

Evaluating Efficacy of a COVID-19 Alternative Care Site Preparedness Assessment Tool for Catastrophic Healthcare Surge Capacity during Pandemic Response


Abstract
:1. Introduction
2. Background
2.1. Emergency Risk Management
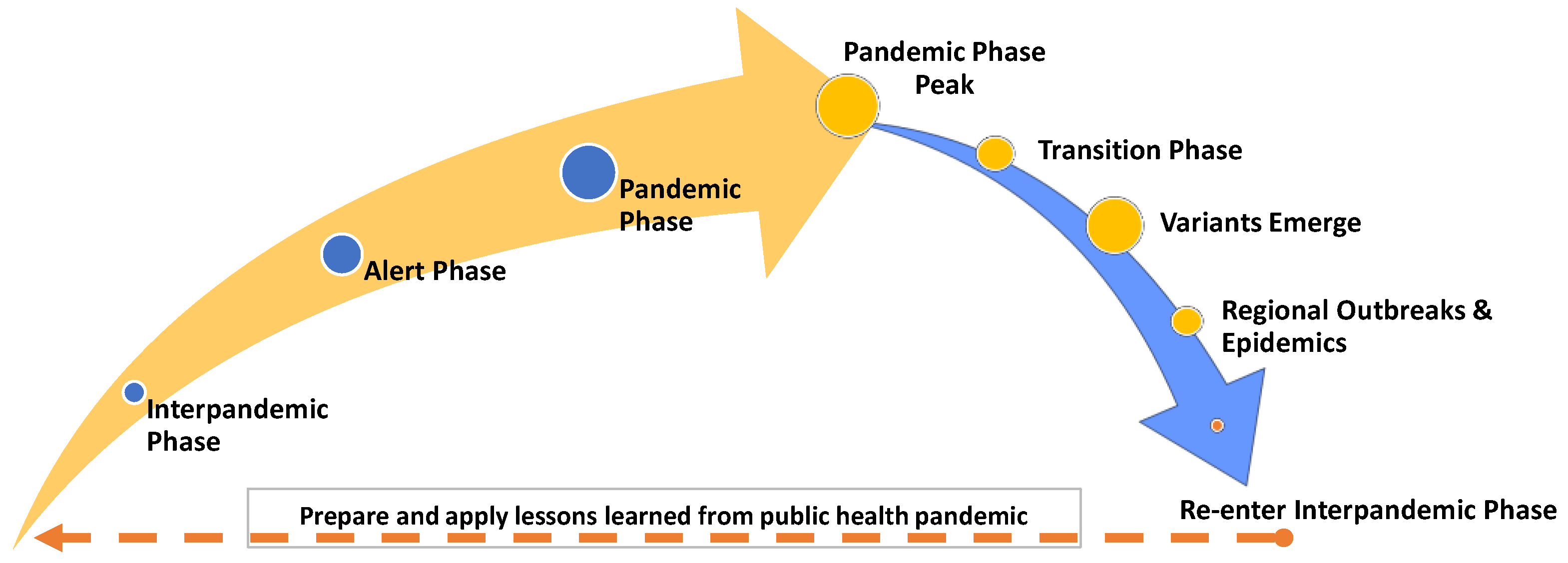
2.2. Pandemic Framework and Phases
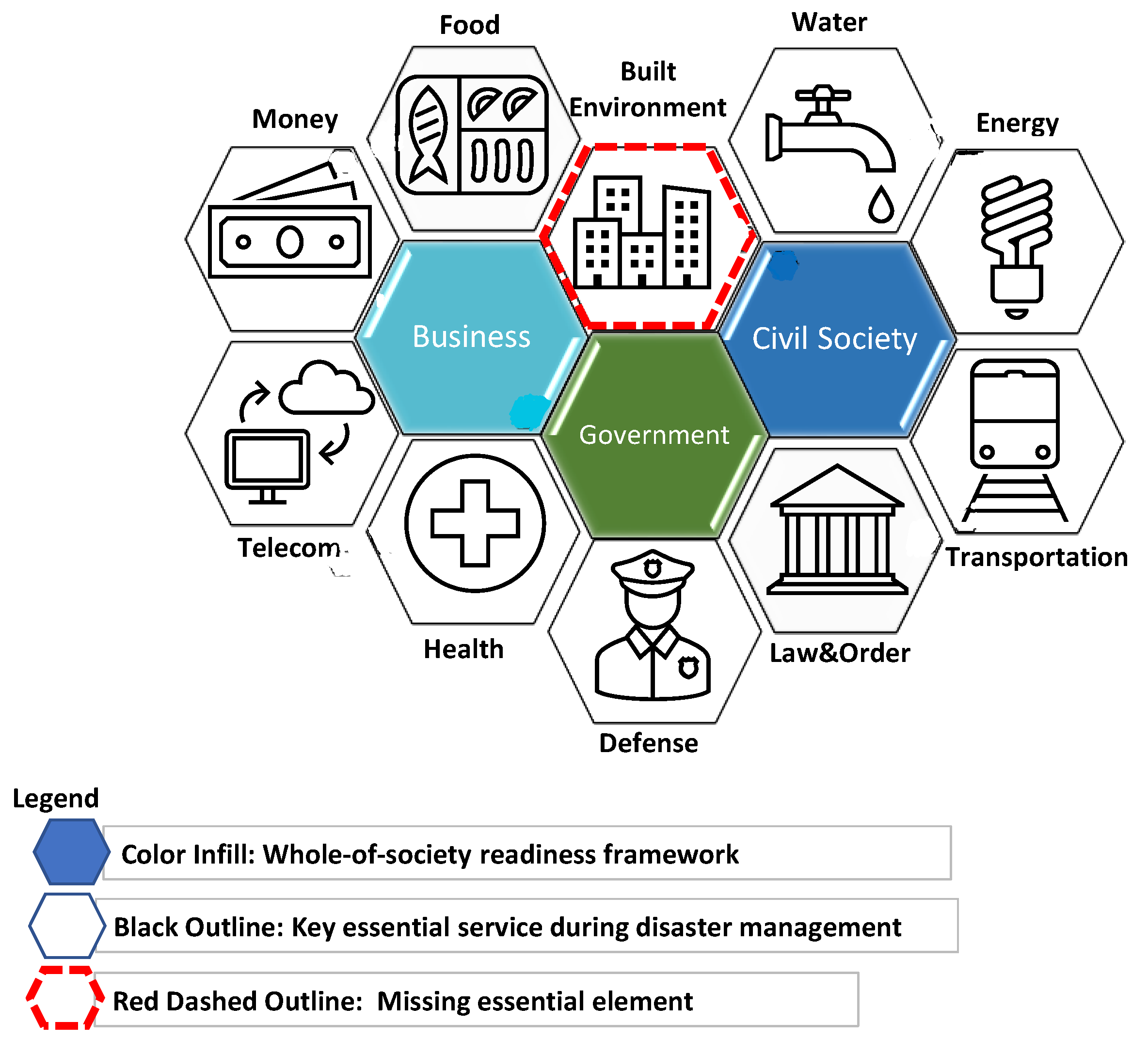
2.3. Whole-of-Society Response & Built Environment
2.4. Catastrophic Healthcare Surge Capacity
- System: Components involve planning with community, government, informal networks, public health, regional health systems, hospital epidemiology and infection control, incident command, and local utility infrastructure. Additional systems preparedness involves anticipating supply chain disruption, coordination of first responders, and maintaining continuity of operations including cybersecurity;
- Space: Catastrophic functional space programming includes determining size and service volumes for medical care, storage, laboratory, mortuary, and staff housing.
- Staff: Analysis of staffing models for patient care ratios, shifts or rotations, capability and skill sets, expertise, stamina, and psychological impacts; and
- Supplies: Catastrophic supplies necessitate review of biologics, respirators, personal protective equipment (PPE), and standard use supplies, as well as food and water.
2.5. Alternative Care Sites
2.6. US COVID-19 Developing Situation
3. Materials and Methods
3.1. Identifying the Task Force Members
3.2. Intensive Workshop—The Charrette Process
3.3. Use of Existing Guidance Documents
3.4. COVID-19 ACS Case Study Article Search Method
4. Results
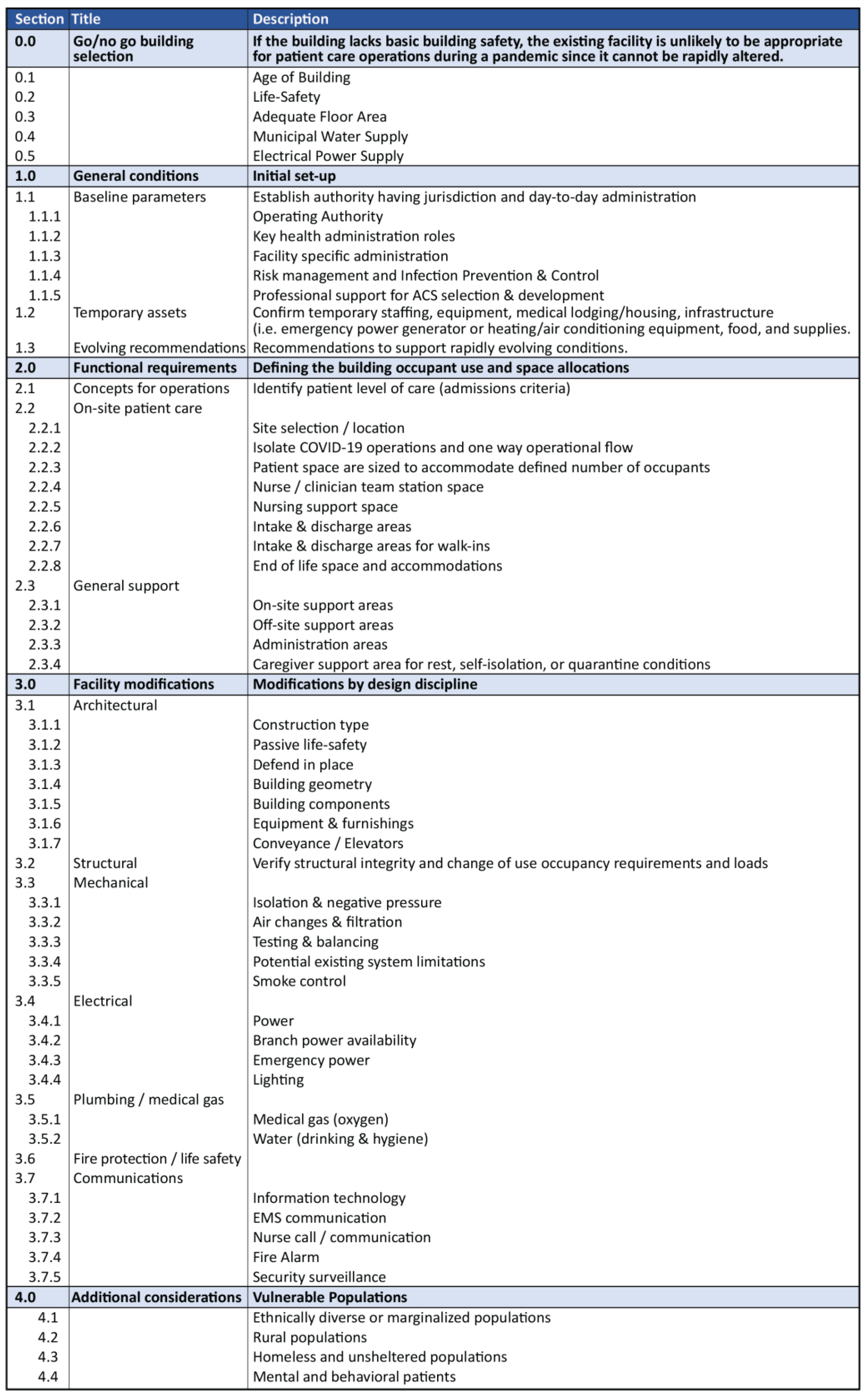
4.1. COVID-19 Alternative Care Sites Preparedness Assessment Tool
4.2. Public Health Dissemination
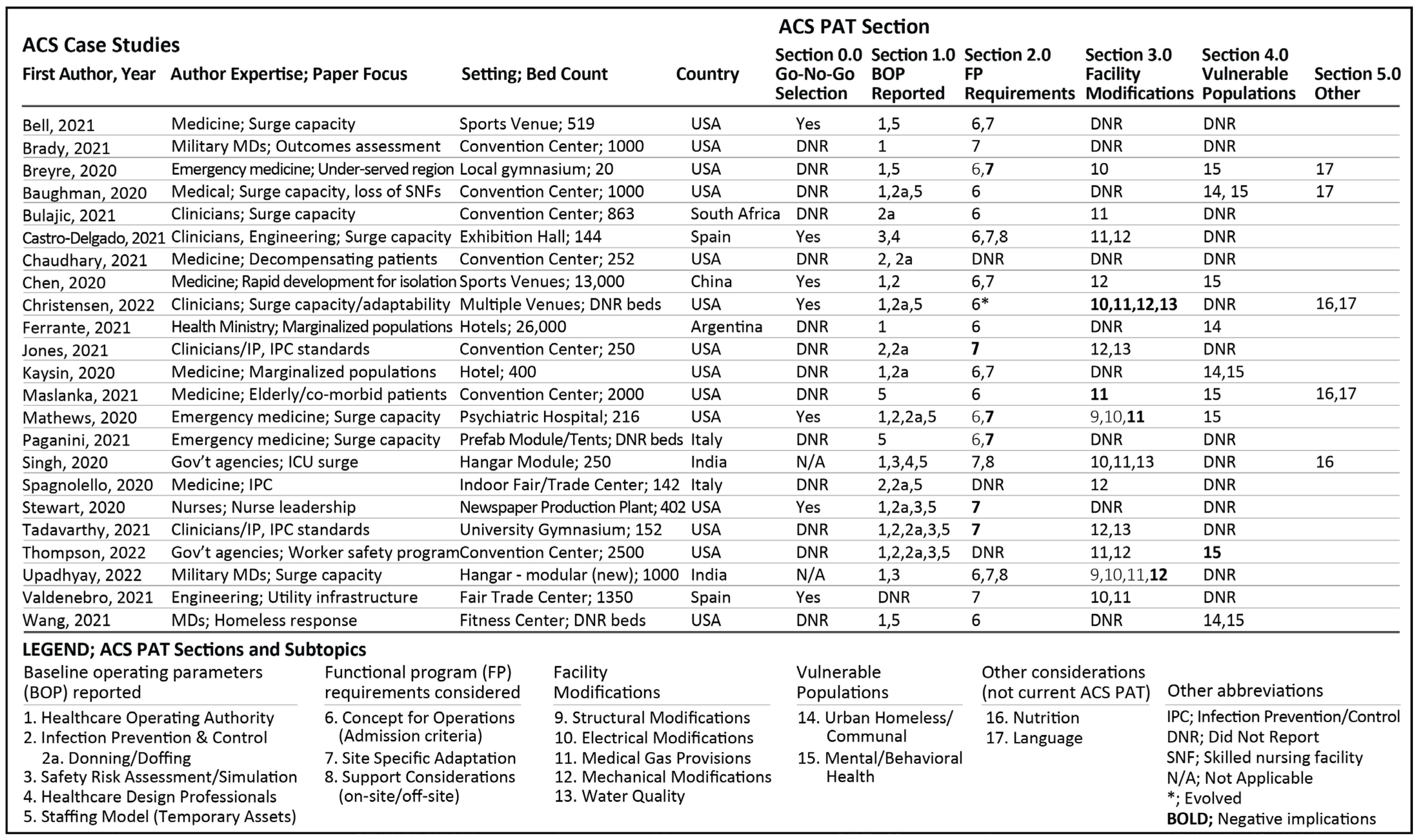
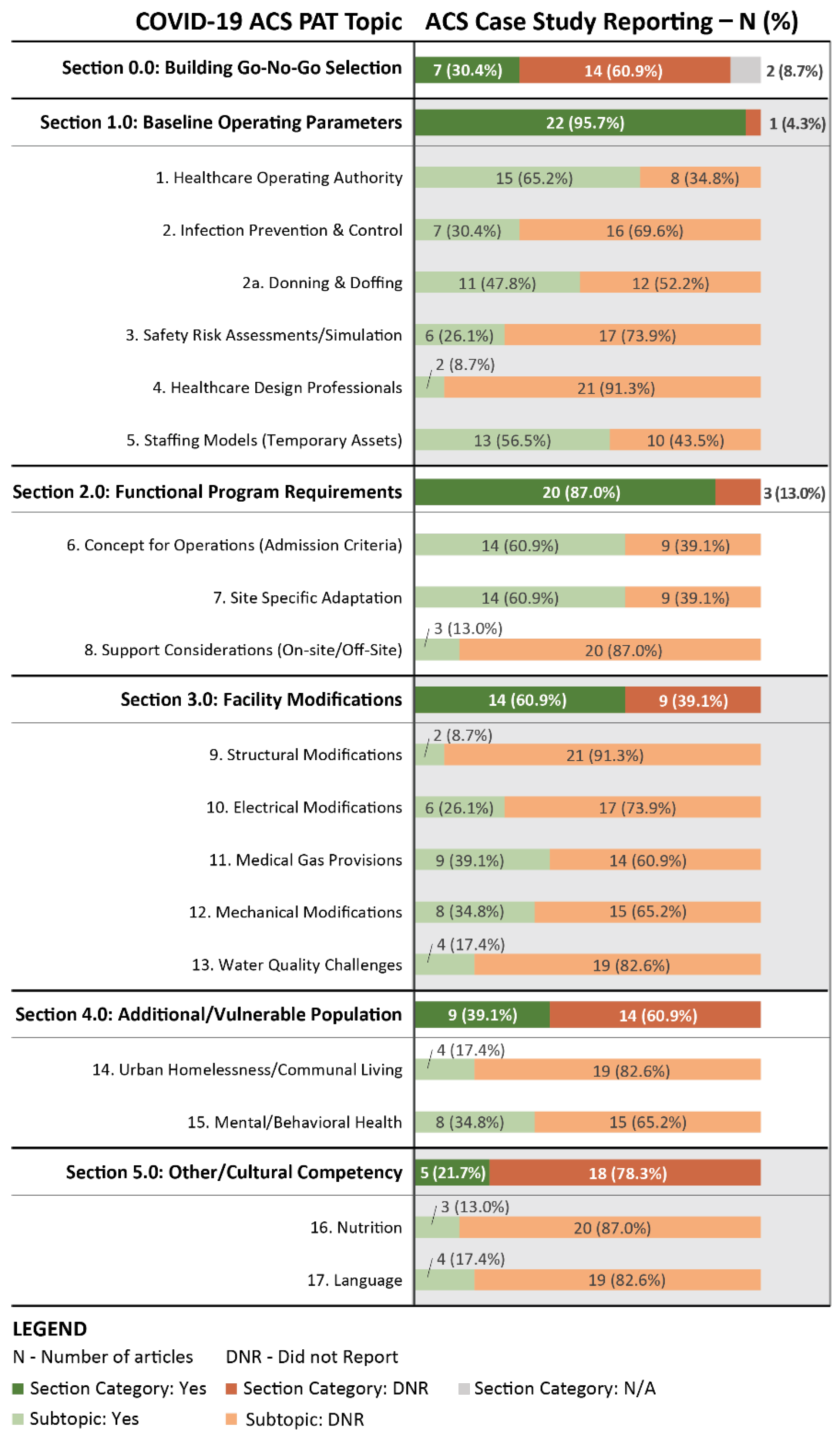
4.3. COVID-19 ACS Case Study Article Search and Coding Results
- 0.0 Go/no-go selection (n = 7, 30.4%);
- 1.0 Baseline operating parameters (n = 22, 95.7%);
- 2.0 Functional program requirements (n = 20, 87.0%);
- 3.0 Facility modifications (n = 14, 60.9%); and
- 4.0 Vulnerable populations (n = 9, 39.1%)
5. Discussion
5.1. Go-No-Go Building Selection
5.2. General Conditions
5.2.1. Baseline Operating Parameters
Establish a Healthcare Operating Authority
Safety Risk Assessment & Running Simulation Exercises
Infection Prevention & Control
Collaborating with Healthcare Design Professionals
5.2.2. Temporary Assets
Staffing
Medical Equipment
5.2.3. Evolving Recommendations
5.3. Functional Program Requirements & Concepts for Operations
5.3.1. Identify Admissions Criteria
5.3.2. Site Selection and Location
5.4. Facility Modifications & Building System Infrastructure
5.4.1. Structural
5.4.2. Mechanical Air Systems
5.4.3. Electrical Power
5.4.4. Plumbing
Medical Gas Systems
Potable Water Systems
5.5. Considerations for Vulnerable Populations and Cultural Competency
5.5.1. Urban Homelessness & Communal Housing Response
5.5.2. Mental & Behavioral Health Response
5.5.3. Language Barriers
5.5.4. Nutrition Barriers
5.6. Limitations
6. Conclusions
- Review and revise the COVID-19 ACS PAT V2.0 checklist based upon ACS case study findings. Specific areas for improvement within a future ACS PAT V3.0 include:
- Healthcare operating authority: identify an incident command center as the common method of operations and allocation for space and communication systems for implementation.
- Infection prevention and control zones: organize a tri-level hierarchy of infection control zones (e.g., low, medium, high) as a space planning concept which includes varying levels of PPE for donning and doffing procedures at the transition between zones.
- Safety Risk Assessments/Simulations: patient care and staff operational simulations should be conducted at various stages of ACS development for making adjustments to the built environmental setting as early as possible including preliminary design reviews, tabletop exercises, and pre-admission operational drills. Additionally, anticipate built environment changes throughout the pandemic as the pathogen of interest evolves and medical treatment changes.
- Functional Program Requirements: each site will need to be continually evaluated and site adaption may be necessary for an evolution of pandemic response that can impact building systems, space allocation, staffing patterns, and medical equipment.
- Electronic Medical Records: anticipate and determine the need to connect the ACS to a local healthcare organization’s existing method of medical record input and archival. Parallel existing systems to reduce logistical difficulties for accurate documentation from initial patient admission.
- Electrical Power and Medical Gas Provisions: during respiratory virus transmission oxygen supplies will be impacted. As the COVID-19 pandemic evolved (i.e., concepts of ‘long COVID’ emerged) approaches to admitting, treating, transferring, and discharging patients were impacted by access to building oxygen supplies and subsequently emergency power resources for ventilators and other medical equipment.
- Cultural Competency: include nutrition and language barriers that may arise in local populations which impeded patient care operations and had potentially negative patient outcomes.
- Introduce all-hazard disaster preparedness training [26] for design professionals to more effectively participate within a public health or clinical response team in order to better guide organizations through the complexity of built environment modifications for catastrophic HSC. This public health architect and engineer role would anticipate built environment challenges and reduce the burden of ad-hoc facility adjustments by public health or clinical teams during pandemic response.
- Engage public health and healthcare organizations in catastrophic HSC and disaster preparedness at the federal, state, and local levels to create awareness in understanding the role of the built environment. Encourage community engagement to determine an appropriate ACS facility during the interpandemic phase of response which in-turn will identify human and material resources, community partnerships, conflicts of interest (i.e., bias), and methods of recovery [27].
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Castro Delgado, R.; Pérez Quesada, P.; Pintado García, E.; Marañón Zabalza, I.; Vallina-Victorero Vázquez, M.; Escribano Balín, R. Alternate Care Sites for COVID-19 Patients: Experience from the H144 Hospital of the Health Service of the Principality of Asturias, Spain. Prehosp. Disaster Med. 2021, 36, 774–781. [Google Scholar] [CrossRef]
- Chen, S.; Zhang, Z.; Yang, J.; Wang, J.; Zhai, X.; Bärnighausen, T.; Wang, C. Fangcang shelter hospitals: A novel concept for responding to public health emergencies. Lancet (Br. Ed.) 2020, 395, 1305–1314. [Google Scholar] [CrossRef]
- Christensen, K.; Metzner, M.; Lovett-Floom, L.; Lindsay, C.; Meghoo, C.A.; Staats, K.; Noste, E.; Devereaux, A.; Backer, H. Utilization of Alternate Care Sites During COVID-19 Surge and Mass Care: California 2020–2021. Disaster Med. Public Health Prep. 2022, 1–19. [Google Scholar] [CrossRef]
- Maslanka, M.; Hurwitz, J.A. An Eye on COVID: Hurricane Preparedness at a COVID-19 Alternative Care Site. Disaster Med. Public Health Prep. 2022, 16, 303–309. [Google Scholar] [CrossRef]
- Iserson, K. Alternative Care Sites: An Option in Disasters. West J. Emerg. Med. 2020, 21, 484–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, S.A.; Krienke, L.; Quanstrom, K. Alternative Care Sites during the COVID-19 Pandemic: Policy Implications for Pandemic Surge Planning. Disaster Med. Public Health Prep. 2021, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Facility Guidelines Institute. FGI Guidelines for the Design and Construction of Hospitals; FGI with American Society of Healthcare Engineering: St. Louis, MO, USA, 2022. [Google Scholar]
- Freihoefer, K.; Zborowsky, T. Making the Case for Practice-Based Research and the Imperative Role of Design Practitioners. HERD 2017, 10, 66–82. [Google Scholar] [CrossRef]
- Dietz, L.; Horve, P.F.; Coil, D.A.; Fretz, M.; Eisen, J.A.; Van Den Wymelenberg, K. 2019 Novel Coronavirus (COVID-19) Pandemic: Built Environment Considerations to Reduce Transmission. mSystems 2020, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, D.; Ward, J.; Yao, C.J.; Lee, J. Built Environment Airborne Infection Control Strategies in Pandemic Alternative Care Sites. HERD 2021, 14, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Abney, S.E.; Bright, K.R.; McKinney, J.; Ijaz, M.K.; Gerba, C.P. Toilet hygiene—Review and research needs. J. Appl. Microbiol. 2021, 131, 2705–2714. [Google Scholar] [CrossRef]
- AIA. Alternative Care Sites Preparedness. Available online: https://www.aia.org/resources/6283331-alternative-care-sites-preparedness-tools (accessed on 18 July 2022).
- AIA. Architects Taking Action to Support COVID-19 Response: New AIA Task Force Will Offer Insights for Adapting Buildings into Healthcare Facilities. American Institute of Architects: Washington, DC, USA. Available online: https://www.aia.org/press-releases/6282337-architects-taking-action-to-support-covid (accessed on 27 July 2022).
- WHO. Health Emergency and Disaster Risk Management Framework; World Health Organization: Geneva, Switzerland, 2019; pp. 1–48. [Google Scholar]
- WHO; Public Health England; United Nations Office for Disaster Risk Reduction. Emergency Risk Management for Health: Overview; World Health Organization: Geneva, Switzerland, 2013; pp. 1–6. [Google Scholar]
- WHO. Pandemic Influenza Risk Management: A WHO Guide to Inform and Harmonize National and International Pandemic Preparedness and Response; World Health Organization: Geneva, Switzerland, 2017; pp. 1–62. [Google Scholar]
- WHO; England, P.H. Safe Hospitals: Prepared for Emergencies and Disasters; World Health Organization: Geneva, Switzerland, 2017; pp. 1–2. [Google Scholar]
- WHO. Whole-of-Society Pandemic Readiness: WHO Guidelines for Pandemic Preparedness and Response in the Non-Healthcare Sector; World Health Organization: Geneva, Switzerland, 2009; pp. 1–18. [Google Scholar]
- WHO. Pandemic Influenza Preparedness Framework for the Sharing of Influenza Viruses and Access to Vaccines and Other Benefits; World Health Organization: Geneva, Switzerland, 2011; pp. 1–68. [Google Scholar]
- WHO. A Checklist for Pandemic Influenza Risk and Impact Management: Building Capacity for Pandemic Response; World Health Organization: Geneva, Switzerland, 2018; pp. 1–44. [Google Scholar]
- Murewanhema, G.; Dzinamarira, T. The COVID-19 Pandemic: Public Health Responses in Sub-Saharan Africa. Int. J. Environ. Res. Public Health 2022, 19, 4448. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus (COVID-19) Dashboard Overview. Available online: https://covid19.who.int/ (accessed on 20 July 2022).
- Schwartz, J.; Yen, M.-Y. Toward a collaborative model of pandemic preparedness and response: Taiwan’s changing approach to pandemics. J. Microbiol. Immunol. Infect. 2017, 50, 125–132. [Google Scholar] [CrossRef]
- Kelen, G.D.; McCarthy, M.L. The Science of Surge. Acad. Emerg. Med. 2006, 13, 1089–1094. [Google Scholar] [CrossRef]
- Adams, L.M. Exploring the concept of surge capacity. Online J. Issues Nurs. 2009, 14, 1F. [Google Scholar] [CrossRef]
- Schultz, C.H.M.D.; Koenig, K.L.M.D.; Whiteside, M.P.; Murray, R.E.M.T.P. Development of National Standardized All-Hazard Disaster Core Competencies for Acute Care Physicians, Nurses, and EMS Professionals. Ann. Emerg. Med. 2012, 59, 196–208. [Google Scholar] [CrossRef]
- Orsini, E.; Mireles-Cabodevila, E.; Ashton, R.; Khouli, H.; Chaisson, N. Lessons on Outbreak Preparedness from the Cleveland Clinic. Chest 2020, 158, 2090–2096. [Google Scholar] [CrossRef]
- Meyer, D.; Martin, E.K.; Madad, S.; Dhagat, P.; Nuzzo, J.B. Preparedness and response to an emerging health threat—Lessons learned from Candida auris outbreaks in the United States. Infect. Control Hosp. Epidemiol. 2021, 42, 1301–1306. [Google Scholar] [CrossRef]
- Breyre, A.M.; Sloane, B.; Herring, C.; Backer, H.; McGinnis, T.; Staats, K. Establishment of an Alternate Care Site (ACS) in Imperial County During COVID-19. West. J. Emerg. Med. 2021, 22, 608–613. [Google Scholar] [CrossRef]
- Maslanka, M.; Carlson, J.C.; Gershanik, E.; Turang, Y.; Hurwitz, J.; Warren, M.; Kanter, J. Unconventional Care at a Convention Center: An Overview of Patient Focused Care at a COVID-19 Alternative Care Site in New Orleans. Disaster Med. Public Health Prep. 2021, 1–7. [Google Scholar] [CrossRef]
- Kaysin, A.; Carvajal, D.N.; Callahan, C.W. The role of alternate care sites in health system responsiveness to COVID-19. Am. J. Public Health 2020, 110, 1362–1364. [Google Scholar] [CrossRef]
- Chaudhary, M.J.; Howell, E.; Ficke, J.R.; Loffredo, A.; Wortman, L.; Benton, G.M.; Deol, G.S.; Kantsiper, M.E. Caring for Patients at a COVID-19 Field Hospital. J. Hosp. Med. 2021, 16, 117–119. [Google Scholar] [CrossRef]
- Paganini, M.; Pizzato, M.; Weinstein, E.; Vecchiato, E.; Bitetti, A.; Compostella, C.; Onesto, C.; Favaro, A. Implementation of a nurse-led alternate care site for the management of the surge of patients with COVID-19 in an Italian emergency department. Emerg. Med. J. 2022. [Google Scholar] [CrossRef]
- Bell, S.A.; Dossett, L.A.; Cespero, J.; Guntupalli, M.; Dickey, K.; Eliason, J.; Coleman, D. T-Minus 10 Days: The Role of an Academic Medical Institution in Field Hospital Planning. Prehosp. Disaster Med. 2021, 36, 338–343. [Google Scholar] [CrossRef]
- Ferrante, D.; Macchia, A.; González Villa Monte, G.A.; Battistella, G.; Baum, A.; Zingoni, P.; Angeleri, P.; Biscayart, C.; Walton, C.; Marcó, F.F.; et al. Use of alternative care sites during the COVID-19 pandemic in the city of Buenos Aires, Argentina. Public Health 2021, 194, 14–16. [Google Scholar] [CrossRef]
- Bragg, L. President Trump Declares State of Emergency COVID-19. Available online: https://www.ncsl.org/ncsl-in-dc/publications-and-resources/president-trump-declares-state-of-emergency-for-covid-19.aspx (accessed on 30 December 2021).
- Phan, P.H.; Wood, G. Doomsday scenarios (or the black swan excuse for unpreparedness). Acad. Manag. Perspect. 2020, 34, 425–433. [Google Scholar] [CrossRef]
- The Secretariat for the Independent Panel for Pandemic Preparedness and Response. Centering communities in pandemic preparedness and response. Backgr. Pap. 2021, 10, 1–36. [Google Scholar]
- Epps, F.; Wiley, Z.; Teunis, L.J.; Johnson Ii, T.M.; Patzer, R.E.; Ofotokun, I.; Franks, N. A Framework for Mobilizing Health Care to Respond to the Community within the COVID-19 Pandemic. Prev. Chronic Dis. 2021, 18, 1–7. [Google Scholar] [CrossRef]
- Cai, H.; Zilm, F.; Sheward, H.; Graham, K. Responding to COVID-19: Healthcare Surge Capacity Design for High-Consequence Infectious Disease. Technol. Archit. Des. 2020, 4, 135–139. [Google Scholar] [CrossRef]
- Facility Guidelines Institute. FGI Guidelines for the Design and Construction of Hospitals; FGI with American Society of Healthcare Engineering: Dallas, TX, USA, 2018; pp. 1–337. [Google Scholar]
- Hercules, W.J.; Anderson, D.C.; Sansom, M. Architecture—A Critical Ingredient of Pandemic Medicine: An Open Letter to Policy Makers. HERD 2020, 13, 247–252. [Google Scholar] [CrossRef]
- Sutton, S.E.; Kemp, S.P. Integrating Social Science and Design Inquiry through Interdisciplinary Design Charrettes: An Approach to Participatory Community Problem Solving. Am. J. Community Psychol. 2006, 38, 125–139. [Google Scholar] [CrossRef]
- US Army Corps of Engineers. Corona Virus Information—Alternative Care Sites. Available online: https://www.usace.army.mil/Coronavirus/ (accessed on 24 March 2020).
- CDC. Hospital Pandemic Influenza Planning Checklist. Available online: https://www.cdc.gov/flu/pandemic-resources/pdf/hospitalchecklist.pdf (accessed on 24 March 2020).
- AIA. AIA Task Force Launches Tool for Assessing COVID-19 Alternative Care Sites. Building Design and Construction: Palatine, IL, USA. Available online: https://www.bdcnetwork.com/aia-task-force-launches-tool-assessing-covid-19-alternative-care-sites (accessed on 27 July 2022).
- Wills, B.U.S. State Department to Distribute AIA COVID-19 Alternate Care Site Checklist for International Use. American Institute of Architects: Washington, DC, USA. Available online: https://www.aia.org/press-releases/6293848-us-state-department-to-distribute-aia-covi (accessed on 17 August 2022).
- Smith, A.C. Architects Are Combating COVID-19 with Site Adaptation. Architect 2020, 109, 122. [Google Scholar]
- Buildings Closed by Coronavirus Present Another Risk: Legionnaires’ Disease. Available online: https://apnews.com/article/coronavirus-pandemic-business-health-legionnaires-disease-2624ee1510c582a1add7f1cc65cc0cb0 (accessed on 21 July 2022).
- Filarski, K.; Millman, J.; Phinney, R.; Scanlon, M.M. Strategies for Safer Buildings: Re-Occupancy in the Face of COVID-19. Available online: https://aiau.aia.org/courses/strategies-safer-buildings-re-occupancy-face-covid19 (accessed on 30 December 2021).
- Gregory, D. The 2021 Clemson University Academy of Nursing Excellence in Healthcare Design Conference: Local to Global-Research, Design and Solutions for Healthcare. HERD 2021, 14, 14–17. [Google Scholar] [CrossRef]
- Tadavarthy, S.N.; Finnegan, K.; Bernatowicz, G.; Lowe, E.; Coffin, S.E.; Manning, M. Developing and implementing an infection prevention and control program for a COVID-19 alternative care site in Philadelphia, PA. Am. J. Infect. Control 2021, 49, 77–81. [Google Scholar] [CrossRef]
- Baughman, A.W.; Hirschberg, R.E.; Lucas, L.J.; Suarez, E.D.; Stockmann, D.; Hutton Johnson, S.; Hutter, M.M.; Murphy, D.J.; Marsh, R.H.; Thompson, R.W.; et al. Pandemic Care through Collaboration: Lessons from a COVID-19 Field Hospital. J. Am. Med. Dir. Assoc. 2020, 21, 1563–1567. [Google Scholar] [CrossRef]
- Bulajic, B.; Ekambaram, K.; Saunders, C.; Naidoo, V.; Wallis, L.; Amien, N.; Ras, T.; Von Pressentin, K.; Tadzimirwa, G.; Hussey, N.; et al. A COVID-19 field hospital in a conference centre—The Cape Town, South Africa experience. Afr. J. Prim. Health Care Fam. Med. 2021, 13, e1–e9. [Google Scholar] [CrossRef]
- Thompson, C.N.; Mugford, C.; Merriman, J.R.; Chen, M.A.; Hutter, J.D.; Maruna, T.J.; Bacon, W.R.; Childs, R.W.; Pati, R.; Clifton, G.T.; et al. Healthcare Worker Safety Program in a COVID-19 Alternate Care Site: The Javits New York Medical Station Experience. Infect. Control Hosp. Epidemiol. 2022, 1–24. [Google Scholar] [CrossRef]
- Brady, K.K.; Milzman, D.D.; Walton, E.E.; Sommer, D.D.; Neustadtl, A.A.; Napoli, A.A. Uniformed Services and the Field Hospital Experience during Coronovirus Disease 2019 (SARS-CoV-2) Pandemic: Open to Closure in 30 Days with 1100 Patients: The Javits New York Medical Station. Mil. Med. 2021, 187, e558–e561. [Google Scholar] [CrossRef]
- Jones, J.A.; Siddiqui, Z.K.; Callahan, C.; Leekha, S.; Smyth, S.; Preas, M.A.; Ficke, J.R.; Cabunoc, M.K.F.; Kantsiper, M.E. Infection Prevention Considerations for a Multi-Mission Convention Center Field Hospital in Baltimore, Maryland during the COVID-19 Pandemic. Disaster Med. Public Health Prep. 2021, 1–8. [Google Scholar] [CrossRef]
- Stewart, T.; Day, S.W.; Russell, J.; Wilbanks, C.; Likes, W.; Webb, S.; Haushalter, A.; Cashion, A.K. Development of a COVID-19 alternate care site from ground zero: A nursing perspective. Public Health Nurs. 2020, 37, 889–894. [Google Scholar] [CrossRef]
- Mathews, K.K.; Podlog, M.M.; Greenstein, J.J.; Cioè-Peña, E.E.; Cambria, B.B.; Ardolic, B.B.; Hahn, B.B.; Basile, J.J. Development and Implementation of an Alternate Care Site During the COVID-19 Pandemic. Curēus 2020, 12, e10799. [Google Scholar] [CrossRef]
- Spagnolello, O.; Rota, S.; Valoti, O.F.; Cozzini, C.; Parrino, P.; Portella, G.; Langer, M. Bergamo Field Hospital Confronting COVID-19: Operating Instructions. Disaster Med. Public Health Prep. 2020, 1–3. [Google Scholar] [CrossRef]
- Wang, C.Y.; Palma, M.L.; Haley, C.; Watts, J.; Hinami, K. Rapid Creation of a Multiagency Alternate Care Site for COVID-19-Positive Individuals Experiencing Homelessness. Am. J. Public Health 2021, 111, 1227–1230. [Google Scholar] [CrossRef]
- Valdenebro, J.-V.; Gimena, F.N.; López, J.J. The transformation of a trade fair and exhibition centre into a field hospital for COVID-19 patients via multi-utility tunnels. Tunn. Undergr. Space Technol. 2021, 113, 103951. [Google Scholar] [CrossRef]
- Singh, S.; Ambooken, G.C.; Setlur, R.; Paul, S.K.; Kanitkar, M.; Singh Bhatia, S.; Singh Kanwar, R. Challenges faced in establishing a dedicated 250 bed COVID-19 intensive care unit in a temporary structure. Trends Anaesth. Crit. Care 2021, 36, 9–16. [Google Scholar] [CrossRef]
- Upadhyay, A.K.; Patnaik, S.K.; Chandrasekhara, T.; Tilak, T.V.S.V.G.K.; Kushagra, P.; Singh Bhatia, S. Lessons Learnt from a Greenfield Hangar-Based 1000-Bedded Temporary Hospital in India. HERD 2022, 15, 246–263. [Google Scholar] [CrossRef]
- Xiong, Y.; Waldrop, T.; Jiang, S. 10 Dead after coronavirus quarantine hotel collapse in China. CNN, 8 March 2020. [Google Scholar]
- Taylor, E.; Quan, X.; Joseph, A. Testing a Tool to Support Safety in Healthcare Facility Design. Procedia Manuf. 2015, 3, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Taylor, E. Designing for Safety. In 2014 FGI Guidelines Update Series; Facility Guidelines Institute: St. Louis, MO, USA, 2013; pp. 1–7. [Google Scholar]
- The Center for Health Design. Safety Risk Assessment Toolkit: A Process to Mitigate Risk. Available online: https://www.healthdesign.org/sra (accessed on 3 October 2022).
- Bartley, J.M.; Olmsted, R.N.; Haas, J. Current views of health care design and construction: Practical implications for safer, cleaner environments. Am. J. Infect. Control 2010, 38, S1–S12. [Google Scholar] [CrossRef]
- McLaren, B. Pillars of Health Care Architecture. Available online: https://network.aia.org/blogs/brian-mclaren/2017/12/31/pillars-of-health-care-architecture?CommunityKey=5ac54771-1122-4d1f-ac18-d2d12d6a94fb&tab= (accessed on 23 July 2022).
- The Center for Health Design Knowledge Repository. Available online: https://www.healthdesign.org/knowledge-repository (accessed on 3 October 2022).
- Harpin, S. Creating COVID-19 alternate care site trainings for interprofessional teams. Public Health Nurs. 2020, 37, 941–945. [Google Scholar] [CrossRef]
- Proctor, C.R.; Rhoads, W.J.; Keane, T.; Salehi, M.; Hamilton, K.; Pieper, K.J.; Cwiertny, D.M.; Prévost, M.; Whelton, A.J. Considerations for large building water quality after extended stagnation. AWWA Water Sci. 2020, 2, e1186. Available online: https://awwa.onlinelibrary.wiley.com/doi/10.1002/aws2.1186 (accessed on 23 July 2022). [CrossRef]
- Scanlon, M.M.; Gordon, J.L.; McCoy, W.F.; Cain, M.F. Water management for construction: Evidence for risk characterization in community and healthcare settings: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 2168. [Google Scholar] [CrossRef] [Green Version]
- Scanlon, M.M.; Gordon, J.L.; Tonozzi, A.A.; Griffin, S.C. Reducing the Risk of Healthcare Associated Infections from Legionella and Other Waterborne Pathogens Using a Water Management for Construction (WMC) Infection Control Risk Assessment (ICRA) Tool. Infect. Dis. Rep. 2022, 14, 341–359. [Google Scholar] [CrossRef] [PubMed]
- IAPMO; AWWA. Manual of Recommended Practices for the Safe Closure and Reopening of Building Water Systems; International Association of Plumbing and Mechanical Officials: Ontario, CA, USA, 2022; pp. 1–39. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scanlon, M.; Taylor, E.; Waltz, K. Evaluating Efficacy of a COVID-19 Alternative Care Site Preparedness Assessment Tool for Catastrophic Healthcare Surge Capacity during Pandemic Response. Healthcare 2023, 11, 324. https://doi.org/10.3390/healthcare11030324
Scanlon M, Taylor E, Waltz K. Evaluating Efficacy of a COVID-19 Alternative Care Site Preparedness Assessment Tool for Catastrophic Healthcare Surge Capacity during Pandemic Response. Healthcare. 2023; 11(3):324. https://doi.org/10.3390/healthcare11030324
Chicago/Turabian StyleScanlon, Molly, Ellen Taylor, and Kirsten Waltz. 2023. "Evaluating Efficacy of a COVID-19 Alternative Care Site Preparedness Assessment Tool for Catastrophic Healthcare Surge Capacity during Pandemic Response" Healthcare 11, no. 3: 324. https://doi.org/10.3390/healthcare11030324