
Mucormycosis in COVID-19 Patients: A Case-Control Study

 , , , ,
, , , ,
Abstract
:1. Introduction
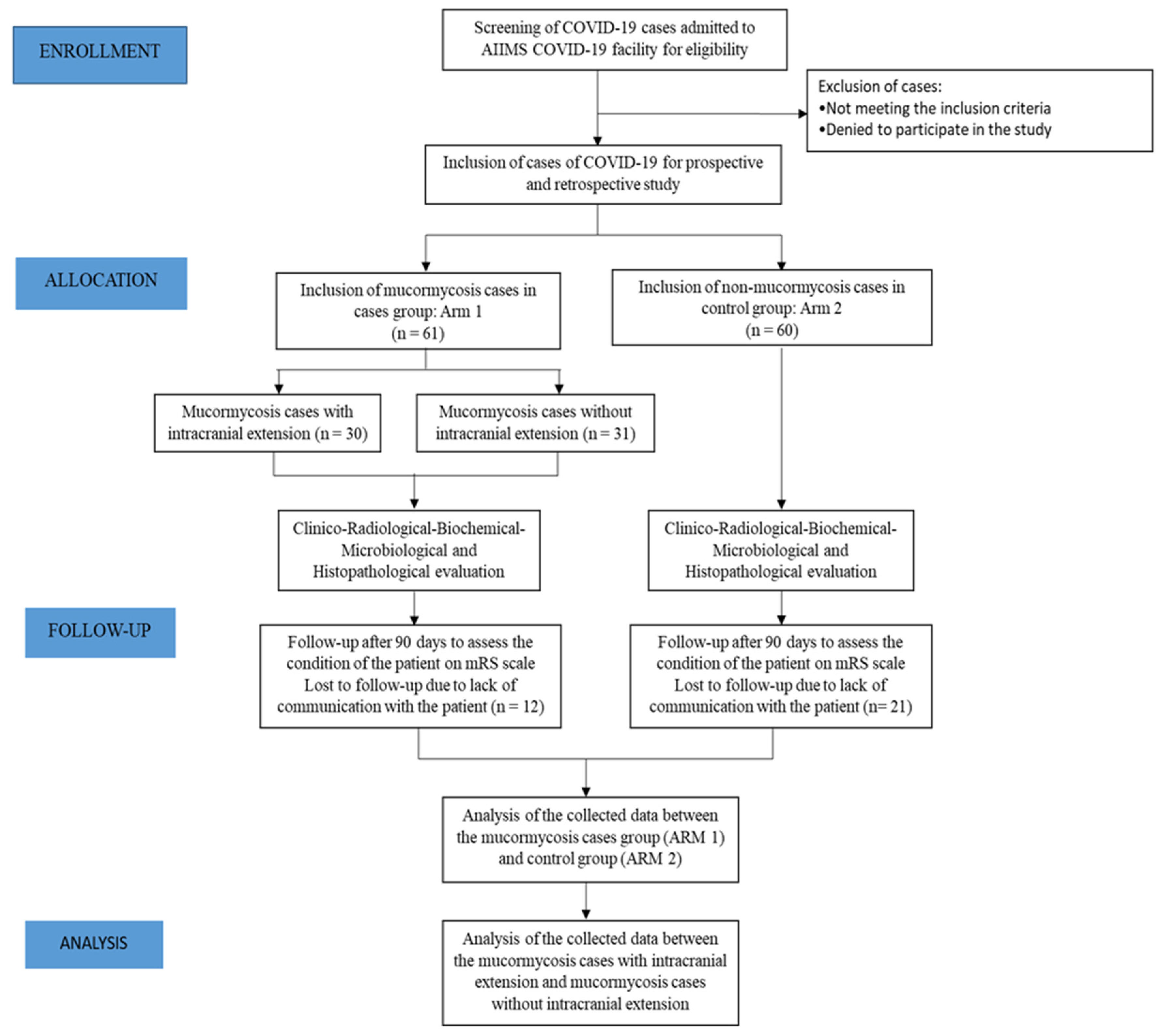
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chikley, A.; Ben-Ami, R.; Kontoyiannis, D.P. Mucormycosis of the Central Nervous System. J. Fungi 2019, 5, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revannavar, S.M.; Supriya, P.S.; Samaga, L.; Vineeth, V.K. COVID-19 triggering mucormycosis in a susceptible patient: A new phenomenon in the developing world? BMJ Case Rep. CP 2021, 14, e241663. [Google Scholar] [CrossRef] [PubMed]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. Epidemiology and diagnosis of mucormycosis: An update. J. Fungi 2020, 6, 265. [Google Scholar] [CrossRef] [PubMed]
- Padma Srivastava, M.V.; Vishnu, V.Y.; Pandit, A.K. Mucormycosis Epidemic and Stroke in India During the COVID-19 Pandemic. Stroke 2021, 52, 622–623. [Google Scholar] [CrossRef] [PubMed]
- Raut, A.; Huy, N.T. Rising incidence of mucormycosis in patients with COVID-19: Another challenge for India amidst the second wave? Lancet Respir. Med. 2021, 9, e77. [Google Scholar] [CrossRef]
- Singh, P. Black fungus: Here is a list of states with highest number of mucormycosis cases. Hindustan Times, 28 May 2021. Available online: https://www.hindustantimes.com/india-news/black-fungus-states-with-highest-number-of-mucormycosis-cases-101621559394002.html (accessed on 22 April 2022).
- Banerjee, I.; Robinson, J.; Asim, M.; Sathian, B.; Banerjee, I. Mucormycosis and COVID-19 an epidemic in a pandemic? Nepal J. Epidemiol. 2021, 11, 1024. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Singh, R.; Joshi, S.R.; Mishra, A. Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102146. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.H. Acquisition, transport, and storage of iron by pathogenic fungi. Clin. Microbiol. Rev. 1999, 12, 394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantadakis, E.; Samonis, G. Clinical presentation of zygomycosis. Clin. Microbiol. Infect. 2009, 15, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terry, A.R.; Kahle, K.T.; Larvie, M.; Vyas, J.M.; Stemmer-Rachamimov, A. Case 5-2016: A 43-Year-Old Man with Altered Mental Status and a History of Alcohol Use. N. Engl. J. Med. 2016, 374, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, J.; Thada, P.K.; Nagalli, S. Rhinocerebral Mucormycosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK559288/ (accessed on 20 May 2022).
- Spellberg, B.; Edwards, J., Jr.; Ibrahim, A. Novel perspectives on mucormycosis: Pathophysiology, presentation, and management. Clin. Microbiol. Rev. 2005, 18, 556–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratre, B.; Kumar, B.; Garg, R.; Vig, S.; Pandit, A.; Bhopale, S.; Bhatnagar, S. Challenges faced in the conversion of a tertiary healthcare centre into a COVID-19 hospital and developing a free-standing isolation centre in India. Int. J. Infect. Control 2022, 18. [Google Scholar] [CrossRef]
- Banks, J.L.; Marotta, C.A. Outcomes Validity and Reliability of the Modified Rankin Scale: Implications for Stroke Clinical Trials. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ICMR Guideline. ADVISORY Newer Additional Strategies for COVID-19 Testing. 2020. Available online: https://www.mohfw.gov.in/pdf/AdvisoryonstrategyforCOVID19TestinginIndia.pdf (accessed on 20 May 2022).
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. 22 November 2021. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 22 April 2022).
- Bala, K.; Chander, J.; Handa, U.; Punia, R.S.; Attri, A.K. A prospective study of mucormycosis in north India: Experience from a tertiary care hospital. Med. Mycol. 2015, 53, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, T.M.; Jacob, C.N.; Kontoyiannis, D.P. When Uncontrolled Diabetes Mellitus and Severe COVID-19 Converge: The Perfect Storm for Mucormycosis. J. Fungi 2021, 7, 298. [Google Scholar] [CrossRef] [PubMed]
- Prakash, H.; Chakrabarti, A. Epidemiology of Mucormycosis in India. Microorganisms 2021, 9, 523. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-F.; Zhang, Z.; Pan, X.-L.; Xing, G.-L.; Zhang, Y.; Liu, Z.-S.; Tu, S.-H. The chronic kidney disease and acute kidney injury involvement in COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0244779. [Google Scholar] [CrossRef] [PubMed]
- Prompetchara, E.; Ketloy, C.; Palaga, T. Immune responses in COVID-19 and potential vaccines: Lessons learned from SARS and MERS epidemic. Asian Pac. J. Allergy Immunol. 2020, 38, 1–9. [Google Scholar] [PubMed]
- Madeleine, V.P.; Nosratola, D.V. Chapter 24—Immune Function in Chronic Kidney Disease. In Chronic Renal Disease; Academic Press: Cambridge, MA, USA, 2015; pp. 285–297. [Google Scholar] [CrossRef]
- He, J.; Sheng, G.; Yue, H.; Zhang, F.; Zhang, H.L. Isolated pulmonary mucormycosis in an immunocompetent patient: A case report and systematic review of the literature. BMC Pulm. Med. 2021, 21, 138. [Google Scholar] [CrossRef] [PubMed]
- Dave, T.V.; Nair, A.G.; Hegde, R.; Vithalani, N.; Desai, S.; Adulkar, N.; Kamal, S.; Mittal, R.; Bradoo, R.A. Clinical Presentations, Management and Outcomes of Rhino-Orbital-Cerebral Mucormycosis (ROCM) Following COVID-19: A Multi-Centric Study. Ophthal. Plast. Reconstr. Surg. 2021, 37, 488. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Variable | Cases | Control | p-Value |
|---|---|---|---|---|
| 1. | Age in years (Median (IQR)) | (58/61) Median (IQR) = 49 (43–59) | (60/60) Median (IQR) = 38 (29–55.5) | 0.0008 |
| 2. | Sex | Male (38/58) 65.5% | Male (40/60) 66.6% | 0.895 |
| Female (20/58) 34.4% | Female (20/60) 33.3% | |||
| 3. | Diabetes | (48/56) 85.71% | (3/43) 6.98% | <0.0001 |
| 4. | Hypertension | (17/56) 30.36% | (8/43) 18.60% | 0.186 |
| 5. | Obesity | (4/25) 16% | (1/43) 2.3% | 0.06 |
| 6. | Smoking | (10/56) 17.86% | (2/43) 4.65% | 0.063 |
| 7. | Alcohol | (7/56) 12.5% | (4/43) 9.30% | 0.752 |
| 8. | Zinc | (8/9) 88.89% | (27/42) 64.29% | 0.178 |
| 9. | Vitamin C | (12/15) 80% | (38/42) 90.48% | 0.299 |
| 10. | Steroid | (30/52) 57.70% | (23/43) 53.49% | 0.681 |
| 11. | Oxygen (In-hospital and/or pre-hospitalization) | (30/56) 53.58% | (14/43) 32.56% | 0.039 |
| 12. | Steam Inhalation | (40/56) 71.43% | (27/42) 64.29% | 0.452 |
| 13. | Vaccination | (16/33) 48.48% | (37/42) 80.09% | 0.000 |
| 14. | Total Leukocyte Count | (55/61) Median (IQR) = 9930 (6200–12010) | (54/60) Median (IQR) = 6720 (5360–10900) | 0.009 |
| 15. | Polymorphonuclear leukocytes (%) | (55/61) Median (IQR) = 79.5 (69.5–85.8) | (54/60) Median (IQR) = 70.8 (60.3–82) | 0.020 |
| 16. | Lymphocytes (%) | (55/61) Median (IQR) = 13 (8–20.8) | (54/60) Median (IQR) = 21.25 (9.6–30.2) | 0.002 |
| 17. | Absolute Lymphocyte Count | (55/61) Median (IQR) = 1153.44 (900.9–1334.64) | (54/60) Median (IQR) = 1174.69 (852.72–2049.52) | 0.29 |
| 18. | Eosinophils (%) | (55/61) Median (IQR) = 1 (0.4–1.9) | (54/61) Median (IQR) = 0.2 (0–0.8) | <0.0001 |
| 19. | Urea | (55/61) Median (IQR) = 38 (23.5–57.8) | (55/60) Median (IQR) = 25 (17–32) | 0.0001 |
| 20. | Creatinine | (55/61) Median (IQR) = 0.8 (0.64–1.53) | (55/60) Median (IQR) = 0.8 (0.6–0.9) | 0.02 |
| 21. | Sodium | (55/61) Median (IQR) = 135 (133–138) | (55/60) Median (IQR) = 139 (138–141) | <0.0001 |
| 22. | D-dimer | (55/61) Median (IQR) = 396 (264–732) | (50/60) Median (IQR) = 283.30 (251.01–466.59) | 0.04 |
| 23. | Ferritin | (50/61) Median (IQR) = 1110.5 (529–1650) | (52/60) Median (IQR) = 385.60 (169–741.5) | <0.0001 |
| 24. | Procalcitonin | (55/61) Median (IQR) = 0.27 (0.08–2) | (52/60) Median (IQR) = 0.04 (0.02–0.10) | <0.0001 |
| 25. | Mortality rate after 90 days | (15/49) 30.61% | (2/39) 5.13% | 0.003 |
| 26. | Poor outcome (after 90 days) | (16/49) 32.66% | (2/39) 5.13% | 0.001 |
| S. No. | Symptoms | Percentage of Patients with the Symptom |
|---|---|---|
| 1. | Fever | 8.93 |
| 2. | Headache | 44.64 |
| 3. | Facial swelling | 42.86 |
| 4. | Swelling of eyes | 51.92 |
| 5. | Diminution of vision | 38.18 |
| 6. | Facial pain | 71.43 |
| 7. | Eye pain | 28.57 |
| 8. | Ptosis | 9.09 |
| 9. | Ulceration | 3.57 |
| 10. | Nasal discharge | 8.93 |
| 11. | Facial paralysis | 1.79 |
| Various forms of intracranial involvement | Percentage of patients displaying this form of involvement | |
| 1. | Infarct | 33.33 |
| 2. | Haemorrhage | 6.66 |
| 3. | Abscess | 10.0 |
| 4. | Meningitis | 6.66 |
| 5. | Thrombosis | 26.66 |
| S. No. | Variable | Cases | Control | p-Value |
|---|---|---|---|---|
| 1. | Age | (16/49) Median (IQR) = 51 (44–66.5) | (2/39) Median (IQR) = 41.5 (20–63) | 0.029 |
| 2. | Sex | Male (11/16) 68.75% | Male (21/33) 63.64% | 0.939 |
| Female (5/16) 31.35% | Female (12/33) 36.36% | |||
| 3. | Diabetes mellitus | (16/16) 100% | (25/33) 75.76% | 0.001 |
| 4. | Hypertension | (2/16) 12.50% | (14/33) 42.42% | 0.38 |
| 5. | Obesity | (2/10) 20% | (2/13) 15.38% | 0.246 |
| 6. | Smoking | (2/16) 12.50% | (6/33) 18.18% | 0.99 |
| 7. | Alcohol | (2/16) 12.50% | (5/33) 15.15% | 0.99 |
| 8. | Zinc | (0/0) | (8/9) 88.89% | - |
| 9. | Hydroxychloroquine | (2/5) 40.00% | (4/18) 22.22% | 0.93 |
| 10. | Steroid usage | (3/15) 20.00% | (23/31) 74.19% | 0.002 |
| 11. | Oxygen Inhalation | (8/16) 50.00% | (21/33) 63.64% | 0.923 |
| 12. | Steam Inhalation | (7/16) 43.75% | (31/33) 93.94% | 0.001 |
| 13. | Haemoglobin | (16/48) Mean = 11.60 ± 1.94 | (2/33) Mean = 15.15 ± 2.47 | 0.374 |
| 14. | Total Leukocyte Count | (16/48) Median (IQR) = 11300 (9435–12310) | (2/33) Median (IQR) = 6475 (2050–10900) | 0.210 |
| 15. | Polymorphonuclear leukocytes | (16/48) Median (IQR) = 79.25 (72.5–86.8) | (2/33) Median (IQR) = 55.65 (19–92.3) | 0.99 |
| 16. | Lymphocyte | (16/48) Median (IQR) = 10.6 (7.5–20.9) | (2/33) Median (IQR) = 18.8 (4.1–33.5) | 0.99 |
| 17. | Absolute Lymphocyte Count | (16/48) Median (IQR) = 1234.09 (958.33–1640.77) | (2/33) Median (IQR) = 566.82 (446.9–686.75) | 0.05 |
| 18. | Monocytes | (16/48) Median (IQR) = 4 (2.55–5.75) | (2/33) Median (IQR) = 6.55 (2.8–10.3) | 0.53 |
| 19. | Eosinophils | (16/48) Median (IQR) = 0.8 (0.1–1.35) | (2/33) 0.3 (0.1–0.5) | 0.32 |
| 20. | Platelet | (16/48) Median (IQR) = 236 (155.5–405.5) | (2/33) Median (IQR) = 211.5 (26–397) | 0.57 |
| 21. | Bilirubin | (16/48) Median (IQR) = 0.52 (0.34–0.69) | (2/34) Median (IQR) = 0.23 (0.2–0.26) | 0.10 |
| 22. | Alanine transaminase (ALT) | (16/48) Median (IQR) = 21 (17.5–43) | (2/34) Median (IQR) = 12 (9–15) | 0.06 |
| 23. | Aspartate Aminotransferase (AST) | (16/48) Median (IQR) = 25.5 (23–35.5) | (2/34) Median (IQR) = 16 (13–19) | 0.04 |
| 24. | Gamma-glutamyl Transferase (GGT) | (16/47) Median (IQR) = 59 (40.5–107) | (2/12) Median (IQR) = 22 (18–26) | 0.12 |
| 25. | Uric acid | (16/47) Mean = 4.73 ± 1.37 | (2/34) Mean = 4.9 ± 1.55 | 0.109 |
| 26. | Urea | (16/48) Median (IQR) = 44.9 (38.5–78.1) | (2/34) Median (IQR) = 29.5 (23–36) | 0.09 |
| 27. | Creatinine | (16/48) Median (IQR) = 1.2 (0.8–2.3) | (2/34) Median (IQR) = 0.6 (0.5–0.7) | 0.07 |
| 28. | Sodium | (16/48) Median (IQR) = 133.5 (132.5–138.5) | (2/34) Median (IQR) = 134.5 (131–138) | 0.78 |
| 29. | Potassium | (16/48) Median (IQR) = 4 (3.5–4.65) | (2/33) Median (IQR) = 4.1 (4–4.2) | 0.94 |
| 30. | D-dimer 1 (Baseline) | (16/48) Median (IQR) = 394 (278.5–2464) | (2/30) Median (IQR) = 2205 (1171–3239) | 0.26 |
| 31. | D-dimer 2 | (16/48) Median (IQR) = 487.5 (355.5–1043.5) | (2/20) Median (IQR) = 2240.5 (801–3680) | 0.18 |
| 32. | D-dimer 3 | (16/48) Median (IQR) = 623 (356.5–847) | (2/14) Median (IQR) = 2314 (948–3680) | 0.08 |
| 33. | LDH | (9/35) Median (IQR) = 283 (271–349) | (2/31) Median (IQR) = 257 (182–332) | 0.64 |
| 34. | Procalcitonin | (16/48) Median (IQR) = 0.16 (0.07–0.43) | (2/31) Median (IQR) = 0.96 (0.75–1.17) | 0.12 |
| 35. | Ferritin | (15/44) Median (IQR) = 1117 (486.9–1650) | (2/33) Median (IQR) = 1001.5 (602–1401) | 0.76 |
| S. No. | Variable | Mucormycosis Cases with Intracranial Involvement | Mucormycosis Cases | p-Value |
|---|---|---|---|---|
| 1. | Age | 30/56 Median (IQR) = 46 (44–54) | 26/56 Median (IQR) = 52 (43–64) | 0.190 |
| 2. | Sex | Male (18/30) 60% | Male (18/26) 69.230% | 0.473 |
| Female (12/30) 40% | Female (8/26) 30.769% | |||
| 3. | Diabetes | (24/28) 85.7% | (23/26) 88.4% | 0.764 |
| 4. | Hypertension | (11/28) 39.2% | (6/26) 23.0% | 0.204 |
| 5. | Obesity | (3/14) 21.4% | (1/11) 9.1% | 0.604 |
| 6. | Smoking | (2/28) 7.1% | (8/26) 30.7% | 0.037 |
| 7. | Alcohol | (1/28) 3.5% | (5/26) 19.2% | 0.095 |
| 8. | Vitamin C | (6/8) 75% | (6/7) 85.7% | 0.609 |
| 9. | Steroid | (11/25) 44% | (18/25) 72% | 0.048 |
| 10. | Oxygen | (14/28) 50% | (14/26) 53.8% | 0.778 |
| 11. | Steam Inhalation | (19/28) 67.8% | (20/26) 76.9% | 0.459 |
| 12. | Vaccination | (7/16) 43.7% | (9/15) 60% | 0.368 |
| 13. | Total Leukocyte Count | (28/30) Median (IQR) = 9990 (5830–11820) | (25/26) Median (IQR) = 9040 (6640–11900) | 0.89 |
| 14. | Polymorphonuclear leukocytes | (28/30) Median (IQR) = 78.25 (69.55–84.5) | (25/26) Median (IQR) = 79 (68.6–83.9) | 0.82 |
| 15. | Lymphocytes | (28/30) Median (IQR) = 12.25 (8.3–20.2) | (25/26) Median (IQR) = 13 (9–20.8) | 0.93 |
| 16. | Absolute Lymphocyte Count | (28/30) Median (IQR) = 1126.8 (953.35–1453.57) | (25/26) Median (IQR) = 1155 (844.9–1333.8) | 0.71 |
| 17. | Eosinophils | (28/30) Median (IQR) = 1 (0.45–2.05) | (25/26) Median (IQR) = 0.9 (0.4–1.5) | 0.56 |
| 18. | Urea | (28/30) Median (IQR) = 34 (22.45–55.4) | (25/26) Median (IQR) = 38 (30–47) | 0.71 |
| 19. | Creatinine | (28/30) Median (IQR) = 0.82 (0.62–1.45) | (25/26) Median (IQR) = 0.8 (0.65–1.37) | 0.92 |
| 20. | Sodium | (28/30) Median (IQR) = 134.5 (132.5–138) | (25/26) Median (IQR) = 136 (133–138) | 0.59 |
| 21. | D-dimer | (28/30) Median (IQR) = 416.5 (275.5–1563.5) | (25/26) Median (IQR) = 347 (243–721) | 0.27 |
| 22. | Ferritin | (28/30) Median (IQR) = 973.05 (499.4–1648.5) | (20/26) Median (IQR) = 1116.5 (752.35–1393.85) | 0.87 |
| 23. | Procalcitonin | (28/30) Median (IQR) = 0.26 (0.08–1.15) | (25/26) Median (IQR) = 0.35 (0.08–2) | 0.98 |
| 24. | Mortality rate after 90 days | (10/26) 38.4% | (5/21) 23.8% | 0.288 |
| 25. | Poor outcome (after 90 days) | (11/26) 42.3% | (5/21) 23.8% | 0.188 |
| S. No. | Variable | Univariable Analysis | Multivariable Analysis |
|---|---|---|---|
| Mucormycosis cases vs. controls | |||
| 1. | Creatinine | OR 2.876; 95% CI (1.264–6.542); p = 0.012 | OR 4.963; 95% CI (1.456–16.911); p = 0.010 |
| 2. | D-dimer | OR 1.0007; 95% CI (1.0001–1.0012); p = 0.018 | OR 1.00089l 95% CI (1.000097–1.0017); p = 0.028 |
| Poor outcome after 90-day follow-up | |||
| 1. | Steroid | OR 0.132; 95% CI (0.034–0.506); p = 0.002 | OR 0.07; 95% CI (0.012–0.414); p = -0.003 |
| 2. | Steam Inhalation | OR 0.134; 95% CI (0.043–0.416); p = 0.001 | OR 0.034; 95% CI (0.003–0.391); p = 0.007 |
| 3. | Diabetes mellitus | OR 12.741; 95% CI (2.713–59.833); p = 0.001 | OR 26.919; 95% CI (1.666–434.892); p = 0.020 |
| Mucormycosis cases vs. mucormycosis cases with intracranial extension | |||
| 1. | Smoking | OR 0.173 (95% CI 0.033–0.912); p = 0.037 | OR 0.08; 95% CI (0.009–0.754); p = 0.027 |
| S No. Author, Year | Age | Gender | Case Description | Investigations | Treatment and Outcome |
|---|---|---|---|---|---|
| 1. Revannavar SM et al., 2021 | Middle-aged | Female | Newly detected DM, left eye ptosis, facial pain—days, fever—3 days, tenderness of all left sinuses, left complete ophthalmoplegia, and reduced visual acuity (6/36). | HbA1c—13.39%, admission glucose 378 mg/dl without ketosis. CT PNS—complete opacification of left ethmoid, maxillary, and frontal sinuses. MRI brain—acute infarct in left parietooccipital lobe with subperiosteal abscess. No ICA thrombus, left ICA showed periarterial inflammation | Conventional amphotericin B for 11 days, aspirin, and FESS. CT showed on follow-up reduction in paranasal sinus opacification. |
| 2. Yukiko Maeda, et al., 2021 | 73 years | Sudden onset left arm weakness and dysarthria. Two months prior had nausea, vomiting, and diplopia with right-side facial pain. NIHSS 13 Past: uncontrolled DM (HbA1C 9.1%) and chronic sinusitis | CT PNS—Mass in right nasal cavity with bony destruction. MRI—acute infarct right frontal lobe, severe right ICA stenosis with thrombus, also cavernous sinus invasion with mass. | Confirmed mucor by PCR. Treated with amphotericin B, capsofungin acetate, and flucytosine. One year follow patient alive. | |
| 3. Vidya Krishna et al., 2021 | 22 years | Male | BMI-44, hypothyroidism, severe COVID pneumonitis, acute ACA territory infarct | Day 11—CT pulmonary angiogram showed segmental pulmonary embolism, CT Head—right ACA infarct with petechial hemorrhages, | Aspirin, LMWH, HCQs, azithromycin, steroids, hemodialysis, meropenem, teicoplanin, argatroban (on event of PE). Died in day 20 with terminal pericarditis, cardiac tamponade, hypotension. Autopsy—disseminated mucormycosis involving lungs, pericardium, lymph nodes, and brain along with thromboembolism in lung, brain, pharynx, nasal mucosa, and trachea. |
| 4. Nehara HR et al., 2021 | 59 years | Female | Headache, ptosis, chemosis, ptosis, loss of vision, complete ophthalmoplegia, nasal black discharge, hard palate black crust | PNS—bilateral maxillary, ethmoid, left frontal and sphenoid sinusitis, cavernous sinus thrombosis | Liposomal amphotericin B, antibiotics. Patient died. |
| 68 years | Female | Headache, facial swelling, ptosis, lid edema, loss of vision, complete ophthalmoplegia nasal black discharge, black crust hard palate | Orbital cellulitis, endophthalmitis, cavernous sinus thrombosis, pansinusitis, multiple lacunar infarcts | Liposomal amphotericin, antibiotics. Patient died | |
| 5. Werthman et al., 2020 | 33 years | Female | Left ptosis proptosis, complete ophthalmoplegia, and altered sensorium with diabetic ketoacidosis | Maxillary and ethmoid sinusitis, MRI brain multiple infarction | Surgical debridement and amphotericin B. Patient died |
| 6. Sen M et al., 2021 N= 2826 | 285 cases (10.1%) with cavernous sinus thrombosis or invasion 95 cases (3.4 %) with ICA stenosis or occlusion | Hemiparesis, altered consciousness, and focal seizures indicating brain invasion and infarction | Surgery, amphotericin B and posaconazole/isavuconazole | ||
| 7. Davide cesrati et al., 2020 | 47 years | Female | Obese women with respiratory problems and COVID 19, worsening respiratory failure, partial left hemispheric syndrome | HRCT scan of her thorax revealed diffuse ground-glass opacities in both lungs, brain CT showed subtle low attenuation within the right insular ribbon and frontal lobe, CT demonstrated large bilateral infarctions of both the cerebellar and cerebral hemisphere | Mechanical thrombectomy could not be performed, patient died after 1 day of witnessing infarctions of both the cerebellar and cerebral hemisphere |
| 8. A patel et al., 2020 | observational study with 465 patients. | Rhino-orbital mucormycosis was the most common (315/465, 67.7%) presentation followed by pulmonary (62/465, 13.3%), cutaneous (49/465, 10.5%), and others. | Amphotericin B was the primary therapy in 81.9% (381/465), and posaconazole was used as combination therapy in 53 (11.4%) individuals | ||
| 9. Rahul Kulkarni et al., 2021 | 49 patients with cerebrovascular involvement were included. Rhino-orbito-cerebral involvement was the most common form of presentation (98%) | Cerebrovascular involvement was seen in 11.8% patients of COVID-associated mucormycosis patients. Type of stroke—infarct, hemorrhage, abscess | Amphotericin B with oral triazoles | ||
| 10. Pal et al., 2021 | Systematic review with 30 case series/ case reports by pooling data from 99 patients with COVID associated mucormycosis | Diabetes mellitus and hypertension were present in patients as co-morbidities. All of the included patients had a history of COVID-19 infection | Parenteral dexamethasone was most commonly used glucocorticoid. Out of the 96 cases followed up, 33 (34%) were dead, only 63 (66%) patients were alive | ||
| 11. Garg Deepak et al., 2021 | 55-year-old Male | End-stage kidney disease, diabetes, COVID-19, and pulmonary mucormycosis. Eight cases of COVID-19-associated mucormycosis included in the review | For treatment received 5 g of liposomal amphotericin B | ||
| 12. Dilek A. et al., 2021 | Case report and systematic review with 30 publications describing 100 patients. 54 years old Male | A 54-year-old male was hospitalized due to severe COVID-19 pneumonia. Common risk factors were corticosteroid use, hypertension, and diabetes. | A 54-year-old male died of sepsis. Death was observed in 33 out of 99 patients. Medical and surgical treatment was given to patients | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandit, A.K.; Tangri, P.; Misra, S.; Srivastava, M.V.P.; Bhatnagar, S.; Thakar, A.; Sikka, K.; Panda, S.; Vishnu, V.Y.; Singh, R.K.; et al. Mucormycosis in COVID-19 Patients: A Case-Control Study. Microorganisms 2022, 10, 1209. https://doi.org/10.3390/microorganisms10061209
Pandit AK, Tangri P, Misra S, Srivastava MVP, Bhatnagar S, Thakar A, Sikka K, Panda S, Vishnu VY, Singh RK, et al. Mucormycosis in COVID-19 Patients: A Case-Control Study. Microorganisms. 2022; 10(6):1209. https://doi.org/10.3390/microorganisms10061209
Chicago/Turabian StylePandit, Awadh Kishor, Poorvi Tangri, Shubham Misra, Madakasira Vasantha Padma Srivastava, Sushma Bhatnagar, Alok Thakar, Kapil Sikka, Smriti Panda, Venugopalan Y. Vishnu, Rajesh Kumar Singh, and et al. 2022. "Mucormycosis in COVID-19 Patients: A Case-Control Study" Microorganisms 10, no. 6: 1209. https://doi.org/10.3390/microorganisms10061209