To the Editor—Patients with cardiovascular and chronic obstructive pulmonary disease are at increased risk of severe coronavirus disease 2019 (COVID-19).1 The hospital environment is particularly prone to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) diffusion; therefore, it is imperative to protect patients and healthcare personnel against COVID-19 outbreaks. COVID-19 vaccination of these populations is the pillar of an effective hospital COVID-19 infection and prevention control (IPC) strategy. To increase its acceptancy and ensure its success, monitoring activities should also be conducted a local level to provide feedback to the targeted populations.
Fondazione Toscana Gabriele Monasterio (FTGM) is a public, tertiary-level, cardiological, pneumological, and heart surgery center with 2 sites, in Pisa and Massa (Italy). It has a cardiac catheterization laboratory hub for acute coronary syndrome and an adult and pediatric cardiac surgery center, and it serves as a referral center for heart failure and primitive pulmonary hypertension patients. FTGM has 123 beds and >5,000 hospital admissions per year. At the beginning of January 2021, according to national and regional regulations, our center started a COVID-19 vaccination campaign for healthcare personnel. The first phase included health workers, administrative staff, and support personnel. The second phase started in March 2021 with an additional vaccination campaign for all outpatients registered on the Tuscany regional COVID-19 vaccination web platform. In the first phase, only Pfizer-BioNTech COVID-19 was used. In the second phase, Pfizer-BioNTech and Moderna vaccines were administered according to Italian clinical recommendations in force.
Our retrospective analysis covers the period between January and May 2021. We evaluated the reported adverse effects (AEs) and the humoral response of the first phase of the vaccination campaign against COVID-19. During the first 10 weeks of the study period, 589 of 811 employees (85%) completed the vaccination cycle, receiving 2 vaccine doses of Pfizer-BioNTech COVID-19 vaccine on day 1 and day 21; of these, 82% were healthcare workers.
At the beginning of March, we invited all people working in FTGM to fill in a questionnaire that included demographic data, medical history, COVID-19–related anamnesis, and local and systemic AE reporting.
Furthermore, 1 month after the second vaccine dose, a serological test to anti–SARS-Cov-2 IgG (Abbott, index value <1.4) and anti–SARS-Cov-2 receptor binding domain (RBD) spike protein antibodies (Abbott, normal range <50 AU/mL) was offered to healthcare workers and administrative staff. We collected data for 272 workers (response rate, 46%).
Clinical characteristics of our population are summarized in Table 1; 14 employees who filled out the questionnaire claimed mild COVID disease before vaccination.
Table 1. Clinical Characteristics of Study Participants

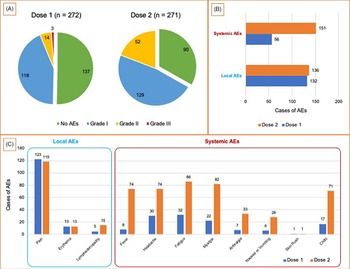
Adverse events were recorded in 50% and 67% of study participants, respectively, after the first and second vaccine doses. Systemic events are more frequent after the second vaccine dose. The postvaccination adverse events (AEs) are summarized in Fig. 1.

Fig. 1. Postvaccination adverse events (AEs). (Panel A) Number of adverse events according to MedDRA classification2 for the first and second doses of vaccine. (Panel B) Total systemic AEs and local AEs for the first and second doses of vaccine. (Panel C) Details of systemic AEs and local AEs for the first and second doses of vaccine.
Furthermore, participants who reported AEs required antipyretic medication in 20% of cases after the first dose and 58% after the second dose. In most cases, adverse effects lasted <3 days (grade I according to MedDRA classification2). After the first dose, we recorded 3 severe AEs that required hospital monitoring due to systemic symptoms. One of these AEs occurred in a study participant with previous COVID-19 disease who required steroid and antihistamine therapy. The second vaccine dose was administered to 271 of 272 patients; 1 participant preferred not to receive the second dose due to previous COVID-19 disease.
Among 272 study participants, 1 had COVID-19 disease within 3 months of follow-up. We found low anti–SARS-Cov-2 IgG values (index value <1.4) at the serological test in 5 of 14 patients with previous COVID-19 infection. All 5 of these study participants had had COVID-19 disease in the previous 6 months.
A preliminary analysis of the data shows a positive correlation between reporting AEs following the second administration and anti–SARS-Cov-2 RBD spike protein antibodies response. The antibody value in patients with AEs at the second dose was 15,664 ± 10,640 AU/mL versus 9,136 ± 7,523 AU/mL in patients who did not report adverse effects (P < .05).
In 4 patients, the anti–SARS-Cov-2 receptor binding domain (RBD) spike protein antibody level was <600 AU/mL, which indicates very poor humoral immune response to vaccine. Of these, 2 patients were on active chemotherapy, 1 had previous hematological malignancy, and 1 did not report any major issues. These patients were referred to the preventive medicine service for dedicated follow-up. According to some studies, cancer patients could need additional doses of vaccine and/or should maintain nonpharmacological preventive measures as suggested for patients who use B-lymphocyte–depleting agents.3
In the first phase of the campaign, 85% of the staff chose to receive the vaccine. Currently, adherence to the vaccination program is progressively improving to 92%. This result is better than that in a similar Canadian experience in which 80.9% of the staff accepted the vaccine.4 This result is even more significant when we consider that in November 2020, a survey administered to FTGM employees to explore vaccination hesitancy in healthcare and nonhealthcare workers found that just 232 (59%) of 396 participants had an intention to be vaccinated against COVID-19. We believe that scheduling of vaccinations outside working hours during the weekend, one-to-one vaccine counseling to hesitant workers, peer pressure from colleagues directly involved in the vaccination campaign, and the introduction of a national vaccination mandate for healthcare workers at the end of May played a significant role in achieving the current vaccination rate.
These AE data are not in line with manufacturer-sponsored studies,5 but they reflect another single-center experience.6 The main limitations of this study are that it is a single-center experience with a short follow-up. We have planned a serological follow-up at 6 and 12 months after the vaccination. Through a dedicated questionnaire, all participants are invited to record any cases of COVID-19 disease to monitor the vaccine’s long-term protection. Furthermore, these data will be included in a surveillance network involving all hospitals in Tuscany, which is being used to monitor the evolution of SARS-CoV-2 immune response in healthcare workers.
In our opinion, independent studies of real-life acceptancy, safety, and effectiveness of SARS-CoV-2 on high-risk cohorts, such as hospital personnel, are required to boost confidence in vaccine campaigns, both in the general population and in healthcare providers.
Acknowledgments
We thank all the Fondazione Toscana Gabriele Monasterio staff who contributed to the success of the vaccination campaign. In particular, we thank the Hospital Pharmacy Unit, the Laboratory Medicine Unit, the Technical and Rehabilitation Nursing Service (SITRA).
Financial support
No financial support was provided relevant to this article.
Conflicts of interest
All authors report no conflicts of interest relevant to this article.