
Physical Activity as a Predictor of the Level of Stress and Quality of Sleep during COVID-19 Lockdown

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
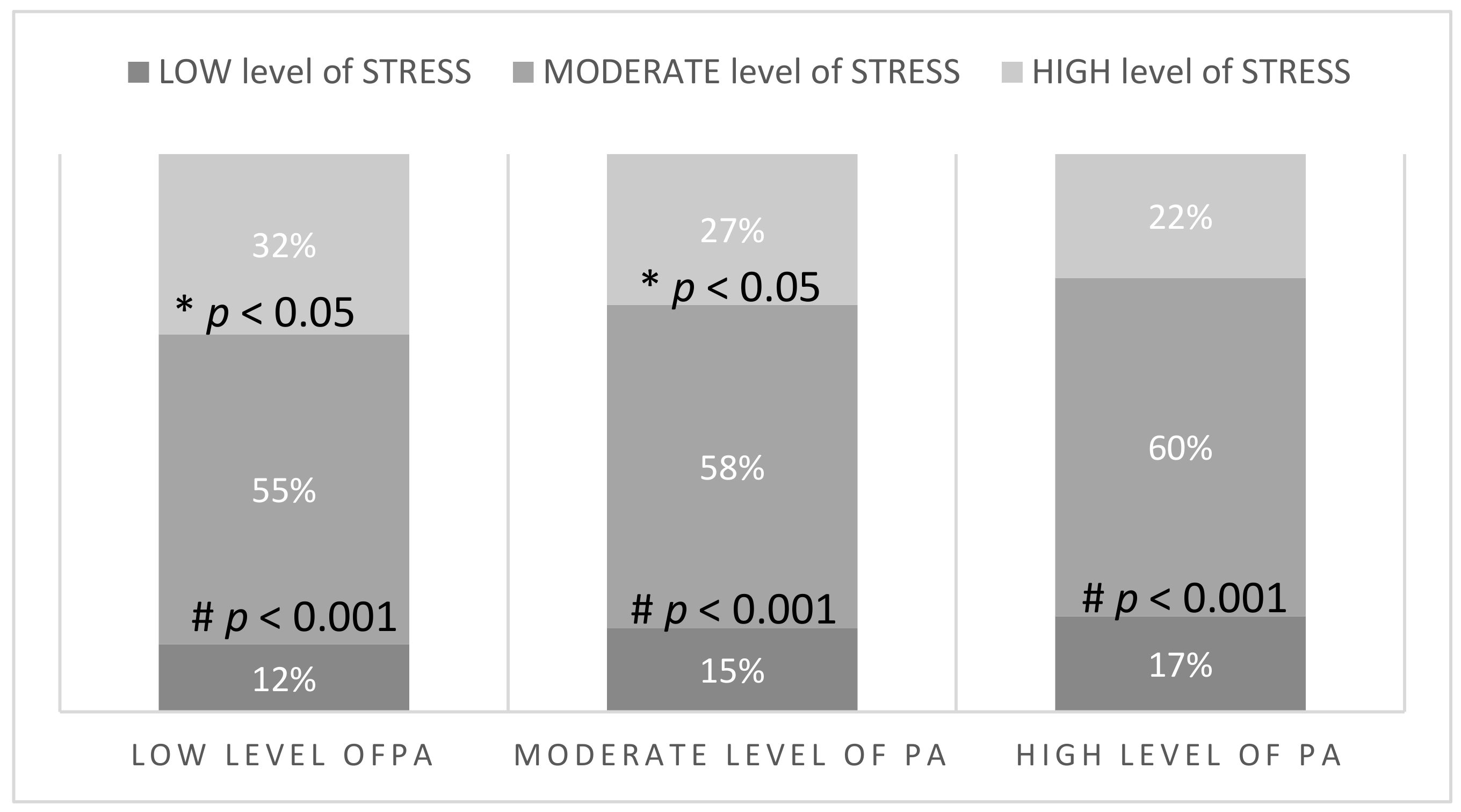
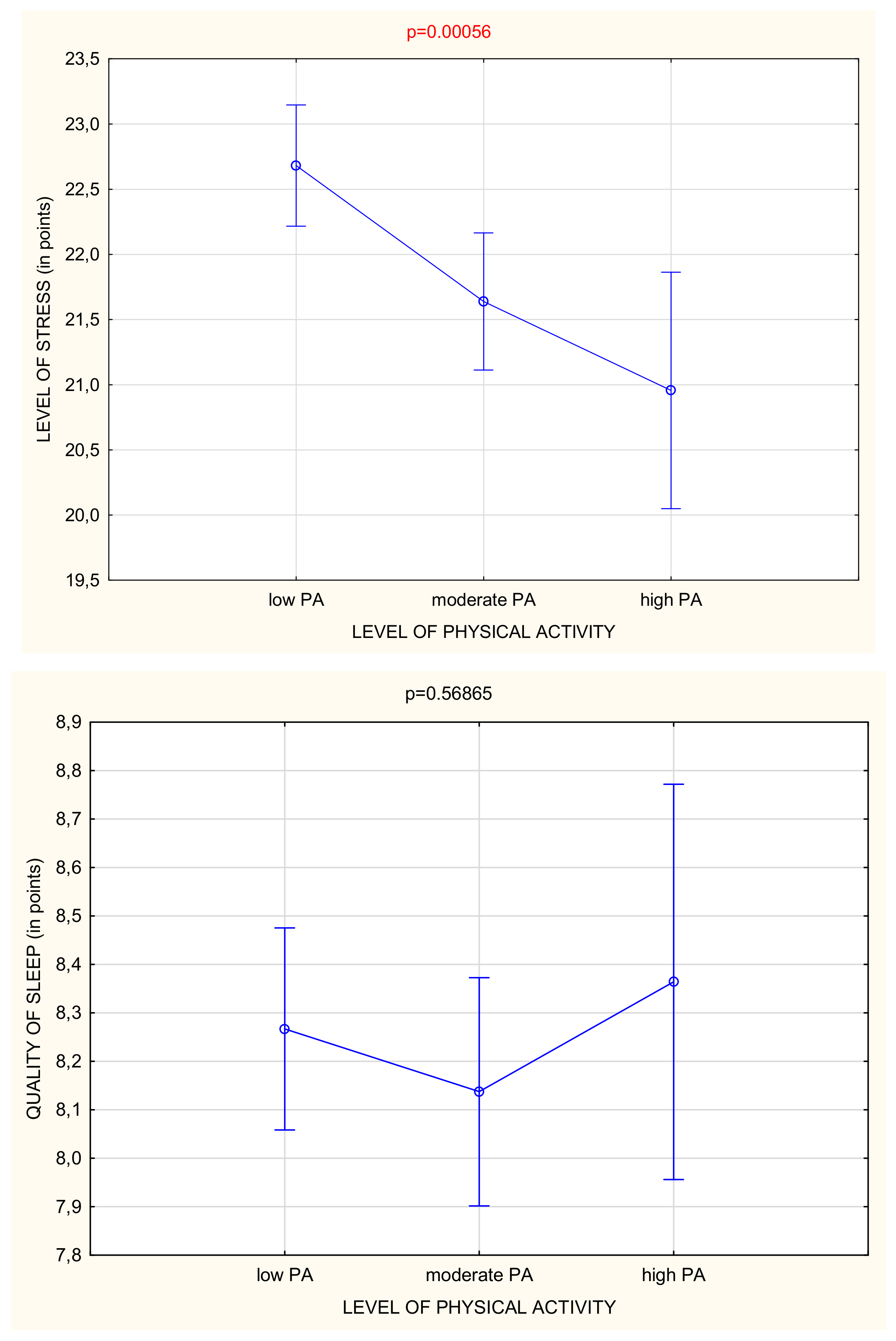
3.2. Level of Stress in Relation to Physical Activity during Lockdown
3.3. Quality of Sleep in Relation to Physical Activity during Lockdown
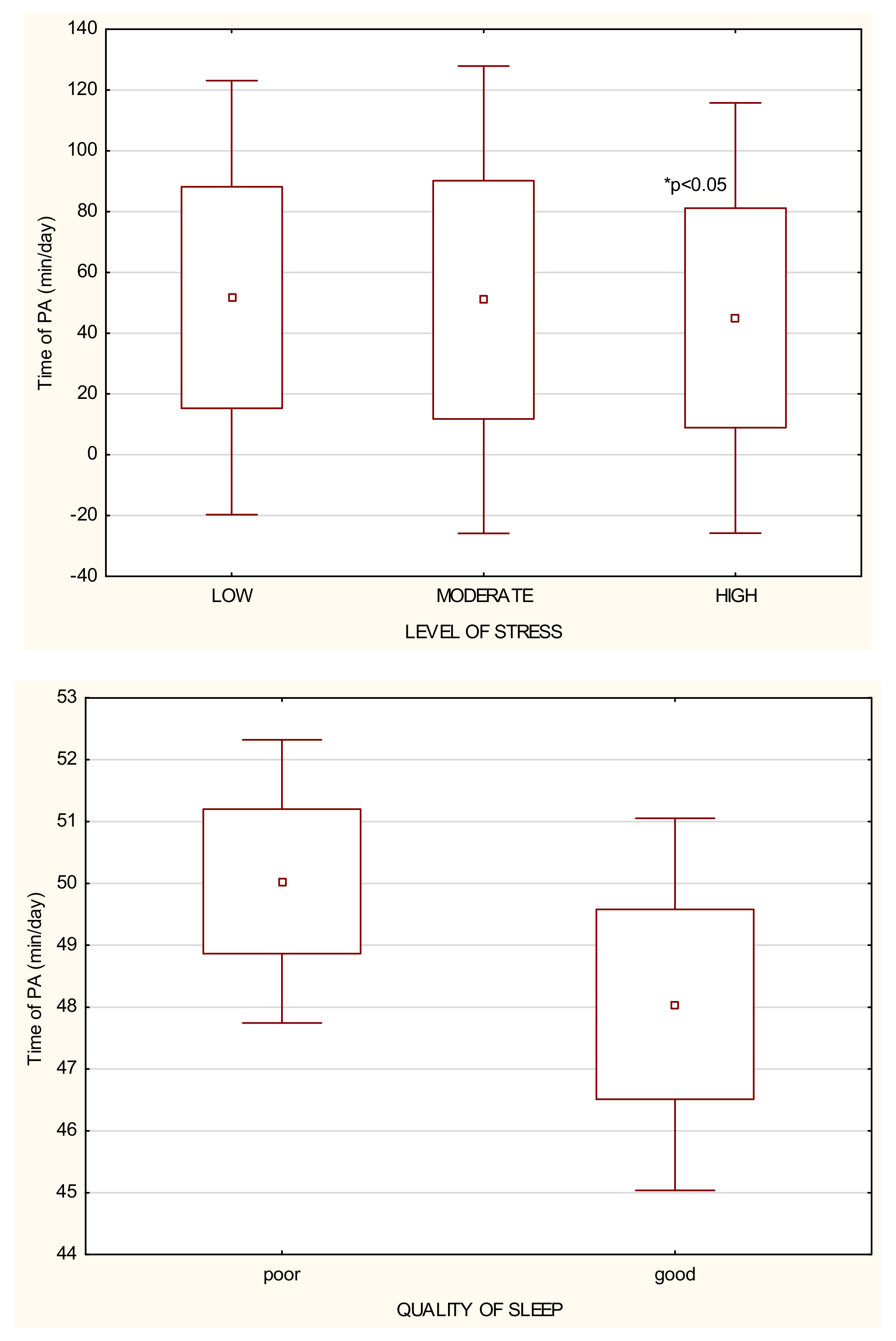
3.4. Optimal Time and Intensity of PA during Lockdown
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stam, H.J.; Stucki, G.; Bickenbach, J. Covid-19 and Post Intensive Care Syndrome: A Call for Action. J. Rehabil. Med. 2020, 52, jrm00044. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, K.; Gao, C.; Wang, X.; Zhang, C.; Wang, Z. Stress and sleep: A survey based on wearable sleep trackers among medical and nursing staff in Wuhan during the COVID-19 pandemic. Gen. Psychiatr. 2020, 33, e100260. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and Stress during COVID-19: Associations with Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian Adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Lahav, Y. Psychological distress related to COVID-19—The contribution of continuous traumatic stress. J. Affect. Disord. 2020, 277, 12316. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. COVID stress syndrome: Concept, structure, and correlates. Depress Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.; Benzeval, M.; Stansfeld, S.A. Employment transitions and mental health: An analysis from the British household panel survey. J. Epidemiol Community Health 2005, 59, 243–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Otsuka, Y.; Kaneita, Y.; Itani, O.; Nakagome, S.; Jike, M.; Ohida, T. Relationship between stress coping and sleep disorders among the general Japanese population: A nationwide representative survey. Sleep Med. 2017, 37, 38–45. [Google Scholar] [CrossRef]
- Xue, Z.; Lin, L.; Zhang, S.; Gong, J.; Liu, J.; Lu, J. Sleep problems and medical isolation during the SARS-CoV-2 outbreak. Sleep Med. 2020, 70, 112–115. [Google Scholar] [CrossRef]
- Voulgaris, A.; Ferini-Strambi, L.; Steiropoulos, P. Sleep medicine and COVID-19. Has a new era begun? Sleep Med. 2020, 73, 170–176. [Google Scholar] [CrossRef]
- Irwin, M.R.; Opp, M.R. Sleep Health: Reciprocal Regulation of Sleep and Innate Immunity. Neuropsychopharmacology 2017, 42, 129–155. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef] [PubMed]
- Ashdown-Franks, G.; Sabiston, C.M.; Stubbs, B. The evidence for physical activity in the management of major mental illnesses: A concise overview to inform busy clinicians’ practice and guide policy. Curr. Opin. Psychiatry 2019, 32, 375–380. [Google Scholar] [CrossRef]
- Bergier, J.; Kapka-Skrzypczak, L.; Biliński, P.; Paprzycki, P.; Wojtyła, A. Physical activity of Polish adolescents and young adults according to IPAQ: A population based study. Ann. Agric. Environ. Med. 2012, 19, 109–115. [Google Scholar] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. The compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IPAQ-Group. International Physical Activity Questionnaire; Cultural adaptation; IPAQ-Group. 2019. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 20 May 2021).
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale—Psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef] [Green Version]
- Baik, S.H.; Fox, R.S.; Mills, S.D.; Roesch, S.C.; Sadler, G.R.; Klonoff, E.A.; Malcarne, V.L. Reliability and validity of the Perceived Stress Scale-10 in Hispanic Americans with English or Spanish language preference. J. Health Psychol. 2019, 24, 628–639. [Google Scholar] [CrossRef]
- Hull, H.F. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2005, 11, 354–355. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Losada-Baltar, A.; Jiménez-Gonzalo, L.; Gallego-Alberto, L.; Pedroso-Chaparro, M.D.S.; Fernandes-Pires, J.; Márquez-González, M. “We’re staying at home”. Association of self-perceptions of aging, personal and family resources and loneliness with psychological distress during the lock-down period of COVID-19. J. Gerontol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting Physical Activity and Exercise: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef] [PubMed]
- Dominski, F.H.; Brandt, R. Do the benefits of exercise in indoor and outdoor environments during the COVID-19 pandemic outweigh the risks of infection? Sport Sci. Health 2020, 1–6. [Google Scholar] [CrossRef]
- Rizza, S.; Luzi, A.; Mavilio, M.; Ballanti, M.; Massimi, A.; Porzio, O.; Magrini, A.; Hannemann, J.; Menghini, R.; Lehrke, M.; et al. Alterations in Rev-ERBα/BMAL1 ratio and glycated hemoglobin in rotating shift workers: The EuRhythDia study. Acta Diabetol. 2021. [Google Scholar] [CrossRef]
- Mead, M.P.; Baron, K.; Sorby, M.; Irish, L.A. Daily Associations Between Sleep and Physical Activity. Int. J. Behav. Med. 2019, 26, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Matias, T.; Dominski, F.H.; Marks, D.F. Human needs in COVID-19 isolation. J. Health Psychol. 2020, 25, 871–882. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef]
- Conn, V.S. Anxiety outcomes after physical activity interventions: Meta-analysis findings. Nurs. Res. 2010, 59, 224–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizza, S.; Coppeta, L.; Grelli, S.; Ferrazza, G.; Chiocchi, M.; Vanni, G.; Bonomo, O.C.; Bellia, A.; Andreoni, M.; Magrini, A.; et al. High body mass index and night shift work are associated with COVID-19 in health care workers. J. Endocrinol. Investig. 2021, 44, 1097–1101. [Google Scholar] [CrossRef]
- Meira, C.M., Jr.; Meneguelli, K.S.; Leopoldo, M.P.G.; Florindo, A.A. Anxiety and Leisure-Domain Physical Activity Frequency, Duration, and Intensity During Covid-19 Pandemic. Front. Psychol. 2020, 11, 603770. [Google Scholar] [CrossRef] [PubMed]
- Crisafulli, A.; Pagliaro, P. Physical activity/inactivity and COVID-19. Eur. J. Prev. Cardiol. 2020. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socio-Demographic Variables | All the Study Group n (%) |
|---|---|
| Sex | |
| Female | 1681 (85.8) |
| Male | 278 (14.2) |
| Place of living | |
| City > 100,000 citizens | 999 (51.0) |
| City 20–100,000 citizens | 379 (19.3) |
| Town < 20,000 citizens | 180 (9.2) |
| Village | 401 (20.5) |
| Type of work | |
| Office work | 1149 (58.6) |
| Physical work | 445 (22.7) |
| Not applicable | 366 (18.7) |
| Occupational status | |
| Unemployed | 421 (21.5) |
| Employed | 1159 (59.1) |
| Retirement | 20 (1.0) |
| Student | 359 (18.4) |
| Form of work during pandemic | |
| Not working/unemployed | 976 (49.8) |
| Remote work | 639 (32.6) |
| In the workplace | 344 (17.6) |
| Form of lockdown | |
| Governmental restrictions | 1538 (78.5) |
| Quarantine | 23 (1.2) |
| No restrictions because of the type of occupation (medical staff, etc.) | 398 (20.3) |
| All the Study Group n (%) | |
|---|---|
| Level of PA during pandemic lockdown | |
| Low PA | 957 (49) |
| Moderate PA | 750 (38) |
| High PA | 252 (13) |
| Level of stress during pandemic lockdown | |
| Low (LLS) | 277 (14) |
| Moderate (MLS) | 1118 (57) |
| High (HLS) | 564 (29) |
| Quality of sleep during pandemic lockdown | |
| Poor | 1256 (64) |
| Good | 703 (36) |
| All the Study Group | Low Level of PA | Moderate Level of PA | High Level of PA | |
|---|---|---|---|---|
| Mean (±SD) | ||||
| Total PA (min/day) | 49.32 ± 38.01 | 24.30 ± 16.74 * | 69.82 ± 23.82 # | 116.12 ± 27.19 |
| Walking PA (min/day) | 30.82 ± 33.01 | 16.00 ± 16.25 | 42.06 ± 35.63 | 65.77 ± 41.73 |
| Moderate PA(min/day) | 7.98 ± 9.66 | 4.98 ± 7.62 | 11.23 ± 10.50 | 12.29 ± 10.81 |
| Vigorous PA (min/day) | 9.57 ± 12.14 | 2.96 ± 5.22 | 15.93 ± 12.85 | 18.71 ± 14.76 |
| PSSQ (in points) | 22.06 ± 7.36 | 22.68 ± 7.37 | 21.63 ± 7.25 | 20.96 ± 7.47 |
| GPQS (in points) | 8.23 ± 3.29 | 8.26 ± 2.71 | 8.13 ± 2.74 | 8.36 ± 5.82 |
| PA and Stress | Low Level of Stress | Moderate Level of Stress | High Level of Stress |
|---|---|---|---|
| Mean (±SD) | |||
| Total PA (min/day) | 51.71 ± 36.43 | 50.99 ± 39.21 | 44.99 ± 36.10 * |
| Walking PA (min/day) | 29.83 ± 30.47 | 31.99 ± 34.09 | 29.01 ± 31.99 |
| Moderate PA(min/day) | 8.93 ± 10.30 | 8.34 ± 9.69 | 6.82 ± 9.20 * |
| Vigorous PA (min/day) | 10.97 ± 12.55 | 9.72 ± 11.99 | 8.60 ± 12.18 * |
| PA and Sleep Quality | Poor Sleep Quality | Good Sleep Quality |
|---|---|---|
| Mean (±SD) | ||
| Total PA (min/day) | 50.03 ± 38.24 | 48.04 ± 37.60 |
| Walking PA (min/day) | 30.92 ± 33.18 | 30.63 ± 32.73 |
| Moderate PA (min/day) | 8.18 ± 9.68 | 7.61 ± 9.61 |
| Vigorous PA (min/day) | 9.94 ± 12.27 | 8.91 ± 11.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipert, A.; Kozłowski, R.; Timler, D.; Marczak, M.; Musiał, K.; Rasmus, P.; Kamecka, K.; Jegier, A. Physical Activity as a Predictor of the Level of Stress and Quality of Sleep during COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 5811. https://doi.org/10.3390/ijerph18115811
Lipert A, Kozłowski R, Timler D, Marczak M, Musiał K, Rasmus P, Kamecka K, Jegier A. Physical Activity as a Predictor of the Level of Stress and Quality of Sleep during COVID-19 Lockdown. International Journal of Environmental Research and Public Health. 2021; 18(11):5811. https://doi.org/10.3390/ijerph18115811
Chicago/Turabian StyleLipert, Anna, Remigiusz Kozłowski, Dariusz Timler, Michał Marczak, Kamila Musiał, Paweł Rasmus, Karolina Kamecka, and Anna Jegier. 2021. "Physical Activity as a Predictor of the Level of Stress and Quality of Sleep during COVID-19 Lockdown" International Journal of Environmental Research and Public Health 18, no. 11: 5811. https://doi.org/10.3390/ijerph18115811