
Cardiovascular Manifestations in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19 According to Age

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. Anoutbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Riphagen, S.; Gomez, X.; Gonzalez-Martinez, C.; Wilkinson, N.; Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 2020, 395, 1607–1608. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). May 2020. Available online: https://emergency.cdc.gov/han/2020/han00432.asp (accessed on 1 September 2021).
- World Health Organization (WHO). Multisystem Inflammatory Syndrome in Children and Adolescents Temporally Related to COVID-19. 2020. Available online: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed on 10 September 2021).
- Royal College of Paediatrics and Child Health. Guidance: Paediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19. 2020. Available online: https://www.rcpch.ac.uk/resources/guidancepaediatric-multisystem-inflammatory-syndrome-temporally-associated-covid-19-pims-guidance) (accessed on 15 September 2021).
- Belhadjer, Z.; Méot, M.; Bajolle, F.; Khraiche, D.; Legendre, A.; Abakka, S.; Auriau, J.; Grimaud, M.; Oualha, M.; Beghetti, M.; et al. Acute Heart Failure in Multisystem Inflammatory Syndrome in Children in the Context of Global SARS-CoV-2 Pandemic. Circulation 2020, 142, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Valverde, I.; Singh, Y.; Sanchez-De-Toledo, J.; Theocharis, P.; Chikermane, A.; Di Filippo, S.; Kuciñska, B.; Mannarino, S.; Tamariz-Martel, A.; Gutierrez-Larraya, F.; et al. Acute Cardiovascular Manifestations in 286 Children with Multisystem Inflammatory Syndrome Associated with COVID-19 Infection in Europe. Circulation 2021, 143, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef]
- Hoste, L.; Van Paemel, R.; Haerynck, F. Multisystem inflammatory syndrome in children related to COVID-19: A systematic review. Eur. J. Pediatr. 2021, 180, 2019–2034. [Google Scholar] [CrossRef]
- Carter, M.J.; Fish, M.; Jennings, A.; Doores, K.J.; Wellman, P.; Seow, J.; Acors, S.; Graham, C.; Timms, E.; Kenny, J.; et al. Peripheral immunophenotypes in children with multisystem inflammatory syndrome associated with SARS-CoV-2 infection. Nat. Med. 2020, 26, 1701–1707. [Google Scholar] [CrossRef]
- Pouletty, M.; Borocco, C.; Ouldali, N.; Caseris, M.; Basmaci, R.; Lachaume, N.; Bensaid, P.; Pichard, S.; Kouider, H.; Morelle, G.; et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): A multicentre cohort. Ann. Rheum. Dis. 2020, 79, 999–1006. [Google Scholar] [CrossRef]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef]
- Godfred-Cato, S.; Bryant, B.; Leung, J.; Oster, M.E.; Conklin, L.; Abrams, J.; Roguski, K.; Wallace, B.; Prezzato, E.; Koumans, E.H.; et al. COVID-19–Associated Multisystem Inflammatory Syndrome in Children—United States, March–July 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Swann, O.V.; Holden, K.A.; Turtle, L.; Pollock, L.; Fairfield, C.J.; Drake, T.M.; Seth, S.; Egan, C.; Hardwick, H.E.; Halpin, S.; et al. Clinical characteristics of children and young people admitted to hospital with covid-19 in United Kingdom: Prospectivemulticentre observational cohort study. BMJ 2020, 370, m3249. [Google Scholar] [CrossRef] [PubMed]
- Alsaied, T.; Tremoulet, A.H.; Burns, J.C.; Saidi, A.; Dionne, A.; Lang, S.M.; Newburger, J.W.; De Ferranti, S.; Friedman, K.G. Review of Cardiac Involvement in Multisystem Inflammatory Syndrome in Children. Circulation 2020, 143, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Kavurt, A.V.; Bağrul, D.; Gül, A.E.K.; Özdemiroğlu, N.; Ece, İ.; Çetin, İ.İ.; Özcan, S.; Uyar, E.; Emeksiz, S.; Çelikel, E.; et al. Korean Society of Kawasaki Disease. Clinical features, diagnosis, and outcomes of multisystem inflammatory syndrome in children associated with coronavirus disease 2019. Clin. Exp. Pediatr. 2021, 64, 68–75. [Google Scholar] [CrossRef]
- Sirico, D.; Basso, A.; Reffo, E.; Cavaliere, A.; Castaldi, B.; Sabatino, J.; Meneghel, A.; Martini, G.; Da Dalt, L.; Zulian, F.; et al. Early Echocardiographic and Cardiac MRI Findings in Multisystem Inflammatory Syndrome in Children. J. Clin. Med. 2021, 10, 3360. [Google Scholar] [CrossRef]
- Caro-Patón, G.D.L.; de Azagra-Garde, A.M.; García-Salido, A.; Cabrero-Hernández, M.; Tamariz, A.; Nieto-Moro, M. Shock and Myocardial Injury in Children with Multisystem Inflammatory Syndrome Associated with SARS-CoV-2 Infection: What We Know. Case Series and Review of the Literature. J. Intensiv. Care Med. 2021, 36, 392–403. [Google Scholar] [CrossRef]
- Brisca, G.; Consolaro, A.; Caorsi, R.; Pirlo, D.; Tuo, G.; Campanello, C.; Castagnola, E.; Moscatelli, A.; Gattorno, M.; Ravelli, A. Timely Recognition and Early Multi-Step Antinflammatory Therapy May Prevent ICU Admission of Patients with MIS-C: Proposal for a Severity Score. Front. Pediatr. 2021, 9, 783745. [Google Scholar] [CrossRef]
- Dionne, A.; Mah, D.Y.; Son, M.B.F.; Lee, P.Y.; Henderson, L.; Baker, A.L.; de Ferranti, S.D.; Fulton, D.R.; Newburger, J.W.; Friedman, K.G. Atrioventricular Block in Children with Multisystem Inflammatory Syndrome. Pediatrics 2020, 146, 5. [Google Scholar] [CrossRef]
- Niaz, T.; Hope, K.; Fremed, M.; Misra, N.; Altman, C.; Glickstein, J.; Sanchez-De-Toledo, J.; Fraisse, A.; Miller, J.; Snyder, C.; et al. Role of a Pediatric Cardiologist in the COVID-19 Pandemic. Pediatr. Cardiol. 2021, 42, 19–35. [Google Scholar] [CrossRef]
- Hung, Y.; Lin, W.-H.; Lin, C.-S.; Cheng, S.-M.; Tsai, T.-N.; Yang, S.-P.; Lin, W.-Y. The Prognostic Role of QTc Interval in Acute Myocarditis. Acta Cardiol. Sin. 2016, 32, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, P.E.; Capecchi, P.L.; Laghi-Pasini, F. Long QT Syndrome: An Emerging Role for Inflammation and Immunity. Front. Cardiovasc. Med. 2015, 2, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ucar, F.M.; Ozturk, C.; Yılmaztepe, M.A. Evaluation of Tp-e interval, Tp-e/QT ratio and Tp-e/QTc ratio in patients with acute myocarditis. BMC Cardiovasc. Disord. 2019, 19, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Buttà, C.; Zappia, L.; Laterra, G.; Roberto, M. Diagnostic and prognostic role of electrocardiogram in acute myocarditis: A comprehensive review. Ann. Noninvasive Electrocardiol. 2019, 25, 12726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasuhara, J.; Watanabe, K.; Takagi, H.; Sumitomo, N.; Kuno, T. COVID-19 and multisystem inflammatory syndrome in children: A systematic review and meta-analysis. Pediatr. Pulmonol. 2021, 56, 837–848. [Google Scholar] [CrossRef]
- Theocharis, P.; Wong, J.; Pushparajah, K.; Mathur, S.K.; Simpson, J.M.; Pascall, E.; Cleary, A.; Stewart, K.; Adhvaryu, K.; Savis, A.; et al. Multimodality cardiac evaluation in children and young adults with multisystem inflammation associated with COVID-19. Eur. Heart J.-Cardiovasc. Imaging 2021, 22, 896–903. [Google Scholar] [CrossRef]
- Rakha, S.; Sobh, A.; Hager, A.H.; Hafez, M.; Alsawah, G.A.; Abuelkheir, M.M.; Zeid, M.S.; Nahas, M.; Elmarsafawy, H. Cardiac implications of multisystem inflammatory syndrome associated with COVID-19 in children under the age of 5 years. Cardiol. Young 2021, 1–6. [Google Scholar] [CrossRef]
- Fabi, M.; Corinaldesi, E.; Pierantoni, L.; Mazzoni, E.; Landini, C.; Bigucci, B.; Ancora, G.; Malaigia, L.; Bodnar, T.; Di Fazzio, G.; et al. Gastrointestinal presentation of Kawasaki disease: A red flag for severe disease? PLoS ONE 2018, 13, e0202658. [Google Scholar] [CrossRef]
- Colomba, C.; La Placa, S.; Saporito, L.; Corsello, G.; Ciccia, F.; Medaglia, A.; Romanin, B.; Serra, N.; Di Carlo, P.; Cascio, A. Intestinal Involvement in Kawasaki Disease. J. Pediatr. 2018, 202, 186–193. [Google Scholar] [CrossRef] [Green Version]
- Muniz, J.-C.G.; Dummer, K.; Gauvreau, K.; Colan, S.D.; Fulton, D.R.; Newburger, J.W. Coronary Artery Dimensions in Febrile Children without Kawasaki Disease. Circ. Cardiovasc. Imaging 2013, 6, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Bratincsak, A.; Reddy, V.D.; Purohit, P.; Tremoulet, A.H.; Pour Molkara, D.; Frazer, J.R.; Dyar, D.; Bush, R.A.; Sim, J.Y.; Sang, N.; et al. Coronary Artery Dilation in Acute Kawasaki Disease and Acute Illnesses Associated with Fever. Pediatr. Infect. Dis. J. 2012, 31, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Cantarutti, N.; Battista, V.; Adorisio, R.; Cicenia, M.; Campanello, C.; Listo, E.; Campana, A.; Trocchio, G.; Drago, F. Cardiac Manifestations in Children with SARS-COV-2 Infection: 1-Year Pediatric Multicenter Experience. Children 2021, 8, 717. [Google Scholar] [CrossRef] [PubMed]
- Sancho-Shimizu, V.; Brodin, P.; Cobat, A.; Biggs, C.M.; Toubiana, J.; Lucas, C.L.; Henrickson, S.E.; Belot, A.; Haddad, E.; Beland, K.; et al. SARS-CoV-2–related MIS-C: A key to the viral and genetic causes of Kawasaki disease? J. Exp. Med. 2021, 218, e20210446. [Google Scholar] [CrossRef]
- Rowley, A.H.; Shulman, S.T. The Epidemiology and Pathogenesis of Kawasaki Disease. Front. Pediatr. 2018, 6, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esper, F.; Shapiro, E.D.; Weibel, C.; Ferguson, D.; Landry, M.L.; Kahn, J.S. Association between a Novel Human Coronavirus and Kawasaki Disease. J. Infect. Dis. 2005, 191, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Cell 2020, 183, 968–981.e7. [Google Scholar] [CrossRef] [PubMed]
- Brodin, P. Why is COVID-19 so mild in children? Acta Paediatr. 2020, 109, 1082–1083. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, A. Ravelli, A. Sindrome Infiammatoria Multisistemica e Sindrome di Kawasaki: Condizioni Diverse o Unico Spettro di Patologia? Il Pediatra. February 2021, Volume 1, pp. 20. Available online: https://reader.paperlit.com/read/prj_5c6d8de746b5d/pub_5c6d8de7a4cc5/5000-01-20 (accessed on 18 April 2022).
- Lee, P.-I.; Hu, Y.-L.; Chen, P.-Y.; Huang, Y.-C.; Hsueh, P.-R. Are children less susceptible to COVID-19? J. Microbiol. Immunol. Infect. 2020, 53, 371–372. [Google Scholar] [CrossRef]
- Malcangi, G.; Inchingolo, A.D.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; Mancini, A.; et al. COVID-19 Infection in Children and Infants: Current Status on Therapies and Vaccines. Children 2022, 9, 249. [Google Scholar] [CrossRef]
- Lu, X.; Xiang, Y.; Du, H.; Wong, G.W. SARS-CoV-2 infection in children—Understanding the immune responses and controlling the pandemic. Pediatr. Allergy Immunol. 2020, 31, 449–453. [Google Scholar] [CrossRef]
- Webster, G.; Patel, A.B.; Carr, M.R.; Rigsby, C.K.; Rychlik, K.; Rowley, A.H.; Robinson, J.D. Cardiovascular magnetic resonance imaging in children after recovery from symptomatic COVID-19 or MIS-C: A prospective study. J. Cardiovasc. Magn. Reson. 2021, 23, 86. [Google Scholar] [CrossRef] [PubMed]
- Son, M.B.F.; Murray, N.; Friedman, K.; Young, C.C.; Newhams, M.M.; Feldstein, L.R.; Loftis, L.L.; Tarquinio, K.M.; Singh, A.R.; Heidemann, S.M.; et al. Multisystem Inflammatory Syndrome in Children—Initial Therapy and Outcomes. N. Engl. J. Med. 2021, 385, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Belot, A.; Antona, D.; Renolleau, S.; Javouhey, E.; Hentgen, V.; Angoulvant, F.; Delacourt, C.; Iriart, X.; Ovaert, C.; Bader-Meunier, B.; et al. SARS-CoV-2-related paediatric inflammatory multisystem syndrome, an epidemiological study, France, 1 March to 17 May 2020. Eurosurveillance 2020, 25, 2001010. [Google Scholar] [CrossRef] [PubMed]
- McArdle, A.J.; Vito, O.; Patel, H.; Seaby, E.G.; Shah, P.; Wilson, C.; Broderick, C.; Nijman, R.; Tremoulet, A.H.; Munblit, D.; et al. Treatment of Multisystem Inflammatory Syndrome in Children. N. Engl. J. Med. 2021, 385, 11–22. [Google Scholar] [CrossRef]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. Clinical Characteristics of 58 Children with a Pediatric Inflammatory Multisystem Syndrome Temporally Associated with SARS-CoV-2. Jama 2020, 324, 259–269. [Google Scholar] [CrossRef]
- Matsubara, D.; Kauffman, H.L.; Wang, Y.; Calderon-Anyosa, R.; Nadaraj, S.; Elias, M.D.; White, T.J.; Torowicz, D.L.; Yubbu, P.; Giglia, T.M.; et al. Echocardiographic Findings in Pediatric Multisystem Inflammatory Syndrome Associated with COVID-19 in the United States. J. Am. Coll. Cardiol. 2020, 76, 1947–1961. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| MIS-C Cohort | Total Patients 25 (100%) | Group 1 <6 Years 13 (52%) | Group 2 ≥6 Years 12 (48%) |
|---|---|---|---|
| Female | 11 (44) | 6 (46.2) | 5 (41.7) |
| Male | 14 (56) | 7 (53.8) | 7 (58.3) |
| Ethnicity | |||
| Caucasian | 16 (64) | 7 (53.8) | 9 (75) |
| Hispanic | 5 (20) | 4 (30.8) | 1 (8.3) |
| African | 2 (8) | 2 (15.4) | 0 (0) |
| Asian | 2 (8) | 0 (0) | 2 (16.7) |
| COVID-19 tests | |||
| Positive SARS-CoV-2 nasopharyngeal swab | 3 (12) | 2 (15.4) | 1 (8.3) |
| Positive SARS-CoV-2 IgG title | 20 (80) | 9 (69.2) | 11 (91.7) |
| Contact with patients with COVID-19 | 2 (8) | 2 (15.4) | 0 (0) |
| Clinical manifestations | |||
| Cardiological | 25 (100) | 13 (100) | 12 (100) |
| Respiratory | 9 (36) | 2 (15.4) | 7 (58.3) |
| Gastrointestinal | 22 (88) | 12 (92.3) | 10 (83.3) |
| Muco-cutaneous | 22 (88) | 12 (92.3) | 10 (83.3) |
| Adenopathy | 14 (56) | 7 (53.8) | 7 (58.3) |
| Therapy | |||
| IVIG | 25 (100) | 13 (100) | 12 (100) |
| Steroid | 24 (96) | 12 (92.3) | 12 (100) |
| Anakinra | 8 (32) | 1 (7.7) | 7 (58.3) |
| Aspirin | 23 (92) | 13 (100) | 10 (83.3) |
| Low molecular weight heparin | 17 (68) | 6 (46.1) | 11 (91.7) |
| Beta-blockers | 6 (24) | 2 (15.4) | 4 (33.3) |
| Diuretics/anti-congestive heart failure drugs | 16 (64) | 7 (53.8) | 9 (75) |
| Inotropic drugs | 0 (0) | 0 (0) | 0 (0) |
| Antibiotics | 14 (56) | 5 (38.5) | 9 (75) |
| Laboratory Findings | Group 1 (<6 Years) Median [IQR] | Group 2 (≥6 Years) Median [IQR] | p Value |
|---|---|---|---|
| ESR (1–10 mm/h) | 47 [29, 66] | 66 [55, 78] | |
| CRP (<0.46 mg/dL) | 12.6 [8.0, 19.3] | 20.3 [12.3, 25.2] | |
| PCT (<0.5 ng/mL) | 5.4 [4.2, 7.8] | 4.2 [2.5, 13.3] | |
| WBC (4–9.8 cell/mm3) | 19.4 [17.3, 21.5] | 15.6 [12.9, 19.8] | |
| Neutrofils (2–6.4 cell/mm3) | 11.9 [9.8, 16.7] | 14.1 [11.9, 16.1] | |
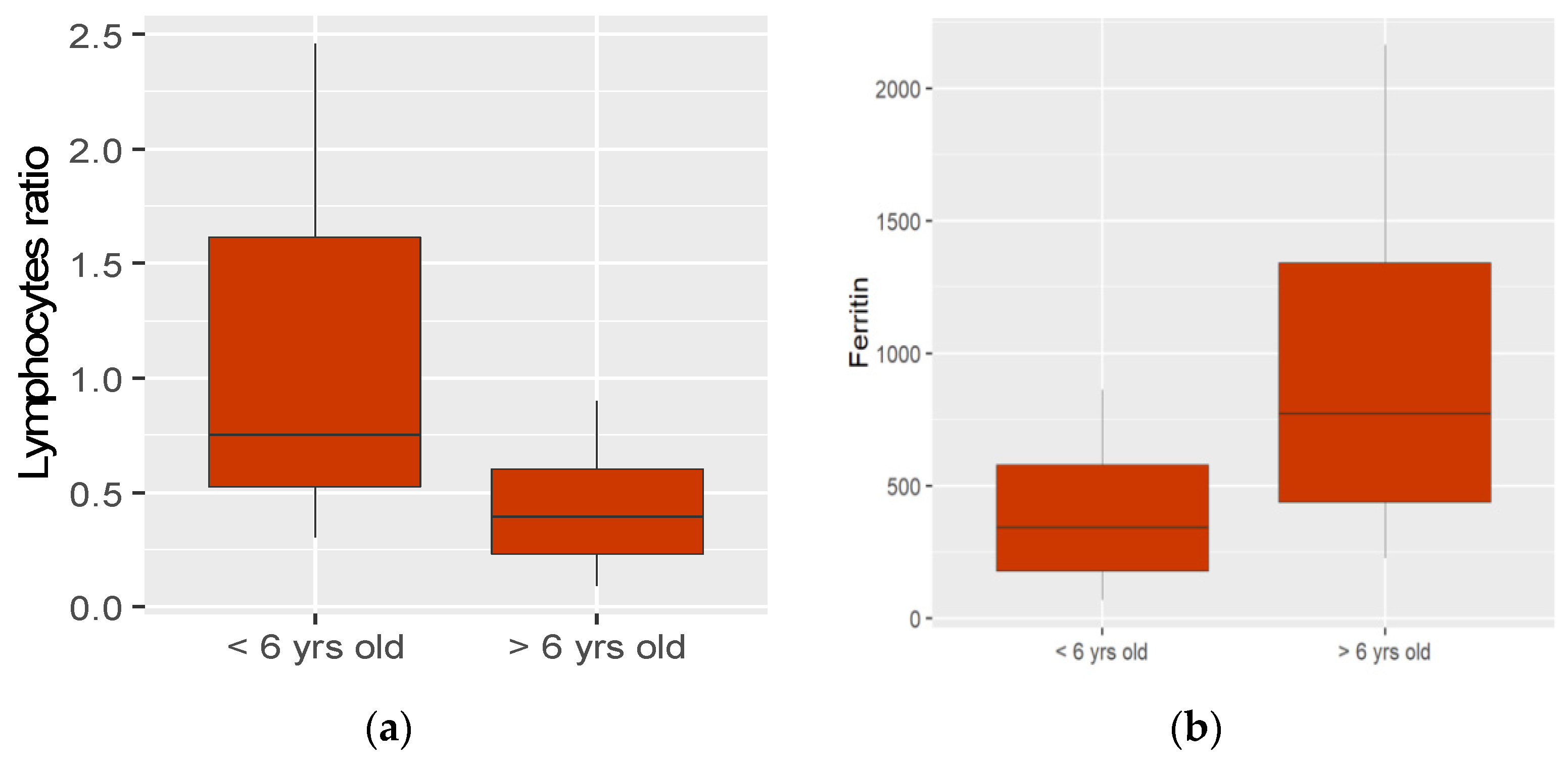
| Lymphocytes (2.0–5.8 cell/mm3) | 1.6 [1.0, 2.8] r 0.5 | 0.6 [0.3, 0.9] r 0.275 | <0.002 <0.014 |
| Hb (11.5–16.5 g/dL) | 12.2 [11.1, 12.6] | 13.1 [12.5, 14] | <0.024 |
| Platelets (150–450 cell/mm3) | 167.000 [103.000, 361.000] | 136.500 [109.750, 182.000] | |
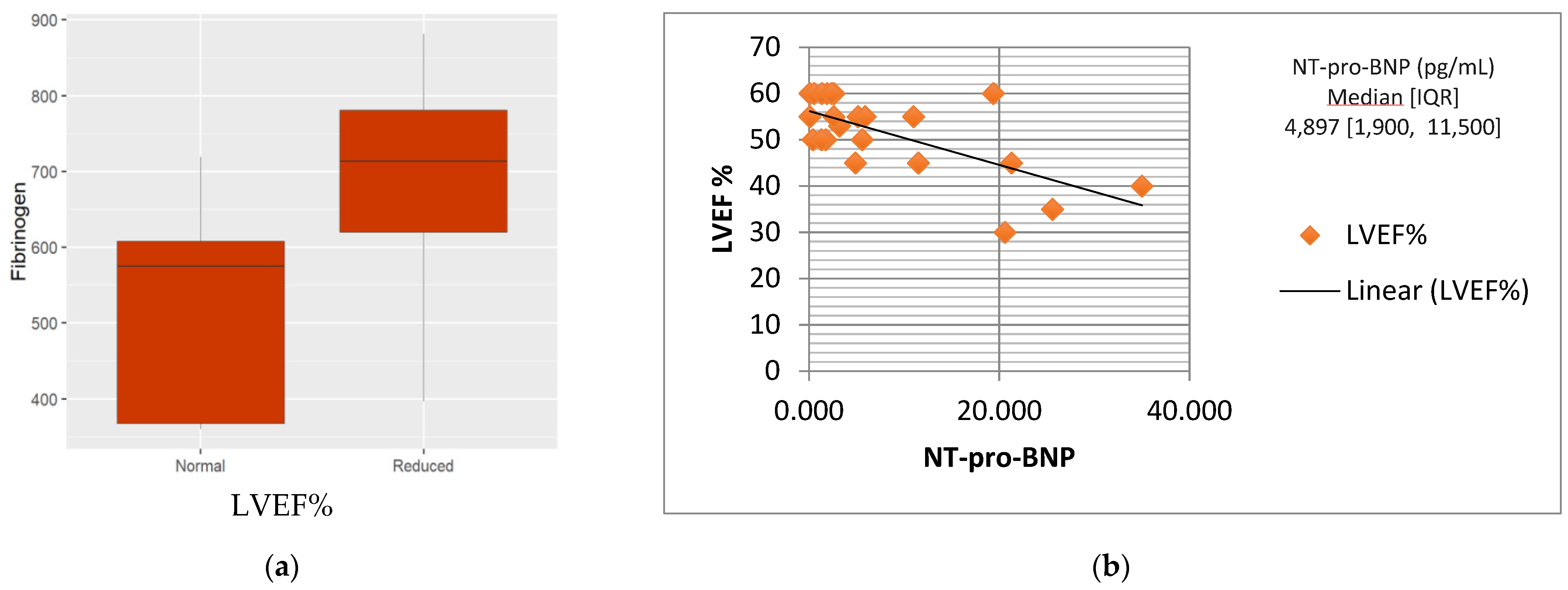
| Fibrinogen (180–350 mg/dL) | 564.0 [373.0, 662.0] | 655.0 [533.8, 840.8] | |
| D Dimer (<0.55 mcg/dL) | 3.0 [1.6, 4.1] | 3.8 [2.3, 6.7] | |
| Albumin (3.800–5.400 mg/dL) | 3000 [2.500, 3.300] | 3100 [2.600, 3.400] | |
| Ferritin (20–200 ng/mL) | 343.0 [177, 578] | 769.5 [437.5, 1340] | <0.012 |
| Troponin I (<0.16 ng/mL) | 0.1 [0.1, 0.1] | 0.2 [0.1, 0.4] | <0.042 |
| CK MB (<4.9 UI/L) | 2.4 [1.6, 3.6] | 3.0 [1.0, 4.2] | |
| NT-pro-BNP (<150 pg/mL) | 3899.5 [2135.2, 9289.5] | 6329.5 [2444.2, 14,848] |
| Cardiovascular Manifestations | No.(%) | |
| Electrocardiogram abnormalities | 15 (60) | |
| Abnormal ST-T wave segment | 14 (56) | |
| Prolonged QTc interval | 10 (40) | |
| Bradicardia | 3 (12) | |
| Atrioventricular Block | 2 (8) | |
| Non-sustained supraventricular/ventricular tachyarrhythmias | 3 (12) | |
| Echocardiogram anomalies | 25 (100) | |
| Coronary involvement | 13 (52) | |
| Dilatation (z-score + 2 − 2.5) | 7 (28) | |
| Small aneurysm (z-score + 2.5 − 5) | 4 (16) | |
| Medium aneurysm (z-score + 5 − 10) | 1 (4) | |
| LVEF% median [IQR] | 55 [50, 60] | |
| LVEF > 53% | 15 (60) | |
| LVEF < 53% | 10 (40) | |
| EF 41–52% | 7 (28) | |
| EF 30–40% | 3 (12) | |
| EF < 30% | 0 (0) | |
| Pericardial effusion | 20 (80) | |
| Mitral regurgitation | 10 (40) | |
| Cardiovascular Manifestations | Group 1 (No.%) | Group 2 (No.%) | p Value |
|---|---|---|---|
| Hypotension | 1 (7.7) | 7 (58.3) | <0.022 |
| Electrocardiogram abnormalities | 4 (30.7) | 11 (91.6) | <0.006 |
| Abnormal ST-T wave segment | 4 (30.7) | 10 (98.3) | <0.008 |
| Prolonged QTc interval | 2 (15.4) | 8 (66.6) | <0.018 |
| Bradicardia | 1 (7.6) | 2 (16.6) | |
| Atrioventricular Block | 1 (7.6) | 1 (8.3) | |
| Non-sustained supraventricular/ventricular tachyarrhythmias | 0 (0) | 3 (25) | <0.05 |
| Echocardiogram anomalies | 13 (100) | 12 (100) | |
| Coronaric involvement | 10 (77) | 2 (16.6) | <0.024 |
| Dilatation (z-score + 2 − 2.5) Small aneurysm (z-score + 2.5 − 5) Medium aneurysm (z-score + 5 − 10) | 4 (30.7) | 2 (100) | |
| 4 (30.7) | 0 (0) | ||
| 1 (7.6) | 0 (0) | ||
| LVEF% median [IQR] | 55 [50, 60] | 51 [45, 60] | |
| LVEF >53% | 11 (84.6) | 4 (33.3) | |
| LVEF <53% | 2 (15.4) | 8 (66.7) | |
| EF 52–41% EF 40–30% EF <30% | 2 (15.4) | 5 (41.7) | |
| 0 (0) | 3 (25) | ||
| 0 (0) | 0 (0) | ||
| Pericardial effusion | 8 (61.5) | 12 (100) | |
| Mitral regurgitation | 3 (23.1) | 7 (58.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campanello, C.; Mercuri, C.; Derchi, M.; Trocchio, G.; Consolaro, A.; Caorsi, R.; Ravelli, A.; Rimini, A.; Marasini, M.; Gattorno, M. Cardiovascular Manifestations in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19 According to Age. Children 2022, 9, 583. https://doi.org/10.3390/children9050583
Campanello C, Mercuri C, Derchi M, Trocchio G, Consolaro A, Caorsi R, Ravelli A, Rimini A, Marasini M, Gattorno M. Cardiovascular Manifestations in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19 According to Age. Children. 2022; 9(5):583. https://doi.org/10.3390/children9050583
Chicago/Turabian StyleCampanello, Claudia, Claudia Mercuri, Maria Derchi, Gianluca Trocchio, Alessandro Consolaro, Roberta Caorsi, Angelo Ravelli, Alessandro Rimini, Maurizio Marasini, and Marco Gattorno. 2022. "Cardiovascular Manifestations in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19 According to Age" Children 9, no. 5: 583. https://doi.org/10.3390/children9050583