
Anakinra versus Baricitinib: Different Strategies for Patients Hospitalized with COVID-19 †

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
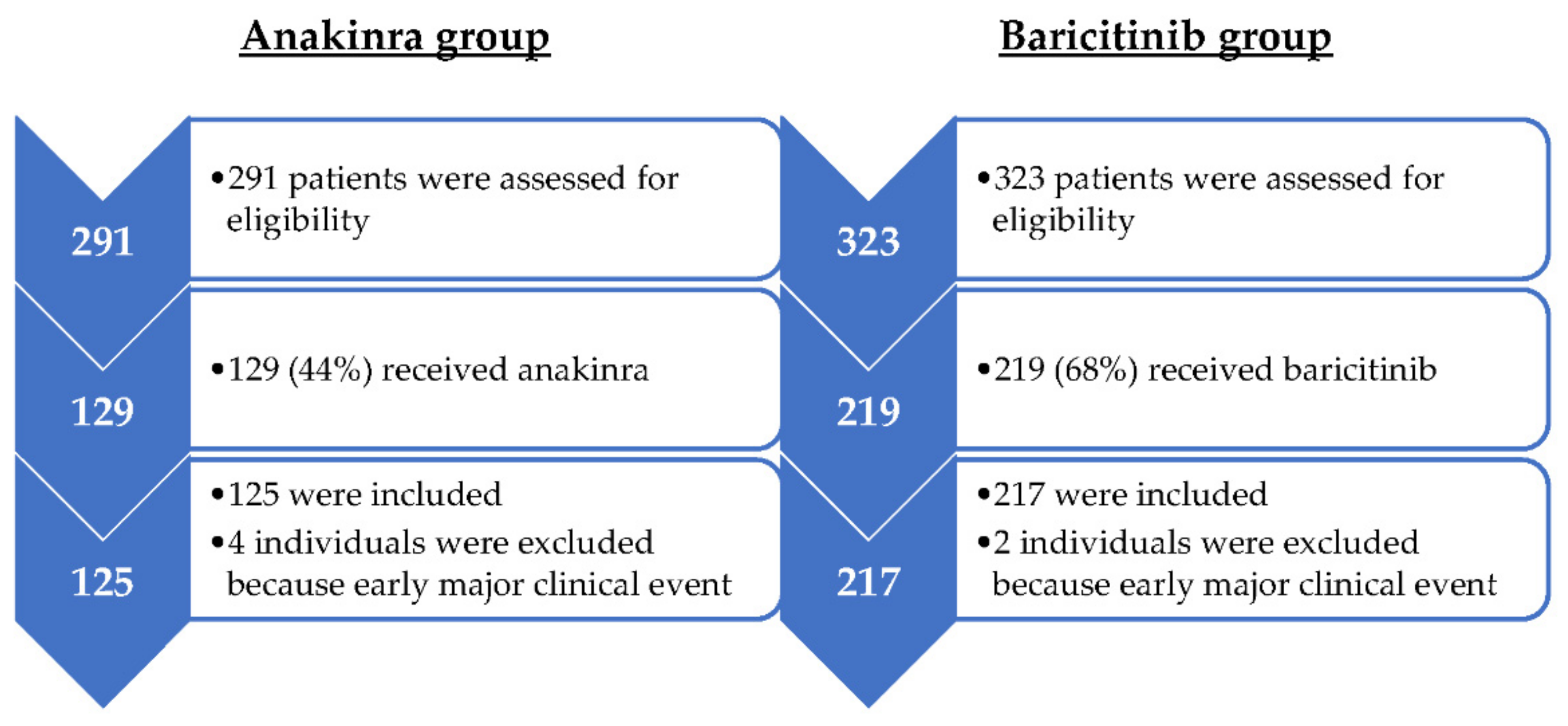
2.1. Design and Patients
2.2. Variables and Follow-Up
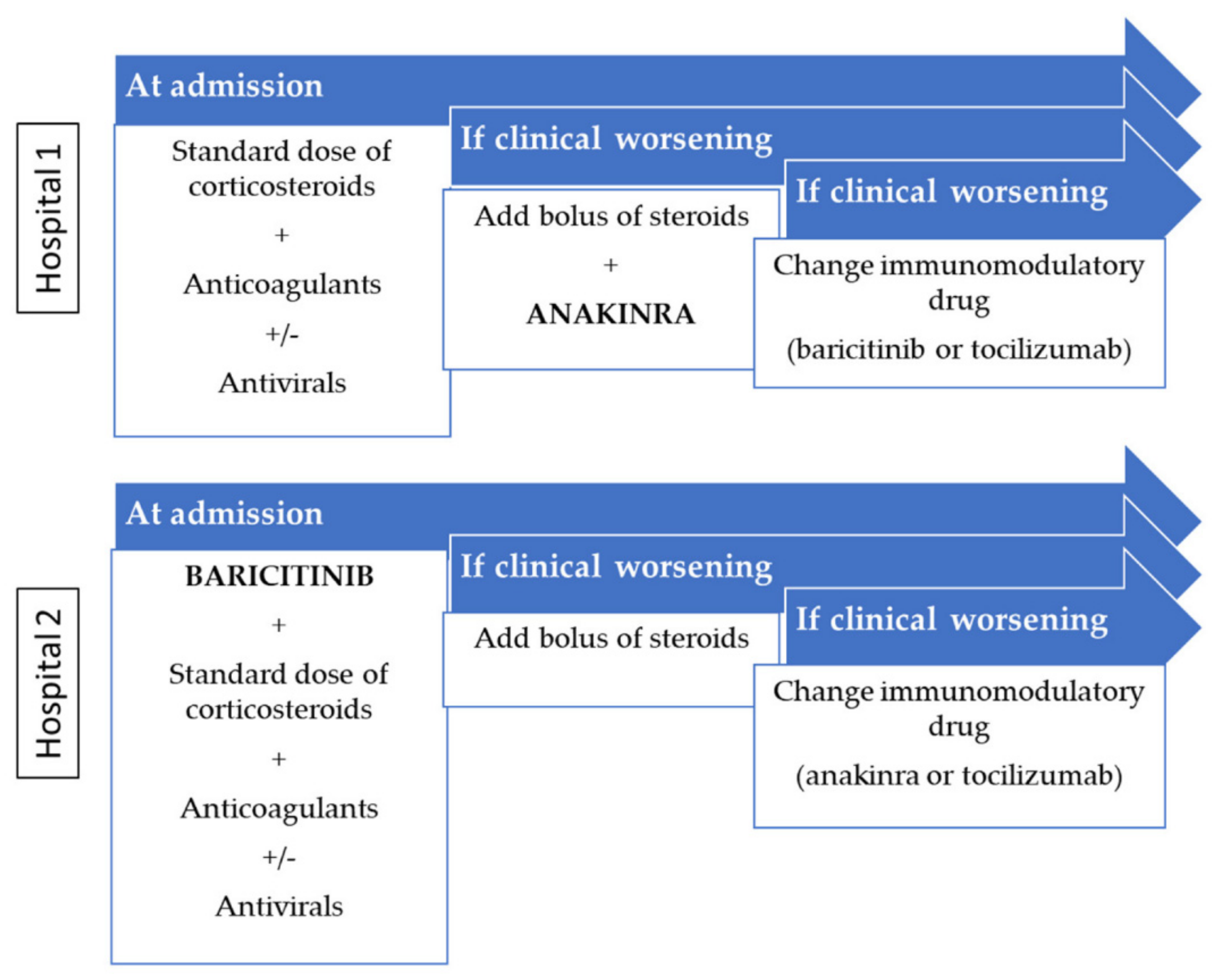
2.3. Treatments
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Treatments
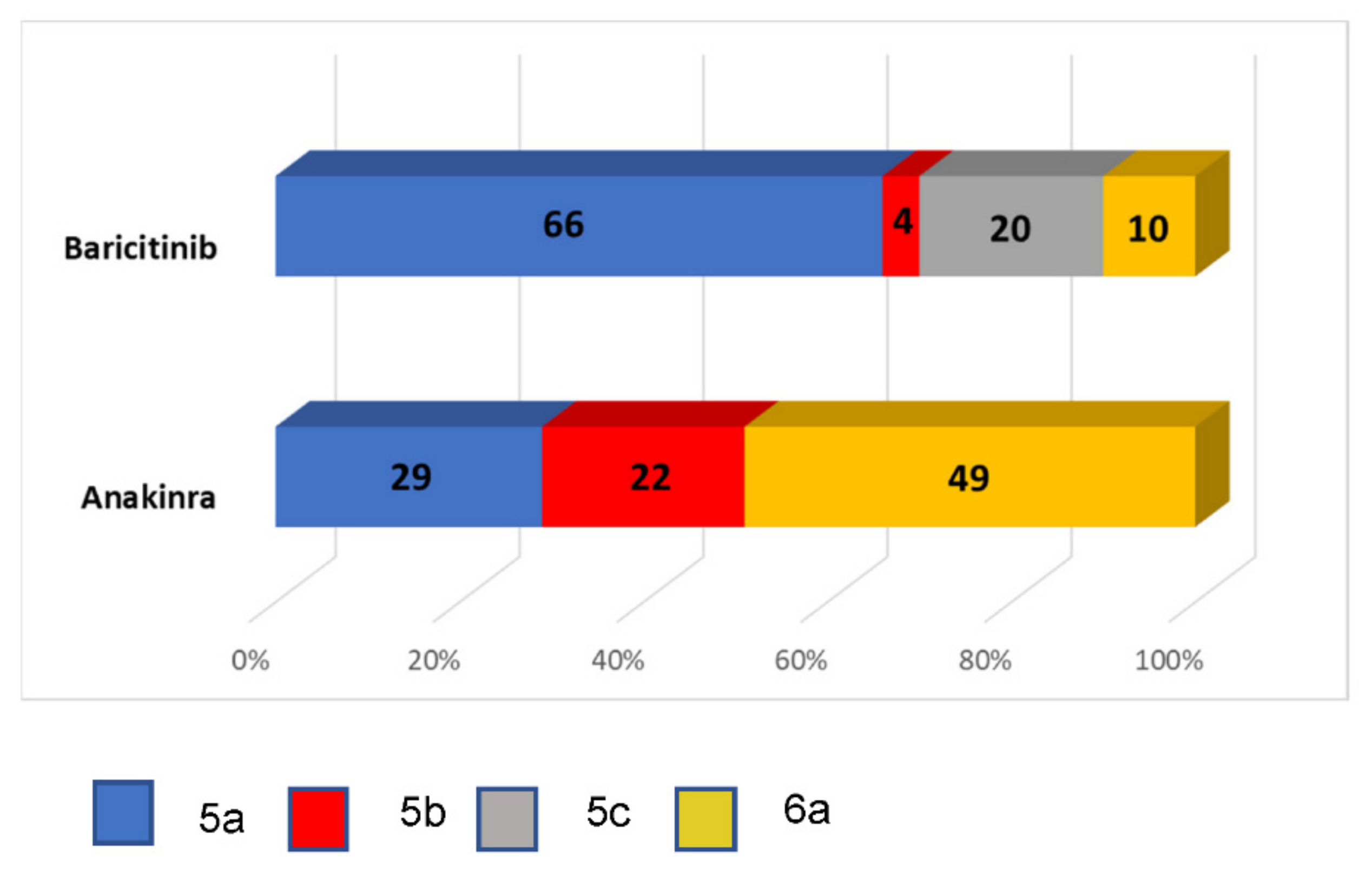
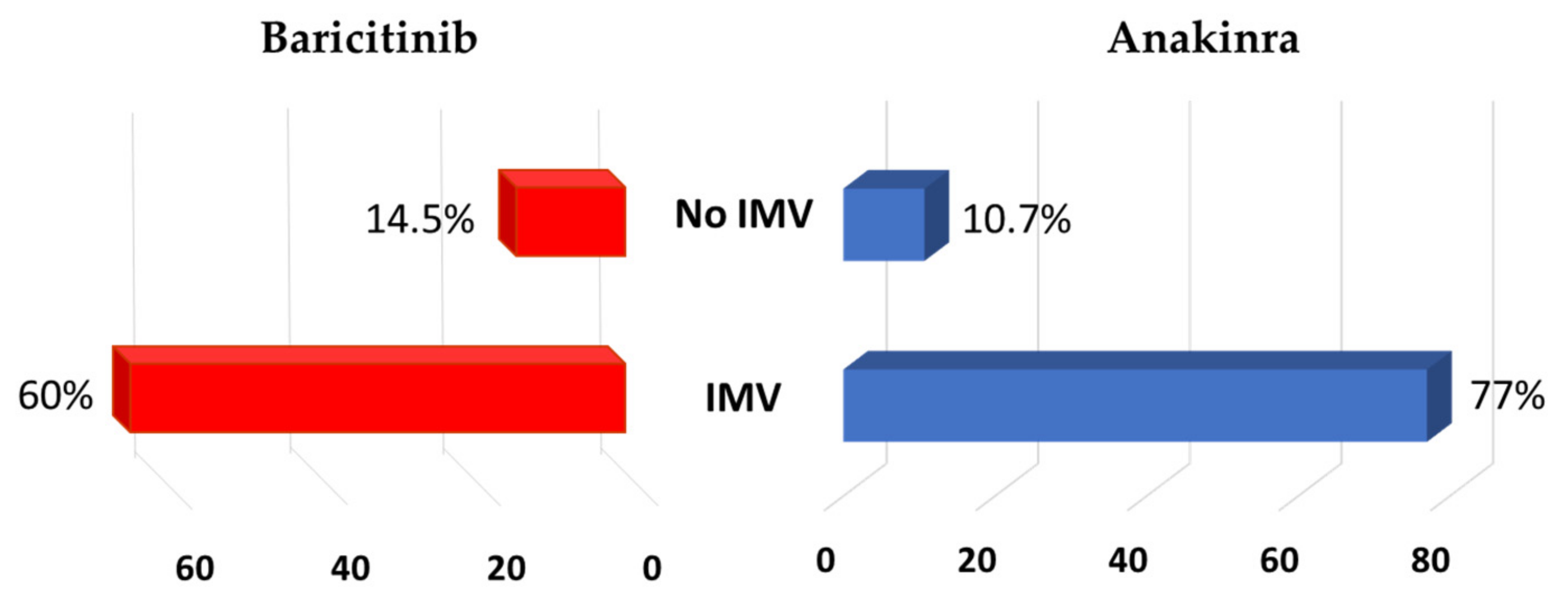
3.3. Outcome Events
3.3.1. Immunomodulatory Drug
3.3.2. Multivariate Analysis
3.3.3. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chan, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.S.; Lee, J.Y.; Yang, J.W.; Lee, K.H.; Effenberger, M.; Szpirt, W.; Kronbichler, E.; Shin, J.I. Immunopathogenesis and treatment of cytokine storm in COVID-19. Theranostics 2021, 11, 316–329. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Dexamethasone in hospitalized patients with Covid-19-preliminary report. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Fadel, R.; Morrison, A.R.; Vahia, A.; Smith, Z.R.; Chaudhry, Z.; Bhargava, P.; Miller, J.; Kenney, R.M.; Alangaden, G.; Ramesh, M.S.; et al. Early short course corticosteroids in hospitalized patients with COVID-19. Clin. Infect. Dis. 2020, 71, 2114–2120. [Google Scholar] [CrossRef]
- Ruiz-Irastorza, G.; Pijoan, J.-I.; Bereciartua, E.; Dunder, S.; Dominguez, J.; Garcia-Escudero, P.; Rodrigo, A.; Gomez-Carballo, C.; Varona, J.; Guio, L.; et al. Second week methyl-prednisolone pulses improve prognosis in patients with severe coronavirus disease 2019 pneumonia: An observational comparative study using routine care data. PLoS ONE 2020, 15, e0239401. [Google Scholar] [CrossRef]
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet Infect. Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Hertanto, D.M.; Sutanto, H.; Wiratama, B.S.; Wungu, C.D.K. Modulating the host immune response to fight against COVID-19: Where are we in 2021? Virulence 2021, 12, 1732–1736. [Google Scholar] [CrossRef]
- Guerson-Gil, A.; Palaiodimos, L.; Assa, A.; Karamanis, D.; Kokkinidis, D.; Chamorro-Pareja, N.; Kishor, P.; Leider, J.M.; Brandt, L.J. Sex-specific impact of severe obesity in the outcomes of hospitalized patients with COVID-19: A large retrospective study from the Bronx, New York. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1963–1974. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Li, M.; Zhou, Z.; Guan, X.; Xiang, Y. Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)? J. Autoimmun. 2020, 111, 102452. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, F.D.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs standard care on clinical worsening in patients hospitalized with COVID-19 Pneumonia: A randomized clinical trial. JAMA Intern. Med. 2021, 181, 24–31. [Google Scholar] [CrossRef]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of tocilizumab in patients hospitalized with Covid-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef]
- Salama, C.; Han, J.; Yau, L.; Reiss, W.G.; Kramer, B.; Neidhart, J.D.; Criner, G.J.; Kaplan-Lewis, E.; Baden, R.; Pandit, L.; et al. Tocilizumab in patients hospitalized with Covid-19 pneumonia. N. Engl. J. Med. 2021, 384, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; van Bentum Puijk, W.; Berry, L.R.; et al. Interleukin-6 receptor antagonists in critically ill patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef]
- Campochiaro, C.; Della-Torre, E.; Cavalli, G.; De Luca, G.; Ripa, M.; Boffini, N.; Tomelleri, A.; Baldissera, E.; Rovere-Querini, P.; Ruggeri, A.; et al. Efficacy and safety of tocilizumab in severe COVID-19 patients: A single-centre retrospective cohort study. Eur. J. Intern. Med. 2020, 76, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Van de Veerdonk, F.L.; Netea, M.G. Blocking IL-1 to prevent respiratory failure in COVID-19. Crit. Care 2020, 24, 445. [Google Scholar] [CrossRef]
- Cavalli, G.; Dinarello, C.A. Anakinra therapy for non-cancer inflammatory diseases. Front Pharmacol. 2018, 9, 1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalli, G.; De Luca, G.; Campochiaro, C.; Della-Torre, E.; Ripa, M.; Canetti, D.; Oltolini, C.; Castiglioni, B.; Din, C.T.; Boffini, N.; et al. Interleukin-1 blockade with high-dose anakinra in patients with COVID-19, acute respiratory distress syndrome, and hyperinflammation: A retrospective cohort study. Lancet Rheumatol. 2020, 6, e325–e331. [Google Scholar] [CrossRef]
- Huet, T.; Beaussier, H.; Voisin, O.; Jouveshomme, S.; Dauriat, G.; Lazareth, I.; Sacco, E.; Naccache, J.M.; Bézie, Y.; Laplanche, S.; et al. Anakinra for severe forms of COVID-19: A cohort study. Lancet Rheumatol. 2020, 2, e393–e400. [Google Scholar] [CrossRef]
- Balkhair, A.; Al-Zakwani, I.; Al Busaidi, M.; Al-Khirbash, A.; Al Mubaihsi, S.; BaTaher, H.; Al Aghbari, J.; Al Busaidi, I.; Al Kindi, M.; Baawain, S.; et al. Anakinra in hospitalized patients with severe COVID-19 pneumonia requiring oxygen therapy: Results of a prospective, open-label, interventional study. Int. J. Infect. Dis. 2021, 103, 288–296. [Google Scholar] [CrossRef]
- Bozzi, G.; Mangioni, D.; Minoia, F.; Aliberti, S.; Grasselli, G.; Barbetta, L.; Castelli, V.; Palomba, E.; Alagna, L.; Lombardi, A.; et al. Anakinra combined with methylprednisolone in patients with severe COVID-19 pneumonia and hyperinflammation: An observational cohort study. J. Allergy Clin. Immunol. 2021, 147, 561–566.e4. [Google Scholar] [CrossRef] [PubMed]
- Pasin, L.; Cavalli, G.; Navalesi, P.; Sella, N.; Landoni, G.; Yavorovskiy, A.G.; Likhvantsev, V.V.; Zangrillo, A.; Dagna, L.; Monti, G. Anakinra for patients with COVID-19: A meta-analysis of non-randomized cohort studies. Eur. J. Intern. Med. 2021, 86, 34–40. [Google Scholar] [CrossRef]
- Zegeye, M.M.; Madelene, L.; Knut, F.; Kumawat, A.K.; Paramel, G.; Grenegard, M.; Sirsjö, A.; Ljungberg, L.U. Activation of the JAK/STAT3 and PI3K/AKT pathways are crucial for IL-6 trans-signaling-mediated pro-inflammatory response in human vascular endothelial cells. Cell Commun. Signal. 2018, 16, 55. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, Y.; Qiao, W.; Zhang, J.; Qi, Z. Baricitinib, a drug with potential effect to prevent SARS-COV-2 from entering target cells and control cytokine storm induced by COVID-19. Int. Immunopharmacol. 2020, 86, 106749. [Google Scholar] [CrossRef]
- Rodriguez-Garcia, J.L.; Sanchez-Nievas, G.; Arevalo-Serrano, J.; Garcia-Gomez, C.; Jimenez-Vizuete, J.M.; Martinez-Alfaro, E. Baricitinib improves respiratory function in patients treated with corticosteroids for SARS-CoV-2 pneumonia: An observational cohort study. Rheumatology 2021, 60, 399–407. [Google Scholar] [CrossRef]
- Cantini, F.; Niccoli, L.; Nannini, C.; Matarrese, D.; Di Natale, M.E.; Lotti, P.; Aquilini, D.; Landini, G.; Cimolato, B.; Di Pietro, M.A.; et al. Beneficial impact of baricitinib in COVID-19 moderate pneumonia; multicentre study. J. Infect. 2020, 81, 647–679. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus remdesivir for hospitalized adults with Covid-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef] [PubMed]
- The CORIMUNO-19 Collaborative Group. Effect of anakinra versus usual care in adults in hospital with COVID-19 and mild-to-moderate pneumonia (CORIMUNO-ANA-1): A randomized controlled trial. Lancet Respir. Med. 2021, 9, 295–304. [Google Scholar] [CrossRef]
- WHO Working Group on the Clinical Characterization and Management of COVID-19 infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Serafim, R.B.; Póvoa, P.; Souza-Dantas, V.; Kalil, A.C.; Salluh, J.I.F. Clinical course and outcomes of critically ill patients with COVID-19 infection: A systematic review. Clin. Microbiol. Infect 2021, 27, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Fink, J.B.; Ehrmann, S. High-flow nasal cannula for COVID-19 patients: Low risk of bio-aerosol dispersion. Eur. Resp. J. 2020, 55, 2000892. [Google Scholar] [CrossRef]
- Fernandez-Cruz, A.; Ruiz-Antoran, B.; Muñoz-Gomez, A.; Sancho-Lopez, A.; Mills-Sanchez, P.; Centeno Soto, G.A.; Blanco-Alonso, S.; Javaloyes-Garachana, L.; Galán-Gómez, A.; Valencia-Alijo, Á.; et al. A retrospective controlled cohort study of the impact of glucocorticoid treatment in SARSCoV-2 infection mortality. Antimicrob. Agents Chemother. 2020, 64, e01168-76. [Google Scholar] [CrossRef]
- Shang, L.; Zhao, J.; Hu, Y.; Du, R.; Cao, B. On the use of corticosteroids for 2019-nCoV pneumonia. Lancet 2020, 395, 683–684. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient State | Descriptor |
|---|---|
| 5. Hospitalized moderate disease | (5a) Supplemental O2 by nasal cannula requiring ≤4 lpm flow |
| (5b) Supplemental O2 by nasal cannula requiring ≥5 lpm flow | |
| (5c) Supplemental O2 by mask using FiO2 between 35% and 50% | |
| 6. Hospitalized severe disease | (6a) Supplemental O2 by mask with reservoir bag |
| (6b) Supplemental O2 by high-flow nasal cannula (HFNC) | |
| (6c) Non-invasive mechanical ventilation |
| Variables | Anakinra Group (n = 125) | Baricitinib Group (n = 217) | p Univariate |
|---|---|---|---|
| Demographic data | |||
| Age (median, IQR), in years | 73 (59–78) | 71 (59–82) | 0.528 |
| Male sex, n (%) | 70 (56) | 127 (58) | 0.649 |
| Charlson index > 2, n (%) | 60 (48) | 127 (58) | 0.060 |
| Barthel scale ≥ 60, n (%) | 116 (93) | 184 (85) | 0.030 |
| Cardiopulmonary resuscitation candidate, n (%) | 97 (78) | 157 (72) | 0.285 |
| Living in a nursing home, n (%) | 3 (2) | 11 (5) | 0.230 |
| Laboratory values (median, IQR) | |||
| Ferritin, in ng/mL | 746 (324–1329) | 579 (299–1312) | 0.577 |
| D-dimers, in µg/mL | 900 (550–1640) | 1055 (595–2163) | 0.936 |
| C-reactive protein, in mg/L | 103 (58–168) | 98 (44–143) | 0.044 |
| Procalcitonin, in ng/mL | 0.14 (0.08–0.23) | 0.11 (0.07–0.20) | 0.770 |
| Erythrocyte sedimentation rate, in mm/h | 42 (14–77) | 51 (25–83) | 0.057 |
| Alanine aminotransferase, in U/L | 30 (20–53) | 26 (17–43) | 0.013 |
| Lactate dehydrogenase, in U/L | 326 (254–414) | 302 (230–387) | 0.078 |
| Platelets × 103/µL | 233 (174–305) | 236 (157–320) | 0.831 |
| Lymphocytes/µL | 880 (620–1265) | 880 (620–1280) | 0.390 |
| Interleukin-6, in pg/mL * | 16 (8–22) | 20 (5–49) | <0.001 |
| Time to event (median, IQR), in days | |||
| Time of symptoms before admission | 7 (5–10) | 7 (5–10) | 0.505 |
| Time from admission to censored date | 11 (8–15) | 10 (7–16) | 0.898 |
| Time under first ID | 10 (8–10) | 8 (5–10) | 0.239 |
| Time from ID to combination event | 7 (5–10) | 9 (6–15) | 0.005 |
| Mean time from admission to ID | 2.41 | 0.93 | <0.001 |
| Treatments, n (%) | |||
| Remdesivir | 2 (2) | 35 (16) | <0.001 |
| Lopinavir/ritonavir | 0 | 77 (35) | <0.001 |
| Dexamethasone at admission | 77 (62) | 172 (79) | <0.001 |
| Pulses of corticosteroids at any time | 125 (100) | 99 (46) | <0.001 |
| Changes in immunomodulatory therapy | 5 (4) | 31 (14) | 0.001 |
| Tocilizumab | 1 (1) | 13 (6) | 0.020 |
| Intermediate or high doses of LMWH 1 | 67 (57) | 82 (38) | <0.001 |
| Mask with reservoir bag at admission | 61 (49) | 22 (10) | <0.001 |
| Variables | Intubation | p Univariate | p Multivariate | Hazard Ratio (95% CI) |
|---|---|---|---|---|
| Lactate dehydrogenase | ||||
| ≥350 U/L | 15 (12.3) | 0.002 | 0.015 | 2.907 (1.227–6.827) |
| <350 U/L | 8 (3.6) | |||
| Mask with reservoir bag | ||||
| Yes | 13 (15.7) | <0.001 | 0.033 | 4.983 (1.141–21.770) |
| No | 10 (3.9) | |||
| Pulses of corticosteroids | ||||
| Yes | 22 (9.9) | 0.002 | 0.176 | – |
| No | 1 (0.8) | |||
| C-reactive protein | ||||
| ≥100 | 17 (10 | 0.017 | 0.241 | – |
| <100 | 6 (3.5) | |||
| Antiviral therapy | ||||
| Yes | 4 (3.6) | 0.110 | 0.228 | – |
| No | 19 (8.2) | |||
| First immunomodulatory drug | ||||
| Anakinra | 13 (10.4) | 0.039 | 0.594 | – |
| Baricitinib | 10 (4.6) | |||
| Dexamethasone at baseline | ||||
| Yes | 8 (3.2) | <0.001 | 0.002 | 0.256 (0.108–0.611) |
| No | 15 (16.1) |
| Variables | Mortality | p Univariate | p Multivariate | Hazard Ratio (95% CI) |
|---|---|---|---|---|
| Lactate dehydrogenase | ||||
| ≥350 U/L | 26 (21.3) | 0.110 | 0.199 | – |
| <350 U/L | 32 (14.5) | |||
| Mask with reservoir bag | ||||
| Yes | 25 (30.1) | <0.001 | 0.118 | – |
| No | 33 (12.7) | |||
| Pulses of corticosteroids | ||||
| Yes | 49 (22) | 0.001 | <0.001 | 1.668 (1.308–2.127) |
| No | 9 (7.6) | |||
| Age | ||||
| ≥70 | 50 (25.6) | <0.001 | <0.001 | 1.634 (1.279–2.087) |
| <70 | 8 (5.4) | |||
| Dose of LMHW | ||||
| Prophylaxis | 22 (12) | 0.008 | 0.072 | – |
| Intermediate or high dose | 36 (22.8) | |||
| Invasive ventilation | ||||
| Yes | 16 (69.6) | <0.001 | <0.001 | 12.576 (5.113–30.932) |
| No | 42 (13.2) | |||
| Barthel index | ||||
| <60 | 19 (45.2) | <0.001 | 0.037 | 1.604 (1.030–2.497) |
| ≥60 | 39 (13) | |||
| Charlson index | ||||
| <3 | 12 (7.7) | <0.001 | 0.076 | – |
| ≥3 | 46 (24.6) |
| Variables | Mortality | p Univariate | p Multivariate | Hazard Ratio (95% CI) |
|---|---|---|---|---|
| Lactate dehydrogenase | ||||
| ≥350 U/L | 18 (26.5) | 0.062 | 0.188 | – |
| <350 U/L | 18 (15.3) | |||
| Mask with reservoir bag | ||||
| Yes | 18 (35.3) | 0.001 | 0.003 | 2.949 (1.463–5.947) |
| No | 18 (13.3) | |||
| Pulses of corticosteroids | ||||
| Yes | 31 (21.8) | 0.125 | 0.289 | – |
| No | 5 (11.4) | |||
| Age | ||||
| ≥70 | 30 (27) | 0.001 | 0.040 | 1.222 (1.024–3.932) |
| <70 | 6 (8) | |||
| Dose of LMHW | ||||
| Prophylaxis | 12 (13) | 0.031 | 0.747 | – |
| Intermediate or high dose | 24 (25.5) | |||
| Invasive ventilation | ||||
| Yes | 10 (71.4) | <0.001 | 0.047 | 2.276 (1.011–6.360) |
| No | 26 (15.1) | |||
| Barthel index | ||||
| <60 | 12 (44.4) | <0.001 | 0.002 | 3.338 (1.559–7.150) |
| ≥60 | 24 (15.1) | |||
| Charlson index | ||||
| <3 | 5 (6.1) | <0.001 | 0.003 | 3.544 (1.330–9.441) |
| ≥3 | 31 (29.8) | |||
| First immunomodulatory drug | ||||
| Anakinra | 15 (16.1) | 0.265 | 0.631 | – |
| Baricitinib | 21 (22.6) | |||
| Dexamethasone at baseline | ||||
| Yes | 21 (16.7) | 0.179 | 0.396 | – |
| No | 15 (25) | |||
| C-reactive protein | ||||
| ≥100 | 22 (23.7) | 0.138 | 0.764 | – |
| <100 | 14 (15.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-García, J.A.; Pérez-Quintana, M.; Ramos-Giráldez, C.; Cebrián-González, I.; Martín-Ponce, M.L.; del Valle-Villagrán, J.; Navarro-Puerto, M.A.; Sánchez-Villegas, J.; Gómez-Herreros, R.; Manoja-Bustos, I.; et al. Anakinra versus Baricitinib: Different Strategies for Patients Hospitalized with COVID-19. J. Clin. Med. 2021, 10, 4019. https://doi.org/10.3390/jcm10174019
García-García JA, Pérez-Quintana M, Ramos-Giráldez C, Cebrián-González I, Martín-Ponce ML, del Valle-Villagrán J, Navarro-Puerto MA, Sánchez-Villegas J, Gómez-Herreros R, Manoja-Bustos I, et al. Anakinra versus Baricitinib: Different Strategies for Patients Hospitalized with COVID-19. Journal of Clinical Medicine. 2021; 10(17):4019. https://doi.org/10.3390/jcm10174019
Chicago/Turabian StyleGarcía-García, José A, Marta Pérez-Quintana, Consuelo Ramos-Giráldez, Isabel Cebrián-González, María L Martín-Ponce, José del Valle-Villagrán, María A Navarro-Puerto, Jorge Sánchez-Villegas, Rocío Gómez-Herreros, Isabel Manoja-Bustos, and et al. 2021. "Anakinra versus Baricitinib: Different Strategies for Patients Hospitalized with COVID-19" Journal of Clinical Medicine 10, no. 17: 4019. https://doi.org/10.3390/jcm10174019