
The Impact of COVID-19 on Hyperhidrosis Patients in the Mental Health and Quality of Life: A Web-Based Surveillance Study



Abstract
:1. Introduction
2. Methods
2.1. Study Population and Design
2.2. Online Survey
2.3. Statistical Analysis
2.4. Ethical Statements
3. Results
3.1. Characteristics of Participants
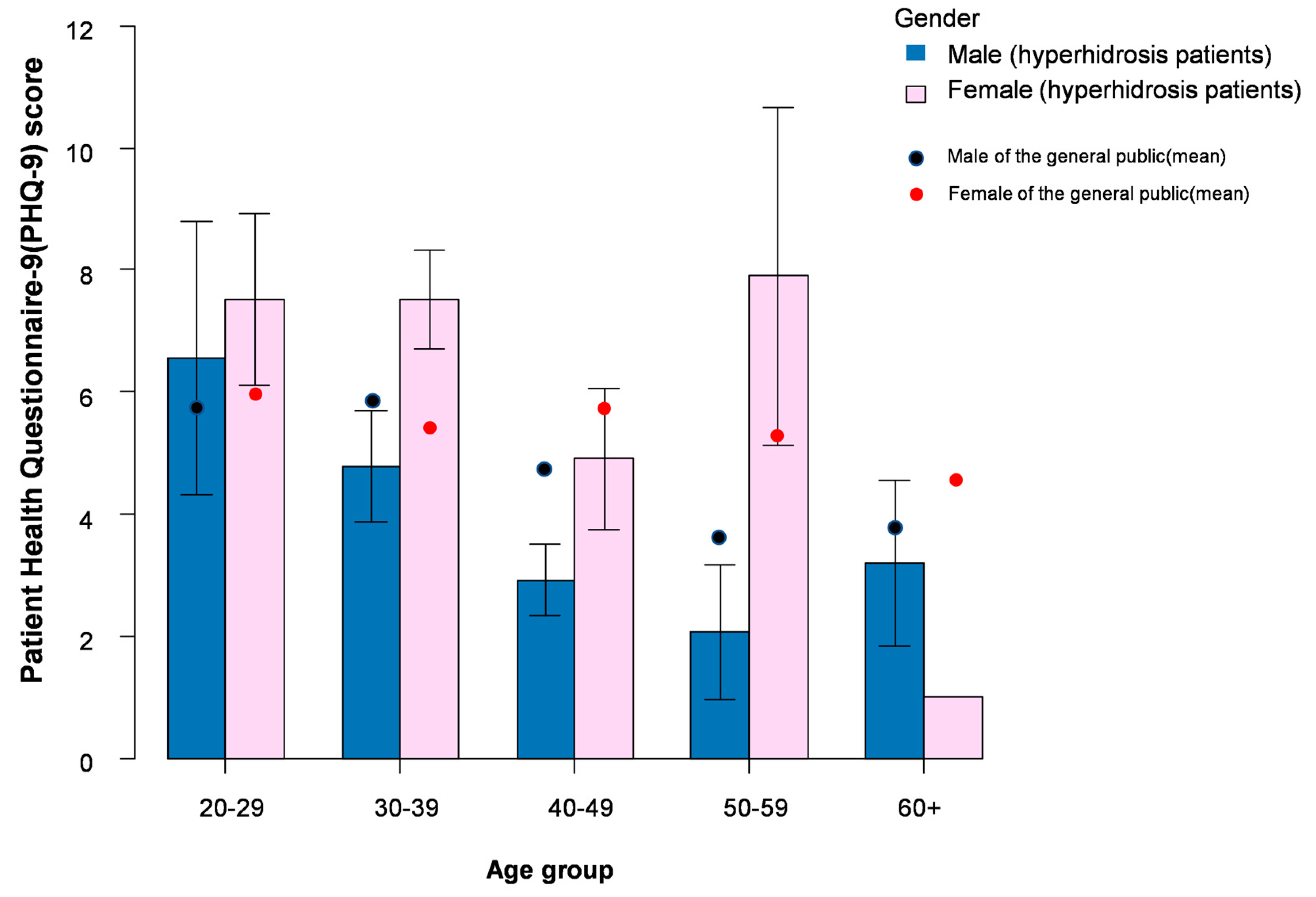
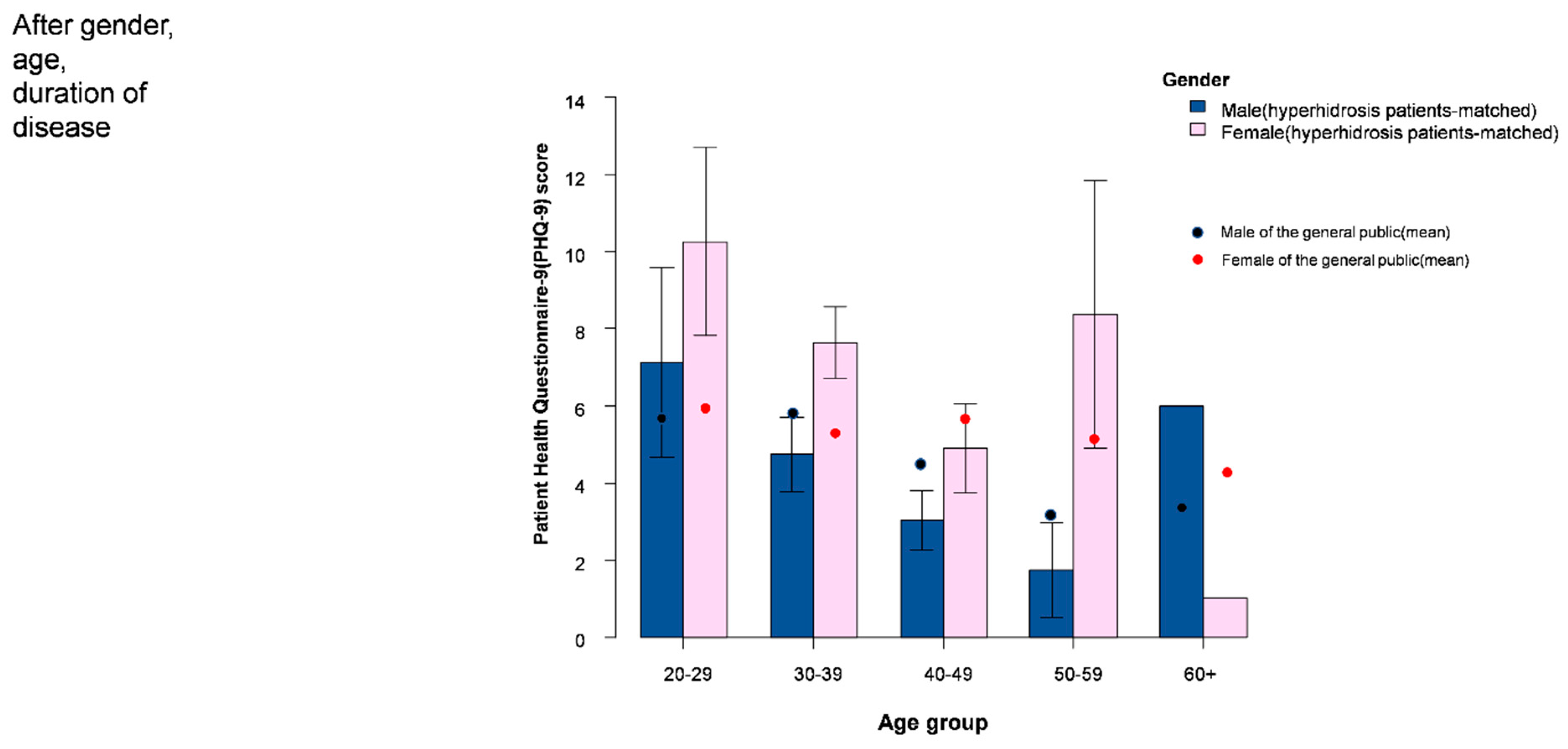
3.2. PHQ-9 Score and Relationship with Hyperhidrosis
3.3. The Effect of COVID-19 Pandemic on Patients’ Experience
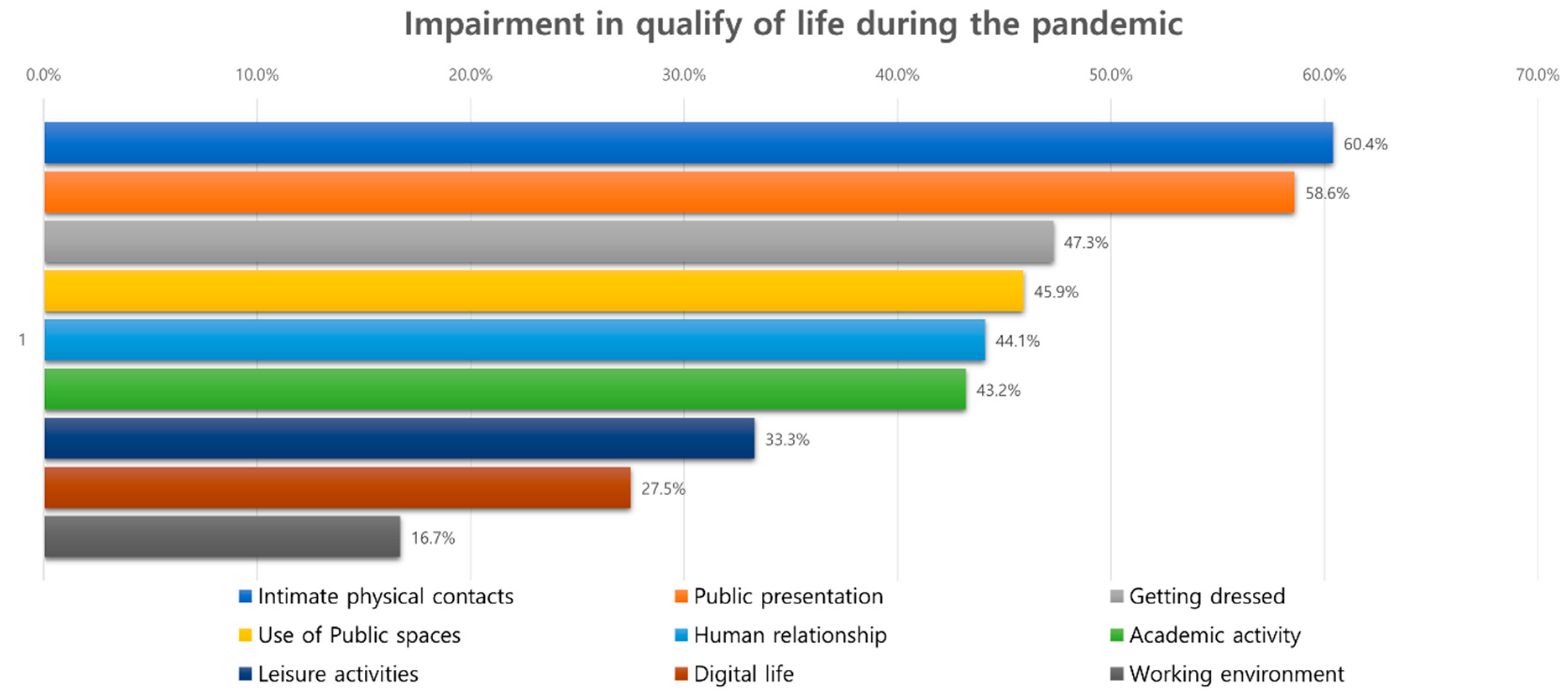
3.3.1. Quality of Life Measurements
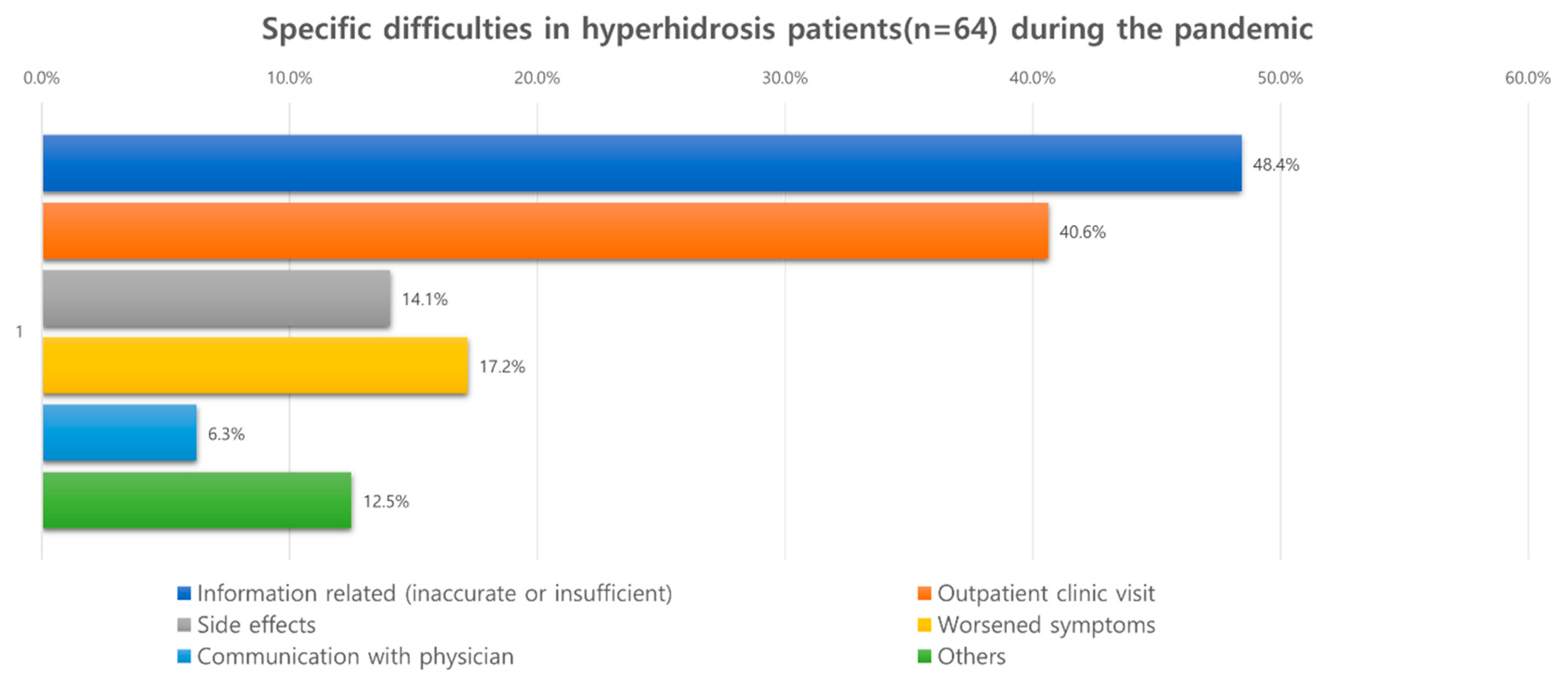
3.3.2. Treatments and Symptoms
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Y.; Chen, H.; Zhang, N.; Wang, X.; Fan, Q.; Zhang, Y.; Huang, L.; Hu, B.; Li, M. Anxiety and depression symptoms of medical staff under COVID-19 epidemic in China. J. Affect. Disord. 2020, 278, 144–148. [Google Scholar] [CrossRef]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef]
- Hyun, J.; Kim, S.; Kim, H.; Choi, Y.-J.; Lee, Y.-R.; Paik, J.-W.; Lee, J.-S.; Kim, K.; Jun, J.Y.; Lee, S.H.; et al. COVID-19 and Risk Factors of Anxiety and Depression in South Korea. Psychiatry Investig. 2021, 18, 801–808. [Google Scholar] [CrossRef]
- Lingelbach, K.; Piechnik, D.; Gado, S.; Janssen, D.; Eichler, M.; Hentschel, L.; Knopf, D.; Schuler, M.; Sernatinger, D.; Peissner, M. Effects of the COVID-19 Pandemic on Psychological Well-Being and Mental Health Based on a German Online Survey. Front. Public Health 2021, 9, 655083. [Google Scholar] [CrossRef]
- Kim, D.M.; Bang, Y.R.; Kim, J.H.; Park, J.H. The Prevalence of Depression, Anxiety and Associated Factors among the General Public during COVID-19 Pandemic: A Cross-sectional Study in Korea. J. Korean Med. Sci. 2021, 36, e214. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Sil, A.; Jaiswal, S.; Rajeev, R.; Thole, A.; Jafferany, M.; Ali, S.N. A Study to Evaluate Depression and Perceived Stress Among Frontline Indian Doctors Combating the COVID-19 Pandemic. Prim. Care Companion CNS Disord. 2020, 22, 26168. [Google Scholar] [CrossRef]
- Fonseca, E.; Quintana, M.; Lallana, S.; Luis Restrepo, J.; Abraira, L.; Santamarina, E.; Seijo-Raposo, I.; Toledo, M. Epilepsy in time of COVID-19: A sur-vey-based study. Acta Neurol. Scand. 2020, 142, 545–554. [Google Scholar] [CrossRef]
- Bahar, R.; Zhou, P.; Liu, Y.; Huang, Y.; Phillips, A.; Lee, T.K.; Su, M.; Yang, S.; Kalia, S.; Zhang, X.; et al. The prevalence of anxiety and depression in patients with or without hyperhidrosis (HH). J. Am. Acad. Dermatol. 2016, 75, 1126–1133. [Google Scholar] [CrossRef]
- Bragança, G.M.G.; Lima, S.O.; Neto, A.F.P.; Marques, L.M.; de Melo, E.V.; Reis, F.P. Evaluation of anxiety and depression prevalence in patients with primary severe hyperhidrosis. An. Bras. Dermatol. 2014, 89, 230–235. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.Z.; Hull, M.; Gillard, K.K.; Peterson-Brandt, J. Treatment Patterns, Depression, and Anxiety Among US Patients Diagnosed with Hyperhidrosis: A Retrospective Cohort Study. Dermatol. Ther. 2020, 10, 1299–1314. [Google Scholar] [CrossRef]
- Kristensen, J.K.; Möller, S.; Vestergaard, D.G.; Horsten, H.-H.; Swartling, C.; Bygum, A. Anxiety and Depression in Primary Hyper-hidrosis: An Observational Study of 95 Consecutive Swedish Outpatients. Acta Derm. Venereol. 2020, 100, adv00240. [Google Scholar] [CrossRef]
- Shayesteh, A.; Boman, J.; Janlert, U.; Brulin, C.; Nylander, E. Primary hyperhidrosis: Implications on symptoms, daily life, health and alcohol consumption when treated with botulinum toxin. J. Dermatol. 2016, 43, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Ruchinskas, R.; Narayan, R.; Meagher, R.; Furukawa, S. The relationship of psychopathology and hyperhidrosis. Br. J. Dermatol. 2002, 147, 733–735. [Google Scholar] [CrossRef]
- Li, D.C.; Hulbert, A.; Waldbaum, B.; Ober, C.; Hooker, C.M.; Huang, P.; Molena, D.; Yang, S.C.; Ito, T.; Perry-Parrish, C.; et al. Endoscopic thoracic sympathectomy for primary focal hyperhidrosis: Impact on psycho-social symptomatology and psychotropic medication use. Eur. J. Cardio-Thoracic Surg. 2018, 54, 904–911. [Google Scholar] [CrossRef]
- Hirakawa, N.; Higashimoto, I.; Takamori, A.; Tsukamoto, E.; Uemura, Y. The impact of endoscopic thoracic sympathectomy on sudomotor function in patients with palmar hyperhidrosis. Clin. Auton. Res. 2021, 31, 225–230. [Google Scholar] [CrossRef]
- Ureña, A.; Masuet-Aumatell, C.; Escobar, I.; Villalonga, R.; Moya, J.; Ramos, R.; Rivas, F.; Macia, I. An assessment of plantar hyperhidrosis after endoscopic thoracic sympathicolysis. Eur. J. Cardio-Thoracic Surg. 2009, 36, 360–363. [Google Scholar] [CrossRef] [Green Version]
- Weber, A.; Heger, S.; Sinkgraven, R.; Heckmann, M.; Elsner, P.; Rzany, B. Psychosocial aspects of patients with focal hyperhidrosis. Marked reduction of social phobia, anxiety and depression and increased quality of life after treatment with botulinum toxin A. Br. J. Dermatol. 2005, 152, 342–345. [Google Scholar] [CrossRef]
- Turkmen, D.; Altunisik, N.; Sener, S.; Colak, C. Evaluation of the effects of COVID-19 pandemic on hair diseases through a web-based questionnaire. Dermatol. Ther. 2020, 33, e13923. [Google Scholar] [CrossRef]
- Korean Ministry of Public health and Welfare—the Fourth Assessment of Mental Well-Being of Korean Populations, Collaborating with Korean Association of Stress and Trauma. 2021. Available online: http://kstss.kr/?p=2065 (accessed on 14 January 2022).
- Hu, Y.; Chen, Y.; Zheng, Y.; You, C.; Tan, J.; Hu, L.; Zhang, Z.; Ding, L. Factors related to mental health of inpatients with COVID-19 in Wuhan, China. Brain Behav. Immun. 2020, 89, 587–593. [Google Scholar] [CrossRef]
- Hyland, P.; Shevlin, M.; McBride, O.; Murphy, J.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. Anxiety and depression in the Republic of Ireland during the COVID-19 pandemic. Acta Psychiatr. Scand. 2020, 142, 249–256. [Google Scholar] [CrossRef]
- Shayesteh, A.; Janlert, U.; Nylander, E. Hyperhidrosis—Sweating Sites Matter: Quality of Life in Primary Hyperhidrosis according to the Sweating Sites Measured by SF-36. Dermatology 2017, 233, 441–445. [Google Scholar] [CrossRef]
- Pohjavaara, P.; Telaranta, T.; Väisänen, E. The role of the sympathetic nervous system in anxiety: Is it possible to relieve anxiety with endoscopic sympathetic block? Nord. J. Psychiatry. 2003, 57, 55–60. [Google Scholar] [CrossRef]
- Fukuda, J.M.; Varella, A.Y.M.; Teivelis, M.P.; de Campos, J.R.M.; Kauffman, P.; Pinheiro, L.L.; Wolosker, N. Video-Assisted Thoracoscopic Sym-pathectomy for Facial Hyperhidrosis: The Influence of the Main Site of Complaint. Ann. Vasc. Surg. 2018, 46, 337–344. [Google Scholar] [CrossRef]
- Smidfelt, K.; Drott, C. Late results of endoscopic thoracic sympathectomy for hyperhidrosis and facial blushing. Br. J. Surg. 2011, 98, 1719–1724. [Google Scholar] [CrossRef]
- Tomitaka, S.; Kawasaki, Y.; Ide, K.; Akutagawa, M.; Ono, Y.; Furukawa, T.A. Stability of the Distribution of Patient Health Questionnaire-9 Scores Against Age in the General Population: Data from the National Health and Nutrition Examination Survey. Front. Psychiatry 2018, 9, 390. Available online: https://www.frontiersin.org/article/10.3389/fpsyt.2018.00390 (accessed on 1 October 2021). [CrossRef]
- Zhang, X.-J.; Wang, A.-P.; Shi, T.-Y.; Zhang, J.; Xu, H.; Wang, D.-Q.; Feng, L. The psychosocial adaptation of patients with skin disease: A scoping review. BMC Public Health 2019, 19, 1404. [Google Scholar] [CrossRef]
- Teuschl, Y.; Bancher, C.; Brainin, M.; Dachenhausen, A.; Matz, K.; Pinter, M.M. COVID-19-related delays of botulinum toxin injections have a negative impact on the quality of life of patients with dystonia and spasticity: A single-center ambulatory care study. J. Neural Transm. 2021, 129, 49–53. [Google Scholar] [CrossRef]
- Gisondi, P.; Piaserico, S.; Conti, A.; Naldi, L. Dermatologists and SARS-CoV-2: The impact of the pandemic on daily practice. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1196–1201. [Google Scholar] [CrossRef]
- Kartal, S.P.; Çelik, G.; Sendur, N.; Aytekin, S.; Serdaroğlu, S.; Doğan, B.; Yazıcı, A.C.; Çiçek, D.; Borlu, M.; Kaçar, N.G.; et al. Multicenter study evaluating the impact of COVID-19 outbreak on dermatology outpatients in Turkey. Dermatol. Ther. 2020, 33, e14485. [Google Scholar] [CrossRef]
- Demirel Öğüt, N.; Tabak, G.H.; Gülseren, D.; Yalıcı-Armağan, B.; Akdoğan, N.; Doğan, S.; Doğan, S.; Elçin, G.; Karaduman, A.; Evans, S.E.; et al. The effect of the COVID-19 pandemic on dermatology consultation requests from adult and paediatric emergency departments. Int. J. Clin. Pract. 2021, 75, e14906. [Google Scholar] [CrossRef]
- Chudry, H. The treatment of palmar hyperhidrosis—A systematic review. Int. J. Dermatol. 2021; ahead of print. [Google Scholar] [CrossRef]
- Choudhary, N.; Lahiri, K.; Singh, M. Increase and consequences of self-medication in dermatology during COVID -19 pandemic: An initial observation. Dermatol. Ther. 2020, 34, e14696. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Male | Female | p Value | |
|---|---|---|---|---|
| n = 222 | n = 111 | n = 111 | ||
| Demographics | ||||
| Age | 39.00 [31.25, 45.00] | 42.00 [34.00, 47.00] | 37.00 [29.00, 43.00] | 0.001 |
| Age group | 0.001 | |||
| 20–29 | 38 (17.1) | 9 (8.1) | 29 (26.1) | |
| 30–39 | 77 (34.7) | 37 (33.3) | 40 (36.0) | |
| 40–49 | 77 (34.7) | 46 (41.4) | 31 (27.9) | |
| 50–59 | 24 (10.8) | 14 (12.6) | 10 (9.0) | |
| 60+ | 6 (2.7) | 5 (4.5) | 1 (0.9) | |
| BMI | 23.10 [21.20, 25.60] | 24.70 [23.00, 26.70] | 21.80 [20.15, 23.50] | <0.001 |
| Marital status | 0.033 | |||
| married | 109 (49.1) | 63 (56.8) | 45 (40.5) | |
| divorced | 5 (2.3) | 1 (0.9) | 4 (3.6) | |
| unmarried | 108 (48.6) | 47 (42.3) | 61 (55.0) | |
| Residential area | ||||
| Small town | 72 (32.4) | 38 (34.2) | 34 (30.6) | 0.667 |
| Urban/Metropolitan area | 150 (67.6) | 73 (65.8) | 77 (69.4) | |
| Depression related | ||||
| PHQ-9 mean (SD) | 5.25 (5.97) | 3.74 (4.89) | 6.77 (6.56) | <0.001 |
| PHQ-9 median (IQR) | 3.5 [1.0, 8.0] | 2.00 [0.00, 6.00] | 5.00 [2.00, 10.00] | <0.001 |
| Mild Depression ¶ | 90 (40.5) | 34 (30.6) | 56 (50.5) | 0.004 |
| Moderate Depression ⁑ | 48 (21.6) | 16 (14.4) | 32 (28.8) | 0.014 |
| Hyperhidrosis related | ||||
| Duration of disease | 29.0 [20.0, 34.0] | 30.00 [20.00, 35.00] | 26.00 [20.00, 33.50] | 0.061 |
| Location of hyperhidrosis | ||||
| Axilla | 111 (50.0) | 45 (40.5) | 66 (59.5) | 0.007 |
| Palmar | 161 (72.5) | 76 (68.5) | 85 (76.6) | 0.229 |
| Plantar | 164 (73.9) | 78 (70.3) | 86 (77.5) | 0.285 |
| Facial | 82 (36.9) | 44 (39.6) | 38 (34.2) | 0.487 |
| Multiple | 188 (84.7) | 88 (79.3) | 100 (90.1) | 0.039 |
| Other areas | 42 (18.9) | 20 (18.0) | 22 (19.8) | 0.864 |
| Comorbidity ⁂ | ||||
| Gastrointestinal diseases | 84 (37.8) | 36 (32.4) | 48 (43.2) | 0.128 |
| Obesity | 62 (27.9) | 33 (29.7) | 29 (26.1) | 0.654 |
| Anxiety | 44 (19.8) | 18 (16.2) | 26 (23.4) | 0.238 |
| Depression | 44 (19.8) | 15 (13.5) | 29 (26.1) | 0.028 |
| Hypertension | 27 (12.2) | 22 (19.8) | 5 (4.5) | 0.001 |
| Diabetes mellitus | 8 (3.6) | 6 (5.4) | 2 (1.8) | 0.280 |
| Neurologic disorder | 17 (7.7) | 9 (8.1) | 8 (7.2) | 1 |
| Factor | Estimate | Standard Error | t Value | p Value |
|---|---|---|---|---|
| (Intercept) | 8.16 (0.39 to 15.93) | 3.94 | 2.07 | 0.040 |
| Age | −0.08 (−0.18 to 0.02) | 0.05 | −1.67 | 0.096 |
| BMI | −0.06 (−0.31 to 0.19) | 0.13 | −0.46 | 0.640 |
| Marital status [single or divorced] | 1.66 (−0.16 to 3.48) | 0.92 | 1.8 | 0.074 |
| Gender [female] | 2.36 (0.7 to 4.03) | 0.84 | 2.79 | 0.006 |
| Residential area [urban/metropolitan] | −1.98 (−3.61 to −0.35) | 0.83 | −2.4 | 0.017 |
| Axillary hyperhidrosis | 0.63 (−0.9 to 2.17) | 0.78 | 0.81 | 0.420 |
| Facial hyperhidrosis | 1.87 (0.25 to 3.5) | 0.83 | 2.27 | 0.024 |
| Total | Male | Female | p Value | |
|---|---|---|---|---|
| n = 222 | n = 111 | n = 111 | ||
| Quality of life problems | ||||
| Use of public spaces, (%) | 102 (45.9) | 43 (38.7) | 59 (53.2) | 0.043 |
| Working environments (%) | 37 (16.7) | 12 (10.8) | 25 (22.5) | 0.030 |
| Interpersonal relationship (%) | 98 (44.1) | 38 (34.2) | 60 (54.1) | 0.004 |
| Public speaking or presentation (%) | 130 (58.6) | 52 (46.8) | 78 (70.3) | 0.001 |
| Digital life ¶ (%) | 61 (27.5) | 25 (22.5) | 36 (32.4) | 0.132 |
| Intimate personal contacts (%) | 134 (60.4) | 59 (53.2) | 75 (67.6) | 0.039 |
| Dressing (%) | 105 (47.3) | 43 (38.7) | 62 (55.9) | 0.015 |
| Hobbies and leisure activity (%) | 74 (33.3) | 30 (27.0) | 44 (39.6) | 0.064 |
| Academic activity (%) | 96 (43.2) | 40 (36.0) | 56 (50.5) | 0.042 |
| Change in symptoms | 0.750 | |||
| Improved | 9 (4.1) | 5 (4.5) | 4 (3.6) | |
| Same as usual | 190 (85.6) | 96 (86.5) | 94 (84.7) | |
| Worsened | 23 (10.4) | 10 (9.0) | 13 (11.7) | |
| Problems in treatments during the pandemic | ||||
| No problem | 158 (71.2) | 82 (73.9) | 76 (68.5) | 0.459 |
| Information related issues | 31 (14.0) | 15 (13.5) | 16 (14.4) | 1 |
| Inaccurate information | 12 (5.4) | 8 (7.2) | 4 (3.6) | 0.374 |
| Insufficient information | 26 (11.7) | 11 (9.9) | 15 (13.5) | 0.532 |
| Visit to outpatient clinics | 26 (11.7) | 13 (11.7) | 13 (11.7) | 1 |
| Side effects | 9 (4.1) | 4 (3.6) | 5 (4.5) | 1 |
| Communication with physicians | 4 (1.8) | 3 (2.7) | 1 (0.9) | 0.622 |
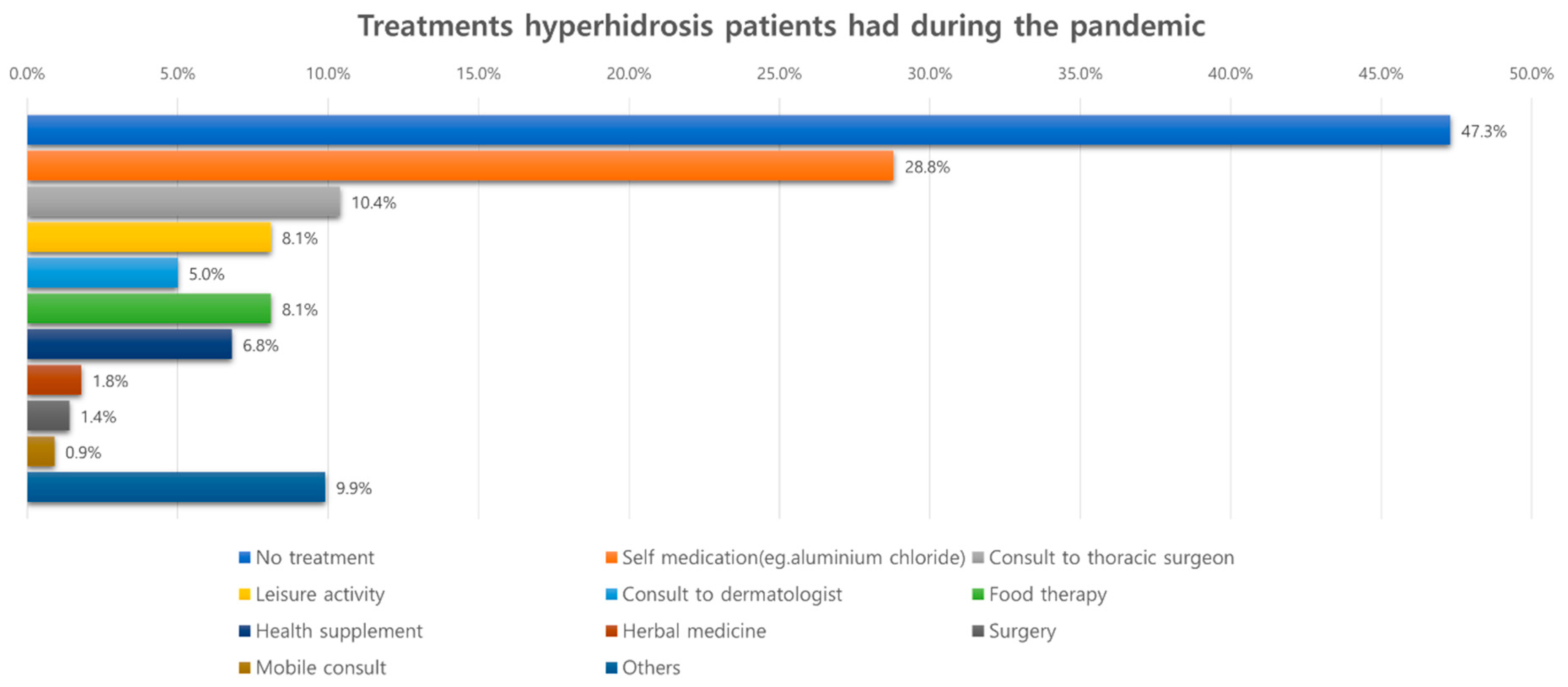
| Treatments received during the pandemic | ||||
| No treatment | 105 (47.3) | 62 (55.9) | 43 (38.7) | 0.015 |
| Self-medication ⁂ | 64 (28.8) | 23 (20.7) | 41 (36.9) | 0.011 |
| OPD visit to thoracic surgeons | 23 (10.4) | 10 (9.0) | 13 (11.7) | 0.660 |
| OPD visit to dermatologist | 11 (5.0) | 5 (4.5) | 6 (5.4) | 1 |
| Surgery | 3 (1.4) | 3 (2.7) | 0 (0.0) | 0.247 |
| Diet therapy | 18 (8.1) | 8 (7.2) | 10 (9.0) | 0.807 |
| Leisure activity | 18 (8.1) | 7 (6.3) | 11 (9.9) | 0.462 |
| Herbal medicine | 4 (1.8) | 1 (0.9) | 3 (2.7) | 0.622 |
| Mobile consultation | 2 (0.9) | 0 (0.0) | 2 (1.8) | 0.498 |
| Health supplement | 15 (6.8) | 6 (5.4) | 9 (8.1) | 0.594 |
| Others | 22 (9.9) | 9 (8.1) | 13 (11.7) | 0.501 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo, W.; Oh, J.; Kim, B.J.; Won, J.; Moon, D.H.; Lee, S. The Impact of COVID-19 on Hyperhidrosis Patients in the Mental Health and Quality of Life: A Web-Based Surveillance Study. J. Clin. Med. 2022, 11, 3576. https://doi.org/10.3390/jcm11133576
Woo W, Oh J, Kim BJ, Won J, Moon DH, Lee S. The Impact of COVID-19 on Hyperhidrosis Patients in the Mental Health and Quality of Life: A Web-Based Surveillance Study. Journal of Clinical Medicine. 2022; 11(13):3576. https://doi.org/10.3390/jcm11133576
Chicago/Turabian StyleWoo, Wongi, Jooyoung Oh, Bong Jun Kim, Jongeun Won, Duk Hwan Moon, and Sungsoo Lee. 2022. "The Impact of COVID-19 on Hyperhidrosis Patients in the Mental Health and Quality of Life: A Web-Based Surveillance Study" Journal of Clinical Medicine 11, no. 13: 3576. https://doi.org/10.3390/jcm11133576