The emergence of the current coronavirus disease 2019 (COVID-19) pandemic has given rise to a massive global health concern that placed an unprecedented strain on healthcare systems and the education and economy of every country. Almost a year later, the approval of different COVID-19 vaccines has given people worldwide a glimmer of hope. However, more than 50% of the COVID-19 vaccine supply has been acquired by high-income nations, forcing low- and middle-income countries to prioritize specific populations for vaccine administration.1,2 For example, despite being a middle-income country, Mexico was ranked as the tenth nation with the highest vaccine acquisition.3 Nonetheless, manufacturers’ uncertainty of vaccine supplies and delays in production have made the programming and roll-out of vaccines quite complicated.
In Mexico, a technical advisory group (GTAVCovid-19) was formed to design the vaccination strategy. This group proposed prioritizing healthcare workers (starting with all COVID-19 centres, followed by the remaining physicians), densely populated areas with higher mortality rates, and citizens > 50 years old to receive the vaccine. By vaccinating 20% of the population, this strategy predicted lowering mortality rates up to 80% and covering the most vulnerable population sectors.4 Nonetheless, the federal government decided to proceed differently, administering vaccines during the first phase only to healthcare personnel working at first line COVID-19 public institutions, excluding COVID-19 private clinics. Furthermore, the second phase, which originally included adults >60 years and the rest of the healthcare providers, was subsequently modified to reactivate face-to-face education, i.e. healthcare providers were replaced by educational workers, leaving health personnel attending non-COVID-19 areas and all private practices unvaccinated.5
The exclusion of the remaining healthcare workers raised several concerns as this population is seven times more likely to present with severe disease than the other essential workers.6 Moreover, as of June 2021, Mexico continued to report the world’s highest death rate among health personnel due to COVID-19 infection with 3.940 deaths, followed by the United States (1.646) and Peru (1.345).7 Most of these infections probably occurred in health providers attending non-COVID-19 areas, which are centres destined to treat any other condition other than COVID-19, since international studies suggest that asymptomatic individuals might be responsible for more than 50% of transmissions.8 Additionally, the lack of specialized personal protective equipment forced it to designate its distribution to institutions attending only COVID-19 patients, thereby leaving non-COVID-19 hospitals and general practitioners in the outpatient setting without adequate protection.9
The suspicion that political motives influence vaccination priorities is prevalent among the Mexican press and media, since 2021 is the Midterm Election year, and the Teachers’ Unions has historically played an important role in this matter. Moreover, the organization of vaccination programs in Mexico has historically been the domain of the Secretary of Health, with vaccines being administrated by healthcare personnel. For COVID-19, however, this dynamic substantially changed, and vaccines were ordered to be administered by “Servidores de la Nación”, composed of about 23,000 members of the political party in power. Also, several members of the Army were instructed to secure vaccination sites, raising criticism regarding the heavily militarized vaccination brigades.1
On the other hand, the struggle for quality and reach of education during the pandemic in low- and middle-income countries should not be underestimated. In Mexico, 43.5% of homes lack internet access, and as an effort to address this problem and mitigate the possible exacerbation of existing inequalities,10 classes are now broadcasted on national T.V. and radio, stretching educational reach to 92.5% of the population.11 Although reopening schools is ideal, attempting to do so by vaccinating teachers may not diminish the spread of the virus since vaccines are tested in terms of mortality or severe disease prevention and have not been proven to reduce transmission yet.12 In addition, the appearance of new strains of COVID-19 possessing a higher rate of severe outcomes supports the need for vaccination of all healthcare personnel in preparation for an imminent spike in cases. The urgency of returning to the original vaccination strategy proposed by Mexico’s GTAVCovid-19 group cannot be overemphasized.
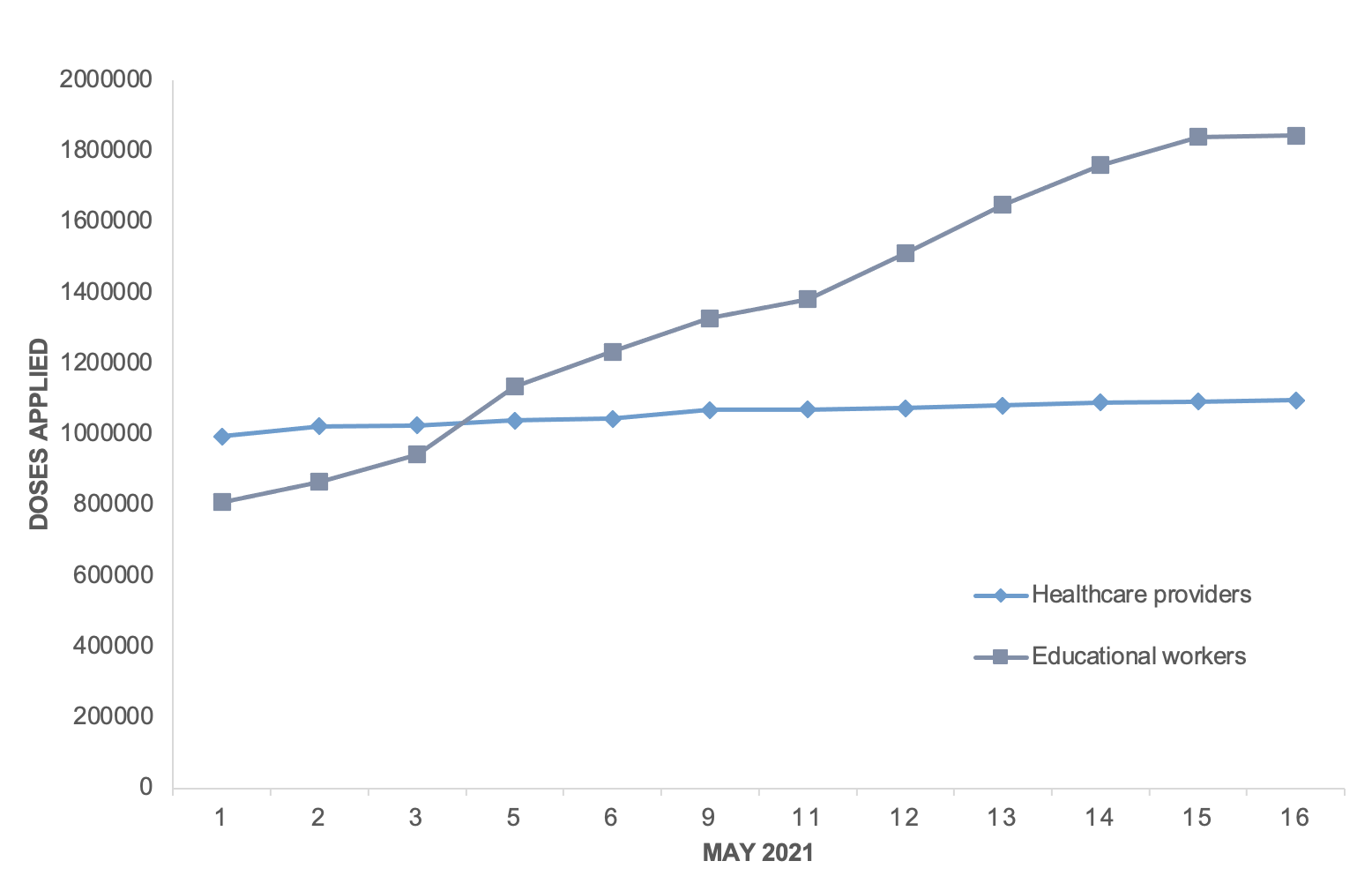
The latest information on health personnel’s vaccination was published on May 16th, a month after the teachers’ vaccination program began. The report informed that a total of 1,097,190 healthcare providers had been vaccinated compared to 1,843,832 educational workers.13 A graphic description of available data comparing these to populations is presented in Figure 1. Unfortunately, there is no information regarding the proportion of health personnel vaccinated. However, it is estimated that 87% of the educational workers received at least one dose.14 Overall, as of August 18th, 23.19% of Mexico’s population had been fully vaccinated, including healthcare providers who had to wait in line for their vaccination turn according to age group.15 Currently, Mexico remains the leading country on health personnel deaths due to COVID-19 infection and faces a third pandemic wave with cases rising to 22,000 daily, most seen in the young and in the unvaccinated.16

The possible framing of vaccination as a political tool takes it out of the realm of medical science altogether. Instead, a successful vaccination program should be built around scientific data, public health benefits and an aim for full population coverage. The remaining should prevail in nations with limited resources, where the latter cannot be immediately fulfilled.17
The federal government in Mexico has ignored its own technical advisory group’s strategic advice and international recommendations to vaccinate all healthcare personnel, regardless of their place of employment (public or private sector), thereby neglecting a considerable proportion of health workers. Therefore, it is essential to share various vaccination experiences so that other nations may be able to optimize their strategies and achieve success in overcoming this pandemic.
Acknowledgements
We would like to thank all Mexican healthcare workers who directly or indirectly contributed to the care of patients, and the support and maintenance of the health system during the pandemic.
Conflict of interests
The authors completed the ICMJE Unified Competing Interest form (available upon request from the corresponding author), and declare no conflicts of interest.
Disclaimer
Authors hold sole responsibility for the views expressed in the manuscript, which may not necessarily reflect the opinion or policy of the Journal.
Availability of data and materials
All data relevant to the study are included in the article. However, study materials and data that support the findings in this paper are available upon reasonable request by contacting the corresponding author.
Funding
No funding was obtained for this study.
Authors’ contributions
All authors have contributed to each stage of the manuscript design and preparation, and approved the final version. All authors agree to be accountable for all aspects of the work.
Correspondence
Michel F. Martinez Resendez, Tec de Monterrey, Monterrey, Mexico. Av. Batallon de San Patricio #112. Col. Real de San Agustin, N.L. CP. 66278 Mexico; tel: +52 (81) 88 88 05 51, fax: +52 (81) 88 88 05 51; drmichelfernando@gmail.com