 Anica Ilic1
Anica Ilic1 Katharina Roser1Grit Sommer2,3Julia Baenziger1,4,5Vera Ruth Mitter6,7
Katharina Roser1Grit Sommer2,3Julia Baenziger1,4,5Vera Ruth Mitter6,7 Luzius Mader8Daniela Dyntar1
Luzius Mader8Daniela Dyntar1 Gisela Michel1*
Gisela Michel1*- 1Department of Health Sciences and Medicine, University of Lucerne, Lucerne, Switzerland
- 2Department of BioMedical Research, University of Bern, Bern, Switzerland
- 3Pediatric Endocrinology, Diabetology and Metabolism, Department of Pediatrics, Bern University Hospital, University of Bern, Bern, Switzerland
- 4Center for Heart Disease and Mental Health, Heart Institute and Division of Behavioral Medicine and Clinical Psychology, Cincinnati Children’s Hospital and the Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, OH, United States
- 5Heart Centre for Children, Sydney Children’s Hospitals Network, Sydney, NSW, Australia
- 6Centre for Fertility and Health, Norwegian Institute of Public Health (NIPH), Oslo, Norway
- 7Department of Gynaecology, Bern University Hospital, University of Bern, Bern, Switzerland
- 8Institute of Social and Preventive Medicine, University of Bern, Bern, Switzerland
Objectives: To describe COVID-19 information-seeking behavior (CISB) during the first stage of the pandemic in Switzerland and identify its determinants.
Methods: We conducted an online cross-sectional survey (4 May to 6 July 2020). Participants self-reported their CISB (information sources and frequency), personal COVID-19 situation (e.g., perception about having had COVID-19), sociodemographic information, and completed validated measures of health literacy, and worry and anxiety. Data were analyzed using descriptive statistics and logistic regressions.
Results: We included 1,505 participants (24.7% male; mean age = 43.0 years, SD = 13.9). Most participants reported searching for information daily (n = 1,023, 68.0%) and referring to multiple information sources (mean 3.7, SD = 1.5). Commonly used sources were official websites (n = 1,129, 75.0%) and newspapers (n = 997, 66.2%). Participants with higher health literacy were more likely to seek information daily and use online resources, but less likely to use personal networks than those with lower health literacy. We did not find any association between CISB and worry and anxiety.
Conclusion: More opportunities for personal dialogue and education about reliable online information resources should be encouraged to optimize the CISB of groups with lower health literacy.
Introduction
With the outbreak of the novel coronavirus disease 2019 (COVID-19) extraordinary public health measures have been undertaken and new information was provided almost daily. People were informed about the introduction of diverse restrictive measures and steadily increasing numbers of new cases and deaths. However, at the same time, accurate information about the disease mechanisms and its consequences was lacking [1]. A feeling of uncertainty and fear can result from the fast changes in everyday life, and cause stress [2]. A strategy that can be used to deal with the uncertainty caused by a health threatening situation is searching for information [3–5].
Several definitions of health information-seeking behavior (HISB) have been provided in the literature. In a concept analysis on the term “health information-seeking behavior,” Lambert and Loiselle [4] defined it as the means that individuals use to obtain knowledge about health, including health promotion, risks and illnesses. The authors concluded that HISB involves only active and intentional engagement in information behaviors with the goal of fostering coping and psychosocial adjustment to an illness or health hazard. However, HISB could also result in negative outcomes as disruptive behaviors, information overload or avoidance, distrust, distress and anxiety [4, 5]. Whether information-seeking will result in positive or negative outcomes depends on personal and contextual factors, as well as the fit between the information sought and the retrieved information [4]. A recent study from China found that online COVID-19 information-seeking was associated with higher respect of preventive behaviors against contracting the disease and that higher worry caused by online information-seeking could further enhance preventive behaviors [6]. In a study from the UK, obsessive-compulsive symptoms were linked to higher information-seeking, which in turn resulted in higher adherence to government guidelines on COVID-19 [7]. Another study from Germany, showed two possible and yet contrasting outcomes associated with distress by information [8]. On one side, the experience of distress by information led to better compliance with preventive measures. On the other side, increased distress was also associated with avoidance of information, and in turn with lower compliance to preventive measures. In a study conducted among students in Finland [9], social media exposure resulted in information overload and information anxiety, which occurs when people perceive a gap between what they know and what they think they need to know about a topic [10]. Furthermore, excessive online health information-seeking might lead to cyberchondria, described as excessive anxiety or distress related to a high intensity of online information-seeking [11]. Especially at the beginning of the COVID-19 pandemic, when information was ample and rapidly evolving, it could have caused affective concerns and ultimately led to information avoidance [12]. Information avoidance might bring under-information about the development of the pandemic and its implications on health care and social life, but also affect health-related behaviors and the psychosocial health of individuals.
People’s HISB and its associated outcomes might depend on their health literacy [13]. In a systematic review of health literacy definitions and models, Sørensen et al. [14] define health literacy as one’s ability “to access, understand, appraise, and apply health information in order to make judgments and take decisions in everyday life concerning healthcare, disease prevention and health promotion to maintain or improve quality of life during the life course” (p. 3). The scientific evidence in a wide range of health fields shows that health literacy is associated with health-related knowledge, behaviors and ultimately health care access [15] and health outcomes [16]. In the context of the COVID-19 pandemic, health literacy can affect the approaches used to obtain information on the disease [17]. Inadequate health literacy could result in a poorer understanding of the risks associated with COVID-19, its preventive measures and symptoms, as well as in a higher possibility for misinformation, distrust in health authorities and ultimately adverse mental and physical health outcomes [18]. Previous research assessing the relationship between health literacy and COVID-19 information-seeking behavior focused mainly on university students, digital health literacy and online information-seeking [19–22] or other minority groups as immigrant women [23] and the deaf community [24].
Our aims were to 1) describe COVID-19 information-seeking during the early stage of the pandemic in Switzerland and 2) determine the association between health literacy, worry and anxiety, personal COVID-19 situation, and sociodemographic characteristics and a) frequency of information-seeking; b) use of traditional media; c) use of online resources and d) use of personal networks for information on COVID-19.
Methods
Sample and Procedure
The current investigation was part of the larger CoWELL study, a cross-sectional survey that assessed Swiss residents’ psychosocial outcomes and well-being during the early stage of the pandemic. We used a convenience sample. Participants were eligible if they were at least 18 years old, living in Switzerland at the time of the study and provided consent for participation after having received information about the study. Between 4 May and 6 July 2020, we distributed an online survey via Qualtrics software using our personal and professional networks. The survey was available in German, French, and Italian and consisted of two parts. Part 1 included measures of household composition and childcare, personal COVID-19 situation, health-related quality of life, health status, psychological distress, employment situation, health literacy, COVID-19 information-seeking behavior, and sociodemographic characteristics. Participants could also choose to complete part 2, which included assessments of worry and anxiety, post-traumatic growth, post-traumatic stress, resilience, and quality of partner relationship.
Measurements
COVID-19 Information-Seeking Behavior
The current study investigated HISB specific to COVID-19, which will be referred to as COVID-19 information-seeking behavior (CISB). Two questions were developed to assess CISB. First, frequency of CISB was assessed with the following question “How often do you inform yourself about COVID-19?” Answer options included: several times per day, about once a day, several times per week but not daily, about once a week, less than once a week, and no active information-seeking on COVID-19. Second, participants were asked to select the information sources they used to get information on COVID-19. Available options were: TV, radio, daily or weekly newspapers (online or offline), online-only news or portals, official websites, social media, health care providers, family/friends, other sources, and no active information-seeking on COVID-19. Participants indicating other sources were asked to provide further details with an open-ended answer. Multiple answers were possible.
Health Literacy
HL was assessed using the 12-item HLS-Q12 [25], a validated short version of the European Health Literacy Survey Questionnaire (HLS-EU-Q; 47 items) [26]. As the HLS-EU-Q, the HLS-Q12 measures HL across three health domains (health care, disease prevention, and health promotion) and four cognitive domains (access, understand, appraise, and apply). For the purpose of the current study, one additional item of the HLS-EU-Q (item 12; judge if the information about illness in the media is reliable) was added to the HLS-Q12 because we considered it important for health literacy associated to COVID-19. Translations of the HLS-EU-Q in the three national languages were provided by the Federal Office of Public Health, and the 13 relevant items were included in the survey. Answers were provided using 4-point Likert scales ranging from “1 = very difficult” to “4 = very easy”. The total health literacy score was then calculated by summing up the scores of the 13 items (possible scoring range: 13–52). The scale (including 13 items) showed very good reliability with a Cronbach’s alpha of 0.89.
Worry and Anxiety
Worry and anxiety was assessed using an adaptation of the worry and anxiety questionnaire (WAQ) that can be used to assess worry and anxiety in nonclinical samples [27]. The original WAQ consists of 6 items, including 1 open-ended question (item 1; what subjects do you worry about most often?) and 5 items scored on 9-point Likert scales (scored 0 to 8, with lower scores indicating lower worry and anxiety). Item 5 lists six somatic symptoms (restlessness; fatigue; concentration problems; irritability; muscle tension; and sleep disturbance). Our questionnaire applied 5-point Likert scales, which were recoded into 0 to 8 scoring for the analysis. In compliance with the questionnaire scoring instructions [27, 28], four binary (yes/no) variables and one sum variable were created to assess cognitive symptoms, somatic symptoms, generalized anxiety disorder (GAD), absence of symptoms, and overall worry and anxiety, respectively. To meet cognitive symptoms criteria, participants had to score “4” or higher on items 2, 3, and 4. To meet somatic symptoms criteria, participants had to score “4” or higher in at least 3 of the 6 somatic symptoms of item 5. To meet the GAD criteria, participants had to indicate at least one worry theme in item 1, meet both cognitive and somatic symptoms criteria, and score “4” or higher on item 6 (To what extent does worry or anxiety interfere with your life? For example, your work, social activities, family life, etc.). Participants who did not meet any of the three criteria were attributed “yes” on the fourth variable “absence of symptoms”. Overall worry and anxiety comprised the sum of all Likert-type items (possible scoring range: 0–80). It showed very good reliability with a Cronbach’s alpha of 0.89.
Personal COVID-19 Situation
Personal COVID-19 situation included three variables based on self-developed questions and two variables generated from effective public health measures at time of study and from the individuals’ health status relative to the COVID-19 pandemic. We assessed physical distancing behavior with the question “Please select the option that best describes your current situation” (with answer options: isolation; self-isolation; preventive self-isolation; physical distancing; initial physical distancing; no physical distancing), contact with a person who tested positive for COVID-19 with the question “Have you had contact with a positive COVID-19 case?” (yes/confirmed; yes/likely; no), and own perception about having already had COVID-19 with the question “Do you think you have already had COVID-19?” (yes/no). The physical distancing variable levels were recoded into three categories: physical distancing, (self-)isolation (isolation, (preventive) self-isolation), and no physical distancing (initial physical distancing, no physical distancing). We further calculated the stage of the pandemic at study completion according to the date of questionnaire completion: extreme restrictions (up to 10 May, 2020); mild easing of restrictions (from 11 May to 5 June 2020); extensive easing of restrictions (from 6 June 2020). Finally, we defined a binary variable resembling the risk to develop severe COVID-19 (yes/no) based on established risk factors according to the Swiss National Science Task Force [29]. Participants who had a BMI>30 kg/m2 (calculated as weight in kilograms divided by height in meters squared) and who reported to have a preexisting chronic condition (including cardiovascular diseases, lung diseases, diabetes, hypertension, a history of cancer) or a transplant were considered at risk for development of severe COVID-19.
Socio-Demographic Characteristics
Data on sex (female; male; other), age at study, highest educational achievement (compulsory schooling; vocational training; upper secondary education; university education), and employment situation (employed: full time or part time employment; unemployed: unemployed, on job search, housemaker, retired, invalid or other situation without employment; in education) were collected. Participants indicating “other” sex (n = 4) were recoded either as male (n = 1) or female (n = 3) based on the smallest difference between their height and the average height of men and women in the Swiss population [30].
Analysis
For participants who completed at least half of items included in the sum variables (overall health literacy and worry and anxiety), we substituted the missing items with the average of the completed items. Missing data in categorical variables were included in the analysis as a separate category.
For aim 1 we used content analysis and descriptive statistics. Open-ended answers to the question on information sources used were coded by the first author (AI), and double-checked by a second author (KR). Disagreement was resolved with discussion. We identified scientific resources, podcasts, employer/colleagues, and unknown internet resources, in addition to the information sources provided in the questionnaire. Sources were grouped into three categories for further analyses: traditional media (TV, radio, newspapers), online resources (online-only news or portals, official websites, social media, scientific resources, podcasts, and unknown internet resources), and personal networks (health care providers, family/friends, and employer/colleagues). The three groups reflect how information is acquired through the sources, with traditional media involving mainly passive information acquisition, online resources assuming mainly active information acquisition, and personal networks implying direct communication and personal interaction.
For aim 2 we first conducted univariable logistic regressions to predict daily information-seeking (yes: several times per day; about once a day/no: several times per week but not daily; about once a week; less than once a week; no active information-seeking on COVID-19), use of traditional media (yes/no), use of online resources (yes/no), and use of personal networks (yes/no) by health literacy, worry and anxiety, personal COVID-19 situation and sociodemographic characteristics. Interactions between health literacy and other independent variables were also included in univariable logistic regression models. Final multivariable logistic regression models included only variables that were significant in univariable regression models. Age, sex, and education were a priori included in every multivariable model. We used Wald tests to calculate global p-values for all categorical variables included in both univariable and multivariable regression models.
Descriptive statistics and logistic regression analyses were performed using Stata 17 [31] and statistical significance was set at level α< 0.05.
Results
Study Population
In total, 1757 persons participated. We included n = 1,505 (85.7%) participants who provided complete answers to the items measuring CISB (24.7% male). Of those, 286 (19.0%) did not complete part 2. Participants were on average 43 years old (SD = 13.9). Most participants completed university education (n = 957, 63.6%), and were employed (n = 1,281, 85.1%). Further information on the sample is displayed in Table 1.
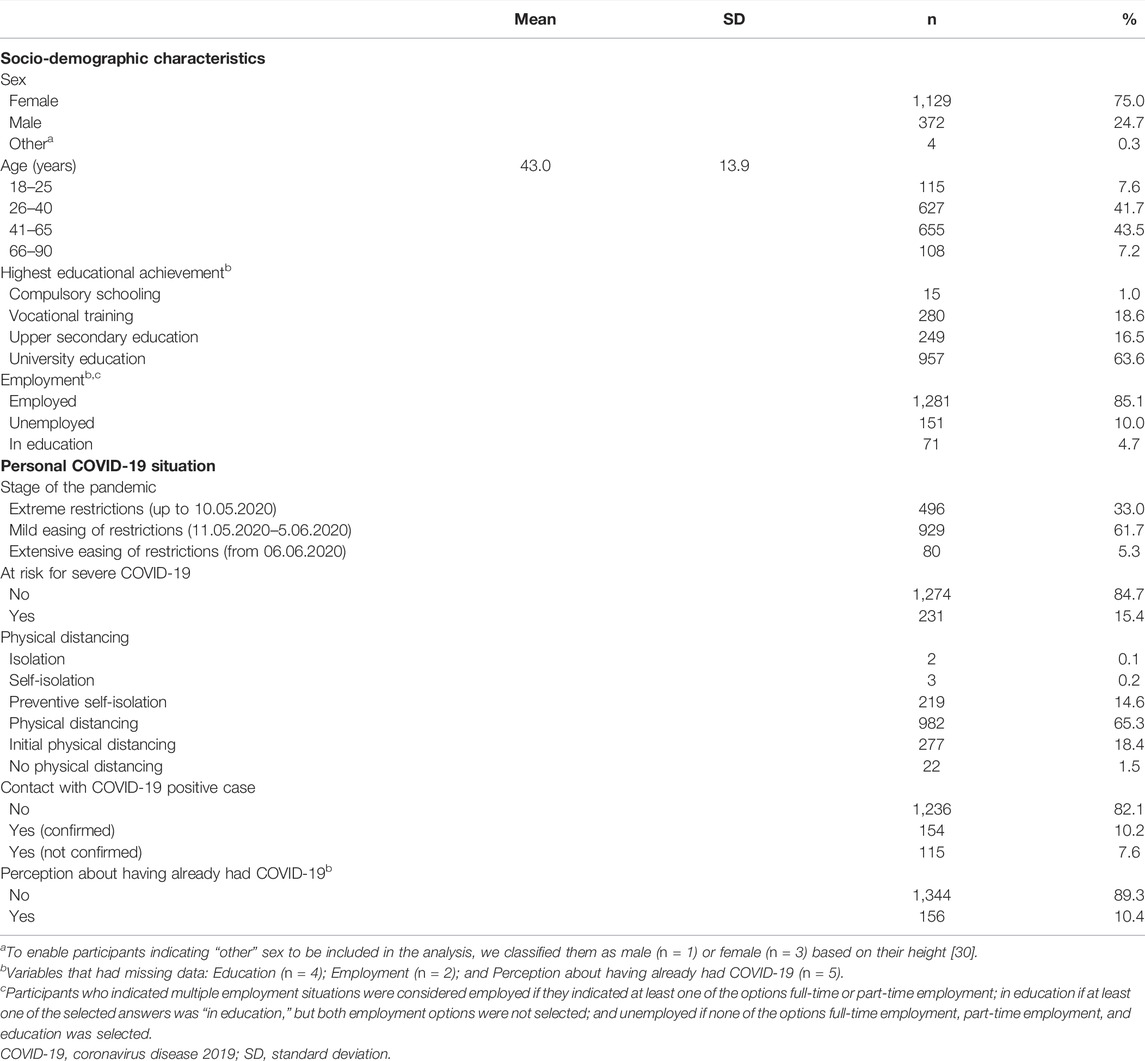
TABLE 1. Participants’ characteristics (n = 1,505), CoWELL study, Switzerland, 2020.
The mean overall health literacy score was 42.3 (SD = 6.2; range: 13–52). Further details about health literacy are available in Supplementary Table S1. The mean overall worry and anxiety score was 21.2 (SD = 14.1, range: 0–72). Two thirds of participants did not meet any WAQ criteria (n = 733, 67.9%), almost one third met somatic symptoms criteria (n = 317, 29.2%), followed by cognitive symptoms criteria (n = 118, 10.8%), and GAD criteria (n = 56, 5.2%).
Aim 1: Description of COVID-19 Information-Seeking
Only 1% of participants (n = 17) were not actively searching for information on COVID-19. The remaining participants were actively searching for information several times a day (n = 377, 25.1%), about once a day (n = 646, 42.9%), several times a week but not daily (n = 334, 22.2%), about once a week (n = 91, 6.1%), or less than once a week (n = 40, 2.7%). Participants reported using on average 3.7 different information sources (SD = 1.5). Online resources (n = 1,292, 85.8%) and traditional media (n = 1,289, 85.6%) were the most used types of sources to obtain information on COVID-19, while only about half of the sample used personal networks (n = 751, 49.9%). Often mentioned sources of information were official websites (n = 1,129, 75.0%), newspapers (n = 997, 66.2%), and TV (n = 924, 61.4%). For further details, see Figure 1.
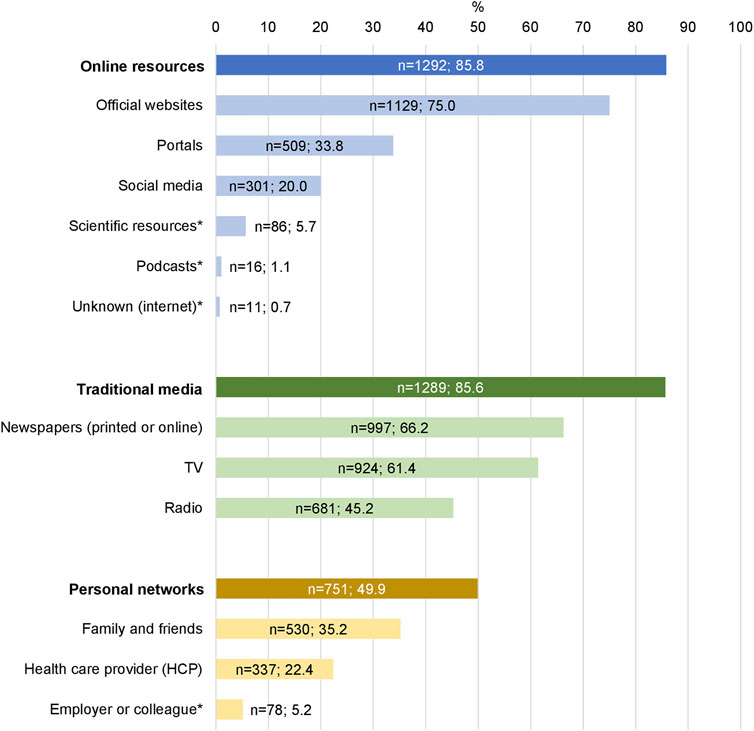
FIGURE 1. Used information sources (n = 1,505), CoWELL study, Switzerland, 2020.* Identified through content analysis of open-ended answers. Note: Totals do not sum up to 100 because of the possibility to provide multiple answers.
Aim 2: Associations
The following results are based on separate multivariable logistic regression models for each outcome (Table 2). Detailed results of the univariable regression models are available in Supplementary Table S2.
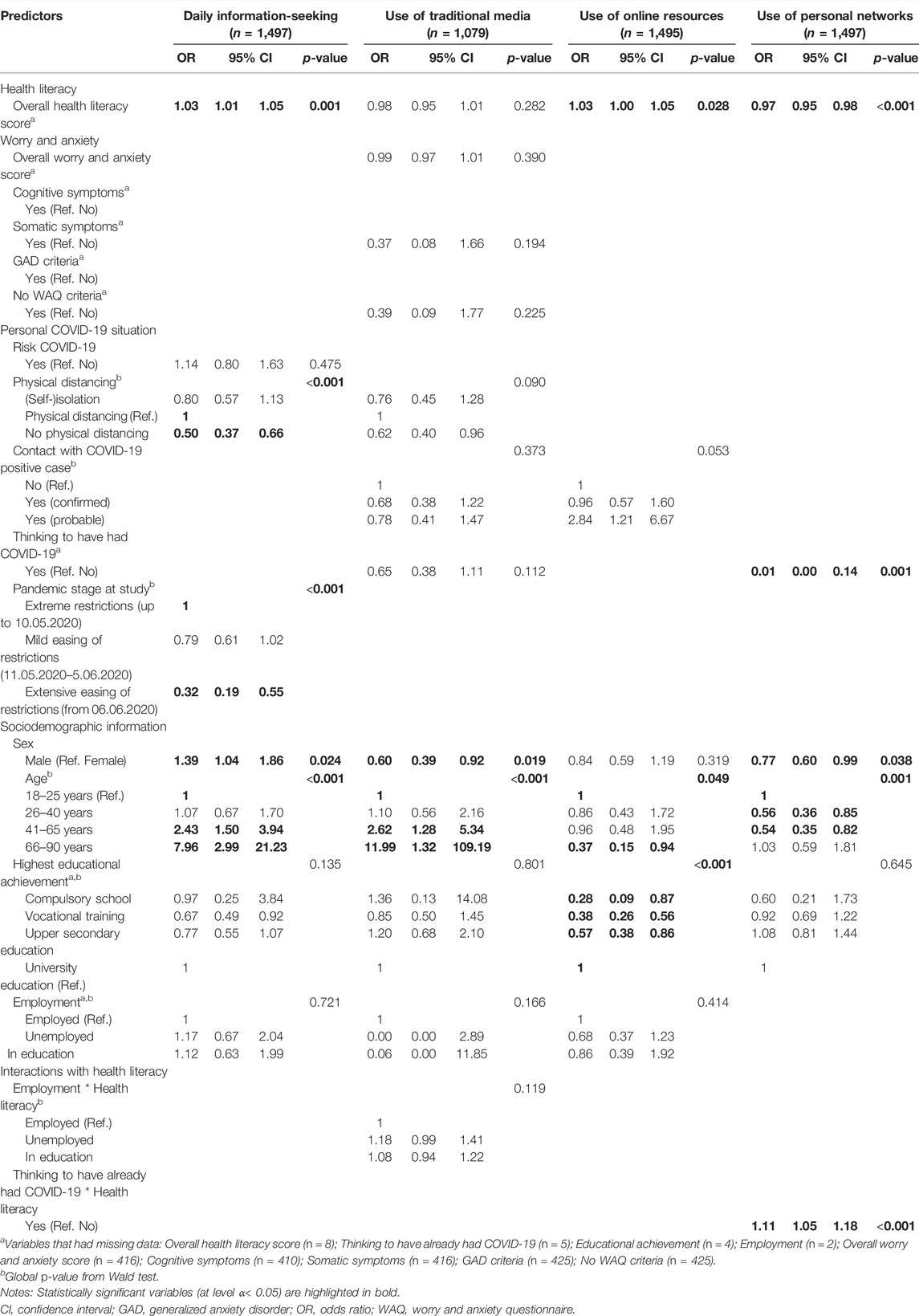
TABLE 2. Results of the multivariable logistic regression models for daily information-seeking, use of traditional media, use of online resources, and use of personal networks, CoWELL study, Switzerland, 2020.
Aim 2a: Daily Information-Seeking
We found daily information-seeking to be associated with higher health literacy (odds ratio (OR) = 1.03, 95% confidence interval (CI) 1.01–1.05). The following factors related to personal COVID-19 situation were associated with a lower likelihood of seeking information daily: not following physical distancing measures (compared with respecting physical distancing measures: OR = 0.50, 95% CI 0.37–0.66) and answering the survey during the phase of the pandemic when restrictions were extensively eased since their introduction (compared with the phase with extreme restrictions: OR = 0.32, 95% CI 0.19–0.55). Being male (OR = 1.39, 95% CI 1.04–1.86) and older age (41–65 years: OR = 2.43, 95% CI 1.50–3.94 and 66–90 years: OR = 7.96, 95% CI 2.99–21.23 compared to 18–25 years) were the only sociodemographic variables that were associated with daily information-seeking. Worry and anxiety was not associated with daily information-seeking.
Aim 2b: Use of Traditional Media
Older people were more likely than younger people (41–65 years: OR = 2.62, 95% CI 1.28–5.34 and 66–90 years: OR = 11.99, 95% CI 1.32–109.19; reference: 18–25 years) and men were less likely than women (OR = 0.60, 95% CI 0.39–0.92) to use traditional media. Health literacy, worry and anxiety, and personal COVID-19 situation were not associated with the use of traditional media.
Aim 2c: Use of Online Resources
Participants with higher health literacy (OR = 1.03, 95% CI 1.00–1.05) were more likely to use online resources. Participants with the following sociodemographic characteristics were less likely to use online resources: those having completed compulsory schooling (OR = 0.28, 95% CI 0.09–0.87), vocational training (OR = 0.38, 95% CI 0.26–0.56), or upper secondary education (OR = 0.57, 95% CI 0.38–0.86; reference: completed university education), and older participants (66–90 years: OR = 0.37, 95% CI 0.15–0.94; reference: 18–25 years). Worry and anxiety and personal COVID-19 situation were not associated with the use of online resources.
Aim 2d: Use of Personal Networks
Participants who believed that they had already had COVID-19 (OR = 0.01, 95% CI 0.00–0.14), young and middle-aged adults (26–40 years: OR = 0.56, 95% CI 0.36–0.85 and 41–65 years: OR = 0.54, 95% CI 0.35–0.82; reference 18–25 years), men (OR = 0.77; 95% CI 0.60–0.99) and participants with high health literacy (OR = 0.97, 95% CI 0.95–0.98) were less likely to use personal networks. We further found the interaction between thinking to have already had COVID-19 and higher health literacy (OR = 1.11, 95% CI 1.05–1.18) to be associated with the use of personal networks. We did not find any association between worry and anxiety and use of personal networks.
Discussion
Respondents reported searching for information on COVID-19 very frequently and using many different sources to get information. We found higher health literacy to be associated with daily information-seeking, use of online resources and less use of personal networks to obtain information on COVID-19. Worries and anxiety did not influence CISB in our sample. Zimmerman [17] showed that during the pandemic people were more likely to use news for health information and to use a higher number of information sources, compared to the period preceding the pandemic. Several sources that report news were often used for CISB in our sample, including newspapers, TV, radio and portals. These sources are common channels of health information for people with lower health literacy [32]. However, our study showed that during a pandemic the use of news sources for obtaining health information is common also among people with higher health literacy. Nonetheless, participants with high health literacy also used online resources to get information; these included mainly official websites that provide public and quality news. Participants with lower health literacy referred more commonly to personal networks. This group might prefer to obtaining health information through dialogue instead of reading, which requires additional comprehension skills. Additionally, it might be more difficult for people with lower health literacy to browse online health information and select reliable information to read, and they might instead prefer being provided with written information [33]. This group might not be aware of the availability of easy-to-access (both in terms of contents and delivery method) and high-quality online information resources. We therefore recommend that efforts aiming at providing information on COVID-19 to people with lower health literacy should concentrate on personal discussion or education about optimal internet navigation and reliable online resources.
An association between health anxiety and information-seeking has been often found in previous research, but there is no evidence that the relationship between the two variables is one-directional [34]. The current study did not find any association between frequency of CISB or any group of information sources and worry and anxiety. A study on the effect of the COVID-19 pandemic on mental health in the Swiss general population identified impaired mental well-being among one third of respondents [35], which is similar to around one third reporting worries and anxiety in our study. A recent study about cyberchondria in the course of the COVID-19 pandemic [36] identified intensive information-seeking as one of the risk factors for greater fear and anxiety. Despite the frequent information-seeking in our participants, we did not identify an association between use of online resources and worry and anxiety. In their concept analysis, Lambert and Loiselle [4] identified two main dimensions of HISB: the information dimension, and the method dimension. The information dimension describes the type (contents) and amount (level of detail) of the search. The method dimension refers to the actions (e.g., reading) performed in order to obtain the information and the used sources (e.g., newspaper). Since our study emphasized on the method dimension, we suggest future research to address the association between worry or anxiety and information type and amount. It is further possible that whether CISB causes further worry and anxiety depends on other aspects than health literacy.
Some aspects related to personal COVID-19 situation were associated with CISB. We found respondents answering during the stage when restrictions were extensively eased to be less likely to seek for information daily. With time people might have gradually decreased the compulsiveness of their searches as a consequence of adaptation to the “new normal.” Additionally, they may have optimized their ideal information path instead of simply avoiding information on the pandemic. However, we have no data on the degree of search detail and time spent to obtain the information. In our study, participants who did not adhere to physical distancing measures did not seek information on COVID-19 daily. In this group the perceived susceptibility to the virus may have been low [37] and resulted in less interest in this topic. Persons who believed to have already had COVID-19 tended not to use personal networks, which might indicate stigmatization of persons with COVID-19 at the early stage of the pandemic [38]. However, among this group, those with high health literacy used personal networks more often than those with low health literacy, indicating that people with a high health literacy might be more capable to communicate about their disease experience with others.
In line with previous literature [39], sex, age and education were associated with CISB. Men were more likely to engage in CISB daily than women, but women used traditional media sources and personal networks more than men. Older participants were more likely to seek for information daily, and preferred traditional media to online resources compared to younger participants. Personal networks were equally important for information-seeking in both old and very young participants, but people in their working age were less likely to use them for information on COVID-19. Older adults might feel higher susceptibility to severe COVID-19. Therefore, they might want to search for information frequently to stay informed about the latest developments. Traditional media might be preferred by this group over online resources because of the ease with which reliable information can be retrieved [33] or familiarity with acquiring health information through these channels [40]. Finally, in line with previous research [39], participants who completed university education reverted to online resources more often than other participants. People with higher education could be more aware of the heterogeneity of online information and trust in their ability to critically assess the retrieved information [41].
Strengths and Limitations
Our findings should be interpreted in light of some limitations. First, data on the exact contents of the sought COVID-19 information including its quality was not available and our results can only refer to the method dimension of CISB. Second, our findings may be generalized only partially because of study participants’ characteristics. The study used a convenience sample, which included mainly female participants, who were well-educated and highly involved in COVID-19 information-seeking. Our recruitment strategy underlies self-selection bias, with people engaged and interested in COVID-19 being more willing to take a survey on this topic. When data collection started, the state of extraordinary situation was still in place in Switzerland. Therefore, alternative ways to recruit participants were hardly attainable. Due to the characteristics of the sample, the results of the current study might have underestimated the association between worry and anxiety and the assessed aspects of CISB. Therefore, we suggest future research to further explore CISB in populations with lower education and health literacy. The main strength of the current study is its large sample size, which gives more reliable results, better precision, and power. Further, at the moment of data collection, a health literacy assessment tool specific to COVID-19 was not yet available. We used items from the HLS-EU-Q, a well-established health literacy assessment scale which has previously been used in Switzerland and showed very good reliability in our sample.
Conclusion
Despite the concern that online CISB could further increase worries and uncertainty in people with lower health literacy, our results indicated that this group prefers obtaining information through personal networks. Individuals with lower health literacy should be addressed by using personal dialogue and education about reliable online information resources should be encouraged.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
KR, GS, VM, and GM initiated the study. Together with AI and JB, KR, GS, VM, and GM designed and implemented the study and collected the data. AI conducted the data analysis with support from KR, JB, GS, and GM. VM, LM, and DD provided feedback to data analysis. AI was the main contributor to the manuscript. GM was the senior author and she additionally secured resources and funding. All authors provided feedback and approved the final version of the manuscript.
Funding
The CoWELL study was supported by the University of Lucerne research committee (FoKo; Grant number: 20-064-GM) and by the Swiss National Science Foundation (SNSF; Grant number: 10001C_182129/1; Early Postdoc.Mobility fellowships to JB: P2LUP1_195091 and VM: P2BEP3_191798).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.ssph-journal.org/articles/10.3389/ijph.2022.1604717/full#supplementary-material
Abbreviations
BMI, body mass index; CI, confidence interval; CISB, COVID-19 information-seeking behavior; COVID-19, coronavirus disease 2019; GAD, generalized anxiety disorder; HISB, health information-seeking behavior; OR, odds ratio; SD, standard deviation; SNSF, Swiss National Science Foundation; UK, United Kingdom.
References
1. Heiat, M, Heiat, F, Halaji, M, Ranjbar, R, Tavangar Marvasti, Z, Yaali-Jahromi, E, et al. Phobia and Fear of COVID-19: Origins, Complications and Management, a Narrative Review. Ann Ig (2021) 33(4):360–70. doi:10.7416/ai.2021.2446
2. Peters, A, McEwen, BS, and Friston, K. Uncertainty and Stress: Why it Causes Diseases and How it Is Mastered by the Brain. Prog Neurobiol (2017) 156:164–88. doi:10.1016/j.pneurobio.2017.05.004
3. Lee, SY, and Hawkins, RP. Worry as an Uncertainty-Associated Emotion: Exploring the Role of Worry in Health Information Seeking. Health Commun (2016) 31(8):926–33. doi:10.1080/10410236.2015.1018701
4. Lambert, SD, and Loiselle, CG. Health Information—Seeking Behavior. Qual Health Res (2007) 17(8):1006–19. doi:10.1177/1049732307305199
5. Zimmerman, MS, and Shaw, G. Health Information Seeking Behaviour: a Concept Analysis. Health Info Libr J (2020) 37(3):173–91. doi:10.1111/hir.12287
6. Liu, PL. COVID-19 Information Seeking on Digital Media and Preventive Behaviors: The Mediation Role of Worry. Cyberpsychol Behav Soc Netw (2020) 23(10):677–82. doi:10.1089/cyber.2020.0250
7. Loosen, AM, Skvortsova, V, and Hauser, TU. Obsessive–compulsive Symptoms and Information Seeking during the Covid-19 Pandemic. Transl Psychiatry (2021) 11(1):309. doi:10.1038/s41398-021-01410-x
8. Siebenhaar, KU, Kother, AK, and Alpers, GW. Dealing with the COVID-19 Infodemic: Distress by Information, Information Avoidance, and Compliance with Preventive Measures. Front Psychol (2020) 11:567905. doi:10.3389/fpsyg.2020.567905
9. Soroya, SH, Farooq, A, Mahmood, K, Isoaho, J, and Zara, S. From Information Seeking to Information Avoidance: Understanding the Health Information Behavior during a Global Health Crisis. Inf Process Manag (2021) 58(2):102440. doi:10.1016/j.ipm.2020.102440
10. Wurman, RS. Information Anxiety : Is Produced by the Ever-Widening gap between what We Understand and what Wie Think We Should Understand. It Is the Black Hole between Data and Knowledge, and it Happens when Information Doesn't Tell Us what We Want or Need to Know. 1st ed. ed. New York: Doubleday (1989).
11. Starcevic, V, Berle, D, and Arnáez, S. Recent Insights into Cyberchondria. Curr Psychiatry Rep (2020) 22(11):56. doi:10.1007/s11920-020-01179-8
12. Howell, JL, Lipsey, NP, and Shepperd, JA. Health Information Avoidance. In: LM Cohen, editor. The Wiley Encyclopedia of Health Psychology. The Social Bases of Health Behavior. Hoboken, New Jersey: John Wiley & Sons (2021). p. 279–86.
13. Lee, HY, Jin, SW, Henning-Smith, C, Lee, J, and Lee, J. Role of Health Literacy in Health-Related Information-Seeking Behavior Online: Cross-Sectional Study. J Med Internet Res (2021) 23(1):e14088. doi:10.2196/14088
14. Sørensen, K, Van den Broucke, S, Fullam, J, Doyle, G, Pelikan, J, Slonska, Z, et al. Health Literacy and Public Health: A Systematic Review and Integration of Definitions and Models. BMC Public Health (2012) 12(1):80. doi:10.1186/1471-2458-12-80
15. Levy, H, and Janke, A. Health Literacy and Access to Care. J Health Commun (2016) 21(Suppl. 1):43–50. doi:10.1080/10810730.2015.1131776
16. Berkman, ND, Sheridan, SL, Donahue, KE, Halpern, DJ, and Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann Intern Med (2011) 155(2):97–107. doi:10.7326/0003-4819-155-2-201107190-00005
17. Zimmerman, MS. Health Information-Seeking Behavior in the Time of COVID-19: Information Horizons Methodology to Decipher Source Path during a Global Pandemic. J Documentation (2021) 77(6):1248–64. doi:10.1108/jd-01-2021-0022
18. Paakkari, L, and Okan, O. COVID-19: Health Literacy Is an Underestimated Problem. Lancet Public Health (2020) 5(5):e249–e50. doi:10.1016/S2468-2667(20)30086-4
19. Zakar, R, Iqbal, S, Zakar, MZ, and Fischer, F. COVID-19 and Health Information Seeking Behavior: Digital Health Literacy Survey Amongst University Students in Pakistan. Int J Environ Res Public Health (2021) 18(8):4009. doi:10.3390/ijerph18084009
20. Rosário, R, Martins, MRO, Augusto, C, Silva, MJ, Martins, S, Duarte, A, et al. Associations between COVID-19-Related Digital Health Literacy and Online Information-Seeking Behavior Among Portuguese University Students. Int J Environ Res Public Health (2020) 17(23):E8987. doi:10.3390/ijerph17238987
21. Vrdelja, M, Vrbovšek, S, Klopčič, V, Dadaczynski, K, and Okan, O. Facing the Growing COVID-19 Infodemic: Digital Health Literacy and Information-Seeking Behaviour of University Students in Slovenia. Int J Environ Res Public Health (2021) 18(16):8507. doi:10.3390/ijerph18168507
22. Dadaczynski, K, Okan, O, Messer, M, Leung, AYM, Rosario, R, Darlington, E, et al. Digital Health Literacy and Web-Based Information-Seeking Behaviors of University Students in Germany during the COVID-19 Pandemic: Cross-Sectional Survey Study. J Med Internet Res (2021) 23(1):e24097. doi:10.2196/24097
23. Chae, S, Lee, YJ, and Han, HR. Sources of Health Information, Technology Access, and Use Among Non-English-Speaking Immigrant Women: Descriptive Correlational Study. J Med Internet Res (2021) 23(10):e29155. doi:10.2196/29155
24. Panko, TL, Contreras, J, Postl, D, Mussallem, A, Champlin, S, Paasche-Orlow, MK, et al. The Deaf Community's Experiences Navigating COVID-19 Pandemic Information. Health Lit Res Pract (2021) 5(2):e162–e170. doi:10.3928/24748307-20210503-01
25. Finbråten, HS, Wilde-Larsson, B, Nordström, G, Pettersen, KS, Trollvik, A, Guttersrud, Ø, et al. Establishing the HLS-Q12 Short Version of the European Health Literacy Survey Questionnaire: Latent Trait Analyses Applying Rasch Modelling and Confirmatory Factor Analysis. BMC Health Serv Res (2018) 18(1):506. doi:10.1186/s12913-018-3275-7
26. Sørensen, K, Van den Broucke, S, Pelikan, JM, Fullam, J, Doyle, G, Slonska, Z, et al. Measuring Health Literacy in Populations: Illuminating the Design and Development Process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health (2013) 13:948. doi:10.1186/1471-2458-13-948
27. Dugas, MJ, Freeston, MH, Provencher, MD, Lachance, S, Ladouceur, R, and Gosselin, P. Le Questionnaire sur l'Inquiétude et l'Anxiété. Validation dans des échantillons non cliniques et cliniques. [The Worry and Anxiety Questionnaire: Validation in non-clinical and clinical samples.]. J de Thérapie Comportementale Cogn (2001) 11(1):31–6.
28.Université du Québec en Outaouais. Laboratoire des troubles d'anxiété. WAQ [Internet]. Gatineau, Canada: Université du Québec en Outaouais (2021).
29.Clinical Group. Risk Factors for Severe Manifestations of SARS-CoV-2 Infection [Internet]. National COVID-19 Science Task Force (NCS-TF) (2020). Available from: https://sciencetaskforce.ch/en/policy-brief/risk-factors-for-severe-manifestations-of-sars-cov-2-infection/(Accessed December 1, 2021).
30.Bundesamt für Statistik. Durchschnittliche Körpergrösse (In Cm) [Internet] (2019). Available from: https://www.bfs.admin.ch/bfs/de/home/statistiken/kataloge-datenbanken/tabellen.assetdetail.7586022.html (Accessed December 1, 2021).
32. Chen, X, Hay, JL, Waters, EA, Kiviniemi, MT, Biddle, C, Schofield, E, et al. Health Literacy and Use and Trust in Health Information. J Health Commun (2018) 23(8):724–34. doi:10.1080/10810730.2018.1511658
33. Manganello, J, Gerstner, G, Pergolino, K, Graham, Y, Falisi, A, Strogatz, D, et al. The Relationship of Health Literacy with Use of Digital Technology for Health Information: Implications for Public Health Practice. J Public Health Manag Pract (2017) 23(4):380–7. doi:10.1097/phh.0000000000000366
34. Jagtap, S, Shamblaw, AL, Rumas, R, and Best, MW. Information Seeking and Health Anxiety during the COVID-19 Pandemic: The Mediating Role of Catastrophic Cognitions. Clin Psychol Psychother (2021) 28(6):1379–90. doi:10.1002/cpp.2684
35. Diaz Hernandez, L, Giezendanner, S, Fischer, R, and Zeller, A. The Effect of COVID-19 on Mental Well-Being in Switzerland: a Cross-Sectional Survey of the Adult Swiss General Population. BMC Fam Pract (2021) 22(1):181. doi:10.1186/s12875-021-01532-7
36. Starcevic, V, Schimmenti, A, Billieux, J, and Berle, D. Cyberchondria in the Time of the COVID-19 Pandemic. Hum Behav Emerg Technol (2021) 3(1):53–62. doi:10.1002/hbe2.233
37. Park, T, Ju, I, Ohs, JE, and Hinsley, A. Optimistic Bias and Preventive Behavioral Engagement in the Context of COVID-19. Res Soc Adm Pharm (2021) 17(1):1859–66. doi:10.1016/j.sapharm.2020.06.004
38. Chew, C-C, Lim, X-J, Chang, C-T, Rajan, P, Nasir, N, Low, W-Y, et al. Experiences of Social Stigma Among Patients Tested Positive for COVID-19 and Their Family Members: a Qualitative Study. BMC Public Health (2021) 21(1):1623. doi:10.1186/s12889-021-11679-8
39. Schmidt, H, Wild, EM, and Schreyögg, J. Explaining Variation in Health Information Seeking Behaviour - Insights from a Multilingual Survey. Health Policy (2021) 125(5):618–26. doi:10.1016/j.healthpol.2021.01.008
40. Chu, L, Fung, HH, Tse, DCK, Tsang, VHL, Zhang, H, Mai, C, et al. Obtaining Information from Different Sources Matters during the COVID-19 Pandemic. Gerontologist (2021) 61(2):187–95. doi:10.1093/geront/gnaa222
Keywords: COVID-19, information-seeking, media sources, health literacy, worry, anxiety
Citation: Ilic A, Roser K, Sommer G, Baenziger J, Mitter VR, Mader L, Dyntar D and Michel G (2022) COVID-19 Information-Seeking, Health Literacy, and Worry and Anxiety During the Early Stage of the Pandemic in Switzerland: A Cross-Sectional Study. Int J Public Health 67:1604717. doi: 10.3389/ijph.2022.1604717
Received: 22 December 2021; Accepted: 06 July 2022;
Published: 09 August 2022.
Edited by:
Gonzalo Martinez-Ales, Columbia University, United StatesReviewed by:
Giacomo Pignataro, University of Catania, ItalySanjeev Gupta, LN Medical College, India
Copyright © 2022 Ilic, Roser, Sommer, Baenziger, Mitter, Mader, Dyntar and Michel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gisela Michel, gisela.michel@unilu.ch
This Original Article is part of the IJPH Special Issue “The Impact of the COVID-19 Pandemic on Mental Health.”