
Impact of School and Peer Connectedness on Adolescent Mental Health and Well-Being Outcomes during the COVID-19 Pandemic: A Longitudinal Panel Survey

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
1.1. Aims
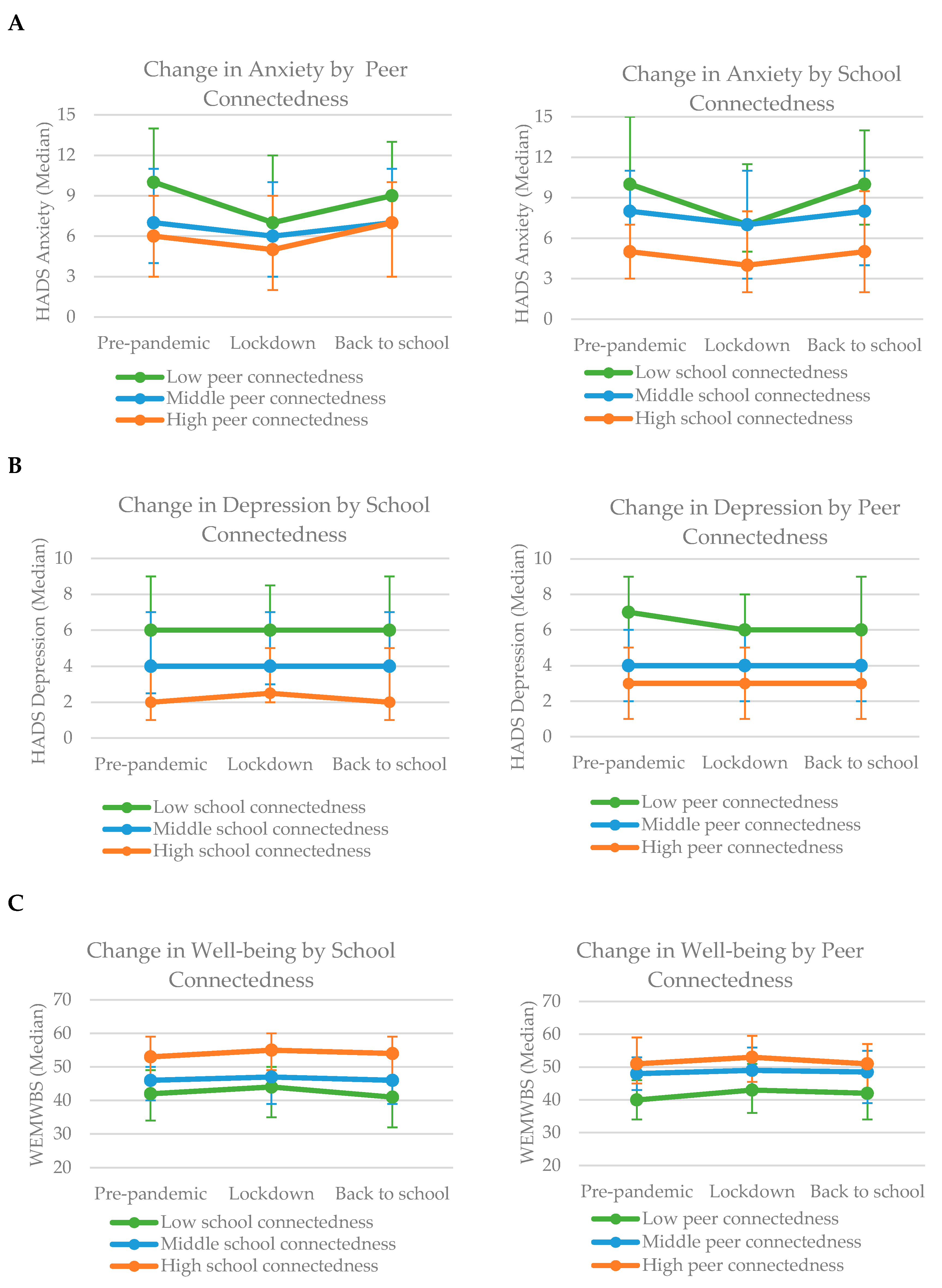
- To explore patterns of change over time in symptoms of anxiety, depression and well-being scores from pre-pandemic, during the first lockdown and when schools first fully reopened.
- To describe whether patterns of change over time differ according to pre-pandemic levels of school and peer connectedness.
- To test the relationship between pre-pandemic levels of school and peer connectedness and changes in mental health and well-being scores between lockdown and on the return to school.
1.2. Hypotheses
- Students with low levels of school and peer connectedness pre-pandemic would experience a greater increase in anxious and depressive symptoms, and a greater reduction in well-being scores on the return to school compared to students with medium levels of pre-pandemic connectedness.
- Students with high levels of school and peer connectedness would experience a greater decrease in anxious and depressive symptoms, and a greater increase in well-being scores on the return to school compared to students with medium levels of pre-pandemic connectedness.
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Predictor Variables
2.4. Outcome Measures
2.5. Statistical Analysis
Missing Data
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vizard, T.; Sadler, K.; Ford, T.; Newlove-Delgado, T.; McManus, S.; Marcheselli, F.; Davis, J.; Williams, T.; Leach, C.; Mandalia, D.; et al. Mental Health of Children and Young People in England. Wave 1 Follow Up to the 2017 Survey: NHS Digital. Health and Social Care Information Centre. 2022. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-of-children-and-young-people-in-england/2020-wave-1-follow-up (accessed on 30 May 2022).
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Burns, J.R.; Rapee, R.M. Adolescent mental health literacy: Young people’s knowledge of depression and help seeking. J. Adolesc. 2006, 29, 225–239. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Xue, Q.; Zhou, Y.; Zhu, K.; Liu, Q.; Zhang, J.; Song, R. Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei Province, China. JAMA Pediatr. 2020, 174, 898–900. [Google Scholar] [CrossRef] [Green Version]
- Hussong, A.M.; Midgette, A.J.; Thomas, T.E.; Coffman, J.L.; Cho, S. Coping and mental health in early adolescence during COVID-19. Res. Child Adolesc. Psychopathol. 2021, 49, 1113–1123. [Google Scholar] [CrossRef]
- Hawes, M.T.; Szenczy, A.K.; Klein, D.N.; Hajcak, G.; Nelson, B.D. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Rogers, A.A.; Ha, T.; Ockey, S. Adolescents’ perceived socio-emotional impact of COVID-19 and implications for mental health: Results from a US-based mixed-methods study. J. Adolesc. Health 2021, 68, 43–52. [Google Scholar] [CrossRef]
- Penner, F.; Ortiz, J.H.; Sharp, C. Change in youth mental health during the COVID-19 pandemic in a majority Hispanic/Latinx US sample. J. Am. Acad. Child Adolesc. Psychiatry 2021, 60, 513–523. [Google Scholar] [CrossRef]
- Creswell, C.; Shum, A.; Pearcey, S.; Skripkauskaite, S.; Patalay, P.; Waite, P. Young people’s mental health during the COVID-19 pandemic. Lancet Child Adolesc. Health 2021, 5, 535–537. [Google Scholar] [CrossRef]
- Bignardi, G.; Dalmaijer, E.S.; Anwyl-Irvine, A.L.; Smith, T.A.; Siugzdaite, R.; Uh, S.; Astle, D.E. Longitudinal increases in childhood depression symptoms during the COVID-19 lockdown. Arch. Dis. Child. 2021, 106, 791–797. [Google Scholar] [CrossRef]
- Demkowicz, O.; Ashworth, E.; O’Neill, A.; Hanley, T.; Pert, K. “Will my Young Adult Years be Spent Socially Distancing?”: A Qualitative Exploration of UK Adolescents’ Lockdown Experiences during the COVID-19 Pandemic. 2021; submitted. [Google Scholar] [CrossRef]
- Pigaiani, Y.; Zoccante, L.; Zocca, A.; Arzenton, A.; Menegolli, M.; Fadel, S.; Ruggeri, M.; Colizzi, M. Adolescent Lifestyle Behaviors, Coping Strategies and Subjective Well-Being during the COVID-19 Pandemic: An Online Student Survey. Healthcare 2020, 8, 472. [Google Scholar] [CrossRef]
- Hawes, M.T.; Szenczy, A.K.; Olino, T.M.; Nelson, B.D.; Klein, D.N. Trajectories of depression, anxiety and pandemic experiences; A longitudinal study of youth in New York during the Spring-Summer of 2020. Psychiatry Res. 2021, 298, 113778. [Google Scholar] [CrossRef]
- Waite, P.; Pearcey, S.; Shum, A.; Raw, J.; Patalay, P.; Creswell, C. How did the mental health of children and adolescents change during early lockdown during the COVID-19 pandemic in the UK? JCPP Adv. 2020, 1, e12009. [Google Scholar] [CrossRef]
- Gotlib, I.H.; Borchers, L.R.; Chahal, R.; Gifuni, A.J.; Teresi, G.I.; Ho, T.C. Early life stress predicts depressive symptoms in adolescents during the COVID-19 pandemic: The mediating role of perceived stress. Front. Psychol. 2021, 11, 3864. [Google Scholar] [CrossRef]
- Lane, J.; Therriault, D.; Dupuis, A.; Gosselin, P.; Smith, J.; Ziam, S.; Roy, M.; Roberge, P.; Drapeau, M.; Morin, P.; et al. The Impact of the COVID-19 Pandemic on the Anxiety of Adolescents in Québec. Child Youth Care Forum 2021, 1–23. [Google Scholar] [CrossRef]
- Pierce, M.; McManus, S.; Jessop, C.; John, A.; Hotopf, M.; Ford, T.; Hatch, S.; Wessely, S.C.; Abel, K.M. Says who? The significance of sampling in mental health surveys during COVID-19. Lancet Psychiatry 2020, 7, 567–568. [Google Scholar] [CrossRef]
- Foulkes, L.; Blakemore, S.-J. Individual differences in adolescent mental health during COVID-19: The importance of peer relationship quality. Neuron 2021, 109, 3203–3205. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef]
- Lee, R.M.; Draper, M.; Lee, S. Social connectedness, dysfunctional interpersonal behaviors, and psychological distress: Testing a mediator model. J. Couns. Psychol. 2001, 48, 310–318. [Google Scholar] [CrossRef]
- Jose, P.E.; Ryan, N.; Pryor, J. Does social connectedness promote a greater sense of well-being in adolescence over time? J. Res. Adolesc. 2012, 22, 235–251. [Google Scholar] [CrossRef]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Platt, B.; Kadosh, K.C.; Lau, J.Y. The role of peer rejection in adolescent depression. Depress. Anxiety 2013, 30, 809–821. [Google Scholar] [CrossRef] [PubMed]
- Moses, J.O.; Villodas, M.T. The potential protective role of peer relationships on school engagement in at-risk adolescents. J. Youth Adolesc. 2017, 46, 2255–2272. [Google Scholar] [CrossRef] [PubMed]
- Van Harmelen, A.-L.; Kievit, R.; Ioannidis, K.; Neufeld, S.; Jones, P.; Bullmore, E.; Dolan, R.; Fonagy, P.; Goodyer, I. Adolescent friendships predict later resilient functioning across psychosocial domains in a healthy community cohort. Psychol. Med. 2017, 47, 2312–2322. [Google Scholar] [CrossRef]
- Lam, C.B.; McHale, S.M.; Crouter, A.C. Time with peers from middle childhood to late adolescence: Developmental course and adjustment correlates. Child Dev. 2014, 85, 1677–1693. [Google Scholar] [CrossRef] [Green Version]
- Albert, D.; Chein, J.; Steinberg, L. The teenage brain: Peer influences on adolescent decision making. Curr. Dir. Psychol. Sci. 2013, 22, 114–120. [Google Scholar] [CrossRef]
- Sebastian, C.L.; Tan, G.C.; Roiser, J.P.; Viding, E.; Dumontheil, I.; Blakemore, S.-J. Developmental influences on the neural bases of responses to social rejection: Implications of social neuroscience for education. Neuroimage 2011, 57, 686–694. [Google Scholar] [CrossRef]
- Somerville, L.H. The teenage brain: Sensitivity to social evaluation. Curr. Dir. Psychol. Sci. 2013, 22, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Foulkes, L.; Blakemore, S.-J. Is there heightened sensitivity to social reward in adolescence? Curr. Opin. Neurobiol. 2016, 40, 81–85. [Google Scholar] [CrossRef]
- Orben, A.; Tomova, L.; Blakemore, S.-J. The effects of social deprivation on adolescent social development and mental health. Lancet Child Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef]
- Shochet, I.M.; Dadds, M.R.; Ham, D.; Montague, R. School connectedness is an underemphasized parameter in adolescent mental health: Results of a community prediction study. J. Clin. Child Adolesc. Psychol. 2006, 35, 70–79. [Google Scholar] [CrossRef]
- Kidger, J.; Araya, R.; Donovan, J.; Gunnell, D. The effect of the school environment on the emotional health of adolescents: A systematic review. Pediatrics 2022, 129, 925–949. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Kaul, A.; Shah, R.; Maddipoti, S. Impact of Coronavirus Disease 2019 Pandemic and Lockdown on Mental Health Symptoms in Children. Indian Pediatr. 2020, 58, 75–76. [Google Scholar]
- Millings, A.; Buck, R.; Montgomery, A.; Spears, M.; Stallard, P. School connectedness, peer attachment, and self-esteem as predictors of adolescent depression. J. Adolesc. 2012, 35, 1061–1067. [Google Scholar] [CrossRef]
- Becker, B.E.; Luthar, S.S. Social-emotional factors affecting achievement outcomes among disadvantaged students: Closing the achievement gap. Educ. Psychol. 2002, 37, 197–214. [Google Scholar] [CrossRef]
- Widnall, E.; Winstone, L.; Mars, B.; Haworth, C.M.; Kidger, J. Young People’s Mental Health during the COVID-19 Pandemic; University of Bristol: Bristol, UK, 2020; Available online: https://sphr.nihr.ac.uk/wp-content/uploads/2020/08/Young-Peoples-Mental-Health-during-the-COVID-19-Pandemic-Report-Final.pdf (accessed on 30 May 2022).
- Social Media and Adolescent Mental Health and Well-Being. Available online: https://osf.io/7xz6u/ (accessed on 30 May 2022).
- Goodenow, C. The psychological sense of school membership among adolescents: Scale development and educational correlates. Psychol. Sch. 1993, 30, 79–90. [Google Scholar] [CrossRef]
- Blum, R.W.; McNeely, C.A.; Reinhart, P.M. Improving the Odds: The Untapped Power of Schools to Improve the Health of Teens; University of Minnesota Center for Adolescent Health and Development: Minneapolis, MN, USA, 2002; Available online: https://www.casciac.org/pdfs/ImprovingtheOdds.pdf (accessed on 30 May 2022).
- White, D.; Leach, C.; Sims, R.; Atkinson, M.; Cottrell, D. Validation of the Hospital Anxiety and Depression Scale for Use with Adolescents. Br. J. Psychiatry 1999, 175, 452–454. [Google Scholar] [CrossRef]
- Clarke, A.; Friede, T.; Putz, R.; Ashdown, J.; Martin, S.; Blake, A.; Adi, Y.; Parkinson, J.; Flynn, P.; Platt, S.; et al. Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): Validated for Teenage School Students in England and Scotland. A Mixed Methods Assessment. BMC Public Health 2011, 11, 487. [Google Scholar] [CrossRef] [Green Version]
- Hartley, J.E.; Levin, K.; Currie, C. A new version of the HBSC family affluence scale-FAS III: Scottish qualitative findings from the international FAS development study. Child Indic. Res. 2016, 9, 233–245. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, K.L.; Newby, D.; Soneson, E.; Vaci, N.; Jindra, C.; Geulayov, G.; Gallacher, J.; Fazel, M. COVID-19 partial school closures and mental health problems: A cross-sectional survey of 11,000 adolescents to determine those most at risk. JCPP Adv. 2021, 1, e12021. [Google Scholar] [CrossRef]
- Soneson, E.; Puntis, S.; Chapman, N.; Mansfield, K.; Jones, P.; Fazel, M. Happier during lockdown: A descriptive analysis of self-reported wellbeing in 17,000 UK school students during COVID-19 lockdown. Eur. Child Adolesc. Psychiatry 2022, 1–16. [Google Scholar] [CrossRef]
- Arseneault, L. Annual Research Review: The Persistent and Pervasive Impact of Being Bullied in Childhood and Adolescence: Implications for Policy and Practice. J. Child Psychol. Psychiatry 2018, 59, 405–421. [Google Scholar] [CrossRef] [Green Version]
- Högberg, B.; Strandh, M.; Hagquist, C. Gender and secular trends in adolescent mental health over 24 years—The role of school-related stress. Soc. Sci. Med. 2020, 250, 112890. [Google Scholar] [CrossRef]
- Silk, J.S.; Scott, L.N.; Hutchinson, E.A.; Lu, C.; Sequeira, S.L.; McKone, K.M.P.; Do, Q.B.; Ladouceur, C.D. Storm clouds and silver linings: Day-to-day life in COVID-19 lockdown and emotional health in adolescent girls. J. Pediatr. Psychol. 2022, 47, 37–48. [Google Scholar] [CrossRef]
- Aldridge, J.M.; McChesney, K. The relationships between school climate and adolescent mental health and well-being: A systematic literature review. Int. J. Educ. Res. 2018, 88, 121–145. [Google Scholar] [CrossRef]
- Singla, D.R.; Shinde, S.; Patton, G.; Patel, V. The mediating effect of school climate on adolescent mental health: Findings from a randomized controlled trial of a school-wide intervention. J. Adolesc. Health 2021, 69, 90–99. [Google Scholar] [CrossRef]
- McNeely, C.A.; Nonnemaker, J.M.; Blum, R.W. Promoting school connectedness: Evidence from the national longitudinal study of adolescent health. J. Sch. Health 2002, 72, 138–146. [Google Scholar] [CrossRef]
- McCabe, E.M.; Davis, C.; Mandy, L.; Wong, C. The role of school connectedness in supporting the health and well-being of youth: Recommendations for school nurses. NASN Sch. Nurse 2022, 37, 42–47. [Google Scholar] [CrossRef]
- Perkins, K.N.; Carey, K.; Lincoln, E.; Shih, A.; Donalds, R.; Kessel Schneider, S.; Holt, M.K.; Green, J.G. School Connectedness Still Matters: The Association of School Connectedness and Mental Health during Remote Learning Due to COVID-19. J. Prim. Prev. 2021, 42, 641–648. [Google Scholar] [CrossRef]
- Wade, M.; Prime, H.; Browne, D.T. Why we need longitudinal mental health research with children and youth during (and after) the COVID-19 pandemic. Psychiatry Res. 2020, 290, 113143. [Google Scholar] [CrossRef]


{kind=link}
| Comparison Variable | <3 Time Points * | All 3 Time Points ** | Sample Comparison | |||
|---|---|---|---|---|---|---|
| n | % or Mean (SD) | N | % or Mean (SD) | Pearson Chi2 | p-Value | |
| Gender (% Female) | 1613 | 56.1% | 592 | 59.6% | 2.19 | 0.139 |
| Ethnicity (% White) | 1648 | 76.9% | 598 | 81.9% | 6.59 | 0.010 |
| Sexual attraction (% heterosexual) | 1666 | 81.1% | 599 | 81.4% | 0.04 | 0.840 |
| Free school meals (% receiving) | 1609 | 11.7% | 595 | 5.7% | 17.38 | <0.001 |
| Family Affluence (% low affluence) | 1630 | 15.9% | 598 | 9.5% | 15.06 | <0.001 |
| Reported a disability, health condition or SEN | 1643 | 15.3% | 599 | 13.8% | 0.70 | 0.403 |
| At risk of depression (HADS ≥ 7) | 1684 | 32.0% | 573 | 27.2% | 4.59 | 0.032 |
| At risk of anxiety (HADS ≥ 9) | 1686 | 43.2% | 577 | 41.2% | 0.70 | 0.404 |
| Pre-Pandemic (T1, October 2019) | During Lockdown (T2, May 2020) | Return to School (T3, October 2020) | |
|---|---|---|---|
| School connectedness | 95.1% | 96.5% | 92.5% |
| Peer connectedness | 95.3% | 96.5% | 93.0% |
| Depressive symptoms (HADS) | 97.6% | 97.3% | 97.6% |
| Anxious symptoms (HADS) | 97.5% | 97.3% | 97.6% |
| Well-being (WEMWBS) | 98.3% | 95.6% | 93.3% |
| Anxious Symptoms (HADS) a | Unadjusted | Partially Adjusted * | Fully Adjusted ** | ||||||
| Est | 95% CI | p-Value | Est | 95% CI | p-Value | Est | 95% CI | p-Value | |
| Low school connectedness | 1.409 | (0.64, 2.17) | <0.001 | 1.414 | (0.64, 2.19) | <0.001 | 1.332 | (0.55, 2.11) | 0.001 |
| Middle school connectedness | 0 | Ref | - | 0 | Ref | - | 0 | Ref | - |
| High school connectedness | 0.174 | (−0.56, 0.91) | 0.641 | 0.179 | (−0.55, 0.91) | 0.630 | 0.203 | (−0.56, 0.96) | 0.602 |
| Depressive Symptoms b (HADS) | Unadjusted | Partially Adjusted * | Fully Adjusted ** | ||||||
| Est | 95% CI | p-Value | Est | 95% CI | p-Value | Est | 95% CI | p-Value | |
| Low school connectedness | 0.953 | (0.32, 1.59) | 0.003 | 0.892 | (0.25, 1.54) | 0.007 | 0.869 | (0.21, 1.53) | 0.010 |
| Middle school connectedness | 0 | Ref | - | 0 | Ref | - | 0 | Ref | - |
| High school connectedness | −0.184 | (−0.79, 0.42) | 0.548 | −0.181 | (−0.79, 0.42) | 0.556 | −0.17 | (−0.79, 0.45) | 0.590 |
| Well-Being Score (WEMWBS) c | Unadjusted | Partially Adjusted * | Fully Adjusted ** | ||||||
| Est | 95% CI | p-Value | Est | 95% CI | p-Value | Est | 95% CI | p-Value | |
| Low school connectedness | −1.898 | (−3.81, 0.02) | 0.053 | −1.849 | (−3.78, 0.08) | 0.061 | −1.91 | (−3.87, 0.05) | 0.056 |
| Middle school connectedness | 0 | Ref | - | 0 | Ref | - | 0 | Ref | - |
| High school connectedness | −0.845 | (−2.65, 0.97) | 0.361 | −0.813 | (−2.61, 0.99) | 0.376 | −0.74 | (−2.58, 1.11) | 0.436 |
| Anxious Symptoms (HADS) a | Unadjusted | Partially Adjusted * | Fully Adjusted ** | ||||||
| Est | 95% CI | p-Value | Est | 95% CI | p-Value | Est | 95% CI | p-Value | |
| Low peer connectedness | 0.902 | (0.43, 1.37) | 0.068 | 0.756 | (0.01, 1.51) | 0.049 | 0.531 | (−0.24, 1.30) | 0.175 |
| Middle peer connectedness | 0 | Ref | - | 0 | Ref | - | 0 | Ref | - |
| High peer connectedness | 0.037 | (−0.72,0.80) | 0.923 | −0.053 | (−0.08, 0.70) | 0.891 | 0.100 | (−0.67, 0.87) | 0.798 |
| Depressive Symptoms (HADS) b | Unadjusted | Partially Adjusted * | Fully Adjusted ** | ||||||
| Est | 95% CI | p-Value | Est | 95% CI | p-Value | Est | 95% CI | p-Value | |
| Low peer connectedness | 0.359 | (−0.26, 0.98) | 0.258 | 0.297 | (−0.33, 0.92) | 0.350 | 0.09 | (−0.55, 0.73) | 0.781 |
| Middle peer connectedness | 0 | Ref | - | 0 | Ref | - | 0 | Ref | - |
| High peer connectedness | −0.354 | (−0.99, 0.27) | 0.266 | −0.375 | (−1.00, 0.25) | 0.241 | −0.232 | (−0.87, 0.40) | 0.473 |
| Well-being Score (WEMWBS) c | Unadjusted | Partially Adjusted * | Fully Adjusted ** | ||||||
| Est | 95% CI | p-Value | Est | 95% CI | p-Value | Est | 95% CI | p-Value | |
| Low peer connectedness | 0.148 | (−1.72, 2.02) | 0.877 | 0.175 | (−1.69, 2.03) | 0.853 | 0.398 | (−1.51, 2.31) | 0.683 |
| Middle peer connectedness | 0 | Ref | - | 0 | Ref | - | 0 | Ref | - |
| High peer connectedness | 0.457 | (−1.38, 2.34) | 0.617 | 0.519 | (−1.34, 2.38) | 0.584 | 0.457 | (−1.43, 2.34) | 0.636 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Widnall, E.; Winstone, L.; Plackett, R.; Adams, E.A.; Haworth, C.M.A.; Mars, B.; Kidger, J. Impact of School and Peer Connectedness on Adolescent Mental Health and Well-Being Outcomes during the COVID-19 Pandemic: A Longitudinal Panel Survey. Int. J. Environ. Res. Public Health 2022, 19, 6768. https://doi.org/10.3390/ijerph19116768
Widnall E, Winstone L, Plackett R, Adams EA, Haworth CMA, Mars B, Kidger J. Impact of School and Peer Connectedness on Adolescent Mental Health and Well-Being Outcomes during the COVID-19 Pandemic: A Longitudinal Panel Survey. International Journal of Environmental Research and Public Health. 2022; 19(11):6768. https://doi.org/10.3390/ijerph19116768
Chicago/Turabian StyleWidnall, Emily, Lizzy Winstone, Ruth Plackett, Emma A. Adams, Claire M. A. Haworth, Becky Mars, and Judi Kidger. 2022. "Impact of School and Peer Connectedness on Adolescent Mental Health and Well-Being Outcomes during the COVID-19 Pandemic: A Longitudinal Panel Survey" International Journal of Environmental Research and Public Health 19, no. 11: 6768. https://doi.org/10.3390/ijerph19116768