
Impact of the COVID-19 Pandemic on Community Consumption of Antibiotics for Systemic Use and Resistance of Invasive Streptococcus pneumoniae in Slovenia

Abstract
:1. Introduction
2. Results
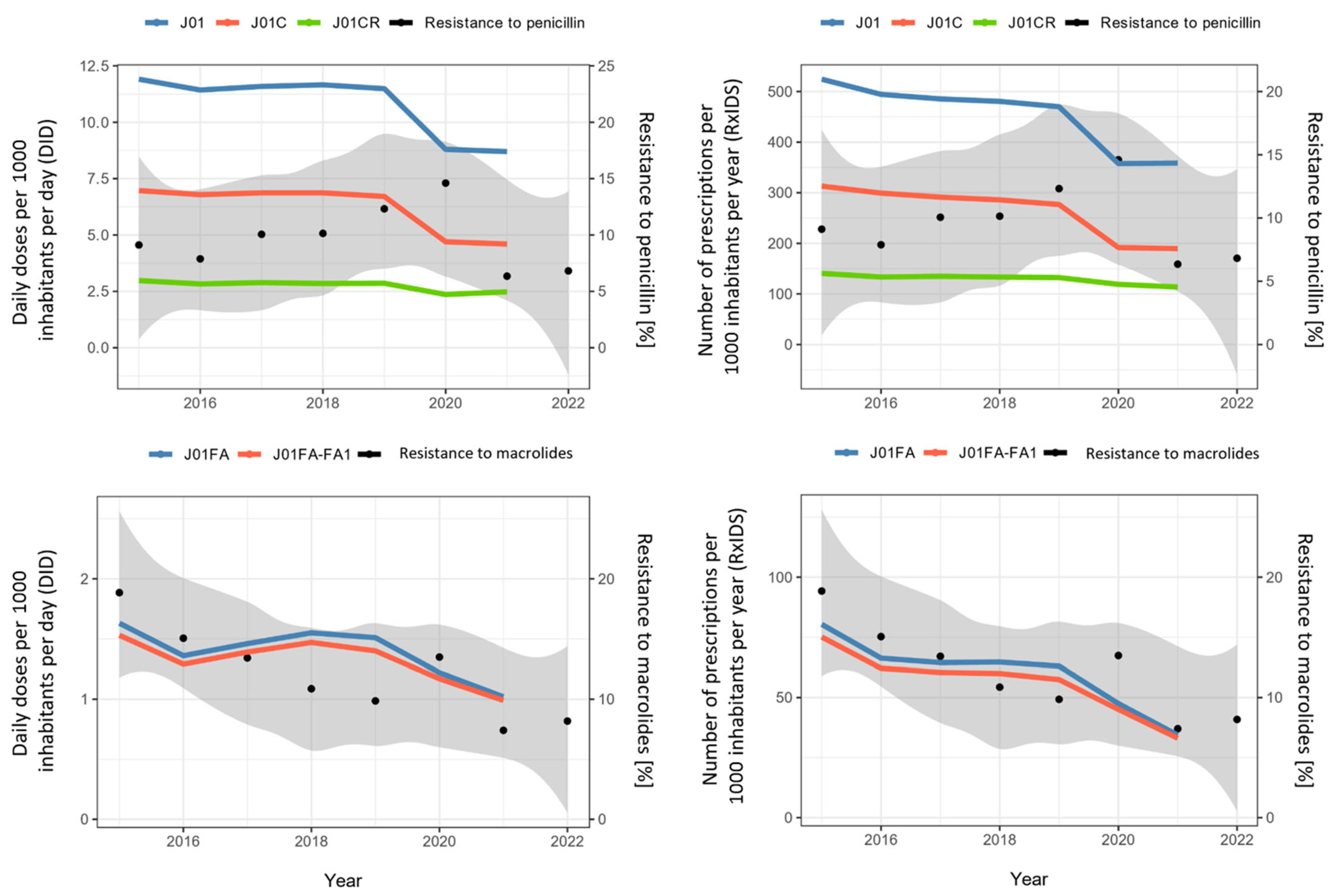
2.1. Consumption of Antibiotics
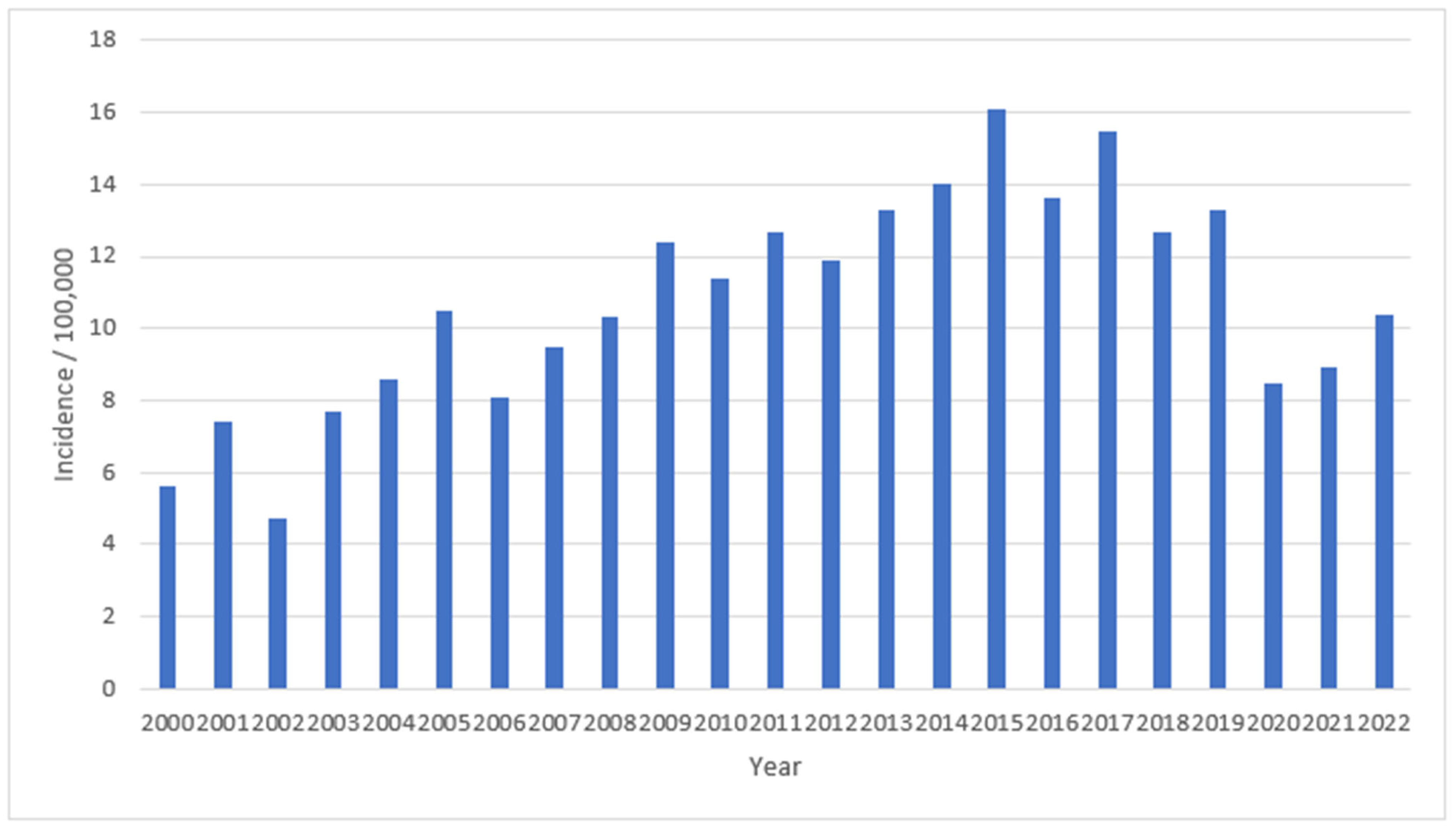
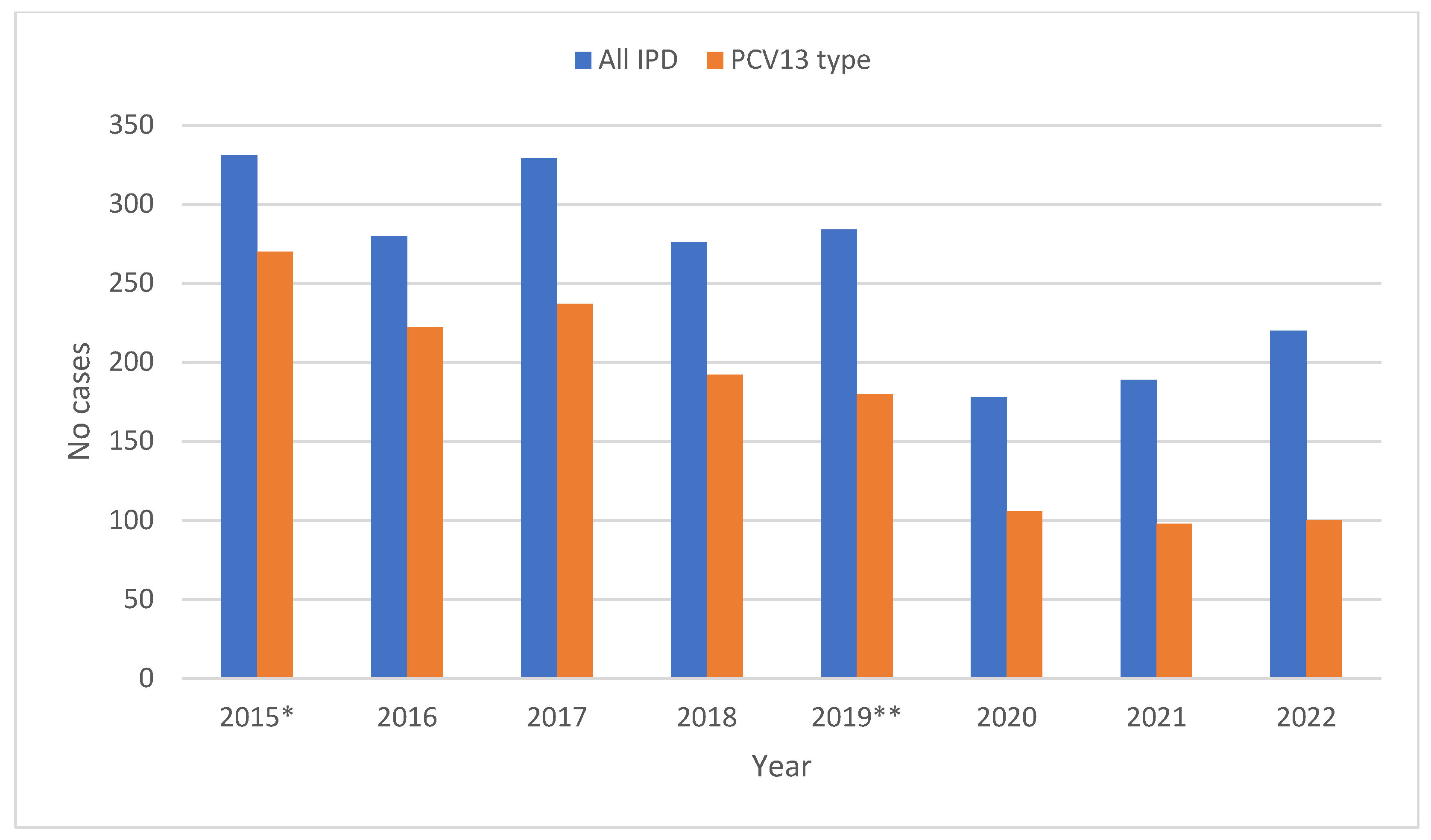
2.2. Incidence of Invasive Streptococcus pneumoniae in Slovenia
2.3. Resistance of Invasive Streptococcus pneumoniae to Penicillin and Macrolides
2.4. Correlation between Consumption of Total Antibiotics for Systemic Use, Penicillins, Broad-Spectrum Penicillins, Macrolides and Broad-Spectrum Macrolides and Resistance of Invasive S. pneumoniae to Penicillin (Intermediate and Resistant) and Macrolides
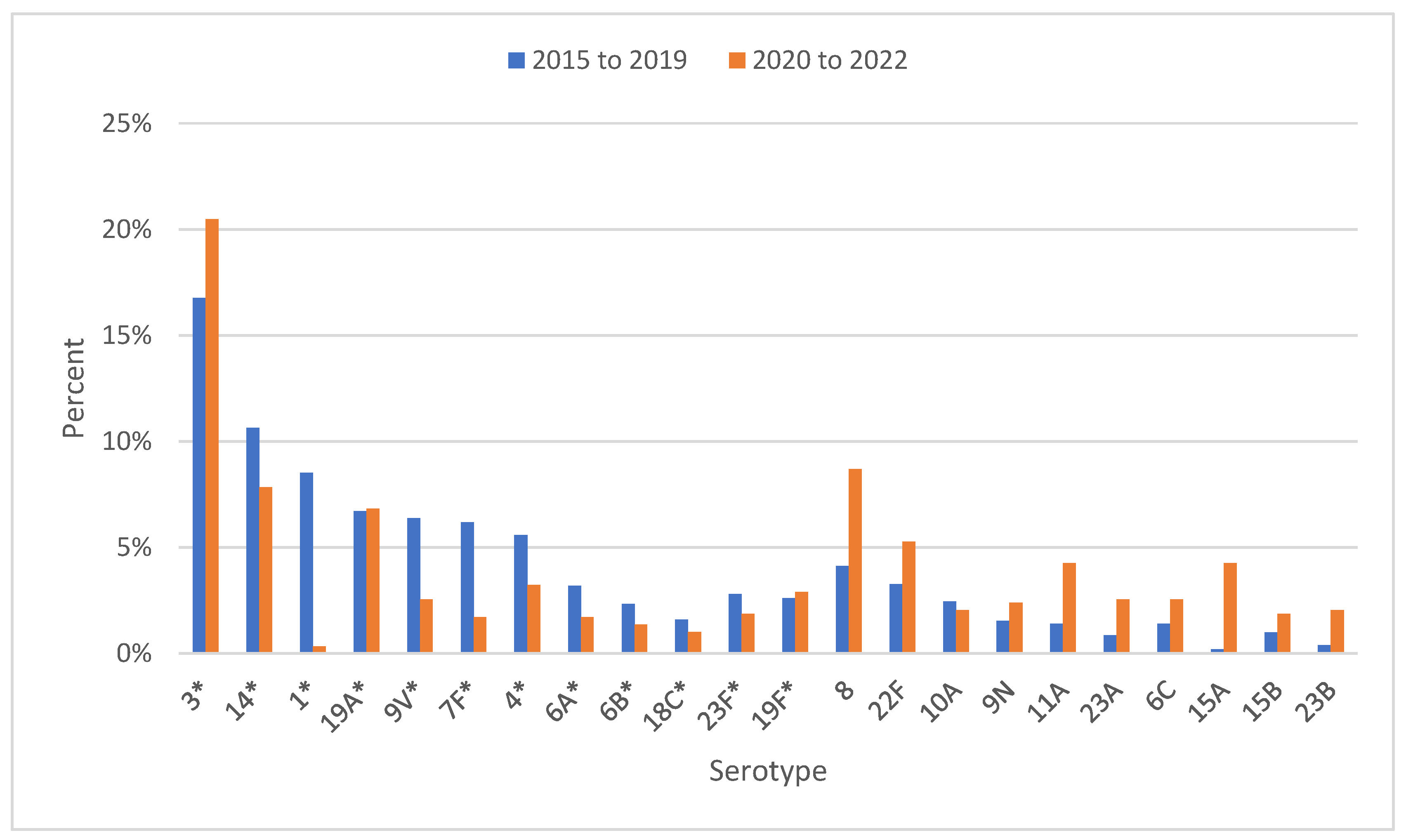
2.5. Serotype Distribution in Invasive S. pneumoniae in Slovenia
3. Discussion
4. Materials and Methods
4.1. Study Site
4.2. Collection of Isolates and Serotyping
4.3. Antibiotic Susceptibility Testing
4.4. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hussain, A.Z.; Paudyal, V.; Hadi, M.A. Impact of the COVID-19 Pandemic on the Prescribing Patterns of First-Line Antibiotics in English Primary Care: A Longitudinal Analysis of National Prescribing Dataset. Antibiotics 2021, 10, 591. [Google Scholar] [CrossRef]
- Kitano, T.; Brown, K.A.; Daneman, N.; MacFadden, D.R.; Langford, B.J.; Leung, V.; So, M.; Leung, E.; Burrows, L.; Manuel, D.; et al. An Interrupted Time Series Analysis. Open. Forum Infect. Dis. 2021, 8, ofab533. [Google Scholar] [CrossRef]
- Högberg, L.D.; Vlahović-Palčevski, V.; Pereira, C.; Weist, K.; Monnet, D.L.; ESAC-Net Study Group; ESAC-Net Study Group Participants. Decrease in community antibiotic consumption during the COVID-19 pandemic, EU/EEA, 2020. Euro. Surveill. 2021, 26, 2101020. [Google Scholar] [CrossRef]
- Bara, W.; Brun-Buisson, C.; Coignard, B.; Watier, L. Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic. Antibiotics 2022, 11, 643. [Google Scholar] [CrossRef]
- Hamilton, A.; Poleon, S.; Cherian, J.; Cosgrove, S.; Laxminarayan, R.; Klein, E. COVID-19 and Outpatient Antibiotic Prescriptions in the United States: A County-Level Analysis. Open. Forum Infect. Dis. 2023, 10, ofad096. [Google Scholar] [CrossRef]
- Bronzwaer, S.L.; Cars, O.; Buchholz, U.; Mölstad, S.; Goettsch, W.; Veldhuijzen, I.K.; Kool, J.L.; Sprenger, M.J.; Degener, J.E. European Antimicrobial Resistance Surveillance System. A European study on the relationship between antimicrobial use and antimicrobial resistance. Emerg. Infect. Dis. 2002, 8, 278–282. [Google Scholar] [CrossRef]
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M.; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Van de Sande-Bruinsma, N.; Grundmann, H.; Verloo, D.; Tiemersma, E.; Monen, J.; Goossens, H.; Ferech, M.; European Antimicrobial Resistance Surveillance System Group; European Surveillance of Antimicrobial Consumption Project Group. Antimicrobial drug use and resistance in Europe. Emerg. Infect. Dis. 2008, 14, 1722–1730. [Google Scholar] [CrossRef]
- Čižman, M.; Mioč, V.; Bajec, T.; Paragi, M.; Kastrin, T.; Gonçalves, J. Correlation between Antibiotic Consumption and Resistance of Invasive Streptococcus pneumoniae. Antibiotics 2021, 10, 758. [Google Scholar] [CrossRef]
- Olesen, S.W.; Barnett, M.L.; MacFadden, D.R.; Brownstein, J.S.; Hernández-Díaz, S.; Lipsitch, M.; Grad, Y.H. The distribution of antibiotic use and its association with antibiotic resistance. eLife 2018, 7, e39435. [Google Scholar] [CrossRef]
- Goossens, H. Antibiotic consumption and link to resistance. Clin. Microbiol. Infect. 2009, 15 (Suppl. S3), 12–15. [Google Scholar] [CrossRef]
- Cizman, M. The use and resistance to antibiotics in the community. Int. J. Antimicrob. Agents 2003, 21, 297–307. [Google Scholar] [CrossRef]
- Enne, V.I. Reducing antimicrobial resistance in the community by restricting prescribing: Can it be done? J. Antimicrob. Chemother. 2010, 65, 179–182. [Google Scholar] [CrossRef]
- Cizman, M.; Beović, B.; Seme, K.; Paragi, M.; Strumbelj, I.; Müller-Premru, M.; Cad-Pecar, S.; Pokorn, M. Macrolide resistance rates in respiratory pathogens in Slovenia following reduced macrolide use. Int. J. Antimicrob. Agents 2006, 28, 537–542. [Google Scholar] [CrossRef]
- Seppälä, H.; Klaukka, T.; Vuopio-Varkila, J.; Muotiala, A.; Helenius, H.; Lager, K.; Huovinen, P. The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. Finnish Study Group for Antimicrobial Resistance. N. Engl. J. Med. 1997, 337, 441–446. [Google Scholar] [CrossRef]
- Kastrin, T.; Paragi, M.; Erčulj, V.; Žohar Čretnik, T.; Slovenian Meningitidis Study Group; Bajec, T.; Čižman, M. Lack of correlation between reduced outpatient consumption of macrolides and macrolide resistance of invasive Streptococcus pneumoniae isolates in Slovenia during 1997–2017. J. Glob. Antimicrob. Resist. 2019, 16, 242–248. [Google Scholar] [CrossRef]
- Precepljenost Predšolskih Otrok v Sloveniji v Letu 2021 PRELIMINARNI PODATKI. Available online: https://www.nijz.si/sites/www.nijz.si/files/uploaded/predsolski_otroci_precepljenost_2021_preliminarno_porocilo.pdf (accessed on 17 April 2023).
- Poraba Protimikrobnih Zdravil v Sloveniji v Letu 2021. Available online: https://www.nijz.si/sl/publikacije/poraba-protimikrobnih-zdravil-v-sloveniji-v-letu-2021 (accessed on 10 January 2023).
- Available online: https://www.nijz.si/sl/publikacije/porabaprotimikrobnihzdravilvSlovenijivletu2020|Nijz (accessed on 17 April 2023).
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2021; ECDC: Stockholm, Sweden, 2022. [Google Scholar]
- Antimicrobial Resistance Surveillance in Europe 2023-2021 Data. Stockholm: European Centre for Disease Prevention and Control and World Health Organization. Cataloguing-in-Publication (CIP) Data. 2023. Available online: http://apps.who.int/iris (accessed on 15 May 2023).
- Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemiological Report for 2021. Available online: https://www.ecdc.europa.eu/ (accessed on 15 May 2023).
- Swedres-Svarm 2019. Sales of Antibiotics and Occurrence of Resistance in Sweden. Solna/Uppsala ISSN1650-6332. Available online: https://www.folkhalsomyndigheten.se/contentassets/fb80663bc7c94d678be785e3360917d1/swedres-svarm-2019.pdf (accessed on 15 May 2023).
- Swedres-Svarm 2020. Sales of Antibiotics and Occurrence of Resistance in Sweden. Solna/Uppsala ISSN1650-6332. Available online: https://www.sva.se/media/8d9678c390929e9/swedres_svarm_2020.pdf (accessed on 15 May 2023).
- Swedres-Svarm 2021. Sales of Antibiotics and Occurrence of Resistance in Sweden. Solna/Uppsala ISSN1650-6332. Available online: https://www.sva.se/media/8da965da486b11e/swedres_svarm_2021.pdf (accessed on 15 May 2023).
- Ribeiro Duarte, A.S.; Borck Høg, B.; Korsgaard, H.B.; Attauabi, M.; Boel, J.; Dalby, T.; Hammerum, A.M.; Hansen, F.; Hasman, H.; Henius, A.E.; et al. DANMAP 2021—Use of Antimicrobial Agents and Occurrence of Antimicrobial Resistance in Bacteria from Food Animals, Food and Humans in Denmark; Statens Serum Institut: Copenhagen, Denmark, 2021; ISSN 1600-2032. [Google Scholar]
- NethMap 2022 Consumption of Antimicrobial Agents and Antimicrobial Resistance among Medically Important Bacteria in The Netherlands in 2021. NethMap|MARAN|2022. Available online: https://www.rivm.nl/bibliotheek/rapporten/2022-0057.pdf (accessed on 15 May 2023).
- Turnidge, J.; Christiansen, K. Antibiotic use and resistance—Proving the obvious. Lancet 2005, 365, 548–549. [Google Scholar] [CrossRef]
- Sempere, J.; Llamosí, M.; López Ruiz, B.; Del Río, I.; Pérez-García, C.; Lago, D.; Gimeno, M.; Coronel, P.; González-Camacho, F.; Domenech, M.; et al. Effect of pneumococcal conjugate vaccines and SARS-CoV-2 on antimicrobial resistance and the emergence of Streptococcus pneumoniae serotypes with reduced susceptibility in Spain, 2004–2020: A national surveillance study. Lancet Microbe 2022, 3, e744–e752. [Google Scholar] [CrossRef]
- Surveillance Atlas of Infectious Diseases. Available online: http://atlas.ecdc.europa.eu/public/index.aspx (accessed on 10 March 2023).
- Bertran, M.; Amin-Chowdhury, Z.; Sheppard, C.L.; Eletu, S.; Zamarreño, D.V.; Ramsay, M.E.; Litt, D.; Fry, N.K.; Ladhani, S.N. Increased Incidence of Invasive Pneumococcal Disease among Children after COVID-19 Pandemic, England. Emerg. Infect. Dis. 2022, 28, 1669–1672. [Google Scholar] [CrossRef]
- Wasserman, M.; Chapman, R.; Lapidot, R.; Sutton, K.; Dillon-Murphy, D.; Patel, S.; Chilson, E.; Snow, V.; Farkouh, R.; Pelton, S. Twenty-Year Public Health Impact of 7- and 13-Valent Pneumococcal Conjugate Vaccines in US Children. Emerg. Infect. Dis. 2021, 27, 1627–1636. [Google Scholar] [CrossRef]
- Gambia Pneumococcal Surveillance Group; Mackenzie, G.A.; Hill, P.C.; Jeffries, D.J.; Ndiaye, M.; Sahito, S.M.; Hossain, I.; Uchendu, U.; Ameh, D.; Adeyemi, O.; et al. Impact of the introduction of pneumococcal conjugate vaccination on invasive pneumococcal disease and pneumonia in The Gambia: 10 years of population-based surveillance. Lancet Infect. Dis. 2021, 21, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Invasive pneumococcal disease. In Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Republic of Slovenia, Statistical Office. Population, Slovenija. 2022. Available online: https://www.stat.si/StatWeb/en/News/Index/10697 (accessed on 17 February 2023).
- WHO Collaborating Centre for Drug Statistics. Methodology, ATC/DDD Index 2023. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 17 February 2023).
- Cizman, M.; Paragi, M.; Jovan-Kuhar, N.; Gubina, M.; Orazem, A.; Pokorn, M. Antimicrobial resistance of invasive Streptococcus pneumoniae in Slovenia, 1993-1995. The Slovenian Meningitis Study Group. Scand. J. Infect. Dis. 1997, 29, 251–254. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 12.0; European Committee: Brussels, Belgium, 2022. [Google Scholar]
- R Core Team, R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | J01 DID | J01C DID | J01CR DID | J01FA DID | J01FA-FA1 DID | J01 RxIDs | J01C RxIDs | J01CR RxIDs | J01FA RxIDs | J01FA-FA1 RxIDs |
|---|---|---|---|---|---|---|---|---|---|---|
| 2015 | 11.9 | 6.97 | 2.98 | 1.63 | 1.54 | 524.4 | 313.0 | 140.6 | 80.4 | 75.1 |
| 2016 | 11.5 | 6.79 | 2.83 | 1.36 | 1.28 | 494.4 | 299.2 | 133.4 | 66.3 | 62.1 |
| 2017 | 11.6 | 6.87 | 2.89 | 1.46 | 1.38 | 485.4 | 291.2 | 134.8 | 64.5 | 60.4 |
| 2018 | 11.7 | 6.87 | 2.85 | 1.55 | 1.46 | 480.6 | 285.9 | 133.3 | 64.7 | 60.0 |
| 2019 | 11.5 | 6.71 | 2.86 | 1.51 | 1.41 | 470.0 | 276.7 | 132.3 | 63.1 | 57.5 |
| 2020 | 8.8 | 4.7 | 2.36 | 1.22 | 1.17 | 357.6 | 191.6 | 118.9 | 47.5 | 45.1 |
| 2021 | 8.7 | 4.6 | 2.48 | 1.02 | 0.99 | 358.6 | 189.5 | 113.6 | 34.4 | 33.1 |
| Year | Resistance to Penicillin% (Number of Resistant Isolates/All) | Resistance to Macrolides % (Number of Resistant Isolates/All) |
|---|---|---|
| 2015 | 9.1 (30/329) | 18.8 (62/329) |
| 2016 | 7.9 (22/279) | 15.1 (42/279) |
| 2017 | 10.1 (33/328) | 13.4 (44/328) |
| 2018 | 10.1 (28/276) | 10.9 (30/276) |
| 2019 | 12.3 (35/284) | 9.9 (28/284) |
| 2020 | 14.6 (26/178) | 13.5 (24/178) |
| 2021 | 6.3 (12/189) | 7.4 (14/189) |
| 2022 | 6.8 (15/220) | 8.2 (18/220) |
| Country (Antibiotic) | Consumption of Antibiotics (J01) and Macrolides (J01FA) in DID | Consumption (2019–2021) | Resistance of S. pneumoniae to Penicillin and Macrolides in % | Resistance (2019–2021) | |||||
|---|---|---|---|---|---|---|---|---|---|
| 2019 | 2020 | 2021 | Δ% | 2019 | 2020 | 2021 | Δ% | ||
| Slovenia (J01) | 11.50 | 8.80 | 8.70 | −24.4 | Penicillin | 12.30 | 14.60 | 6.30 | −48.8 |
| (J01FA) | 1.51 | 1.22 | 1.02 | −32.5 | Macrolides | 9.90 | 13.50 | 7.40 | −25.3 |
| Sweden (J01) | 9.60 | 8.20 | 8.01 | −16.6 | Penicillin | 6.90 | 8.30 | 6.30 | −8.7 |
| (J01FA) | 0.25 | 0.25 | 0.22 | −12.0 | Macrolides | 6.50 | 6.50 | 4.80 | −26.2 |
| Denmark (J01) | 13.40 | 12.50 | 12.60 | −6.0 | Penicillin | 4.90 | 7.20 | 10.10 | +106.1 |
| (J01FA) | 1.41 | 1.15 | 1.11 | −21.3 | Macrolides | 3.40 | 3.60 | 5.00 | +47.0 |
| The Netherlands (J01) | 8.70 | 7.70 | 7.60 | −12.7 | Penicillin | 4.00 | 4.80 | 6.20 | +55.0 |
| (J01FA) | 1.22 | 1.13 | 1.07 | −30.5 | Macrolides | 4.80 | 3.50 | 3.30 | −31.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kastrin, T.; Mioč, V.; Mahnič, A.; Čižman, M.; Slovenian Meningitidis Study Group. Impact of the COVID-19 Pandemic on Community Consumption of Antibiotics for Systemic Use and Resistance of Invasive Streptococcus pneumoniae in Slovenia. Antibiotics 2023, 12, 945. https://doi.org/10.3390/antibiotics12060945
Kastrin T, Mioč V, Mahnič A, Čižman M, Slovenian Meningitidis Study Group. Impact of the COVID-19 Pandemic on Community Consumption of Antibiotics for Systemic Use and Resistance of Invasive Streptococcus pneumoniae in Slovenia. Antibiotics. 2023; 12(6):945. https://doi.org/10.3390/antibiotics12060945
Chicago/Turabian StyleKastrin, Tamara, Verica Mioč, Aleksander Mahnič, Milan Čižman, and Slovenian Meningitidis Study Group. 2023. "Impact of the COVID-19 Pandemic on Community Consumption of Antibiotics for Systemic Use and Resistance of Invasive Streptococcus pneumoniae in Slovenia" Antibiotics 12, no. 6: 945. https://doi.org/10.3390/antibiotics12060945