination rooms was not associated with higher HCWs seroprevalence in univariate analysis (9.5% vs 10.9%, p=0.49), but when examined jointly with all other factors in the multivariable logistic model, a significant effect was detected with OR=0.62, p=0.026 (online supplemental figure 2). Defects in reported PPE problems did not correlate with increased seropositivity (online supplemental table 4).
No significant differences were identified between HCWs who transferred to remote work compared with those who did not (9.4% vs 10.4%, p=0.48), although trend towards decreased seropositivity rates was associated with increased percentage of remote work activity (online supplemental table 5). Similarly, HCWs reallocated to COVID-19 units did not show a higher seroprevalence compared with other HCWs (9.3% vs 10.1%, p=0.73) (online supplemental table 5).
The presence of a suspected or confirmed COVID-19 case among household contacts was significantly linked to seropositive status (19.0% vs 8.7%, p<0.001 and 42.1% vs 9.4%, p<0.001, respectively; online supplemental table 6). In the multivariable logistic regression analysis, the likelihood of a seropositive result was more than doubled by a housemate with suspected or confirmed COVID-19 (OR=2.21, p<0.0001 and OR=2.87, p<0.0001, respectively; online supplemental figure 2). In contrast, having household contacts irrespective of COVID-19 status did not correlate with seropositivity (other persons in household 10.2% vs no other persons in household 9.1%, p=0.60; online supplemental table 6).
The impact of travel and commuting on SARS-CoV-2 serostatus among HCWs was also examined. In total, 837 HCWs reported having travelled outside of Switzerland between January and mid-March. Travel to Asia or neighbouring countries (France, Italy or Germany; online supplemental table 7) did not correlate with increased seroprevalence compared with non-travelling controls (9.3% vs 10.6%, p=0.40). We also interrogated the impact of commuting as a potential source of exposure. A trend was observed between frequency of public transportation use and seroprevalence, except in case of use of more than five times per week of public transportation (table 4). Furthermore, reported mask adherence while commuting was associated with a statistically significant lower seropositivity rate (mask at all times 5.3% vs no mask/occasional mask usage 11.2%, p=0.030), and reduced the odds of seropositivity by 58% (OR=0.42, p=0.025) in multivariable analysis (online supplemental figure 2).
COVID-19 seropositivity according to public transportation use
We further looked at the trainees/apprentices/students because of their increased seroprevalence. Only 6 of the 55 worked in a COVID-19 unit and 20 of the 55 had contact with patients. Seroprevalence was higher in those without contact (23.3% vs 16%). In contrast, 13 reported a suspected (11) or a confirmed (2) COVID-19 case within their household. Moreover, 42 of the 55 commuted on a regular basis but only 1 consistently used a mask on that occasion.
Symptomatology/PCR testing and seropositivity
Of the 188 HCWs who tested seropositive, 118 (63%) reported symptoms or signs compatible with SARS-CoV-2 infection (table 5). Only six (3%) HCWs reported being hospitalised and none required intensive care. Seventy seropositive HCWs (37%) reported no symptoms, consistent with rates of asymptomatic COVID-19 reported previously.10 18 Symptoms most strongly correlating with SARS-CoV-2 positive serology were fever, myalgia and sore throat, as well as dysgeusia and anosmia (all p<0.01, online supplemental table 8).6 14 In total, 708 out of the 1874 HCWs (37.8%) reported symptoms consistent with COVID-19, of which 118 (16.7%) were seropositive (as expected, high significant association in univariate analysis, table 5; and in multivariable logistic model with OR=2.87, p<0.0001, online supplemental figure 2). For both seropositive and seronegative HCWs, the symptoms occurred primarily in the first month of the outbreak (figure 2). Finally, among the 708 participants with symptoms, 52 of the 54 who had prior PCR-positive test had a positive serology, resulting in an observed sensitivity of 96.3%. Conversely, among the 233 participants with a negative PCR test, 13 had a positive serology, and assuming they did not become infected in the meantime the specificity would be 94.4% (table 5).
Association between COVID-19 seropositivity and presence of symptoms of infection and results of PCR

{kind=link}
{kind=link}
Timing of symptoms in healthcare workers (HCWs) according to SARS-CoV-2 serological status. Number of HCWs experiencing symptoms consistent with COVID-19 (see Methods section) plotted against time (2-week intervals). The patient groups are segregated according to SARS-CoV-2 serostatus (white seronegative, red seropositive).
Discussion
We report an average seroprevalence for SARS-CoV-2 in HCWs of 10% at the end of the first COVID-19 wave, without statistically significant variations according to work category or hospital department. Direct contact with patients did not correlate with increased seropositivity though specific contacts with patients in inpatient rooms and in waiting rooms did. Daily contact with patients with COVID-19 as well as work on COVID-19 units was not found to increase seroprevalence. Considering the timeline of COVID-19 infection in HCWs as documented by PCR and the progressive rollout of protective measures, these findings argue in favour of limited intrahospital transmission, particularly in high-risk areas such as COVID-19 units. Early transmission sites for unrecognised or asymptomatic patients or coworkers in particular at-risk areas may have accounted for early intrahospital infections. Conversely, a strong correlation between infection or suspected infection in the household and seroprevalence argues in favour of a community acquisition.
Strengths and weaknesses of the study
We present a detailed analysis of the efficacy of preventive measures taken to prevent SARS-CoV-2 transmission among HCWs strengthened by a large and well-balanced study sample and a particularly favourable epidemiological context: (1) after the first wave of the COVID-19 outbreak, (2) in a high incidence region and (3) when minimal ongoing transmission was present.
On the other hand, our study has several limitations. First and foremost, as this is an observational study, association but not causality, can be established. Second, the use of a self-administered questionnaire as main outcomes (public transport, contact with suspected or confirmed COVID-19 cases at home, etc) is potentially fraught with reporting bias. Third, serology remains an imperfect surrogate marker for SARS-CoV-2 infection. Evidence suggests that the antibody response to SARS-CoV-2 infection may wane rapidly19 20 potentially leading to false negative findings in our sample. Long et al reported a 13% rate testing seronegative at 8 weeks, though the serological testing did not use the same method.20 We note that only 2 of 54 (3.7%) of our participants with previous positive PCR test for SARS-CoV-2 on nasopharyngeal swabs were seronegative, arguing against a consequent loss due to waning serological responses.
Comparison with other studies
The average SARS-CoV-2 seroprevalence of 10% is in the range of other studies in HCWs after the first wave.8–11 Importantly, seroprevalence was similar to the SerocoViD population study of the Canton of Vaud (Lausanne is the capital) at the same period: 8% in the general population (aged 20–65 years) and 12% in non-healthcare settings workers (personal communication VD’A). A comparable seroprevalence rate was also reported among the general population of the neighbouring Canton of Geneva (8%–11% seropositive), where COVID-19 incidence was similar.21 Within this regional context, infections rates were therefore not disproportionately higher among HCWs in the Centre, despite an increased exposure risk. Furthermore, the strongest correlation with seropositivity in our study was a confirmed case of COVID-19 among household contacts, which is consistent with other studies.9 22–25
The lack of difference in seroprevalence between HCWs exposed to patients with COVID-19 compared with those exposed to patients without COVID-19—including intensive care units where exposure was presumably highest—contrasts with recently published studies reporting increased seroprevalence among HCWs involved in direct patient care.12 26
Meaning of the study
Our results suggest that, once the bundle of measures aimed at limiting SARS-CoV-2 transmission was fully implemented, spread of the virus was limited among HCWs based on two lines of reasoning. First, the comparable seroprevalence with workers in non-healthcare companies argues against exacerbated SARS-CoV-2 infection rates in the hospital. Second, the lack of increased seropositivity among HCWs working in the COVID-19 units established in mid-March strongly argues against failures of the preventive measures implemented despite being less stringent than those enforced in other countries.27
However, direct contact with patients in patient rooms or waiting rooms correlating with seropositive status—and to a lesser extent the trend seen in intervention rooms—may suggest that atypical clinical presentations may have indeed been an Achilles’ heel at the beginning of the pandemic.1 28 29 A major challenge early on was a lack of knowledge about the breadth of clinical presentation of COVID-19.1 Initial preventive measures were designed based on SARS-CoV-1 and targeted clinically suspected or confirmed cases. However, a significant fraction of patients can be contagious prior to symptoms or asymptomatic but still be contagious.29–32 Contrary to other components of the anti-SARS-CoV-2 bundle, expanded surgical mask use for all patient care was not introduced until mid-March in our institution, and most of the SARS-CoV-2 infections among HCWs were documented prior to that point. Infection of HCWs early in the first wave due to undetected cases is likely (figure 1) and supported by timing of symptoms among symptomatic seropositive HCWs, when considering the incubation period (figure 2). The correlation of seropositivity with specific contact to patients in reception areas or in patients’ rooms but not with COVID-19-confirmed patients or work on COVID-19 units suggests that infections may have occurred early on via interactions with patients—or coworkers—with undetected SARS-CoV-2 infection. Wearing a surgical mask consistently on public transportation also correlated with decreased seroprevalence, highlighting the potential benefit of a surgical mask and the risk of transmission on public transport. Taken together, these observations support the use of a surgical mask as an important part of protection from SARS-CoV-2 infection.
The absence of a significant increase in infection among HCWs in contact with patients with COVID-19 is also interesting considering that mainly surgical masks were used for direct patient care, while FFP2/N95 mask usage was limited to high-exposure procedures such as intubation, nasopharyngeal swabbing or endoscopy. Indeed, indoor transmission by aerosols has been an increasing concern.2 33 The present study suggests that this mode of transmission is probably limited if ventilation fulfils some requirements for filtration and air exchanges. Regular audits from the infection control staff may also have increased adherence to the implementation of the anti-SARS-CoV-2 bundle. The abrupt decrease in the number of HCWs reporting symptoms at the end of March, both in seropositive and seronegative HCWs, likely reflects the impact of measures to contain viral transmission, with good adherence to infection control measures and nationwide lockdown.
Considering the limitations, this study reinforces the value of the protective measures implemented to prevent intrahospital transmission of SARS-CoV-2 to HCWs. It also reveals that comparatively simple measures, compared with those used elsewhere, can efficiently limit risk exposure in healthcare settings.27 Finally, our data support the assertion that consistent mask usage on public transportation may significantly reduce community spread of SARS-CoV-2.
Unanswered questions and future research
With our study design, we assessed the protection of HCWs. We did not, however, assess the protection of patients from nosocomial infections. Assessing whether protective measures also protect patients from asymptomatic HCWs becomes highly relevant as the second wave is impacting many countries in a more lasting way.
Data availability statement
Data are available upon reasonable request. The data related to this study can be requested at CHUV to Dr Sylvain Meylan (Sylvain.Meylan@chuv.ch). Such transfer is submitted to the Human Research and the Data Protection Swiss Legislation and, accordingly, to the signature of a Data Sharing and User Agreement.
Ethics statements
Acknowledgments
Our many thanks for helpful comments and suggestions to Patrick Francioli. We thank Sofia Tsouprou for helpful comments. We also thank COVID-19 MISS Hotline team: Magali Bilien, Elena Dall’Olio, Leana Gonzalez, Lisa Montagnese, Tatiana Pretre, Alexandra Risse, Jelena Saric, Elena Veselinovska; and Unisanté (Director Jacques Cornuz and Kevin Selby) for their help. Special thanks to our sponsors Philippe Eckert and Oliver Peters. Thanks to the head of nursing department Isabelle Lehn and her team for staffing support, head of human resources Antonio Racciatti and his team, head of constructions Catherine Borghini-Polier and her team for supplying resources and rooms for the study, as well as Gerald Golaz and his team for technical support. We also wish to thank Pierre Merminod for his assistance. Many thanks to the service of logistics for its assistance in shuttling the samples.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators COVID-19 MISS group: Occupational health unit: Michael Currat, Laurence Posset and the entire staff for ongoing outstanding work. Clinical Trial Unit Lausanne University and University Hospital: Fady Fares, Vassili Soumas. Investigator delegates. Investigator delegates: Séverine Bignon, Elisa Corne, Michael Currat, Joana Da Silva Quelhas, Allan Dussex, Dominique Ker, Patricia Mosset, Estelle Moulin, Eugénie Prouvost, Kyllian Ruscio, Sandrine Piccon and Fleur Valterio. Collection of blood samples: Emilie Allain, Charles Guay, Zahra Hezari, Yoann Levet, Laurence Posset, Marie-Agnès Prevost, Adeline Rognon, Homa Salehi-Gysel, Cécile Starck, Aurélie Tornier, Sara Torres da Fonseca and Aline Udriot.
Contributors SM, CL-B, GG, GP, OM and FL conceived the study. SM and CL-B drafted the first version of the manuscript. UD and ZT contributed to drafting sections of the manuscript. SM, CL-B, JR, VD’A and IG took part in data collection. ZT, UD, SM, IG and CL-B performed data analyses. CA, CF, AC and GP did lab analyses. UD, JR, AC, GG, GP and TC participated in the study design. SM, CL-B, FL, MAL, LS, BG and OM helped to draft the manuscript. All authors contributed to the interpretation of data and read and approved the final manuscript.
Funding The work was fully funded by the Lausanne University Hospital.
Disclaimer The CHUV sponsored this study but had no role in the study design, data collection, analysis and interpretation, or in writing of the manuscript. The corresponding author had full access to all data of the study and had final responsibility for the decision to submit for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.