
Evaluation of Four Fully Integrated Molecular Assays for the Detection of Respiratory Viruses during the Co-Circulation of SARS-CoV-2, Influenza and RSV


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Analytical Performances of the Idylla Assays
2.3. Prospective Analysis
3. Results
3.1. Analytical Performances of the Idylla Assays
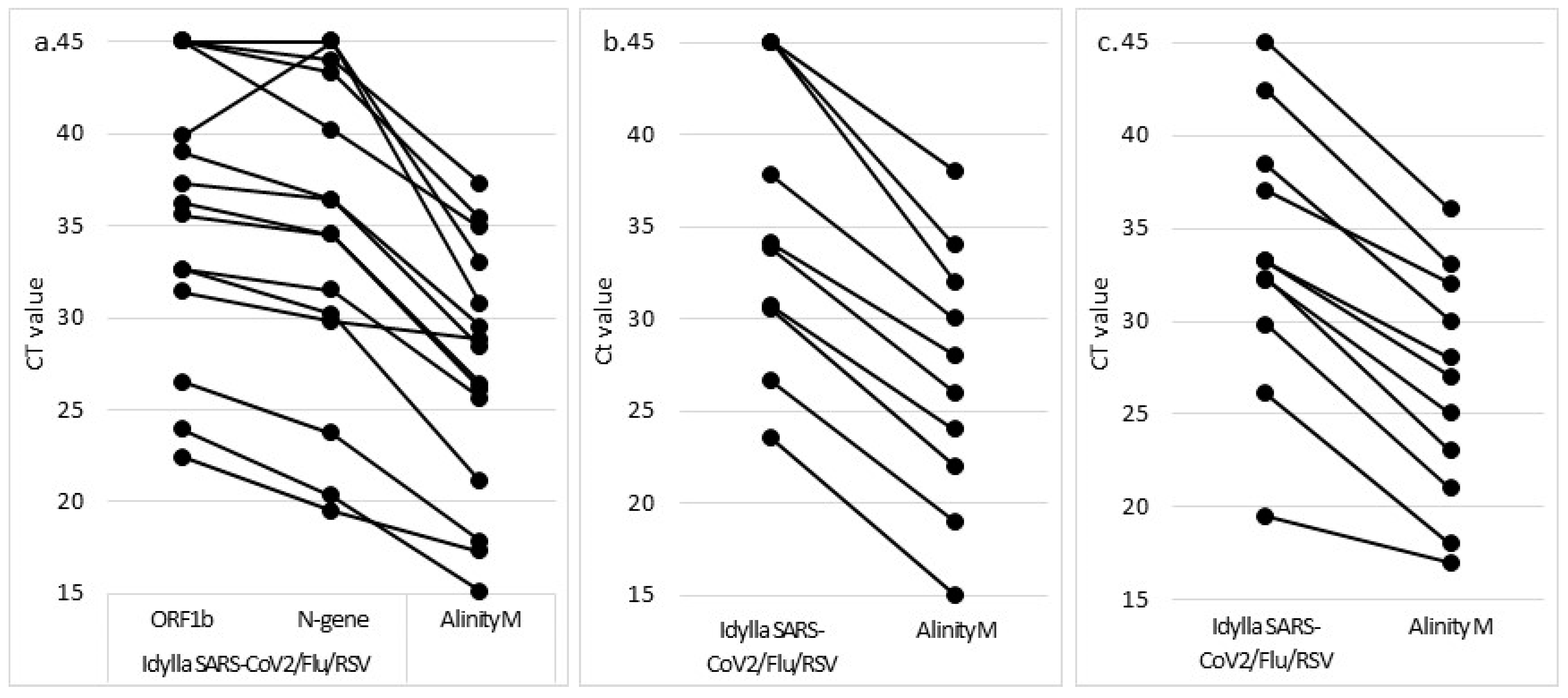
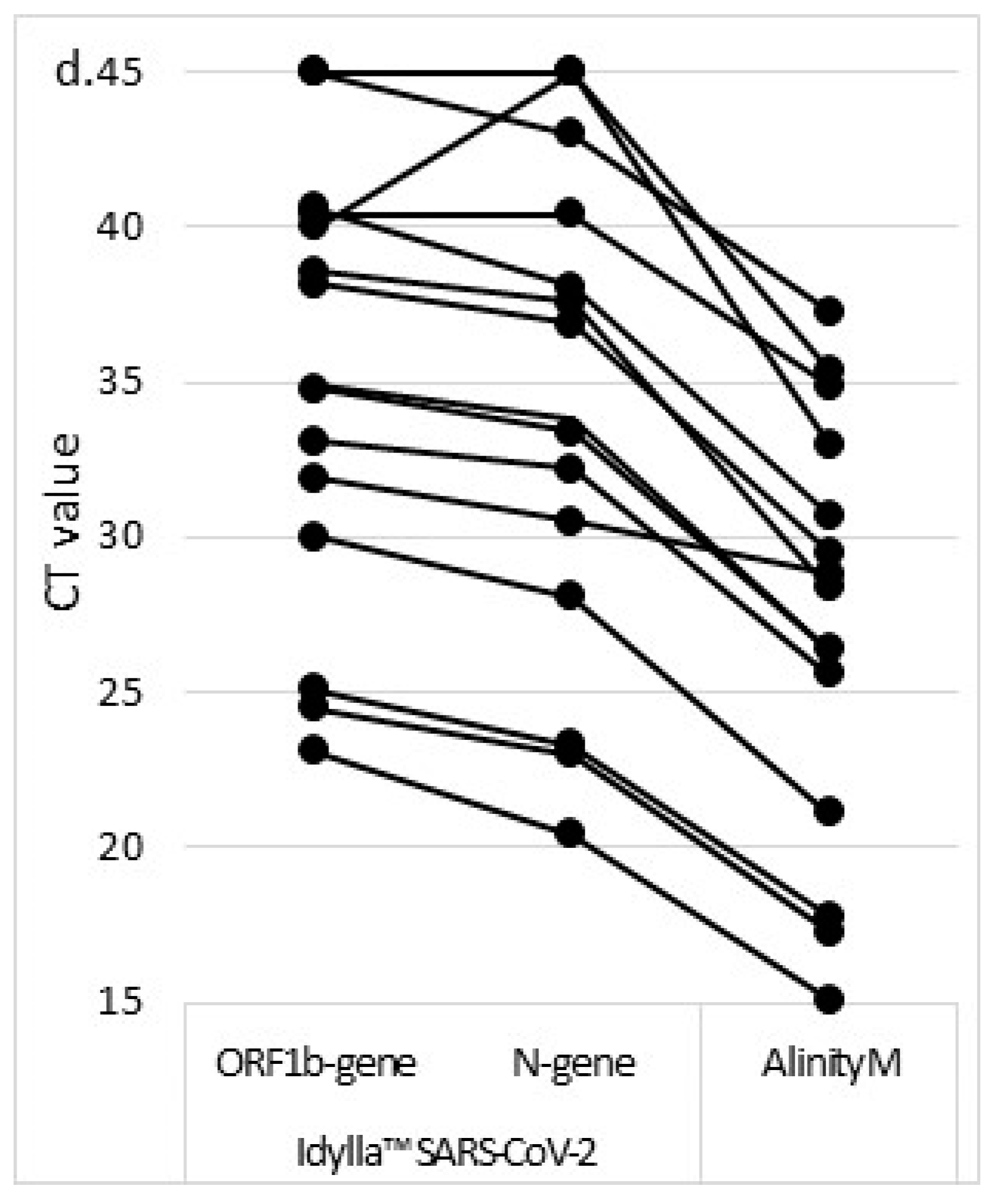
3.2. Prospective Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Uyeki, T.M.; Bernstein, H.H.; Bradley, J.S.; Englund, J.A.; File, T.M.; Fry, A.M.; Gravenstein, S.; Hayden, F.G.; Harper, S.A.; Hirshon, J.M.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America: 2018 Update on Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management of Seasonal Influenzaa. Clin. Infect. Dis. 2019, 68, 1–47. [Google Scholar] [CrossRef] [PubMed]
- European Center for Disease Prevention and Control. Treatment and Pharmaceutical Prophylaxis of COVID-19 2021. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/treatment (accessed on 5 February 2022).
- Farfour, E.; Ballester, M.-C.; Lecuru, M.; Verrat, A.; Imhaus, E.; Mellot, F.; Karnycheff, F.; Vasse, M.; Cerf, C.; Lesprit, P. COVID-19: Before stopping specific infection prevention and control measures; be sure to exclude the diagnosis. J. Hosp. Infect. 2020, 105, 375–376. [Google Scholar] [CrossRef] [PubMed]
- Farfour, E.; Pascreau, T.; Jolly, E.; Zia-Chahabi, S.; Mazaux, L.; Vasse, M. Spring is coming, where are the Respiratory Syncytial Virus and Influenza viruses? J. Clin. Virol. 2021, 139, 104824. [Google Scholar] [CrossRef] [PubMed]
- Casalegno, J.S.; Ploin, D.; Cantais, A.; Masson, E.; Bard, E.; Valette, M.; Fanget, R.; Targe, S.C.; Myar-Dury, A.-F.; Doret-Dion, M.; et al. Characteristics of the delayed respiratory syncytial virus epidemic, 2020/2021, Rhône Loire, France. Eurosurveillance 2021, 26, 2100630. [Google Scholar] [CrossRef]
- Marriott, D.; Beresford, R.; Mirdad, F.; Stark, D.; Glanville, A.; Chapman, S.; Harkness, J.; Dore, G.J.; Andresen, D.; Matthews, G.V. Concomitant Marked Decline in Prevalence of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Other Respiratory Viruses Among Symptomatic Patients Following Public Health Interventions in Australia: Data from St Vincent’s Hospital and associated screening clinics, Sydney, NSW. Clin. Infect. Dis. 2021, 72, 649–651. [Google Scholar] [CrossRef]
- De Luca, C.; Gragnano, G.; Conticelli, F.; Cennamo, M.; Pisapia, P.; Terracciano, D.; Malapelle, U.; Montella, E.; Triassi, M.; Troncone, G.; et al. Evaluation of a fully closed real time PCR platform for the detection of SARS-CoV-2 in nasopharyngeal swabs: A pilot study. J. Clin. Pathol. 2021. [Google Scholar] [CrossRef]
- Hofman, P.; Boutros, J.; Benchetrit, D.; Benzaquen, J.; Leroy, S.; Tanga, V.; Bordone, O.; Allégra, M.; Lespinet, V.; Fayada, J.; et al. A rapid near-patient RT-PCR test for suspected COVID-19: A study of the diagnostic accuracy. Ann. Transl. Med. 2021, 9, 921. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Found Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org (accessed on 7 June 2022).
- Smithgall, M.C.; Scherberkova, I.; Whittier, S.; Green, D.A. Comparison of Cepheid Xpert Xpress and Abbott ID Now to Roche cobas for the Rapid Detection of SARS-CoV-2. J. Clin. Virol. 2020, 128, 104428. [Google Scholar] [CrossRef]
- Mitchell, S.L.; George, K.S. Evaluation of the COVID-19 ID NOW EUA assay. J. Clin. Virol. 2020, 128, 104429. [Google Scholar] [CrossRef]
- Jin, R.; Pettengill, M.A.; Hartnett, N.L.; Auerbach, H.E.; Peiper, S.C.; Wang, Z. Commercial Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Molecular Assays: Superior Analytical Sensitivity of cobas SARS-CoV-2 Relative to NxTAG CoV Extended Panel and ID NOW COVID-19 Test. Arch. Pathol. Lab. Med. 2020, 144, 1303–1310. [Google Scholar] [CrossRef]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Scola, B.; Le Bideau, M.; Andreani, J.; Hoang, V.T.; Grimaldier, C.; Colson, P.; Gautret, P.; Raoult, D. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1059–1061. [Google Scholar] [CrossRef] [PubMed]
- Bullard, J.; Dust, K.; Funk, D.; Strong, J.E.; Alexander, D.; Garnett, L.; Boodman, C.; Bello, A.; Hedley, A.; Schiffman, Z.; et al. Predicting infectious severe acute respiratory syndrome coronavirus 2 from diagnostic samples. Clin. Infect. Dis. 2020, 71, 2663–2666. [Google Scholar] [CrossRef] [PubMed]
- Singanayagam, A.; Patel, M.; Charlett, A.; Bernal, J.L.; Saliba, V.; Ellis, J.; Ladhani, S.; Zambon, M.; Gopal, R. Duration of infectiousness and correlation with RT-PCR cycle threshold values in cases of COVID-19, England, January to May 2020. Eurosurveillance 2020, 25, 2001483. [Google Scholar] [CrossRef] [PubMed]
- Mowrer, C.; Creager, H.; Cawcutt, K.; Birge, J.; Lyden, E.; Van Schooneveld, T.C.; Rupp, M.E.; Hewlett, A. Evaluation of cycle threshold values at deisolation. Infect. Control Hosp. Epidemiol. 2021, 43, 794–796. [Google Scholar] [CrossRef]
- Therese, S.S.; Julian, D.; Bianca, J.; Carmen, S.; Sarah, G.; Stephan, K.; Sturmbauer, C.; Posch, W.; Walder, G. An in vitro model for assessment of SARS-CoV-2 infectivity by defining the correlation between virus isolation and quantitative PCR value: Isolation success of SARS-CoV-2 from oropharyngeal swabs correlates negatively with Cq value. Virol. J. 2021, 18, 71. [Google Scholar] [CrossRef]
- Basso, D.; Aita, A.; Navaglia, F.; Franchin, E.; Fioretto, P.; Moz, S.; Bozzato, D.; Zambon, C.F.; Martin, B.; Prà, C.D.; et al. SARS-CoV-2 RNA identification in nasopharyngeal swabs: Issues in pre-analytics. Clin. Chem. Lab. Med. 2020, 58, 1579–1586. [Google Scholar] [CrossRef]
- Cao, X.J.; Fang, K.Y.; Li, Y.P.; Zhou, J.; Guo, X.G. The Diagnostic Accuracy of Xpert Xpress to SARS-CoV-2: A systematic review. J. Virol. Methods 2022, 301, 114460. [Google Scholar] [CrossRef]
- Lee, J.; Song, J.U. Diagnostic accuracy of the Cepheid Xpert Xpress and the Abbott ID NOW assay for rapid detection of SARS-CoV-2: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 4523–4531. [Google Scholar] [CrossRef]
- Mahmoud, S.A.; Ganesan, S.; Ibrahim, E.; Thakre, B.; Teddy, J.G.; Raheja, P.; Zaher, W.A. Evaluation of six different rapid methods for nucleic acid detection of SARS-CoV-2 virus. J. Med. Virol. 2021, 93, 5538–5543. [Google Scholar] [CrossRef]
- Farfour, E.; Roux, A.; Ballester, M.; Gagneur, L.; Renaux, C.; Jolly, E.; Vasse, M. Improved performances of the second generation of the ID NOW influenza A & B 2® and comparison with the GeneXpert®. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1681–1686. [Google Scholar] [CrossRef] [PubMed]
- Trabattoni, E.; Le, V.; Pilmis, B.; de Ponfilly, G.P.; Caisso, C.; Couzigou, C.; Vidal, B.; Mizrahi, A.; Ganansia, O.; Le Monnier, A.; et al. Implementation of Alere i Influenza A & B point of care test for the diagnosis of influenza in an ED. Am. J. Emerg. Med. 2018, 36, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, N.; Michael, J.; Doran, K.; Montgomery, E.; Selvarangan, R. Comparison of the ID Now Influenza A & B 2, Cobas Influenza A/B, and Xpert Xpress Flu Point-of-Care Nucleic Acid Amplification Tests for Influenza A/B Virus Detection in Children. J. Clin. Microbiol. 2020, 58, 3. [Google Scholar] [CrossRef] [Green Version]
- NguyenVan, J.C.; Gerlier, C.; Pilmis, B.; Mizrahi, A.; Péan de Ponfilly, G.; Khaterchi, A.; Enouf, V.; Ganansia, O.; Monnier, A. Prospective evaluation of ID NOW COVID-19 assay used as point-of-care test in an emergency department. J. Clin. Virol. 2021, 145, 105021. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Method | Volume of Sample ** | Viral Genes Amplified (Number of Fluorphore) | ||||
|---|---|---|---|---|---|---|
| SARS-CoV-2 | Influenza A | Influenza B | RSV | |||
| Alinity M RESP-4-Plex | RT-PCR | 500 µL | ORF1b and N (1) | Matrix (1) | NS1 (1) | Matrix (1) |
| Idylla™ SARS-CoV-2 | RT-PCR | 200 µL | ORF1b (3) N (2) | |||
| Idylla™ SARS-CoV2/Flu/RSV | RT-PCR | 400 µL | ORF1b (1) N (2) | - * | - | - |
| ID NOW COVID-19 | Isothermal amplification | 200 µL | ORF1b (1) | |||
| ID NOW influenza A & B 2 | Isothermal amplification | 200 µL | Matrix (1) | Matrix (1) | Fusion and Nucleocapsid (1) | |
| Conservation | Idylla™ SARS-CoV-2 | Idylla™ SARS-CoV2/Flu/RSV | ID NOW COVID | ID NOW Influenza A & B 2 | |
|---|---|---|---|---|---|
| Analytical | |||||
| 15 SARS-CoV-2 | Fresh | X * | X | ||
| 11 influenza A | Fresh | X | |||
| 1 influenza B | Fresh | X | |||
| 1 RSV | Fresh | X | |||
| 20 Others viruses | Frozen | X | X | ||
| Prospective | |||||
| 218 NPS | Fresh | X | X | X | X |
| Clinical NPS * with Known Viruses | Number Tested | |
|---|---|---|
| Idylla™ SARS-CoV2/Flu/RSV | Idylla™ SARS-CoV-2 | |
| Influenza A | - | 3 |
| Influenza B | - | 1 |
| RSV | - | 3 |
| Parainfluenza 1 | 1 | 1 |
| Parainfluenza 3 | 1 | 1 |
| Parainfluenza 4 | 1 | 1 |
| Coronavirus OC43 | 2 | 2 |
| Coronavirus NL63 | 2 | 2 |
| Coronavirus 229E | 2 | 2 |
| Human Metapneumovirus | 1 | 1 |
| Adenovirus | 1 | 1 |
| Enterovirus | 1 | 1 |
| Rhinovirus | 1 | 1 |
| Sample ID | Idylla™ SARS-CoV2/Flu/RSV (Ct Value) | Alinity M Target (Ct Value) | ID NOW COVID-19 | ID NOW Influenza A & B 2 | Idylla™ SARS-CoV-2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ORF1b | N | N | Flu A | VRS | Flu B | RNAseP | |||||
| 959702 | 29.1 | 27.2 | 27.3 | n.d. * | n.d. | n.d. | 37.2 | COVID (17.6) | Positive | Negative | Positive |
| 811101 | n.d. | n.d. | n.d. | n.d. | n.d. | n.d. | 37.6 | COVID (31.5) | Positive | Negative | Positive |
| 879801 | 31.1 | 28.9 | 29.1 | n.d. | n.d. | n.d. | 36.6 | COVID (19.1) | Positive | Negative | Positive |
| 345101 | n.d. | n.d. | n.d. | n.d. | 37.1 | n.d. | 36.5 | RSV (24.0) | Negative | Negative | Negative |
| (a) | |||||||||||||
| Sample ID | Sex | Age | Alinity M (Ct) | ID NOW COVID | Idylla™ SARS-CoV-2 | Idylla™ SARS-CoV2/Flu/RSV | Delay since Symptoms Onset | COVID-19 Vaccine | Symptoms | Oxygen Therapy | Outcome | ||
| Qualitative Result | Targets Ct | RNAseP (Ct) | |||||||||||
| 832301 | F | 21 | 31.2 | Negative | Positive | Negative | ORF1b a = nd N b = 44.3 N c = 44.3 | 34,5 | 3 | No | Abdominal pain | No | Discharge |
| 930001 | M | 46 | 31.8 | Negative | Negative | Negative | ORF1b a = nd N b = nd N c = nd | 34.3 | 14 | No | Flu-like syndrome | No | Discharge |
| 882501 | F | 31 | 32.3 | Negative | Positive | Negative | ORF1b a = nd N b = nd N c = nd | 35.3 | 5 | No | Flu-like syndrome | No | Discharge |
| 909701 | M | 29 | 33.9 | Negative | Positive | Negative | ORF1b a = nd N b = nd N c = 43.13 | 33.4 | 10 | n.a. | Headhache hypoaesthesia of the right side | No | Discharge |
| 909301 | M | 22 | 36.4 | Negative | Positive | Negative | ORF1b a = nd N b = 41.15 N c = 43.29 | 30.2 | 14 | No | Flu-like syndrome | No | Discharge |
| (b) | |||||||||||||
| Sample ID | Sex | Age | Alinity M (Ct) | ID NOW Indluenza A & B 2 | Idylla™ SARS-CoV2/Flu/RSV | Delay since Symptoms Onset | Symptoms | Oxygen Therapy | Outcome | ||||
| Flu A (Ct) | RNAseP | ||||||||||||
| 501001 | M | 68 | 31 | Negative | Positive (39.7) | 33.6 | 7 | Dyspnea | 4 L | Hospitalization | |||
| 661701 | M | 39 | 36 | Negative | Negative | 33.6 | 1 | Flu-like syndrome | No | Discharge | |||
| (c) | |||||||||||||
| Sample ID | Sex | Age | Alinity M (Ct) | Idylla™ SARS-CoV2/Flu/RSV | Delay since Symptoms Onset | Symptoms | Oxygen Therapy | Outcome | |||||
| RSV | RNAseP E | ||||||||||||
| 842101 | F | 81 | 31 | Negative | 33.4 | n.a. | Dyspnea | 6 L | Hospitalization | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farfour, E.; Yung, T.; Baudoin, R.; Vasse, M. Evaluation of Four Fully Integrated Molecular Assays for the Detection of Respiratory Viruses during the Co-Circulation of SARS-CoV-2, Influenza and RSV. J. Clin. Med. 2022, 11, 3942. https://doi.org/10.3390/jcm11143942
Farfour E, Yung T, Baudoin R, Vasse M. Evaluation of Four Fully Integrated Molecular Assays for the Detection of Respiratory Viruses during the Co-Circulation of SARS-CoV-2, Influenza and RSV. Journal of Clinical Medicine. 2022; 11(14):3942. https://doi.org/10.3390/jcm11143942
Chicago/Turabian StyleFarfour, Eric, Thomas Yung, Robin Baudoin, and Marc Vasse. 2022. "Evaluation of Four Fully Integrated Molecular Assays for the Detection of Respiratory Viruses during the Co-Circulation of SARS-CoV-2, Influenza and RSV" Journal of Clinical Medicine 11, no. 14: 3942. https://doi.org/10.3390/jcm11143942