
Attitudes toward COVID-19 Vaccines among Patients with Complex Non-Communicable Disease and Their Caregivers in Rural Malawi

 ,
, 
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design and Study Population
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Demographic Characteristics, Vaccine Uptake, and Intention to Vaccinate
3.2. Reasons to Not Be Vaccinated
“…Some people will die within a few years. Others will become disabled. Others will be so sick after the vaccine...”
“…The vaccine was meant to reduce the population of people in the world...”
“…Those with non-communicable diseases, they will get very sick if they receive the vaccine….”
“…She is expectant, the clinician advised not to get the jab….”
“…People are saying that there are special vaccines for the medical team and the local people….”
“…The vaccine is a symbol of 666, which is associated with Satanism….”
“…People who were vaccinated are also getting sick, therefore the vaccine is useless.”
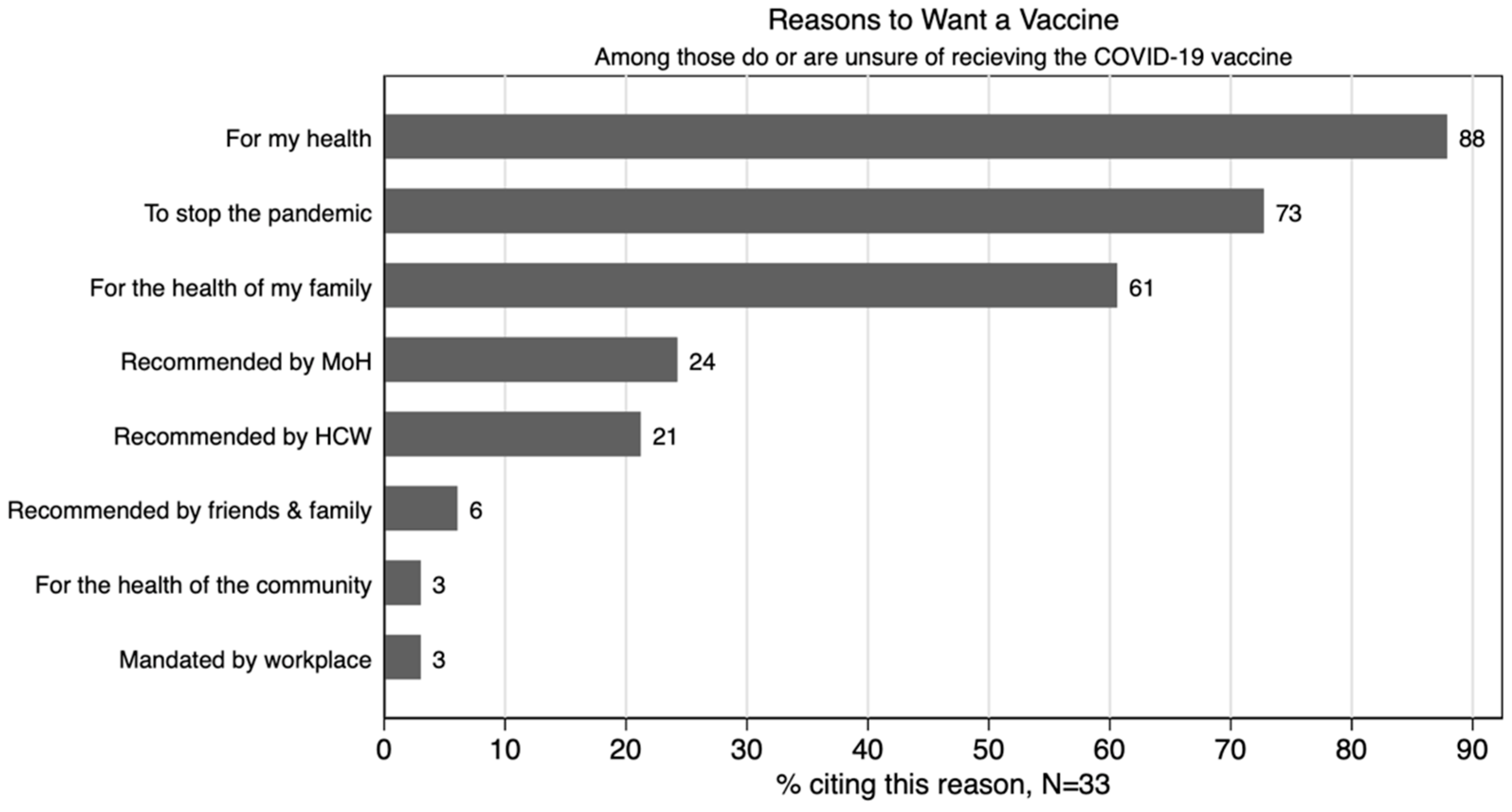
3.3. Reasons to Accept the COVID-19 Vaccine
“…I was very impressed with the message from health officers that [for] patients with NCDs the immune system is deficient. Once they get infected with the disease, they will be critically ill and possibly lose their life….”
“…She has been impressed by people who got the jab. They are okay. No side effects as some people have been speculating….”
“…there is a need for the health personnel to come to them with a strong message about the vaccine….”
“…he is not feeling any side effects after getting the jab as speculated by other people. He is the village headman; many people in his village are willing to be vaccinated...”
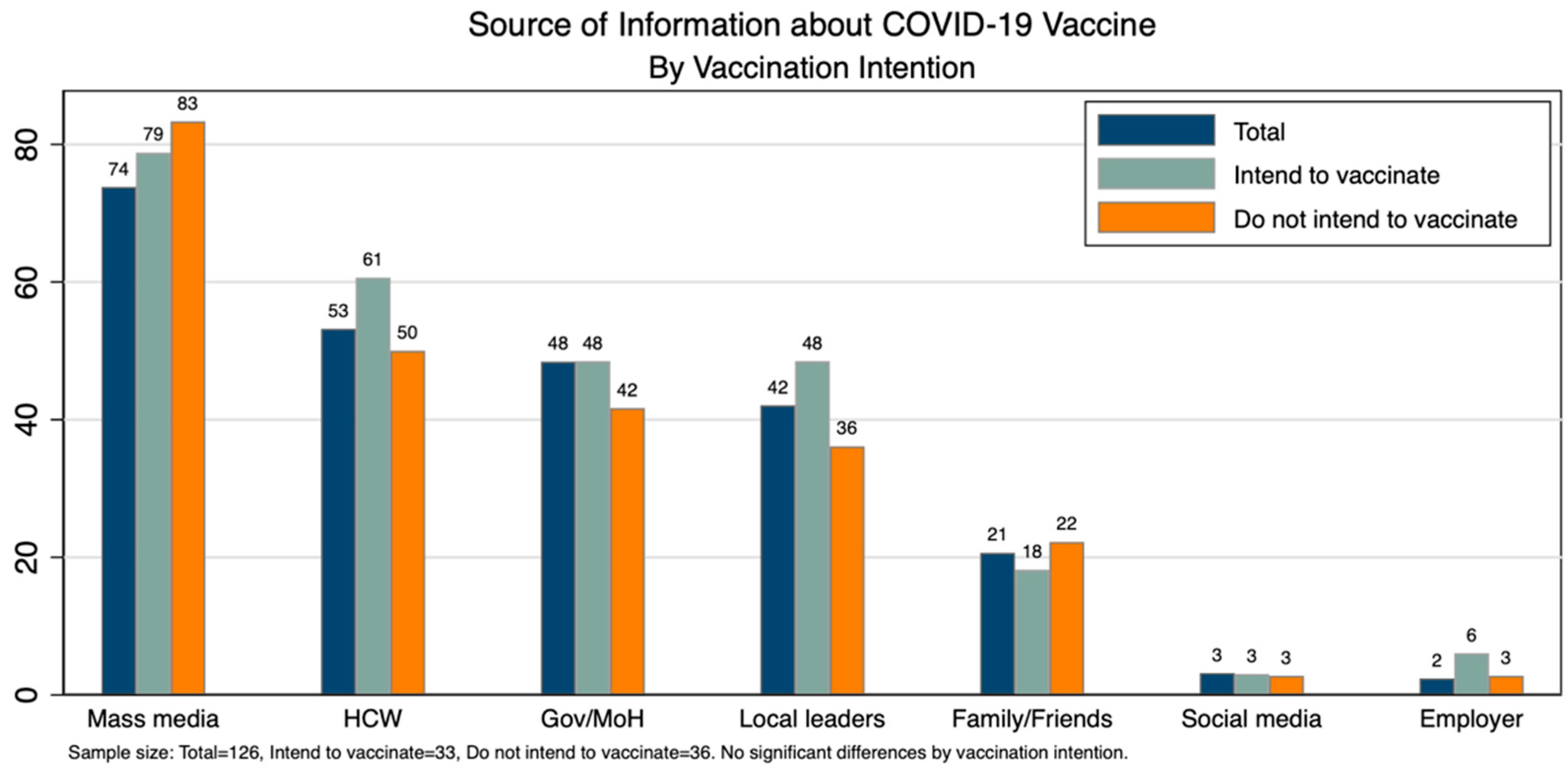
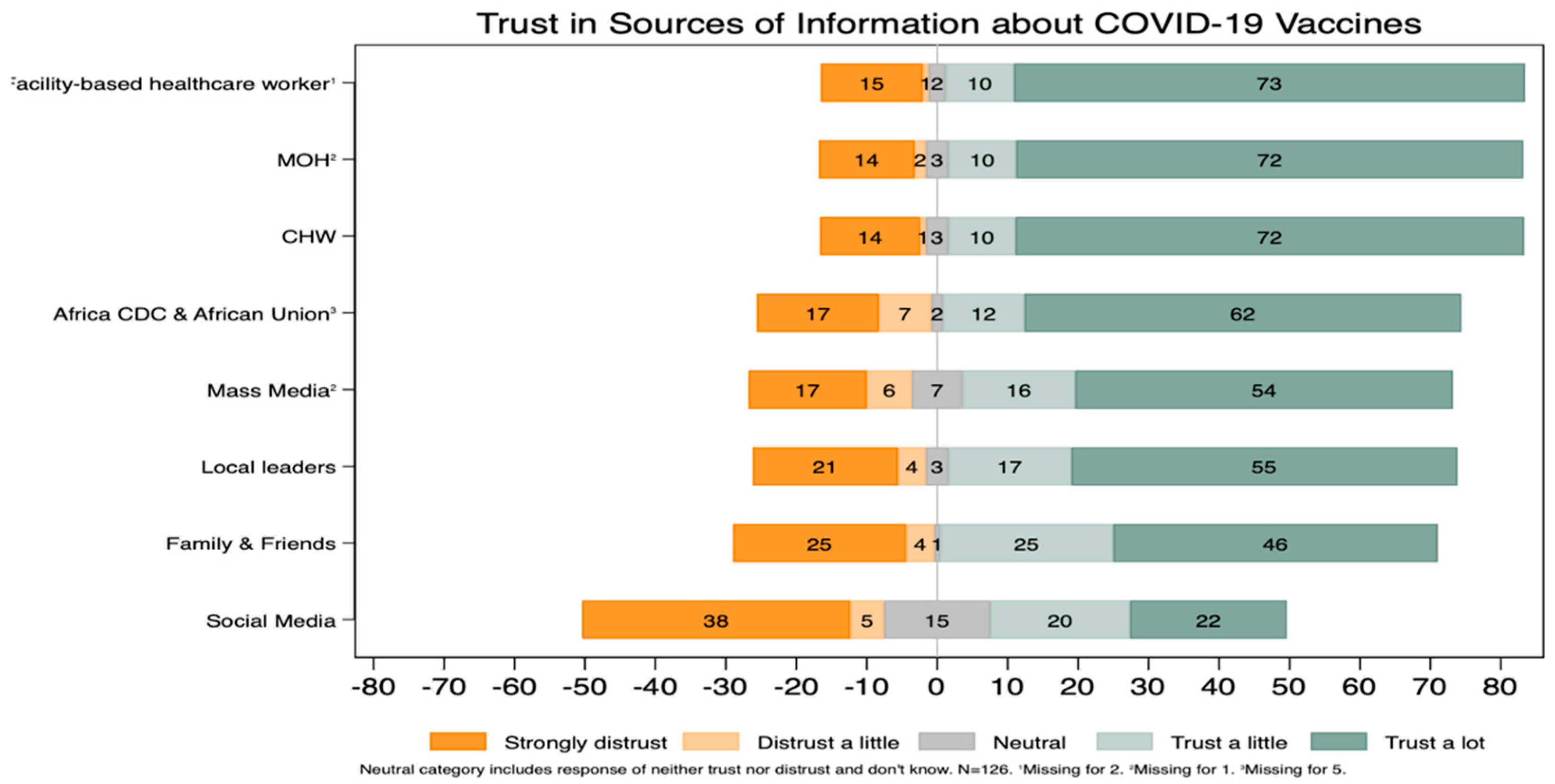
3.4. Sources of Information about the COVID-19 Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- 1.
- Have you ever had the opportunity to receive a vaccine for COVID-19?
- Yes
- No
- 2.
- Have you ever received a vaccine for COVID-19?
- Yes
- No
- 2a.
- Which COVID-19 vaccine did you receive?
- AstraZeneca/Oxford
- Johnson & Johnson/Janssen
- Pfizer
- Don’t know
- 2b.
- [if 2a! = Johsnon & Johnson]. Have you received two doses of the COVID-19 vaccine?
- Yes
- No
- Don’t know
- 3.
- [if 2 = “No”] Why did you not receive COVID-19 vaccine when it was offered to you?Select all that are mentioned. Do not read specific items, but you can prompt the respondent with “Any other reasons?Logistics concerns☐ No transport☐ Too expensivePerceived risk of COVID-19☐ COVID-19 is not dangerous or does not exist☐ I am not personally at risk of COVID-19☐ I have already been infected with COVID-19COVID-19 vaccine☐ The COVID-19 vaccine is unsafe or has side effects☐ The COVID-19 vaccine has not been tested enough☐ The COVID-19 vaccine is not effective at stopping infection☐ The COVID-19 vaccine is specifically designed to harm me (e.g., conspiracy theory)☐ I have concerns about specific type(s) of COVID-19 vaccineTrust☐ Lack of trust in national government☐ Lack of trust in international donors/foreign governments☐ Lack of trust in vaccine manufacturesOther Specify other:_______________________[if 1 = Yes] We understand that you previously had the opportunity to be vaccinated against COVID-19. However, some people’s opinions about vaccination can change over time.”[if 2 = Yes] For the next set of questions, we would like you to imagine that you had never received any doses of the COVID-19 vaccine before today.
- 4.
- If an approved vaccine to prevent COVID-19 was available to you today at no cost, would you agree to be vaccinated?
- Yes
- No
- Not sure/It depends
- 5.
- [if 4 = No or 4 = Not sure/It depends] What are some of the reasons you would not want to be vaccinated?Select all that are mentioned. Do not read specific items, but you can prompt the respondent with “Any other reasons?” Until they have nothing to say.Perceived risks of COVID-19☐ COVID-19 is not dangerous or does not exist☐ I am not personally at risk of COVID-19☐ I have already been infected with COVID-19COVID-19 vaccine☐ The COVID-19 vaccine is unsafe or has side effects☐ The COVID-19 vaccine has not been tested enough☐ The COVID-19 vaccine is not effective at stopping infection☐ The COVID-19 vaccine is specifically designed to harm me (e.g., conspiracy theory)☐ I have concerns about specific type(s) of COVID-19 vaccineTrust☐ Lack of trust in national government☐ Lack of trust in international donors/foreign governments☐ Lack of trust in vaccine manufactures☐ Other. Specify other:_______________________________________
- 6.
- What are the some of reasons you would want to be vaccinated?Select all that are mentioned. Do not read specific items, but prompt the respondent with “Any other reasons?” Until they have nothing to say.Perceived benefits☐ For my health☐ For the health of my family☐ For the health of the community☐ To stop the COVID-19 pandemicMandates☐ It is required by my workplace☐ It is mandated by someone elseSpecify who mandated it:_____________________________Recommendations☐ The government or ministry of health recommends it☐ A healthcare worker recommends it☐ A friend or family member recommends it☐ Someone else recommends itSpecify who recommended it:_____________________________☐ Other. Specify other: ___________________________
- 7.
- What are your primary sources of COVID-19 vaccines informationSelect all that are mentioned. Do not read specific items.☐ National government/ministry of health☐ Health care workers☐ Social media (Facebook, WhatsApp, Twitter)☐ Mass media (radio, TV, newspapers)☐ Employer☐ Local leaders and village headmans☐ Family or friendsHow much would you trust each of the following people or institutions to help you decide whether you should get a COVID vaccine? Your options are “Strongly distrust”, “Distrust a little”, “Neither trust nor distrust” “Trust a little” “Trust a lot”
- 8.
- The World Health Organization
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 9.
- The African CDC and African Union
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 10.
- The Malawi Ministry of Health
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 11.
- Facility-based health care worker
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 12.
- Community-based health care worker
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 13.
- Mass media, such as newspapers, radio, and TV
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 14.
- Local leaders and village headmen
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 15.
- Family or Friends
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 16.
- Social Media
- Strongly distrust
- Distrust a little
- Neither trust nor distrust
- Trust a little
- Trust a lot
- Don’t know
- 17.
- Do you know where to go to get a COVID-19 vaccine?
- Yes
- No
- 18.
- Where would you go to get a vaccine
- Hospital
- Health care center
- NCD clinic
- Other: _________
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 7 February 2022).
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Dyer, O. Covid-19: Unvaccinated Face 11 Times Risk of Death from Delta Variant, CDC Data Show. BMJ 2021, 374, n2282. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association between MRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, K.; Shavaleh, R.; Forouhi, M.; Disfani, H.F. Effectiveness of COVID-19 Vaccines and Post-Vaccination SARS-COV2 Infection, Hospitalization, and Mortality: A Systematic Review and Meta-Analysis of Observational Studies. medRxiv 2021. [Google Scholar] [CrossRef]
- Lewis, N.M.; Naioti, E.A.; Self, W.H.; Ginde, A.A.; Douin, D.J.; Keipp Talbot, H.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; Gaglani, M.; et al. Effectiveness of MRNA Vaccines Against COVID-19 Hospitalization by Age and Chronic Medical Conditions Burden Among Immunocompetent US Adults, March–August 2021. J. Infect. Dis. 2022, 225, 1694–1700. [Google Scholar] [CrossRef]
- Verger, P.; Dubé, E. Restoring Confidence in Vaccines in the COVID-19 Era. Expert Rev. Vaccines 2020, 19, 991–993. [Google Scholar] [CrossRef]
- Chagla, Z.; Pai, M. COVID-19 Boosters in Rich Nations Will Delay Vaccines for All. Nat. Med. 2021, 27, 1659–1660. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Gao, X.; Li, H.; He, W.; Zeng, W. COVID-19 Vaccine Hesitancy Among Medical Students: The Next COVID-19 Challenge in Wuhan, China. Disaster Med. Public Health Prep. 2021, 43, 1–6. [Google Scholar] [CrossRef]
- Africa CDC. Majority of Africans Would Take a Safe and Effective COVID-19 Vaccine; Africa CDC: Addiss Ababa, Ethiopia, 2020; Available online: https://africacdc.org/news-item/majority-of-africans-would-take-a-safe-and-effective-covid-19-vaccine (accessed on 7 February 2022).
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 Vaccine Acceptance and Hesitancy in Low- and Middle-Income Countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- United Nations Declaration of State of Disaster by Malawi President Peter Mutharika|United Nations in Malawi. Available online: https://malawi.un.org/en/46778-declaration-state-disaster-malawi-president-peter-mutharika (accessed on 7 February 2022).
- Kanyanda, S.; Markhof, Y.; Wollburg, P.; Zezza, A. The Acceptance of Covid-19 Vaccines in Sub-Saharan Africa: Evidence from 6 National Phone Surveys. BMJ Open 2021, 11, e055159. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Malawi Receives First Shipment of COVID-19 Vaccines from COVAX; UNICEF: Lilongwe, Malawi, 2021; Available online: https://www.unicef.org/malawi/press-releases/malawi-receives-first-shipment-covid-19-vaccines-covax (accessed on 7 February 2022).
- Oyekale, A.S.; Maselwa, T.C. An Instrumental Variable Probit Modeling of COVID-19 Vaccination Compliance in Malawi. Int. J. Environ. Res. Public Health 2021, 18, 13129. [Google Scholar] [CrossRef] [PubMed]
- Masina, L. Malawi Adds More COVID-19 Vaccines in Attempt to Stem Surge. VOA. 2021. Available online: https://www.voanews.com/a/covid-19-pandemic_malawi-adds-more-covid-19-vaccines-attempt-stem-surge/6208376.html (accessed on 3 December 2021).
- World Bank Rolling out COVID-19 Vaccines in Malawi Amid Hesitancy and Supply Challenges. Available online: https://www.worldbank.org/en/news/feature/2021/10/19/rolling-out-covid-19-vaccines-in-malawi-amid-hesitancy-and-supply-challenges (accessed on 11 March 2022).
- World Health Organization. Malawi Marks One Year of COVID-19 Vaccination, 828,080 People Receive Full Dose. Available online: https://www.afro.who.int/countries/malawi/news/malawi-marks-one-year-covid-19-vaccination-828-080-people-receive-full-dose (accessed on 1 April 2022).
- Government of Malawi. Neno District Council Socio-Economic Profile 2017–2022; Government of Malawi: Lilongwe, Malawi, 2020.
- NSO. Malawi National and District Population Projections 2018–2050; National Statistical Office: Zomba, Malawi, 2020; pp. 1–276.
- MOH. Malawi COVID-19 National Information Dashboard. Available online: https://covid19.health.gov.mw/ (accessed on 23 April 2022).
- Wroe, E.B.; Kalanga, N.; Mailosi, B.; Mwalwanda, S.; Kachimanga, C.; Nyangulu, K.; Dunbar, E.; Kerr, L.; Nazimera, L.; Dullie, L. Leveraging HIV Platforms to Work toward Comprehensive Primary Care in Rural Malawi: The Integrated Chronic Care Clinic. Healthcare 2015, 3, 270–276. [Google Scholar] [CrossRef] [PubMed]
- WHO PEN-Plus Meeting in Kigali–The Management and Treatment of Non-Communicable Diseases at Primary Levels Strengthened. Available online: https://www.afro.who.int/news/pen-plus-meeting-kigali-management-and-treatment-non-communicable-diseases-primary-levels (accessed on 1 February 2022).
- Wacksman, J.; Sampat, K. CommCare Fundamentals–CommCare Overview–CommCare Public–Global Site. Available online: https://confluence.dimagi.com/display/commcarepublic/CommCare+Fundamentals+-+CommCare+Overview (accessed on 23 April 2022).
- Rodriguez, V.J.; Alcaide, M.L.; Salazar, A.S.; Montgomerie, E.K.; Maddalon, M.J.; Jones, D.L. Psychometric Properties of a Vaccine Hesitancy Scale Adapted for COVID-19 Vaccination among People with HIV. AIDS Behav. 2022, 26, 96–101. [Google Scholar] [CrossRef]
- StataCorp. Statistical Software: Release 15; StataCorp: College Station, TX, USA, 2017. [Google Scholar]
- Wake, A.D. The Acceptance Rate toward COVID-19 Vaccine in Africa: A Systematic Review and Meta-Analysis. Glob. Pediatric Health 2021, 8, 2333794X211048738. [Google Scholar] [CrossRef]
- Magadmi, R.M.; Kamel, F.O. Beliefs and Barriers Associated with COVID-19 Vaccination among the General Population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Bendezu-Quispe, G.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, V.A.; Benites-Zapata, V.A. Cross-Sectional Analysis of COVID-19 Vaccine Intention, Perceptions and Hesitancy across Latin America and the Caribbean. Travel Med. Infect. Dis. 2021, 41, 102059. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.-Y.; Ho, K.-F.; Cheung, A.W.-L.; Yau, P.S.-Y.; Dong, D.; Wong, S.Y.-S.; Yeoh, E.-K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef]
- Harapan, H.; Anwar, S.; Yufika, A.; Sharun, K.; Gachabayov, M.; Fahriani, M.; Husnah, M.; Raad, R.; Abdalla, R.Y.; Adam, R.Y.; et al. Vaccine Hesitancy among Communities in Ten Countries in Asia, Africa, and South America during the COVID-19 Pandemic. Pathog. Glob. Health 2021, 1–8. [Google Scholar] [CrossRef]
- Ebrahimi, O.V.; Johnson, M.S.; Ebling, S.; Amundsen, O.M.; Halsøy, Ø.; Hoffart, A.; Skjerdingstad, N.; Johnson, S.U. Risk, Trust, and Flawed Assumptions: Vaccine Hesitancy During the COVID-19 Pandemic. Front. Public Health 2021, 9, 849. [Google Scholar] [CrossRef]
- Danabal, K.G.M.; Magesh, S.S.; Saravanan, S.; Gopichandran, V. Attitude towards COVID 19 Vaccines and Vaccine Hesitancy in Urban and Rural Communities in Tamil Nadu, India—A Community Based Survey. BMC Health Serv. Res. 2021, 21, 994. [Google Scholar] [CrossRef] [PubMed]
- Kirzinger, A.; Muñana, C.; Brodie, M. Vaccine Hesitancy in Rural America. KFF. 2021. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/vaccine-hesitancy-in-rural-america (accessed on 23 January 2022).
- Mahmud, S.; Mohsin, M.; Khan, I.A.; Mian, A.U.; Zaman, M.A. Knowledge, Beliefs, Attitudes and Perceived Risk about COVID-19 Vaccine and Determinants of COVID-19 Vaccine Acceptance in Bangladesh. PLoS ONE 2021, 16, e0257096. [Google Scholar] [CrossRef] [PubMed]
- Al-Wutayd, O.; Khalil, R.; Rajar, A.B. Sociodemographic and Behavioral Predictors of COVID-19 Vaccine Hesitancy in Pakistan. J. Multidiscip. Healthc. 2021, 14, 2847–2856. [Google Scholar] [CrossRef] [PubMed]
- Murthy, B.P. Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties—United States, 14 December 2020–10 April 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 759. [Google Scholar] [CrossRef]
- Scherer, A.M.; Gedlinske, A.M.; Parker, A.M.; Gidengil, C.A.; Askelson, N.M.; Petersen, C.A.; Woodworth, K.R.; Lindley, M.C. Acceptability of Adolescent COVID-19 Vaccination Among Adolescents and Parents of Adolescents—United States, 15–23 April 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 997–1003. [Google Scholar] [CrossRef]
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and Attitudes toward COVID-19 Vaccines: A Cross-Sectional Study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef]
- Allen, J.D.; Mohllajee, A.P.; Shelton, R.C.; Othus, M.K.D.; Fontenot, H.B.; Hanna, R. Stage of Adoption of the Human Papillomavirus Vaccine among College Women. Prev. Med. 2009, 48, 420–425. [Google Scholar] [CrossRef]
- Latkin, C.; Dayton, L.A.; Yi, G.; Konstantopoulos, A.; Park, J.; Maulsby, C.; Kong, X. COVID-19 Vaccine Intentions in the United States, a Social-Ecological Framework. Vaccine 2021, 39, 2288–2294. [Google Scholar] [CrossRef]
- Goldman, R.D.; McGregor, S.; Marneni, S.R.; Katsuta, T.; Griffiths, M.A.; Hall, J.E.; Seiler, M.; Klein, E.J.; Cotanda, C.P.; Gelernter, R.; et al. Willingness to Vaccinate Children against Influenza after the Coronavirus Disease 2019 Pandemic. J. Pediatr. 2021, 228, 87–93.e2. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Respondent type | ||
| Patient | 90 | 71% |
| Caregiver | 36 | 29% |
| Sex (N = 120) | ||
| Male | 40 | 44% |
| Female | 50 | 56% |
| Age category (N = 120) | ||
| 18–39 | 40 | 33% |
| 40–59 | 45 | 38% |
| ≥60 | 35 | 29% |
| Vaccination Status (N = 126) | ||
| Refused vaccine | 46 | 37% |
| Partially vaccinated | 4 | 3% |
| Fully vaccinated | 24 | 19% |
| Had not had the opportunity to be vaccinated | 52 | 41% |
| Intention to vaccinate among those with at least one dose (N = 28) | ||
| Would accept a vaccine today | 23 | 82% |
| Would not accept a vaccine today | 5 | 18% |
| Unsure | 0 | 0% |
| Intention to vaccinate among unvaccinated (N = 41) 1 | ||
| Would accept a vaccine today | 10 | 24% |
| Would not accept a vaccine today | 31 | 76% |
| Unsure | 0 | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aron, M.B.; Connolly, E.; Vrkljan, K.; Zaniku, H.R.; Nyirongo, R.; Mailosi, B.; Ruderman, T.; Barnhart, D.A.; on behalf of the Partners In Health Cross-Site COVID-19 Cohort Research Network. Attitudes toward COVID-19 Vaccines among Patients with Complex Non-Communicable Disease and Their Caregivers in Rural Malawi. Vaccines 2022, 10, 792. https://doi.org/10.3390/vaccines10050792
Aron MB, Connolly E, Vrkljan K, Zaniku HR, Nyirongo R, Mailosi B, Ruderman T, Barnhart DA, on behalf of the Partners In Health Cross-Site COVID-19 Cohort Research Network. Attitudes toward COVID-19 Vaccines among Patients with Complex Non-Communicable Disease and Their Caregivers in Rural Malawi. Vaccines. 2022; 10(5):792. https://doi.org/10.3390/vaccines10050792
Chicago/Turabian StyleAron, Moses Banda, Emilia Connolly, Kaylin Vrkljan, Haules Robbins Zaniku, Revelation Nyirongo, Bright Mailosi, Todd Ruderman, Dale A Barnhart, and on behalf of the Partners In Health Cross-Site COVID-19 Cohort Research Network. 2022. "Attitudes toward COVID-19 Vaccines among Patients with Complex Non-Communicable Disease and Their Caregivers in Rural Malawi" Vaccines 10, no. 5: 792. https://doi.org/10.3390/vaccines10050792